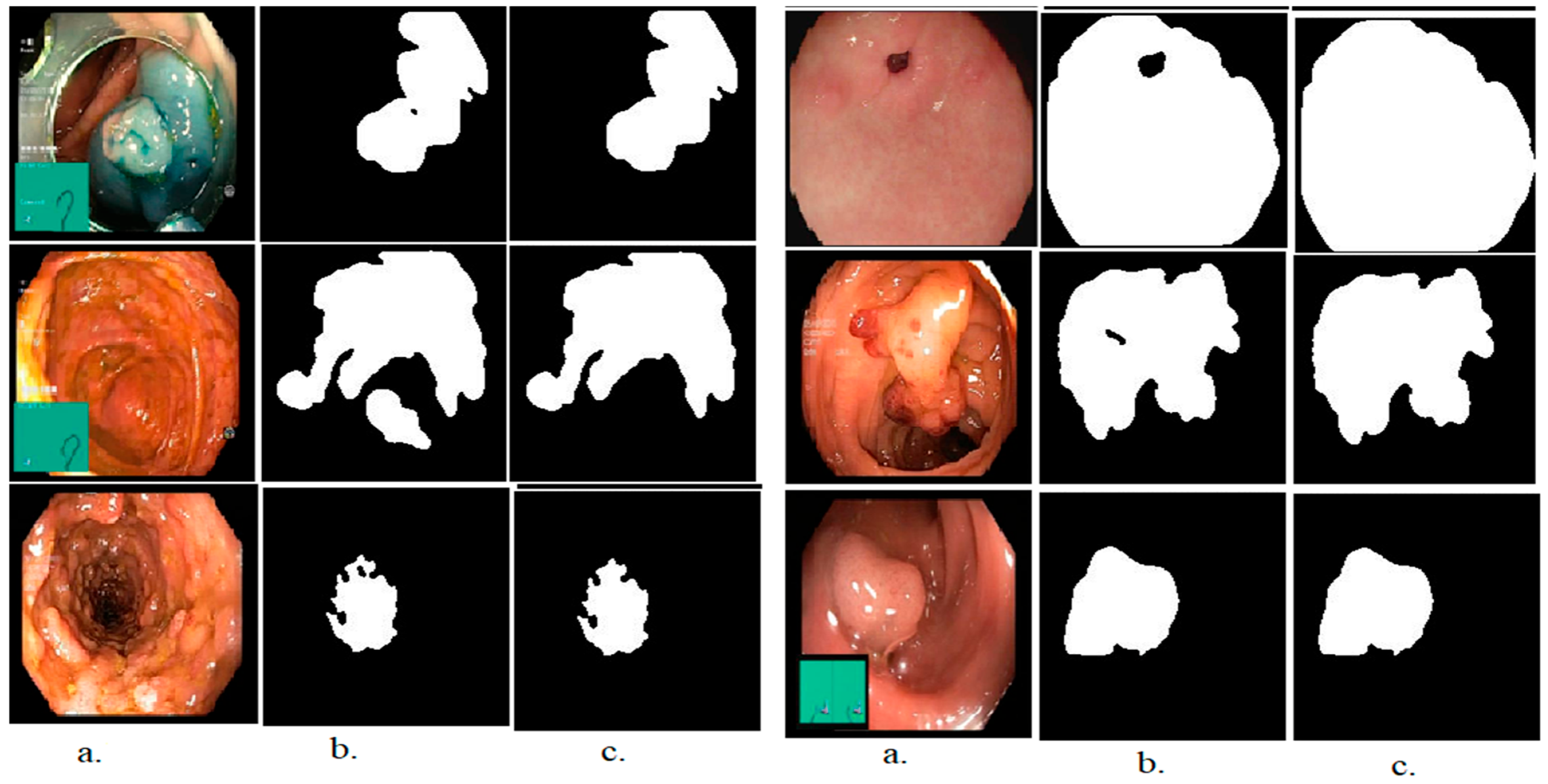
4.3. Segmentation Performance Evaluation
The segmentation method is one of the most important steps to biomedical image processing, which is widely used in this field to select the affected region and separate it from the rest of the image. In this study, the Active Contour method was applied, which acts as a snake movement and starts with a point and moves along the edges of the lesion until the region of interest (the lesion region) is completely selected, then separated it from the rest of the image. The segmentation method based on Active Contour models was validated by accuracy, precision and recall measures, which reached 99.3%, 99.7%, and 99.6%, respectively. Thus, the lesion region was separated with a promising accuracy and high efficiency, and the region of interest was sent to the feature extraction stage, to extract the most important color, texture, and shape features.
4.5. Results of Second Proposed System (CNN Models)
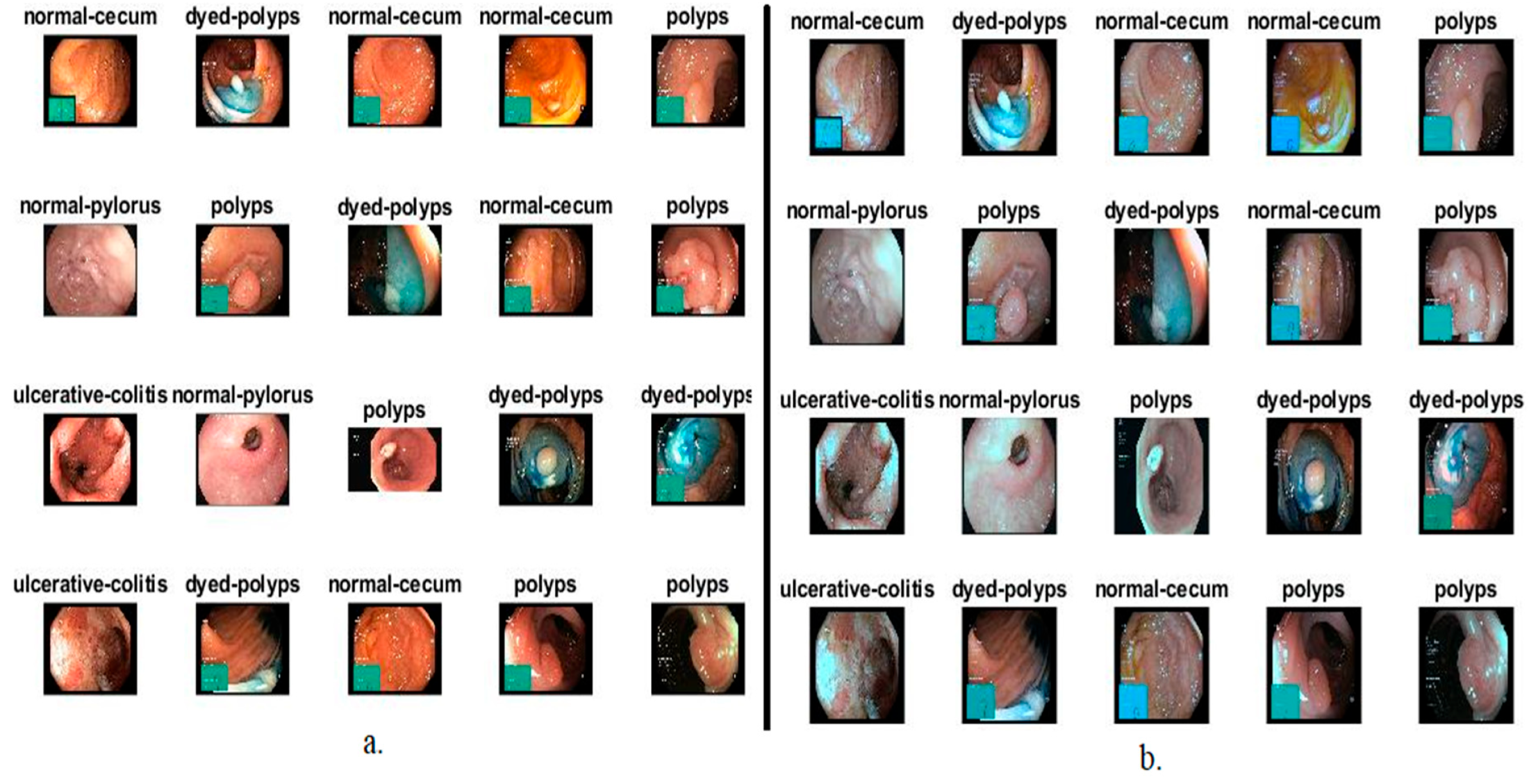
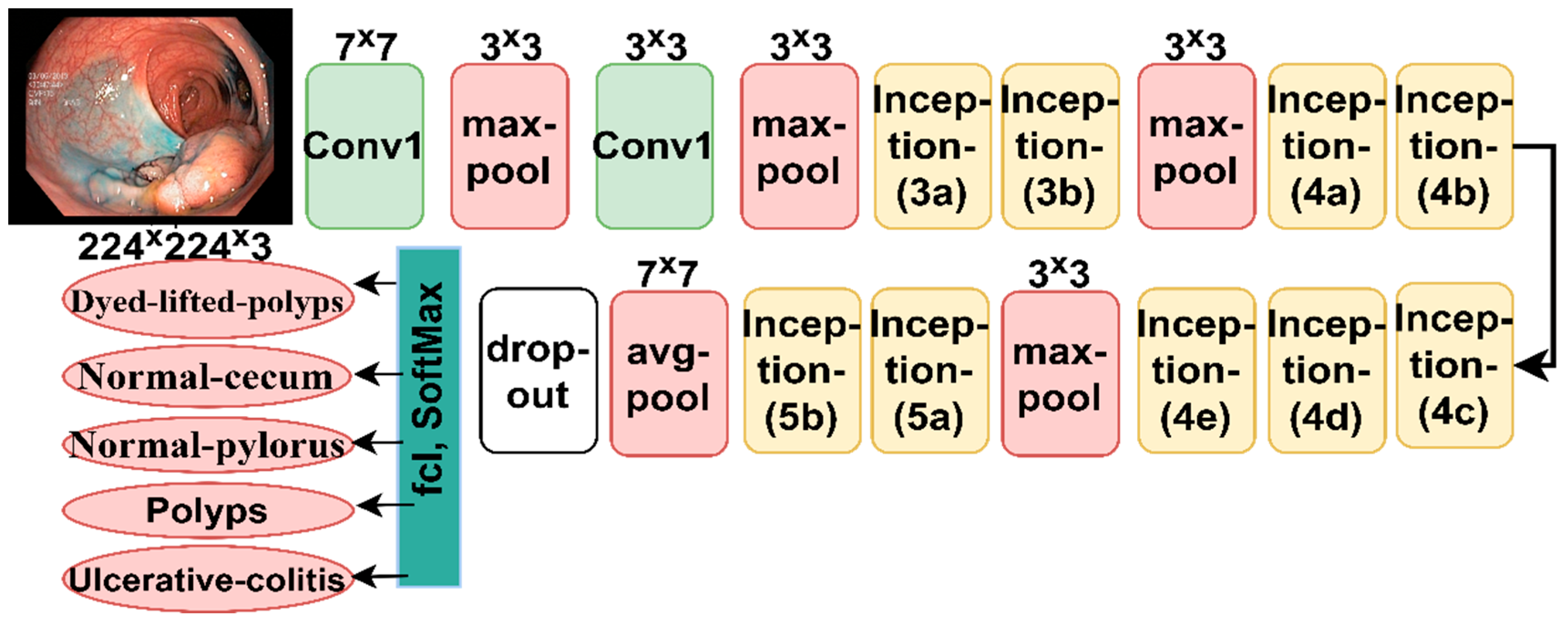
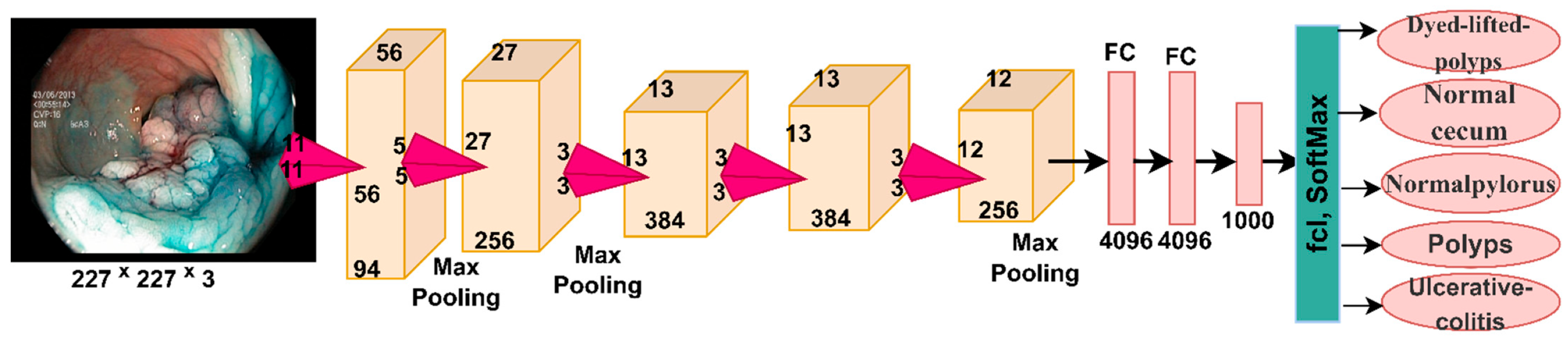
In this section, the endoscopic image of the lower GI dataset is evaluated using the pre-trained CNN models, GoogLeNet and AlexNet. Transfer learning method is pre-trained CNN models on more than one million images to produce more than a thousand classes. Thus, the performance of the experience of the previously trained models is transferred to perform new tasks, as in this study, where the experience of the CNN models for diagnosing lower GI dataset is transferred. One of the challenges facing CNN models is the overfitting problem during the training phase of the dataset. Thus, CNN models introduce the data augmentation technique to overcome this challenge, which artificially augments dataset images.
Table 3 summarizes the lower GI dataset before and after using the data augmentation during the training phase. Images are artificially augmented through many operations such as rotation, flipping, shifting, and others. Each image was incremented seven times for all classes equally.
Table 4 summarizes the tuning of the CNN GoogLeNet and AlexNet models, where the adam optimizer and Mini Batch Size, Mini Batch Size, Initial Learn Rate, dataset training time for each model and Validation Frequency were set.
The GoogLeNet and AlexNet models achieved superior results for diagnosing endoscopic images of the gastro-intestinal disease dataset.
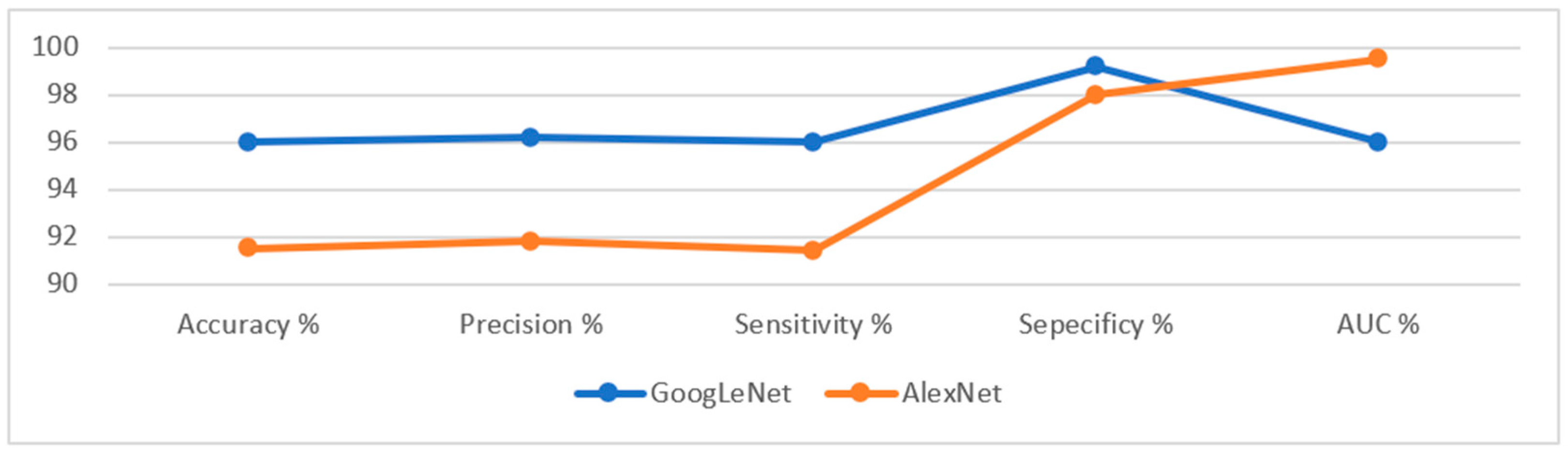
Table 5 describes the evaluation results of the GoogLeNet and AlexNet models, where it is noted that the GoogLeNet model is superior to the AlexNet model. The GoogLeNet model achieved an accuracy of 96%, a precision of 96.2%, a sensitivity of 96%, a specificity of 99.2%, and an AUC of 96%. In contrast, the AlexNet model achieved an accuracy of 91.5%, a precision of 91.8%, a sensitivity of 91.4%, a specificity of 98%, and an AUC of 99.53%.
Figure 18 presents the evaluation results of the performance of the GoogLeNet and AlexNet models on the lower GI dataset in a graph.
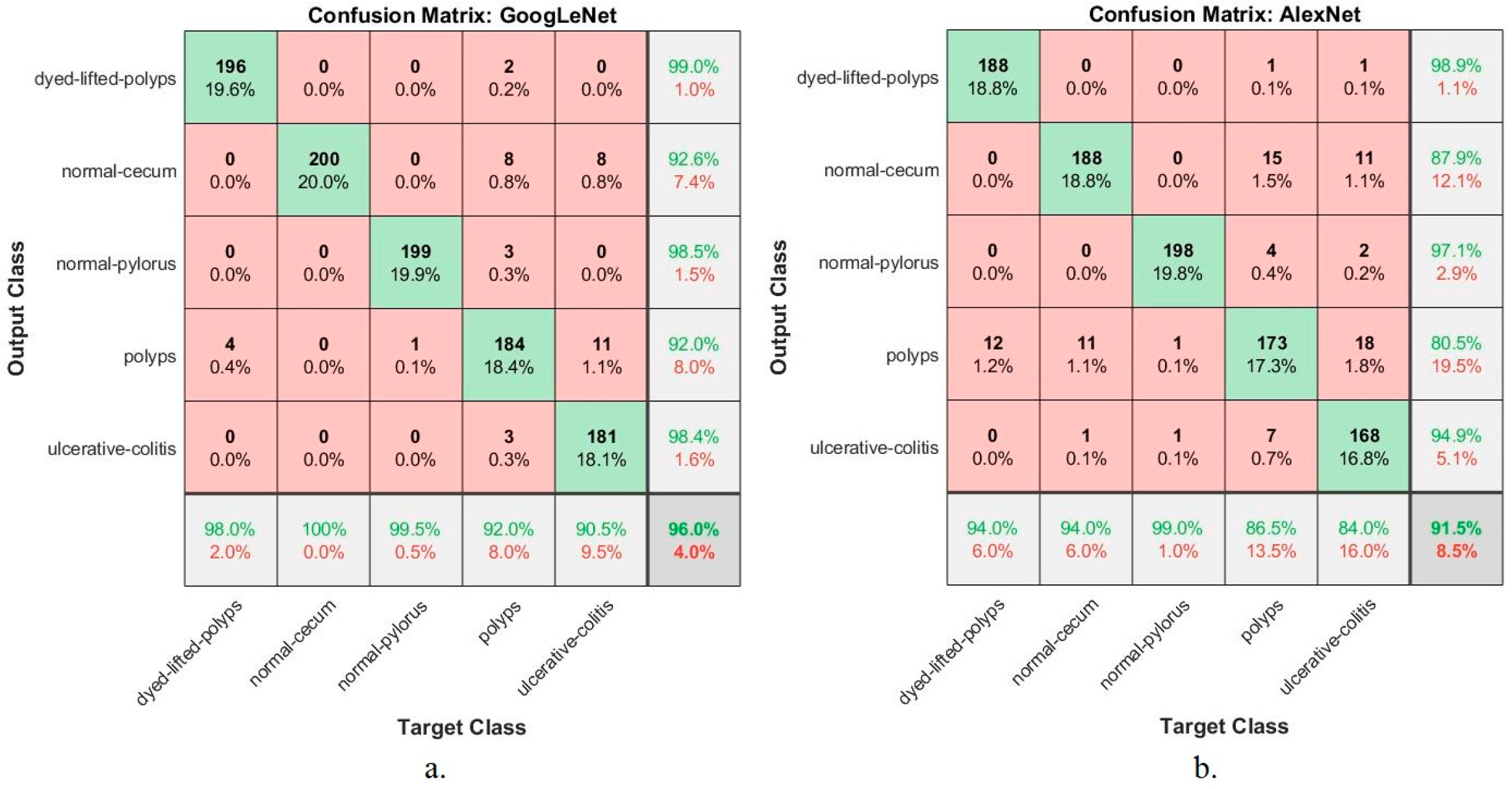
Figure 19 describes the confusion matrix generated by the CNN models, GoogLeNet and AlexNet for the early diagnosis of lower GI disease. In contrast, the confusion matrix describes all dataset samples that are correctly or incorrectly categorized. It also describes the diagnostic accuracy reached by the models for each class. The figure shows that dyed-lifted-polyps was diagnosed with 98% and 94% accuracy for GoogLeNet and AlexNet, respectively. Normal-cecum was diagnosed with 100% and 94% accuracy for GoogLeNet and AlexNet, respectively. Normal-pylorus was diagnosed with 99.5% and 99% accuracy for GoogLeNet and AlexNet, respectively. Polyps were diagnosed with an accuracy of 92% and 86.5% for GoogLeNet and AlexNet, respectively. Ulcerative colitis was diagnosed with an accuracy of 90.5% and 84% for GoogLeNet and AlexNet, respectively.
4.6. Results of Third Proposed System (Hybrid CNN with SVM)
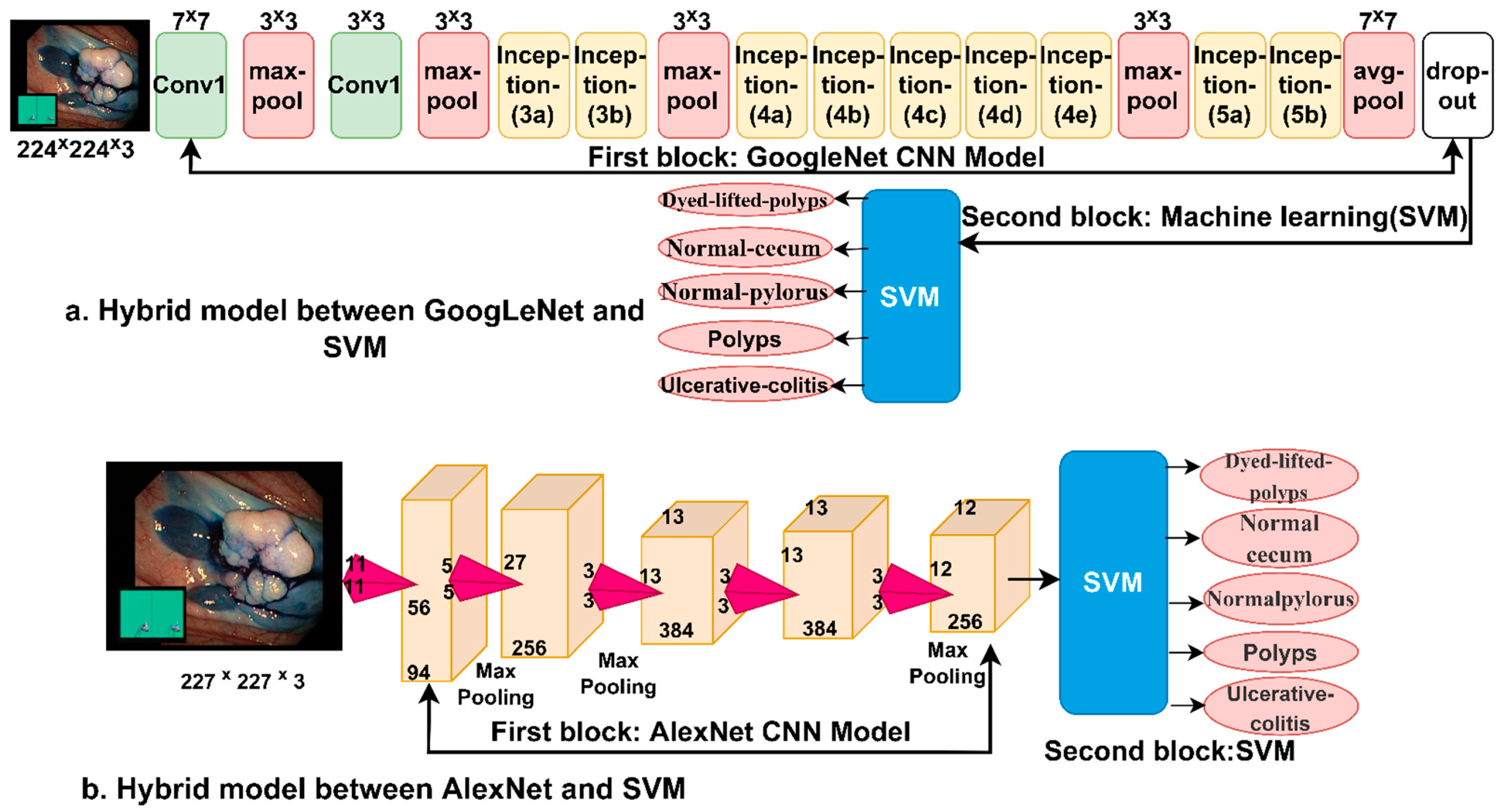
This section presents the findings of the hybrid techniques between CNN models (GoogLeNet and AlexNet) and the SVM algorithm. The technique consists of two blocks: the first is CNN models for extracting feature maps, and the second block is the SVM algorithm for classifying feature maps. One of the most important reasons for using this technique is that it requires medium-specification computer resources, speed in training the dataset, and high accuracy in diagnosis.
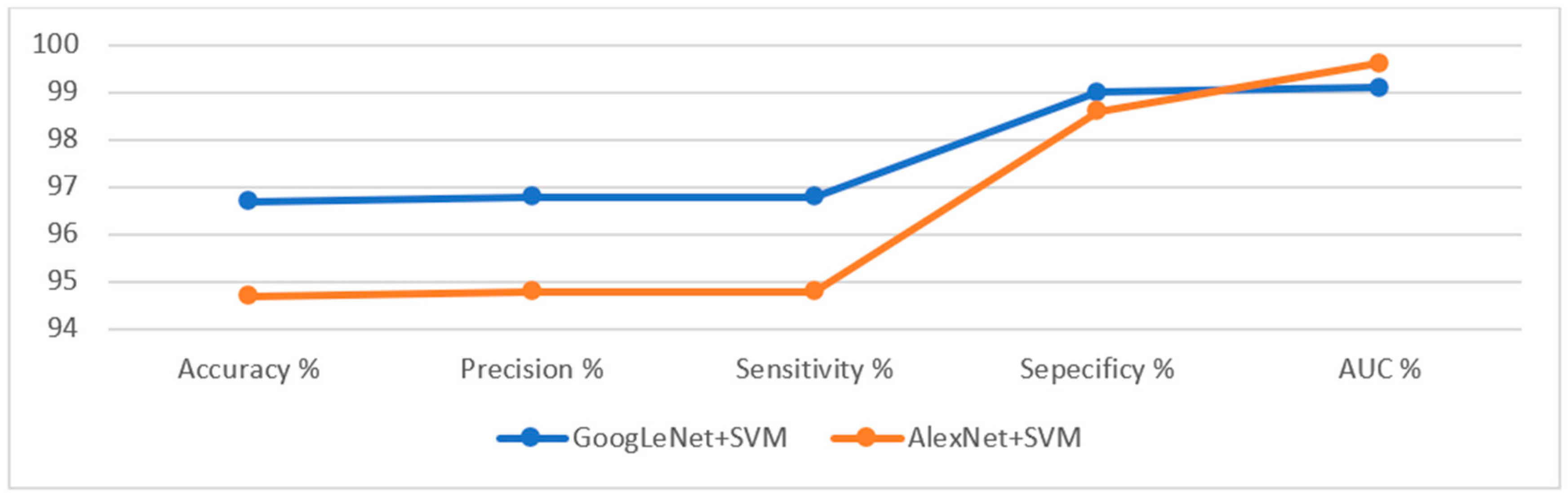
Table 6 summarizes the assessment of the lower gastrointestinal diseases dataset by hybrid GoogLeNet+SVM and AlexNet+SVM technique for early diagnosis of gastrointestinal tumors and ulcers. The GoogLeNet+SVM hybrid technique is superior to AlexNet+SVM. The GoogLeNet+SVM achieved an accuracy of 96.7%, a precision of 96.8%, a sensitivity of 96.8%, a specificity of 99%, and an AUC of 99.1%. In contrast, the AlexNet+SVM model achieved an accuracy of 94.7%, a precision of 94.8%, a sensitivity of 94.8%, a specificity of 98.6%, and an AUC of 99.6%.
Figure 20 displays the evaluation results of the GoogLeNet+SVM and AlexNet+SVM techniques on the lower GI dataset in a graph.
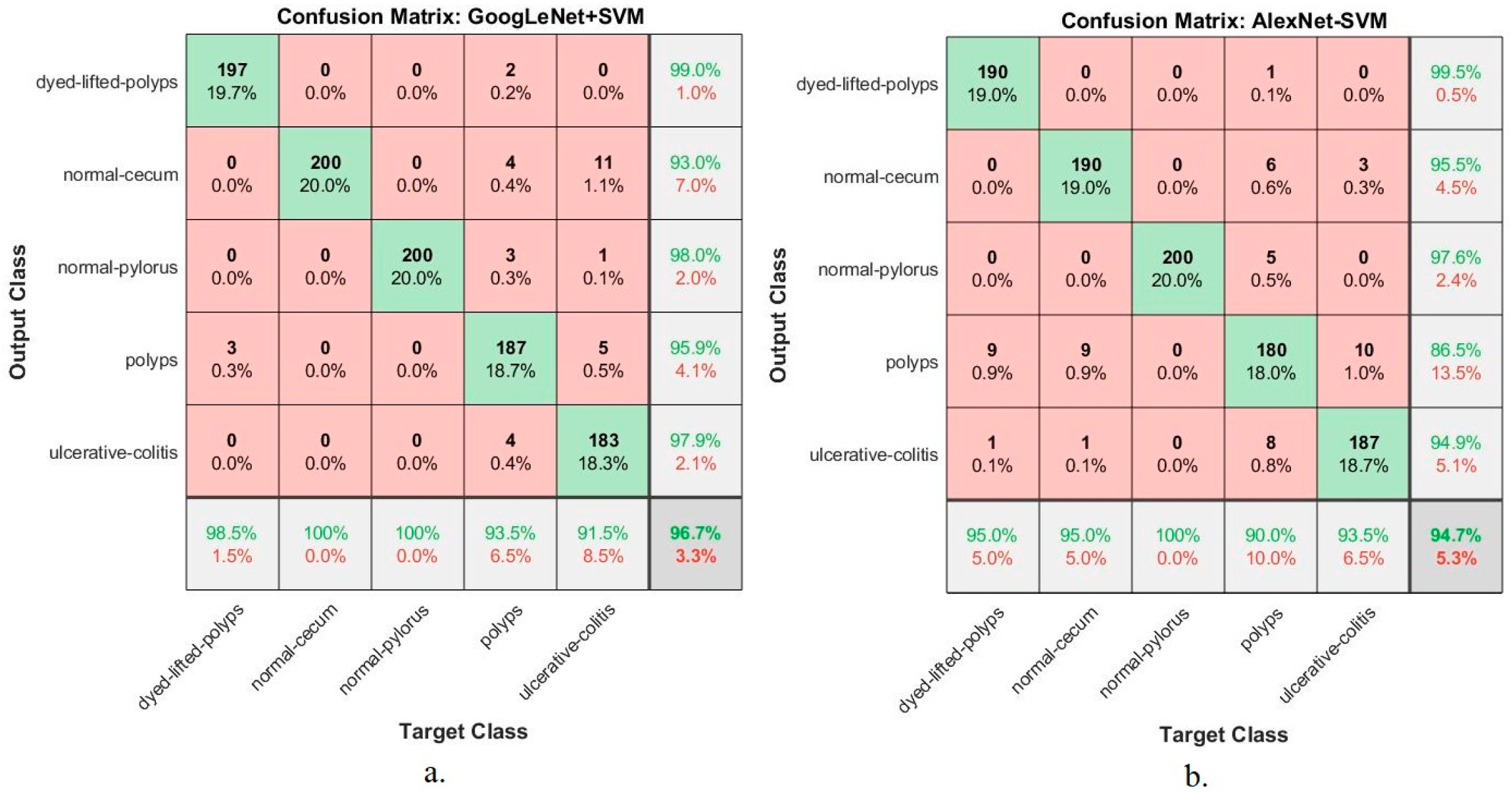
Figure 21 shows the performance of the hybrid techniques GoogLeNet+SVM and AlexNet+SVM for diagnosing lower gastrointestinal disease dataset in the form of a confusion matrix. The hybrid methods produced a confusion matrix that describes all samples of the dataset correctly labelled represented in the primary diameter and all samples incorrectly classified and distributed over the rest of the matrix cells. The figure shows the performance of hybrid techniques for diagnosing each disease and the overall accuracy. The figure shows that dyed-lifted-polyps was diagnosed with 98.5% and 95% accuracy for GoogLeNet+SVM and AlexNet+SVM, respectively. Normal-cecum was diagnosed with 100% and 95% accuracy for GoogLeNet+SVM and AlexNet+SVM, respectively. Normal-pylorus was diagnosed with 100% and 100% accuracy for GoogLeNet+SVM and AlexNet+SVM, respectively. Polyps were diagnosed with an accuracy of 93.5% and 90% for GoogLeNet+SVM and AlexNet+SVM, respectively. Ulcerative colitis was diagnosed with an accuracy of 91.5% and 93.5% for GoogLeNet+SVM and AlexNet+SVM, respectively.
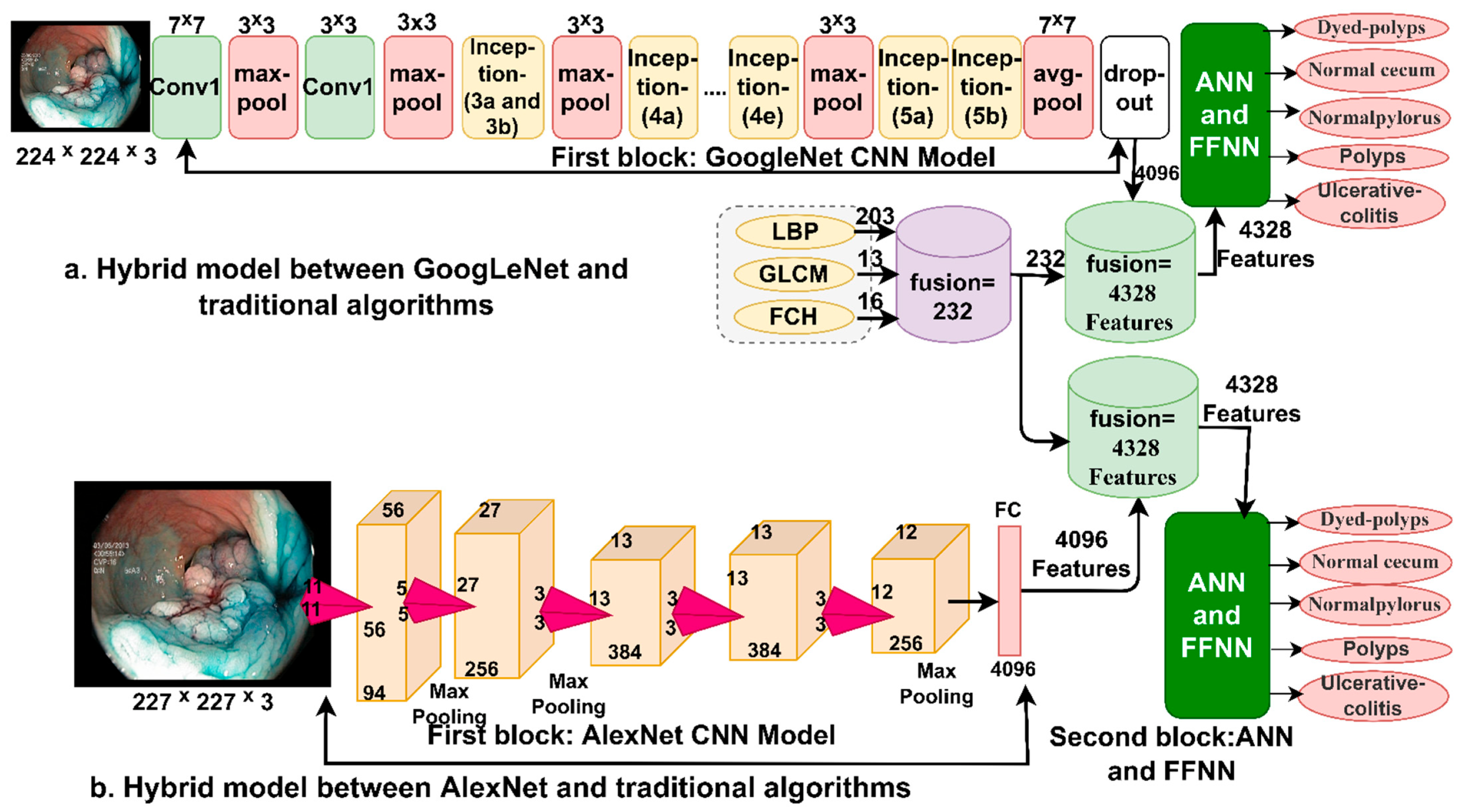
4.7. Results of Fourth Proposed System (Hybrid Features CNN and Traditional Algorithms)
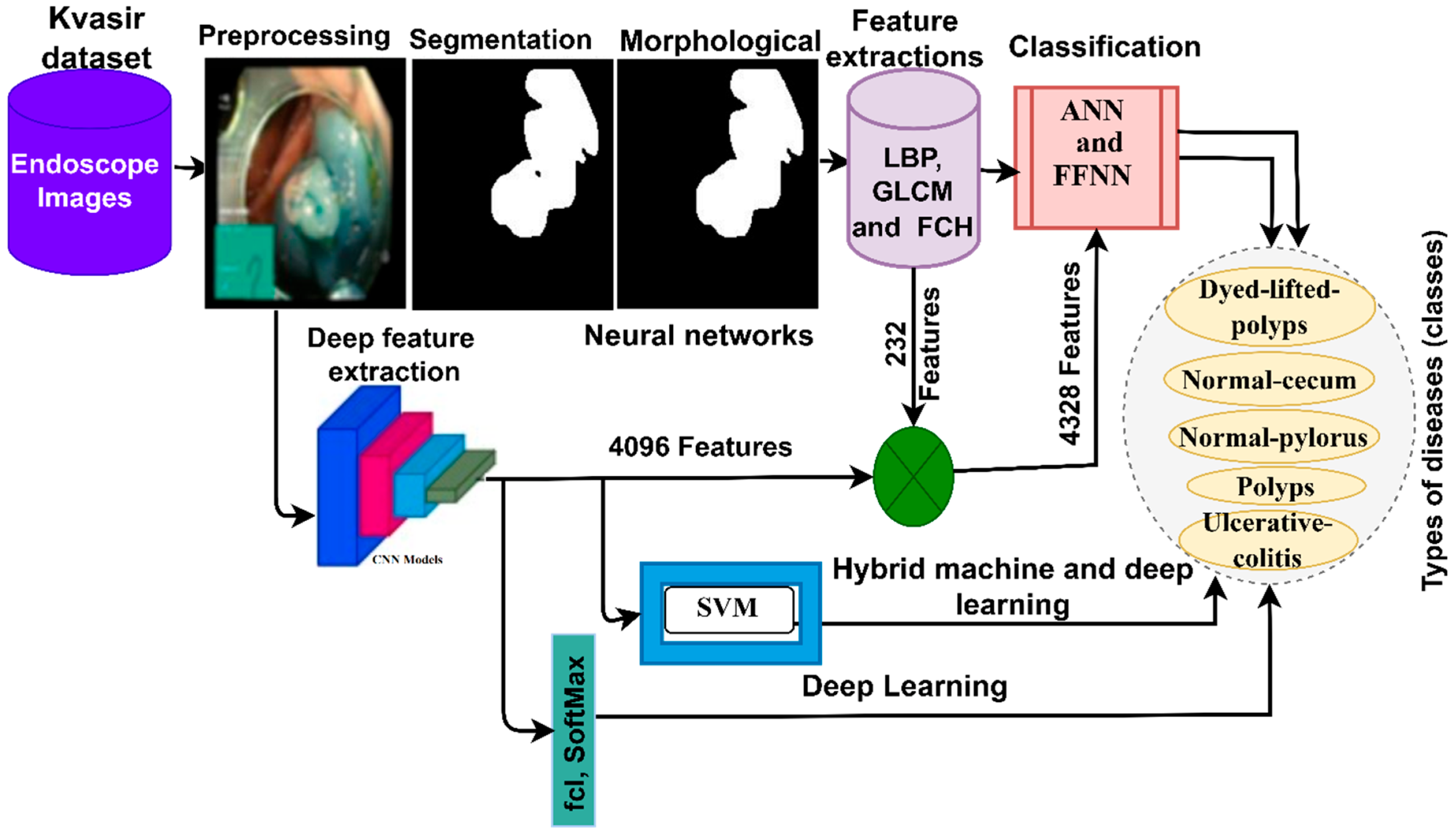
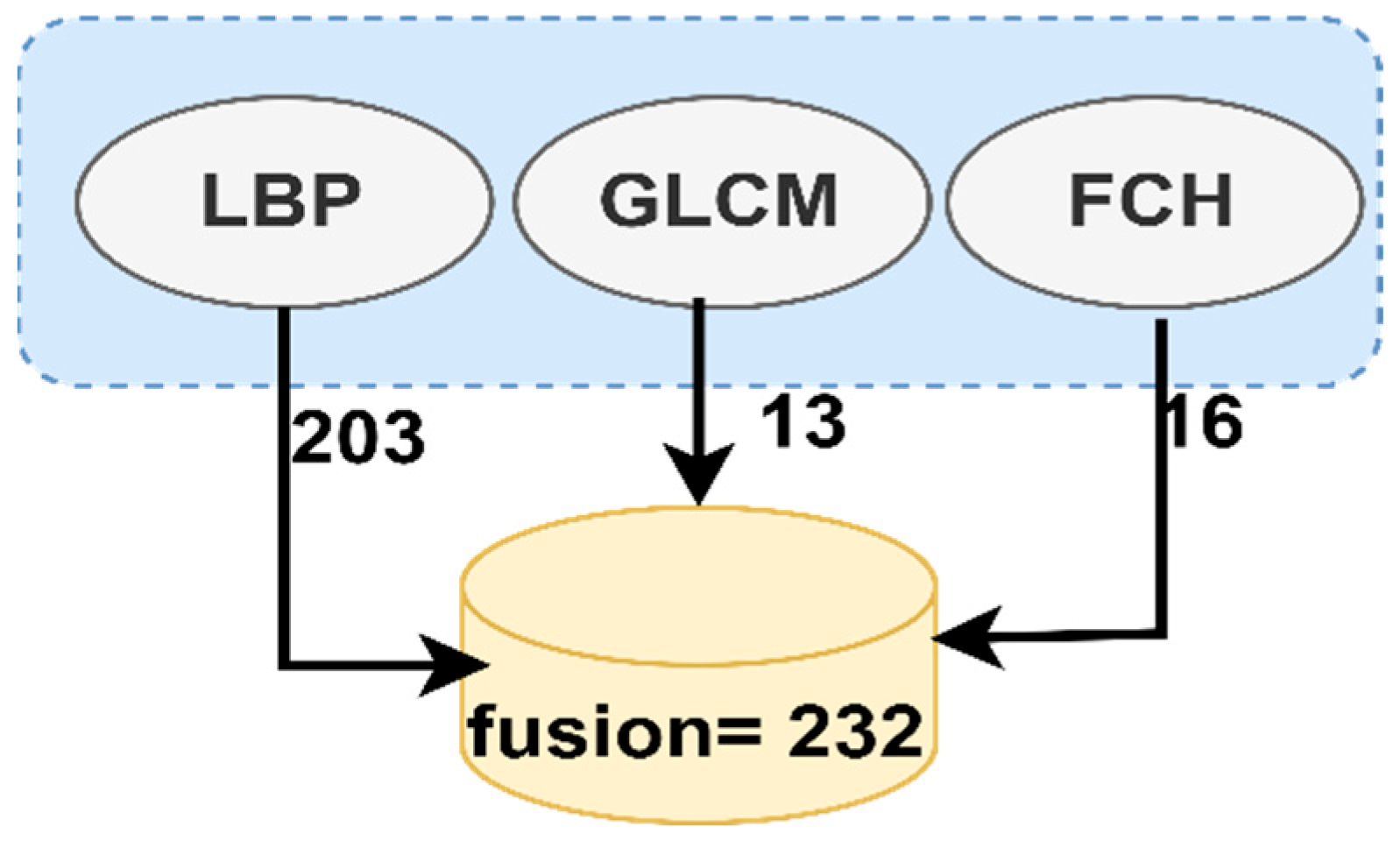
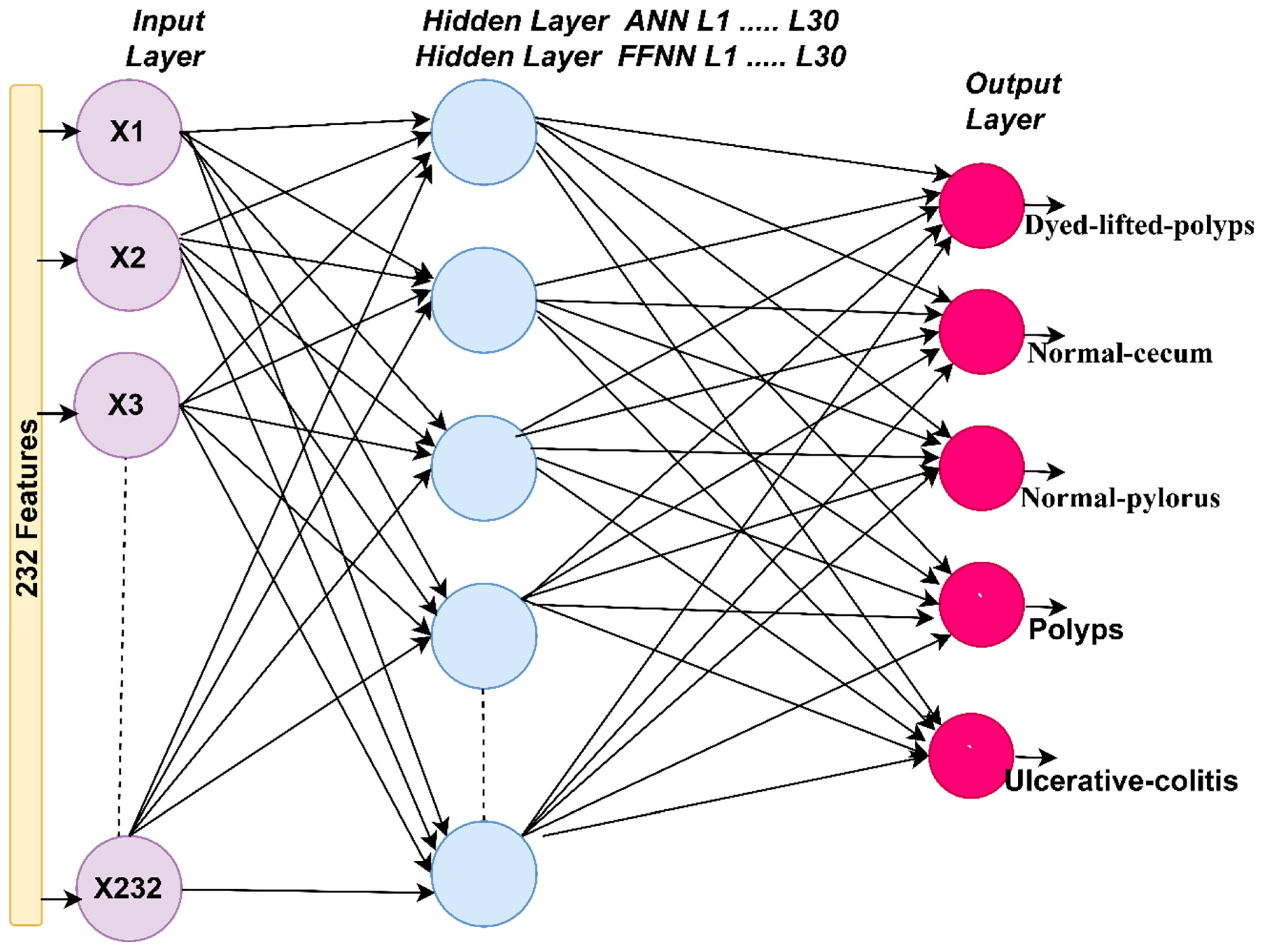
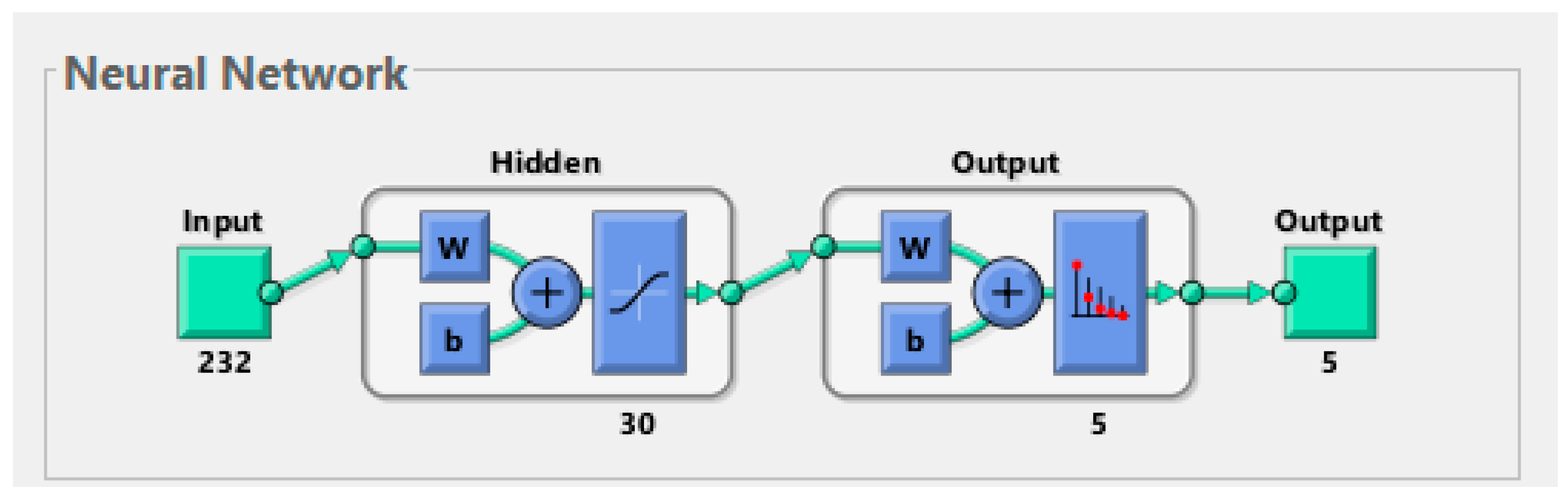
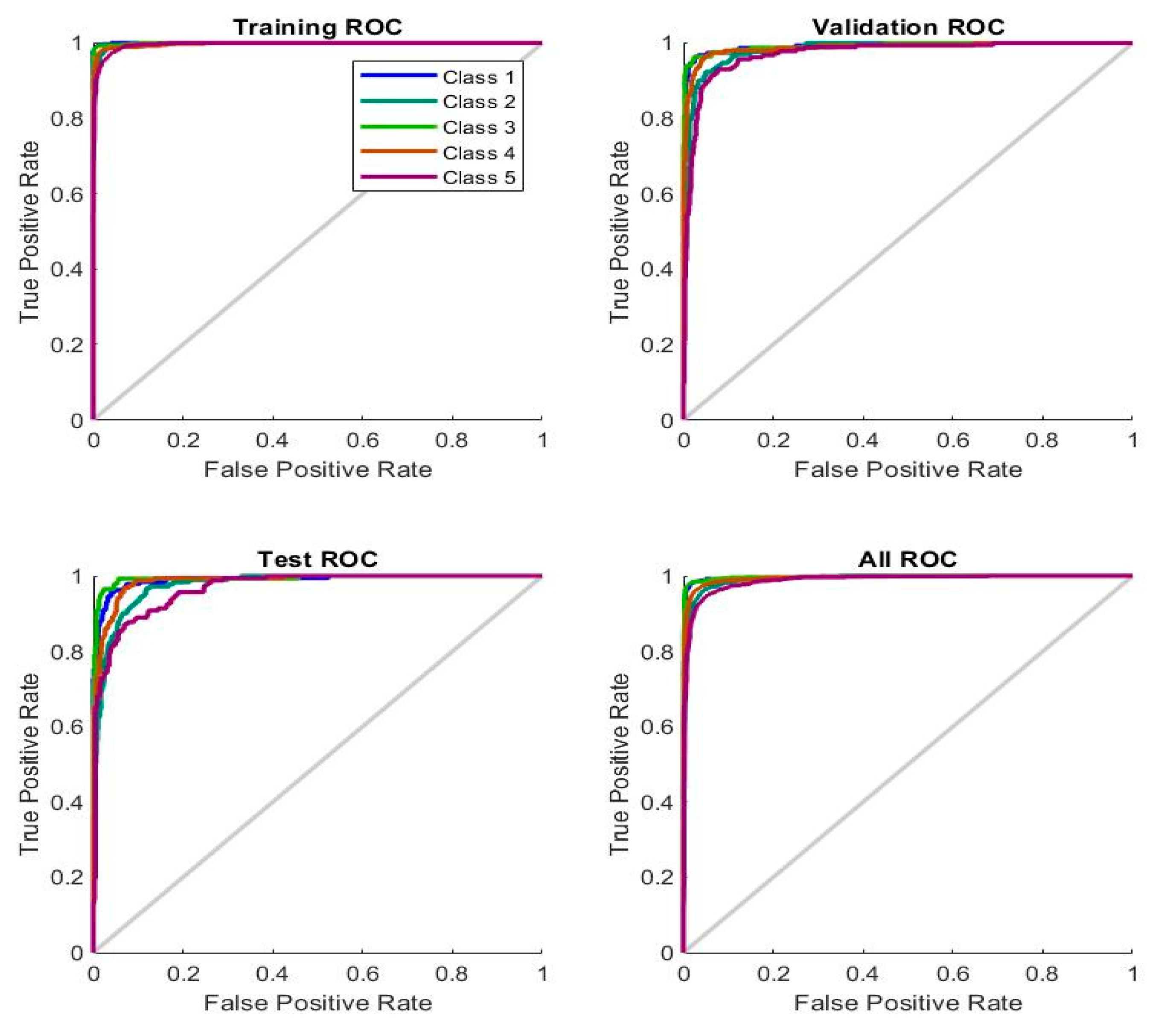
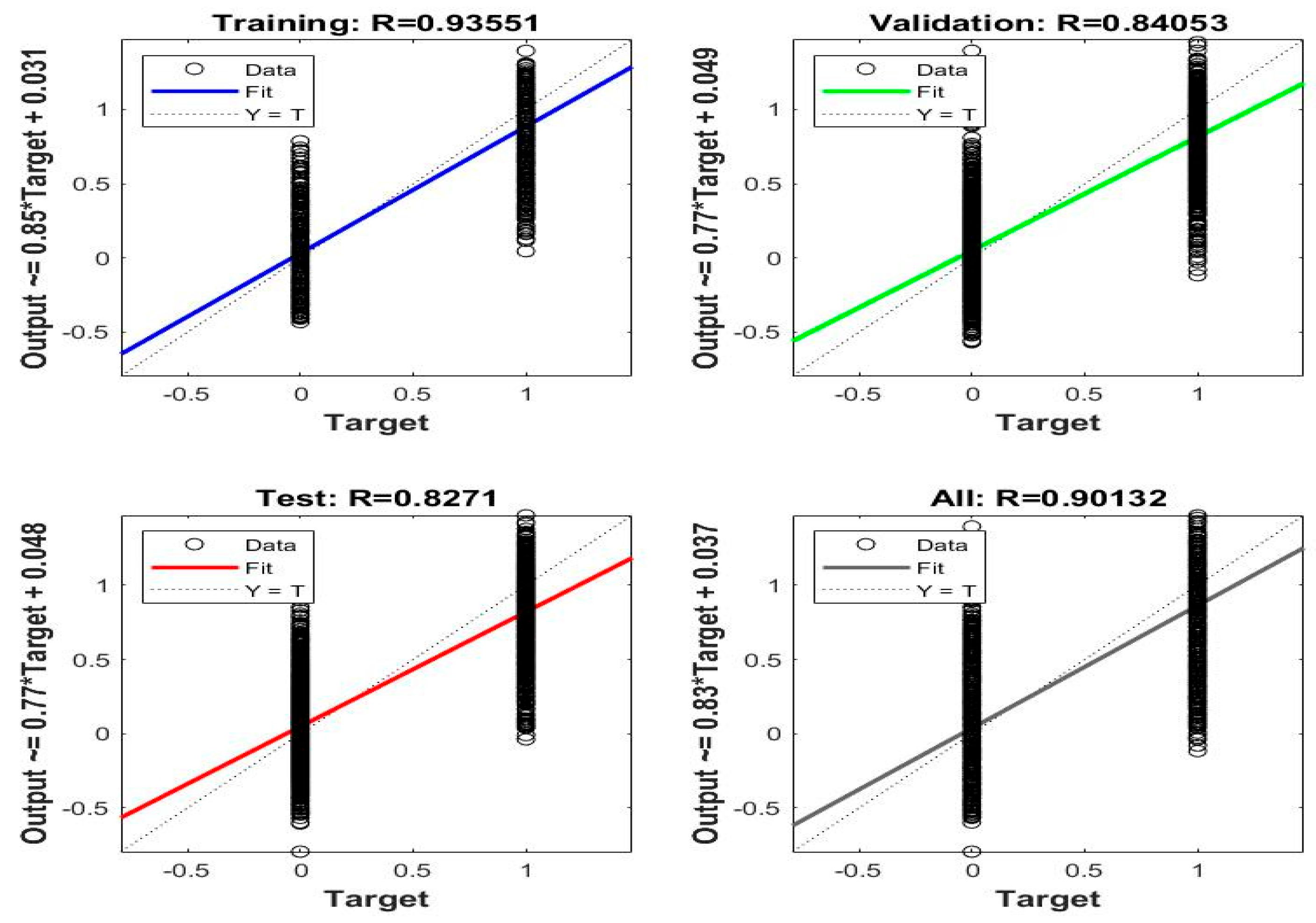
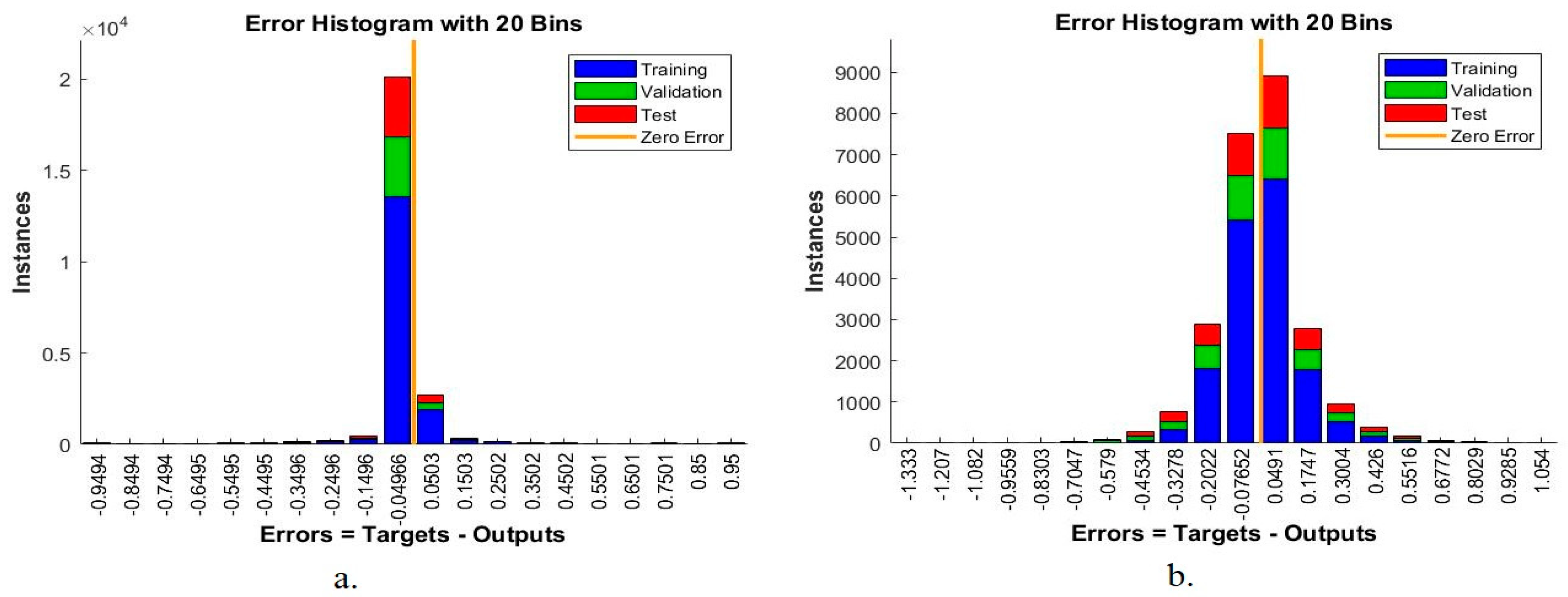
This section presents the evaluation results of hybrid feature techniques between CNN models (GoogLeNet and AlexNet) and features extracted by traditional algorithms (LBP, GLCM and FCH); after fusion, all the features are classified by ANN and FFNN algorithms. These techniques require low-resource computer specifications, execution speed, and high accuracy in diagnosing endoscopic images of the lower GI dataset.
Table 7 summarizes the evaluation results of the performance of the ANN algorithm. When using the hybrid features extracted by CNN models and traditional algorithms (LBP, GLCM and FCH), the systems reached superior results in diagnosing the lower GI dataset. All features are fused into a single feature vector for each image, where each feature vector contains 4328 features fed into the ANN and FFNN classifiers.
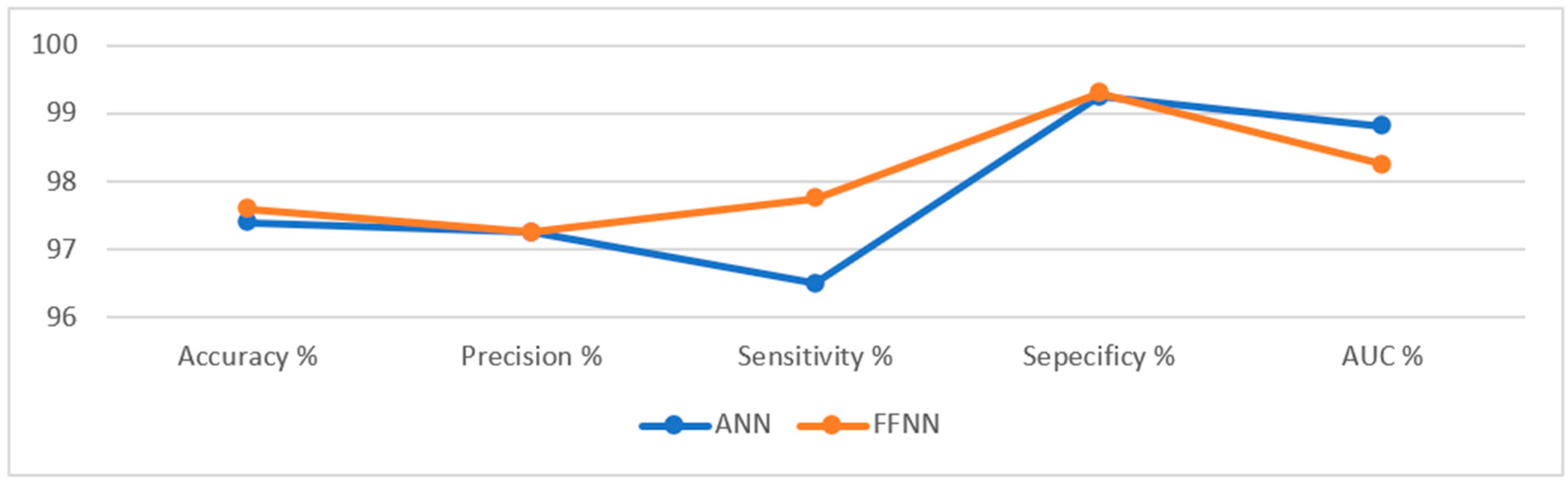
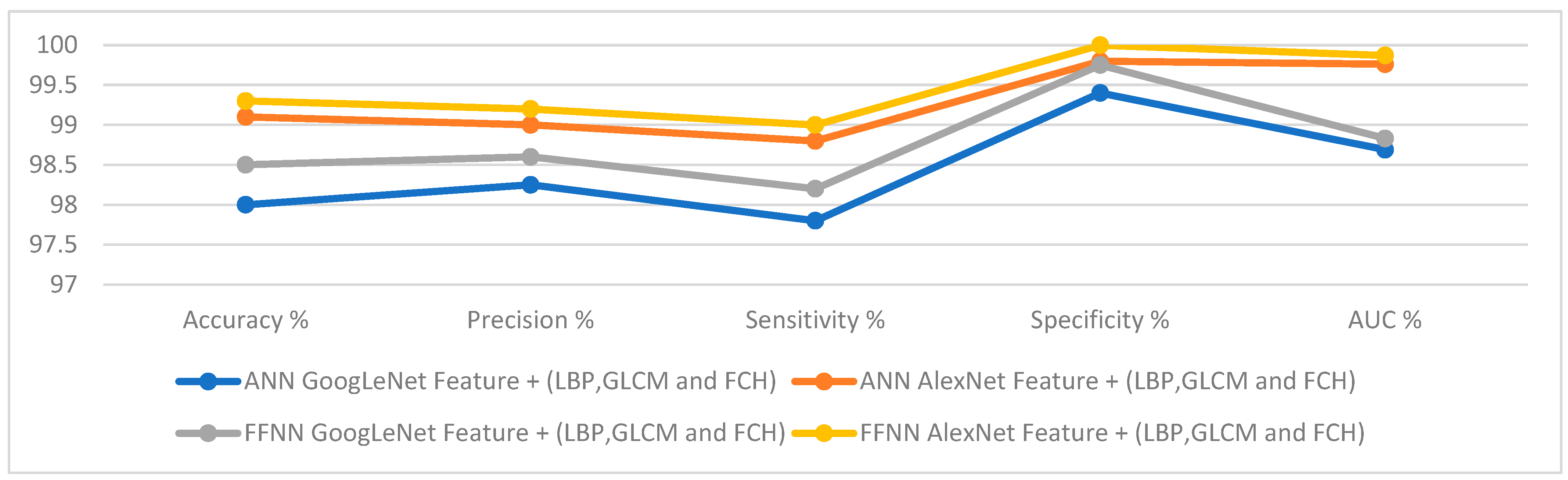
First, when diagnosing by ANN algorithm based on the combined features of GoogLeNet and traditional algorithms (LBP, GLCM and FCH), the system reached accuracy, precision, sensitivity, specificity and AUC of 98%, 98.25%, 97.8%, 99.4% and 98.69%, respectively. When using the hybrid features between AlexNet and traditional algorithms (LBP, GLCM and FCH), the system reached accuracy, precision, sensitivity, specificity and AUC with a percentage of 99.1%, 99%, 98.8%, 99.8% and 99.76%, respectively.
Second, when diagnosing by FFNN algorithm based on the combined features of GoogLeNet and traditional algorithms (LBP, GLCM and FCH), the system reached accuracy, precision, sensitivity, specificity and AUC of 98.8%, 98.6%, 98.2%, 99.75% and 98.83%, respectively. When using the hybrid features between AlexNet and traditional algorithms (LBP, GLCM and FCH), the system reached accuracy, precision, sensitivity, specificity and AUC with a percentage of 99.3%, 99.2%, 99%, 100% and 99.87%, respectively.
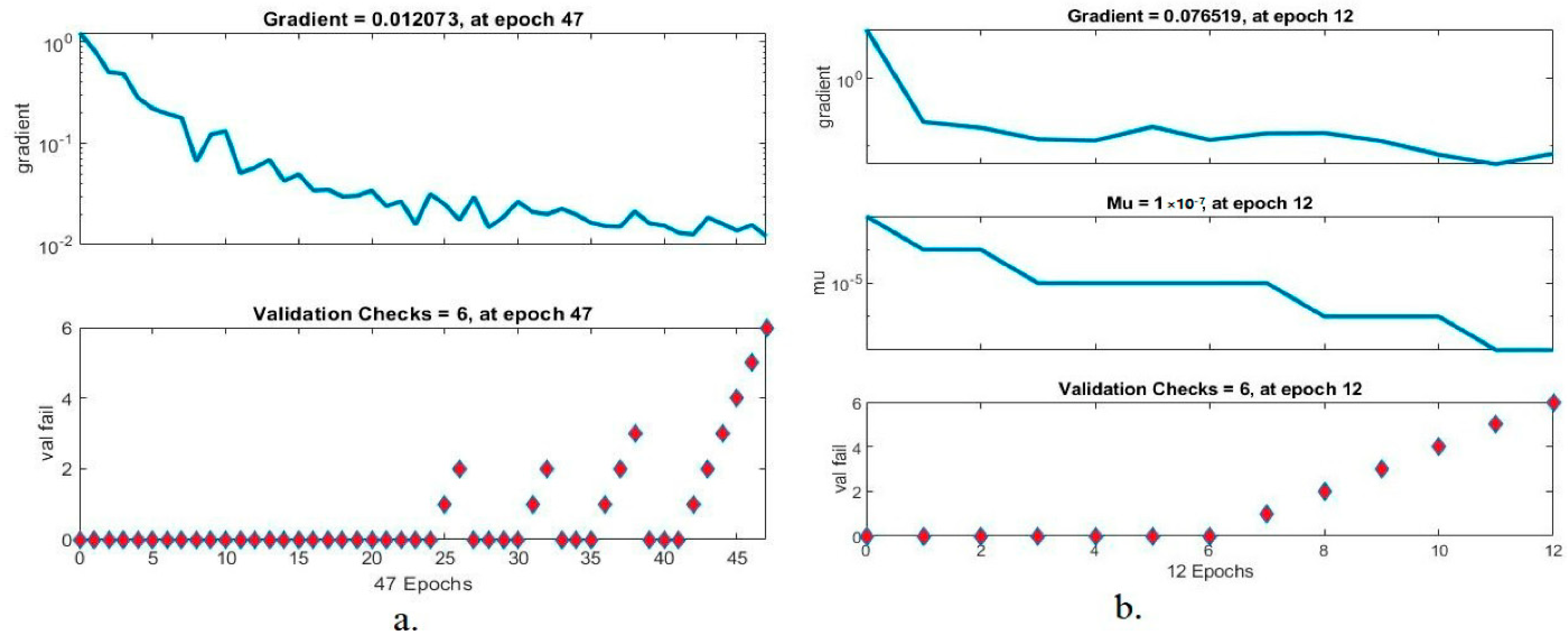
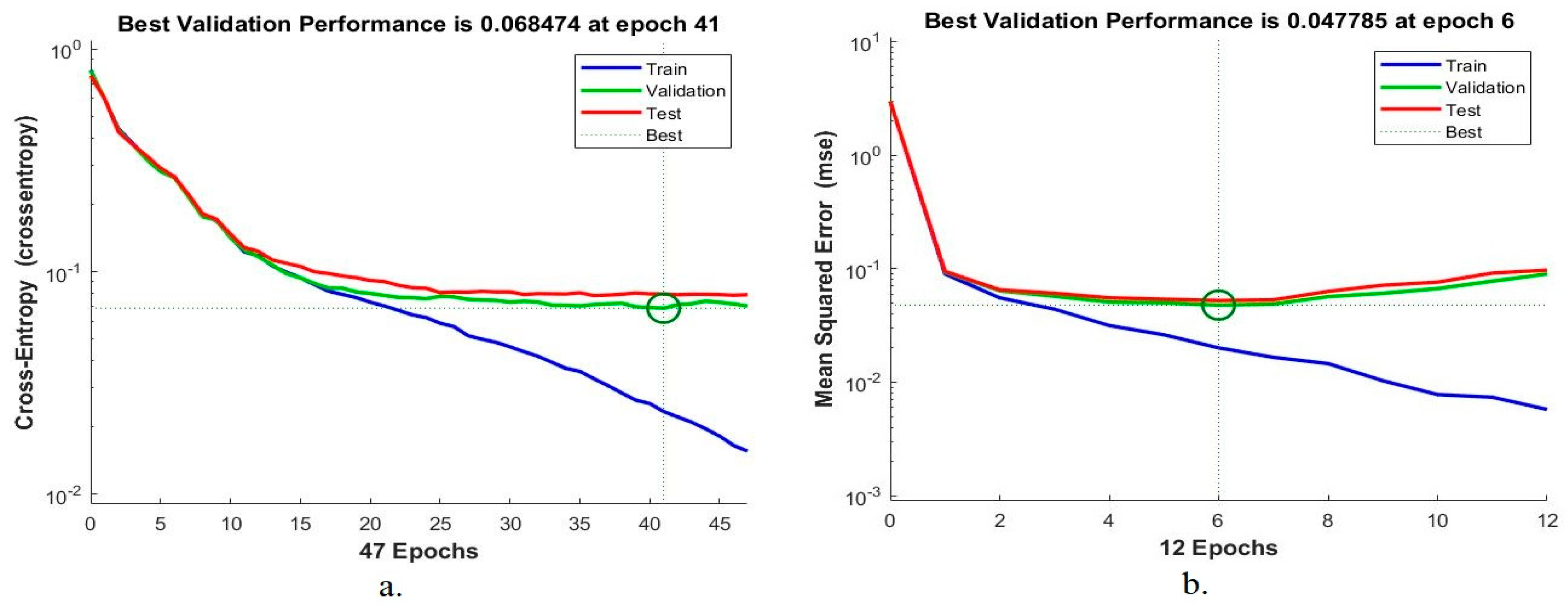
Figure 22 displays the evaluation of the ANN and FFNN algorithms based on the fusion of features between CNN models and traditional algorithms to classify the lower GI dataset accurately.
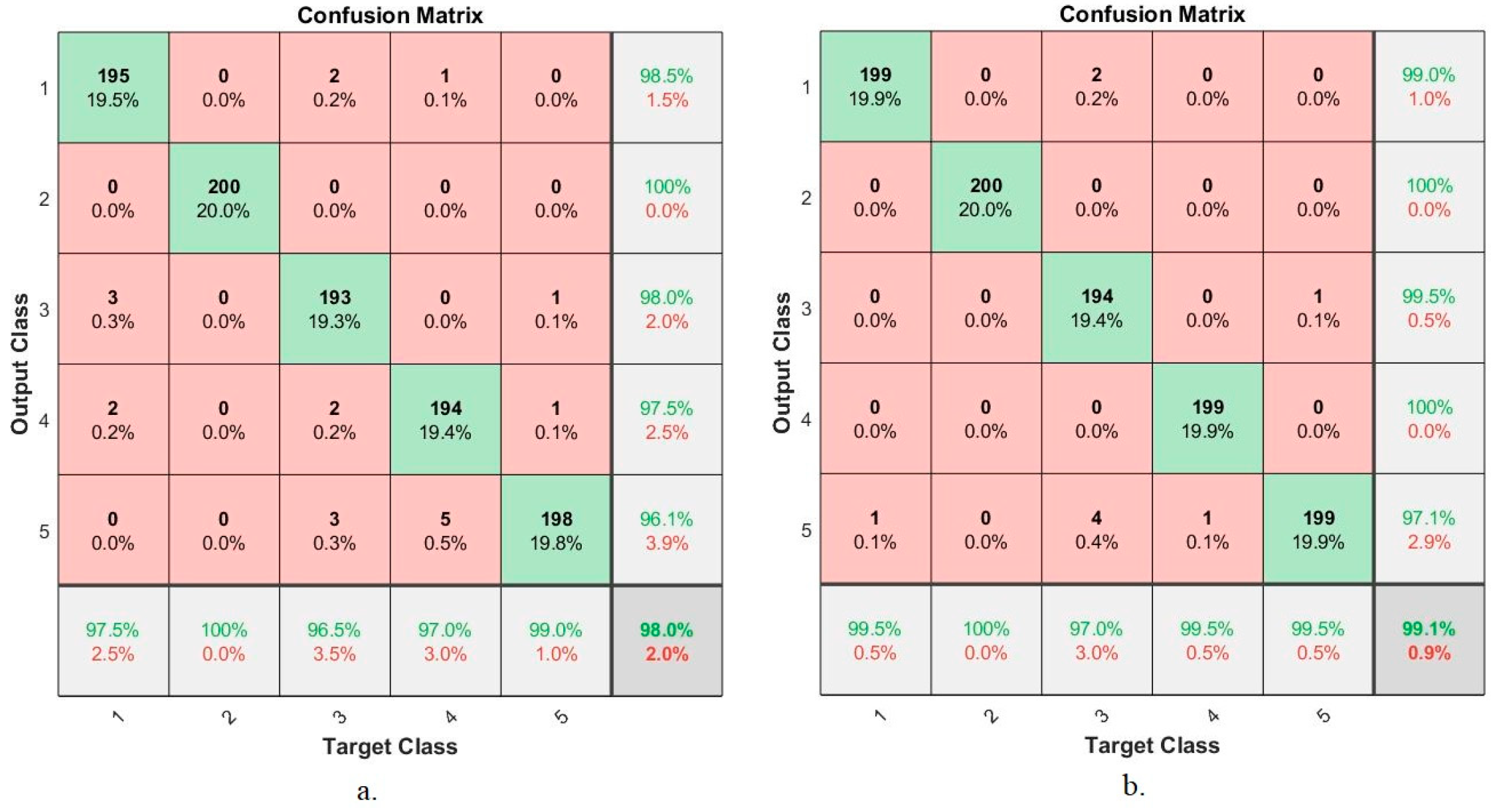
Figure 23 shows the evaluation results of the ANN algorithm based on the hybrid features between CNN models (GoogLeNet and AlexNet) with the features extracted by LBP, GLCM and FCH methods for early diagnosis of lower gastrointestinal diseases. The figure summarizes all samples of the correctly classified and incorrectly classified dataset and displays the diagnostic accuracy of each class (disease) in the dataset. First, when using hybrid features extracted from GoogLeNet and conventional, ANN reached an accuracy of 95.4%, 98.5%, 99.5%, 99.5%, and 100% for diagnosing dyed-lifted-polyps, normal-cecum, normal-pylorus, polyps, and ulcerative-colitis, respectively. Second, when using the hybrid features extracted from AlexNet and conventional, ANN reached an accuracy of 97.2%, 99%, 100%, 99.4%, and 100% for diagnosing dyed-lifted-polyps, normal-cecum, normal-pylorus, polyps, and ulcerative-colitis, respectively.
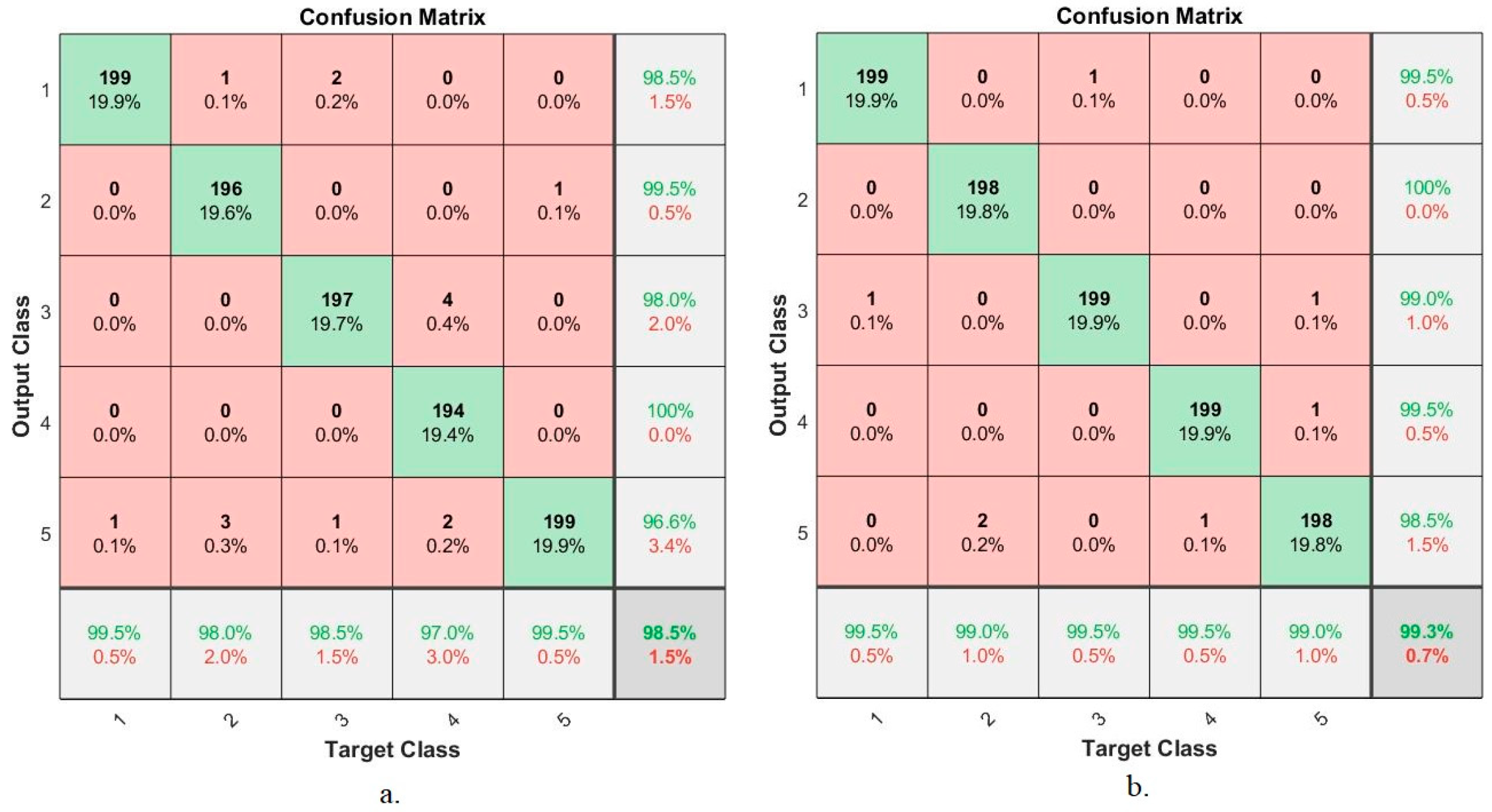
Figure 24 shows the confusion matrix produced by the FFNN algorithm based on the hybrid features between CNN models (GoogLeNet and AlexNet) with the features extracted by LBP, GLCM and FCH methods for early diagnosis of lower gastrointestinal diseases. The figure summarizes all samples of the correctly classified and incorrectly classified dataset and displays the diagnostic accuracy of each class (disease) in the dataset. First, when using hybrid features extracted from GoogLeNet and conventional, FFNN reached an accuracy of 99.5%, 98%, 98.5%, 97%, and 99.5% for diagnosing dyed-lifted-polyps, normal-cecum, normal-pylorus, polyps, and ulcerative-colitis, respectively. Second, when using the hybrid features extracted from AlexNet and conventional, FFNN reached an accuracy of 99.5%, 99%, 99.5%, 99.5%, and 99% for diagnosing dyed-lifted-polyps, normal-cecum, normal-pylorus, polyps, and ulcerative-colitis, respectively.































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}