
Motor Signatures in Digitized Cognitive and Memory Tests Enhances Characterization of Parkinson’s Disease



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
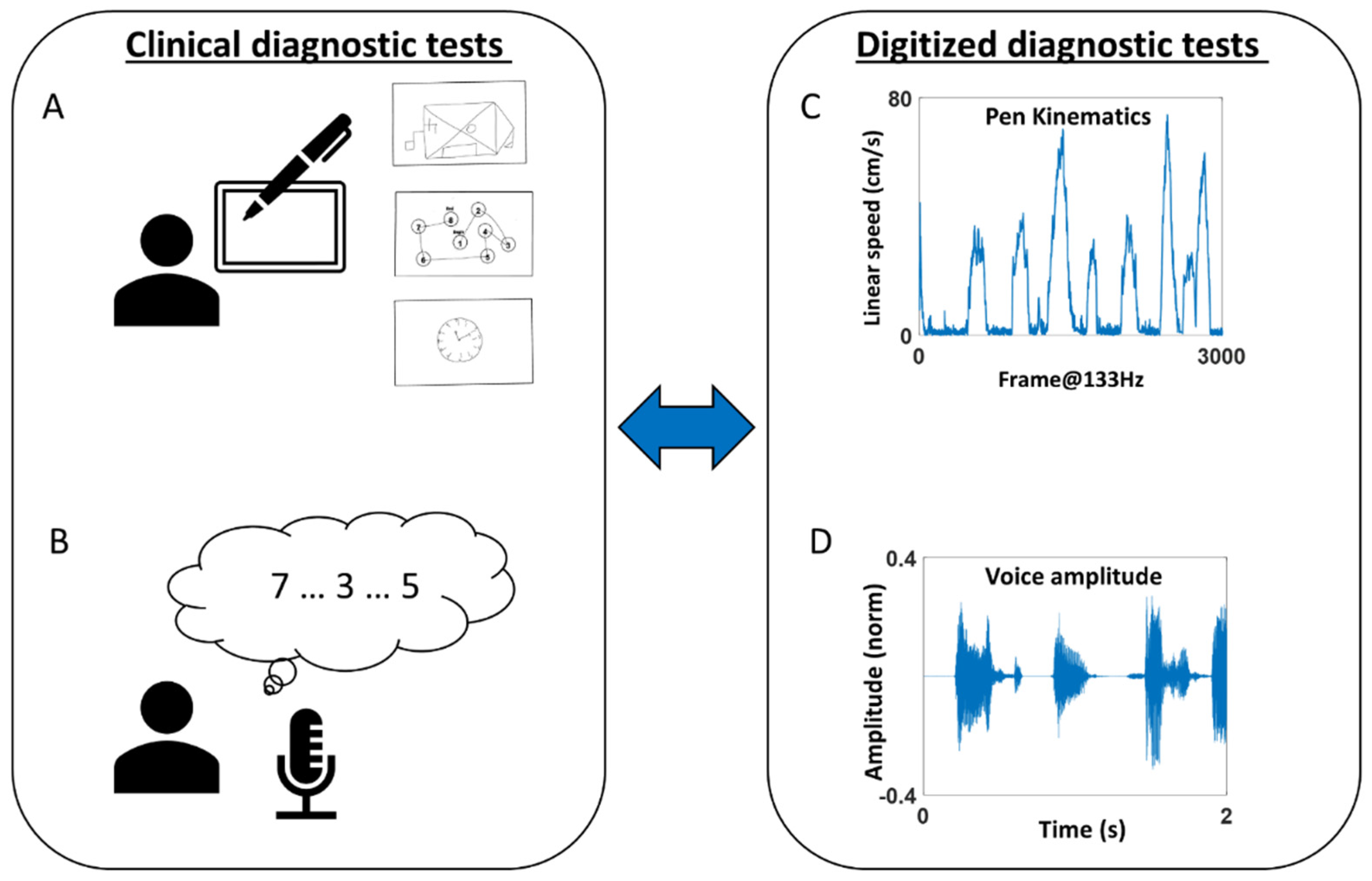
2.2. Experiment Procedure
2.3. Preprocessing Methods
2.4. Data Analysis
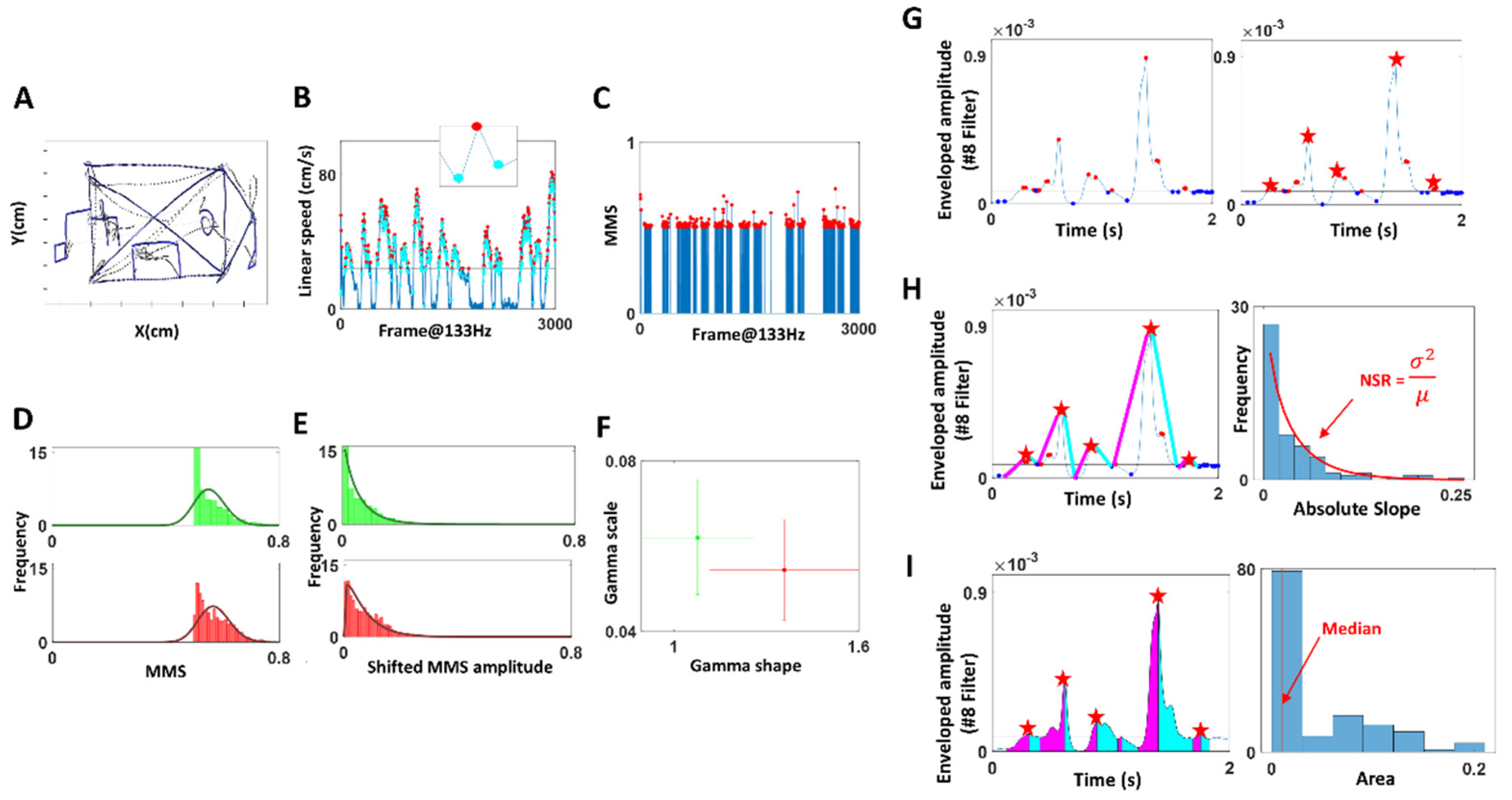
2.4.1. Stochasticity of Pen Movement during Drawing Task
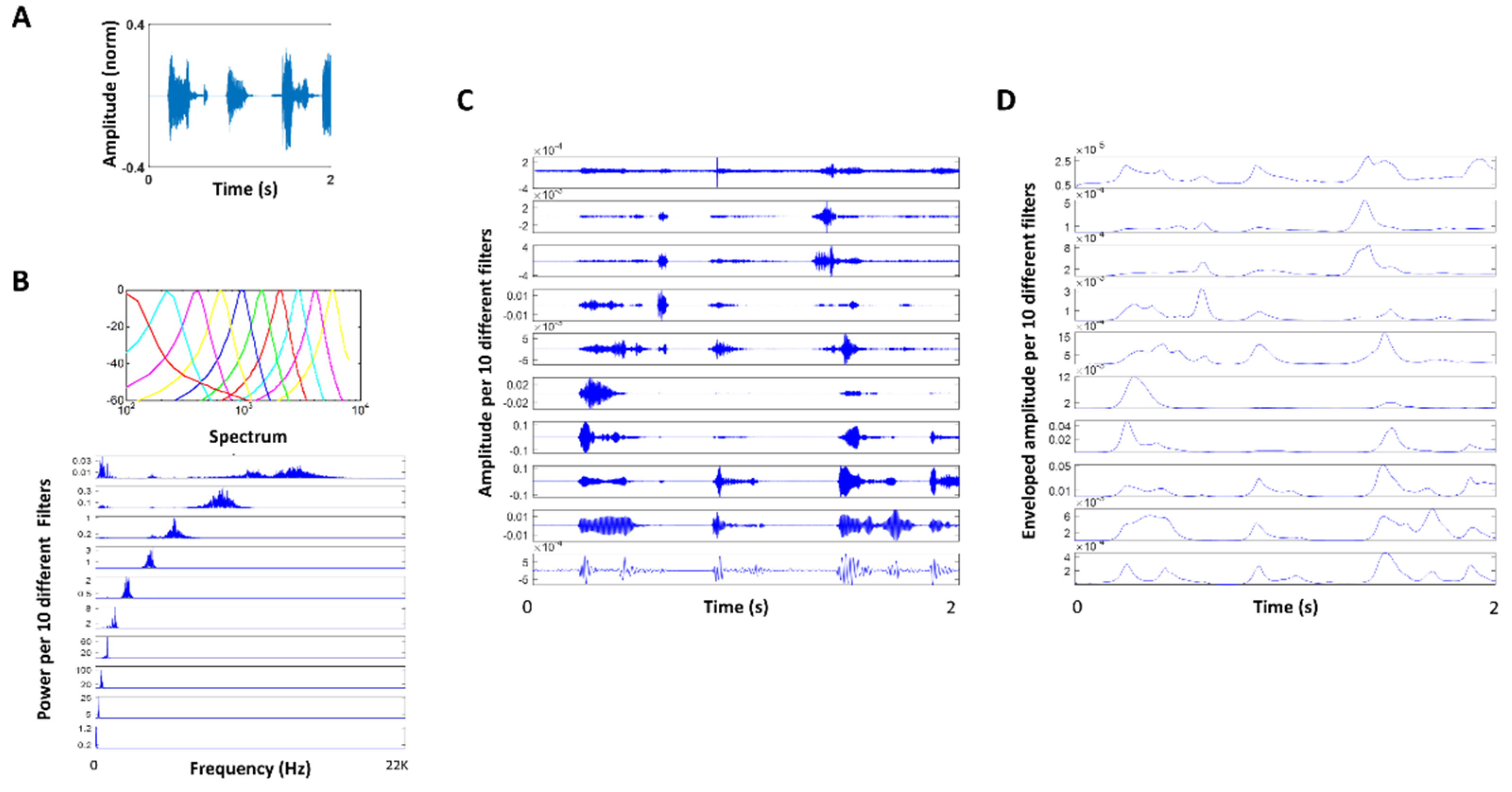
2.4.2. Stochasticity of Attack and Decay Phases of Speech
- (1)
- The data of interest for analyses are not the absolute value of the original waveform, but rather the relative positive deviation obtained from the empirically estimated mean/median of the set from the individual participant. Since we do not average the absolute amplitude values (or temporal values) under an a priori assumed (theoretical) distribution, our data form is a standardized version of the original. They reflect the rate of change of the values in the time series, relative to the empirical mean.
- (2)
- This standardized deviation from the empirical mean, taken point by point, is now a time series that retains the temporal information of when the original peaks occurred, but is normalized between 0–1 to build a standard metric that is independent of anatomical size differences across the population (Equation (1)), impacting the values of the kinematic parameters of interest (e.g., distance traveled, speed, acceleration, in their linear or angular rotation forms, etc. which are scalar positive values with skewed distributions).
- (3)
- The sampling resolution of the sensors allows us to sample thousands of points/windows of unit time in this standardized space, thus providing enough power to make a statement about the person’s biorhythms under consideration.
- (4)
- The empirical estimation then of the distribution of those values per window and the resulting continuous family of probability distributions representing the overall stochastic process defines a standardized parameter space where we represent the empirically estimated parameter values of the person. It is in this sense that the methods are standardized for personalized statistical inference. Any cluster of points (i.e., probability distributions) representing subtypes, self-emerge in these standardized parameter spaces and can be assessed using appropriate similarity (distance) metrics in probability spaces.)
3. Results
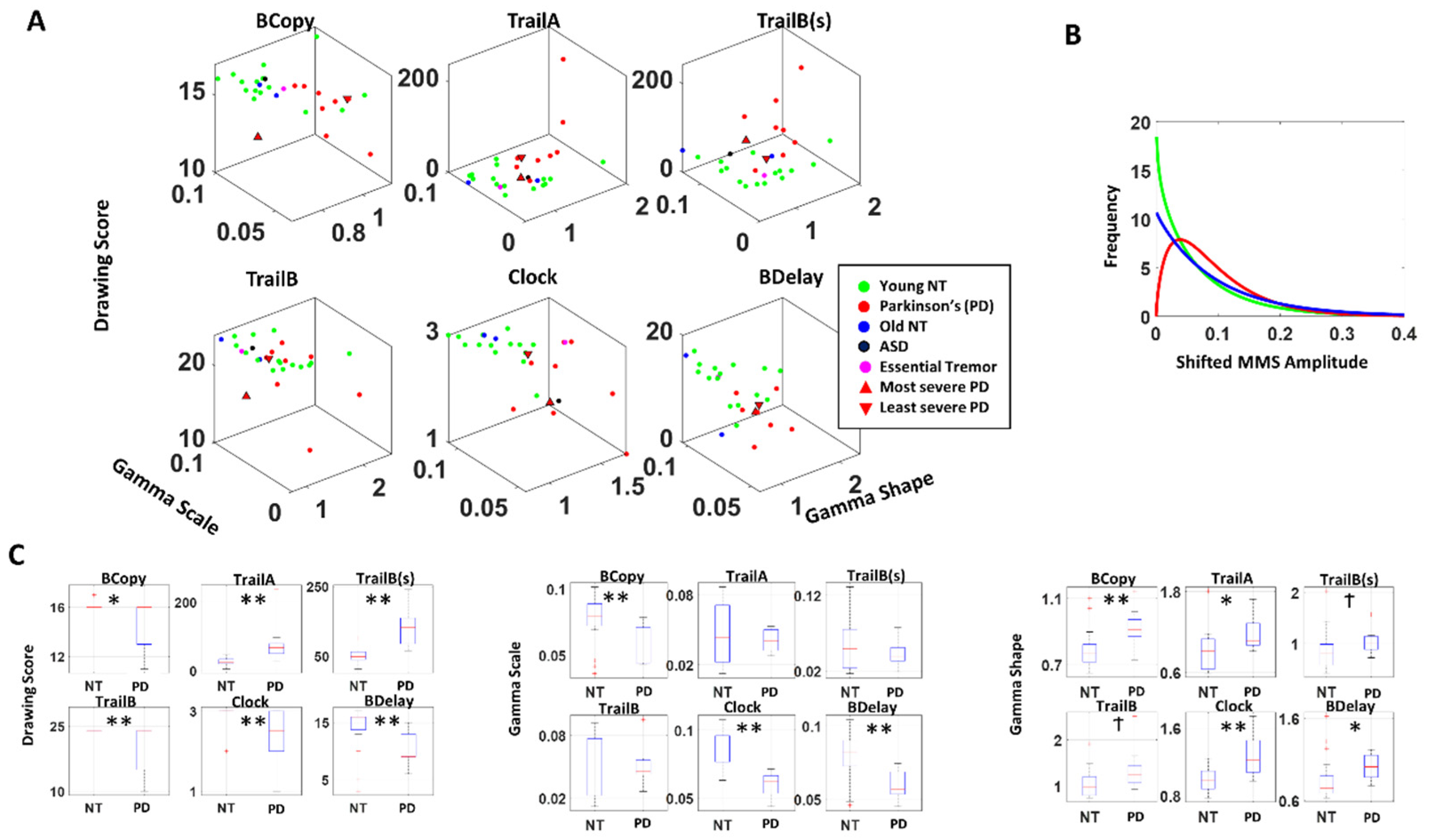
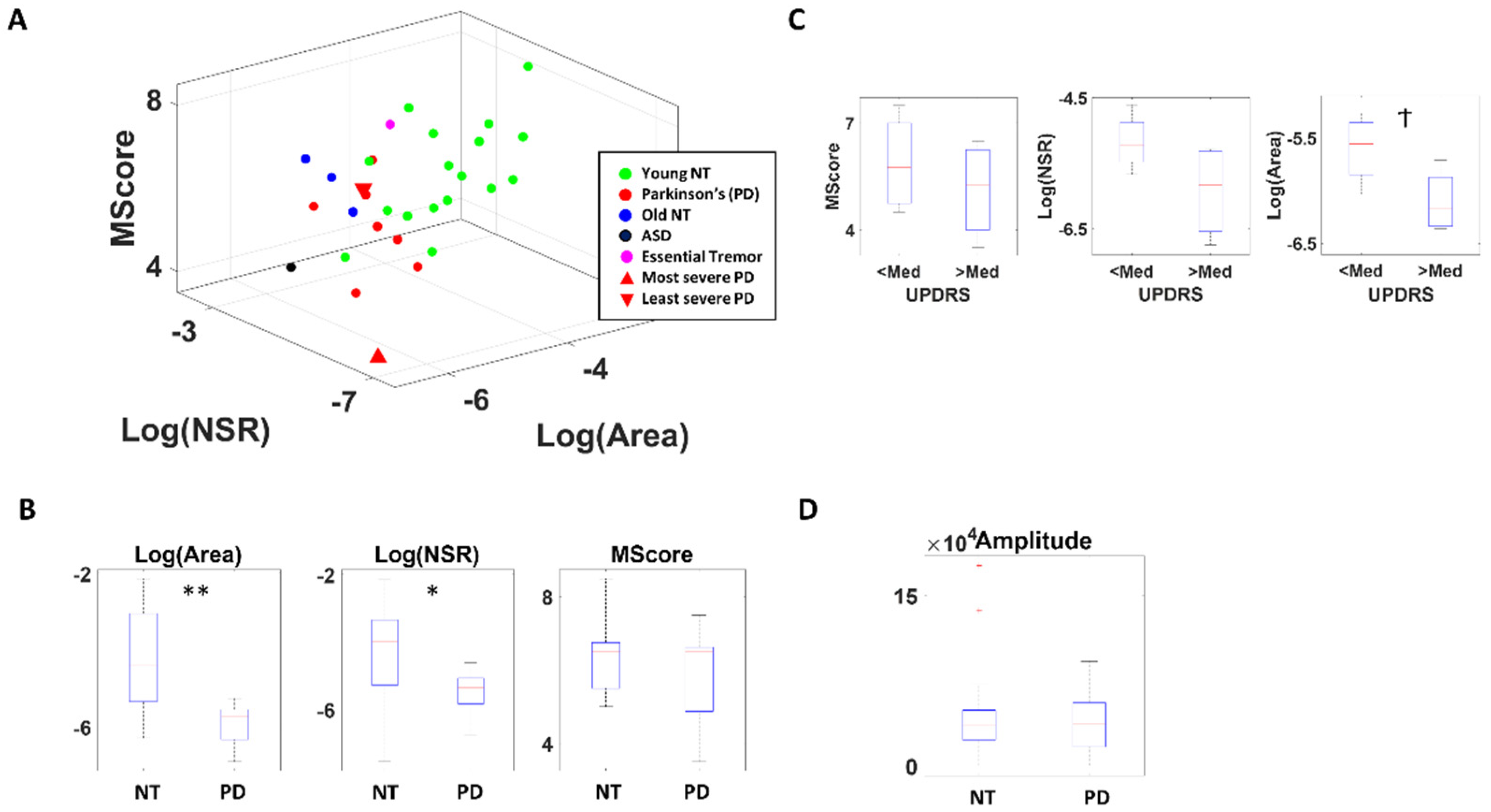
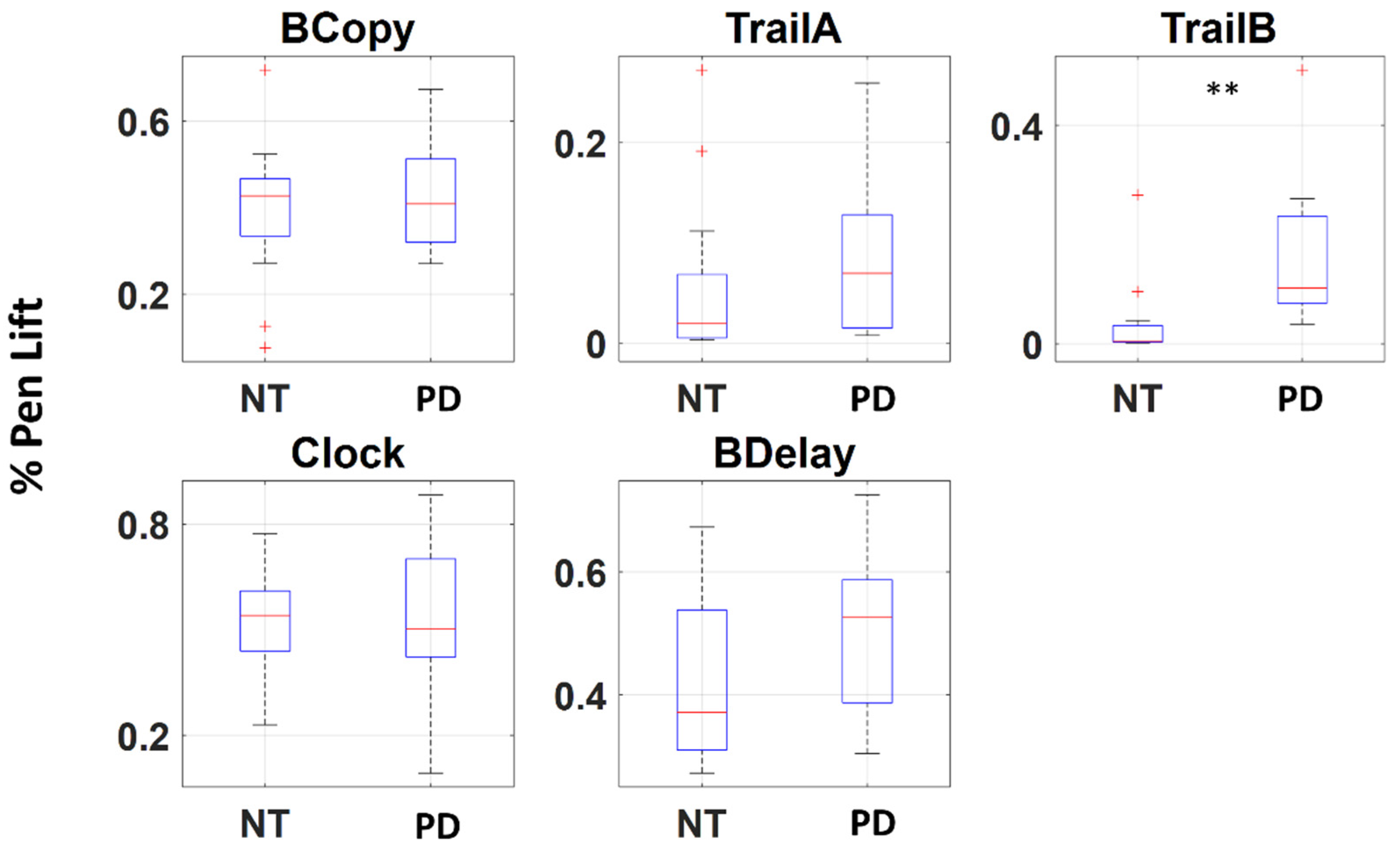
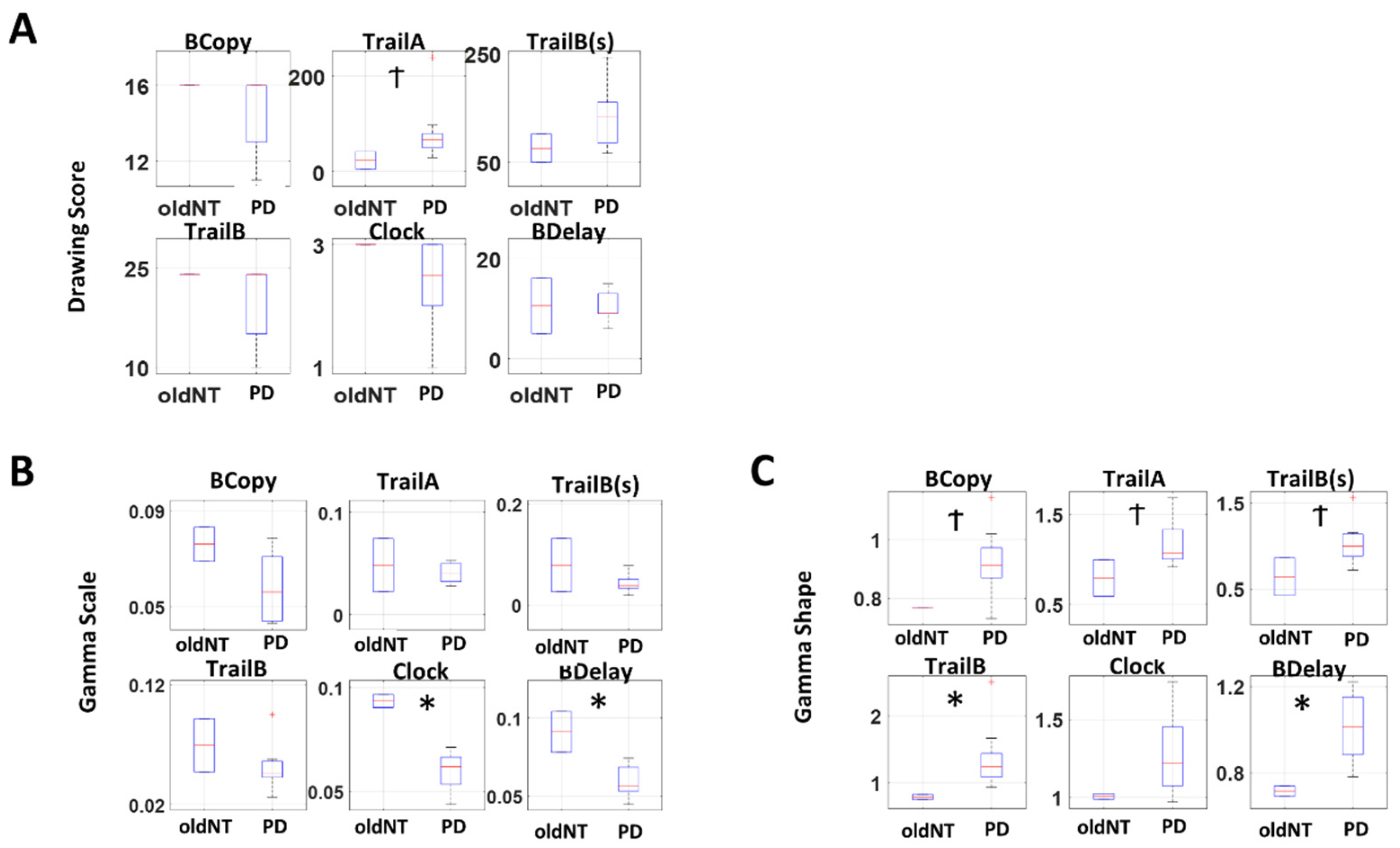
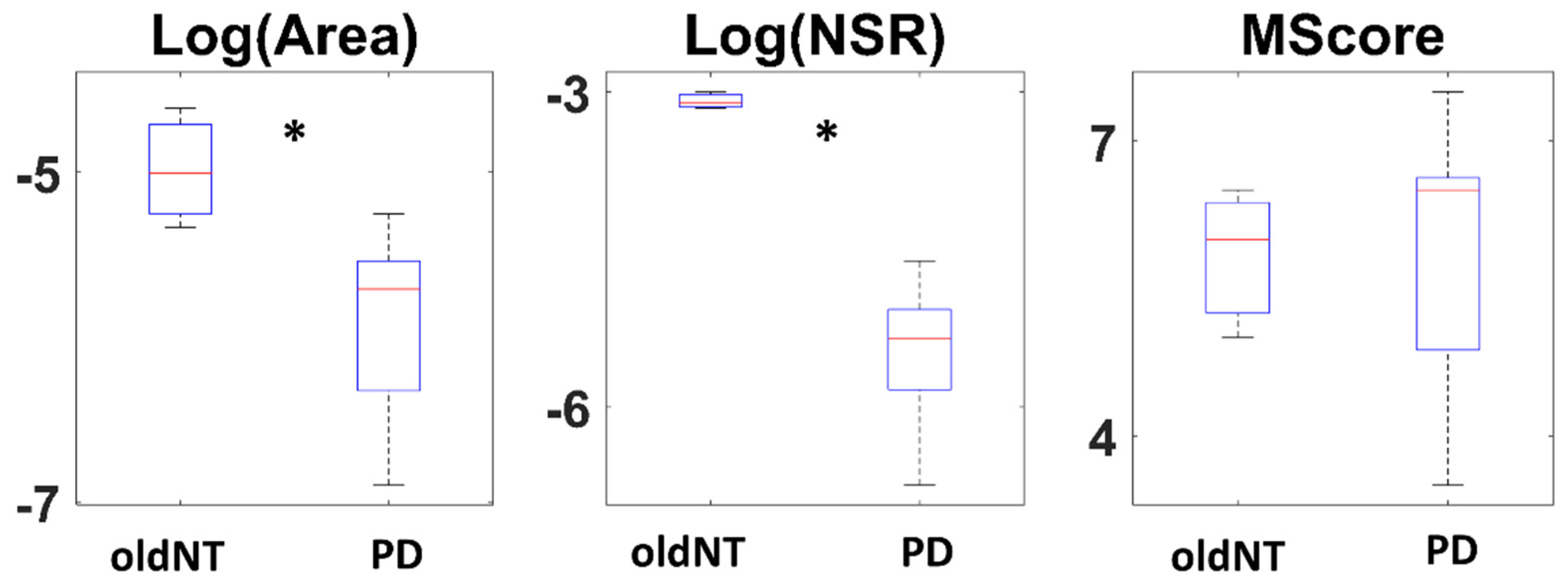
3.1. Patients with PD Show Higher Signal-to-Noise Ratio (SNR) in Their Pen Motion
3.2. Patients with PD Show Lower Change and Higher SNR in Voice Amplitude
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant 1 | Gender | Age | UPDRS | Hoehn and Yahr Scale | Medication (Motor/Non-Motor) 2 | Pen Data | Voice Data |
|---|---|---|---|---|---|---|---|
| PD 1 | M | 51–60 | 6 | 2.5 | Yes/Yes | Yes | Yes |
| PD 2 | F | 61–70 | 44 | 4 | Yes/Yes | Yes | Yes |
| PD 3 | M | 61–70 | 24.5 | 2.5 | Yes/Yes | Yes | Yes |
| PD 4 | M | 61–70 | 19 | 3 | Yes/Yes | Yes | Yes |
| PD 5 | M | 51–60 | 29 | 3 | Yes/Yes | Yes | No |
| PD 6 | F | 61–70 | - | 3 | Yes/No | Yes | Yes |
| PD 7 | M | 61–70 | 16 | 2 | Yes/Yes | Yes | Yes |
| PD 8 | M | 71–80 | 21 | 3 | Yes/No | Yes | Yes |
| PD 9 | F | 71–80 | 27 | 3 | Yes/Yes | Yes | No |
| PD 10 | M | 41–50 | - | 2 | Yes/Yes | Yes | Yes |
| PD 11 | M | 61–70 | 20 | - | - | No | Yes |
| ASD 1 | F | 21–30 | - | - | - | No | Yes |
| ET 1 | M | 31–40 | - | - | - | Yes | Yes |
| Old NT 1 | F | 61–70 | - | - | - | Yes | No |
| Old NT 2 | M | 61–70 | - | - | - | Yes | No |
| Old NT 3 | F | 51–60 | - | - | - | No | Yes |
| Old NT 4 | F | 71–80 | - | - | - | No | Yes |
| Old NT 5 | M | 71–80 | - | - | - | No | Yes |
References
- Spasojevic, S.; Ilic, T.V.; Stojkovic, I.; Potkonjak, V.; Rodic, A.; Santos-Victor, J. Quantitative Assessment of the Arm/Hand Movements in Parkinson’s Disease Using a Wireless Armband Device. Front. Neurol. 2017, 8, 388. [Google Scholar] [CrossRef] [PubMed]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Schwarz, M.; Winkler, J.; Storch, A. Wearable sensor-based objective assessment of motor symptoms in Parkinson’s disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.J.; Chen, J.A.; Little, M.A. Machine learning for large-scale wearable sensor data in Parkinson’s disease: Concepts, promises, pitfalls, and futures. Mov. Disord. 2016, 31, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.B.; Heilman, K.M.; Poizner, H. Impaired endogenously evoked automated reaching in Parkinson’s disease. J. Neurosci. 2011, 31, 17848–17863. [Google Scholar] [CrossRef]
- Torres, E.B. The rates of change of the stochastic trajectories of acceleration variability are a good predictor of normal aging and of the stage of Parkinson’s disease. Front. Integr. Neurosci. 2013, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.B.; Cole, J.; Poizner, H. Motor output variability, deafferentation, and putative deficits in kinesthetic reafference in Parkinson’s disease. Front. Hum. Neurosci. 2014, 8, 823. [Google Scholar] [CrossRef]
- Van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Ryu, J.; Vero, J.; Dobkin, R.D.; Torres, E.B. Dynamic Digital Biomarkers of Motor and Cognitive Function in Parkinson’s Disease. J. Vis. Exp. 2019, 149, e59827. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Torres, E.B.; Isenhower, R.W.; Nguyen, J.; Whyatt, C.; Nurnberger, J.I.; Jose, J.V.; Silverstein, S.M.; Papathomas, T.V.; Sage, J.; Cole, J. Toward Precision Psychiatry: Statistical Platform for the Personalized Characterization of Natural Behaviors. Front. Neurol. 2016, 7, 8. [Google Scholar] [CrossRef]
- Torres, E.B.; Vero, J.; Rai, R. Statistical Platform for Individualized Behavioral Analyses Using Biophysical Micro-Movement Spikes. Sensors 2018, 18, 1025. [Google Scholar] [CrossRef]
- Possin, K.L.; Laluz, V.R.; Alcantar, O.Z.; Miller, B.L.; Kramer, J.H. Distinct neuroanatomical substrates and cognitive mechanisms of figure copy performance in Alzheimer’s disease and behavioral variant frontotemporal dementia. Neuropsychologia 2011, 49, 43–48. [Google Scholar] [CrossRef]
- Beekly, D.L.; Ramos, E.M.; Lee, W.W.; Deitrich, W.D.; Jacka, M.E.; Wu, J.; Hubbard, J.L.; Koepsell, T.D.; Morris, J.C.; Kukull, W.A. The National Alzheimer’s Coordinating Center (NACC) database: The uniform data set. Alzheimer Dis. Assoc. Disord. 2007, 21, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.D.; Robinson, K.; Holdsworth, J.; McKeown, D.; Zhang, C.; Allerhand, M. Complex sounds and auditory images. In Auditory Physiology and Perception; Elsevier: Amsterdam, The Netherlands, 1992; pp. 429–446. [Google Scholar]
- Slaney, M. Auditory Toolbox; Technical Report; Interval Research Corporation: Palo Alto, CA, USA, 1998. [Google Scholar]
- Lartillot, O.; Toiviainen, P. A Matlab toolbox for musical feature extraction from audio. In Proceedings of the International Conference on Digital Audio Effects, Bordeaux, France, 10–15 September 2007; pp. 237–244. [Google Scholar]
- Torres, E.B. Objective Biometric Methods for the Diagnosis and Treatment of Nervous System Disorders; Academic Press: London, UK, 2018; 568p. [Google Scholar]
- Torres, E.B.; Jose, J.V. Novel Diagnostic Tool to Quantify Signatures of Movement in Subjects with Neurobiological Disorders, Autism and Autism Spectrum Disorders. In US Patent Application; Office of Technology Commercialization, Rutgers, The State University of New Jersey: New Brunswick, NJ, USA, 2012. [Google Scholar]
- Lleonart, J.; Salat, J.; Torres, G.J. Removing allometric effects of body size in morphological analysis. J. Theor. Biol. 2000, 205, 85–93. [Google Scholar] [CrossRef]
- Tanaka, Y.; Nishio, M.; Niimi, S. Vocal acoustic characteristics of patients with Parkinson’s disease. Folia Phoniatr. Logop. 2011, 63, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Vojtech, J.M.; Stepp, C.E. Effects of Age and Parkinson’s Disease on the Relationship between Vocal Fold Abductory Kinematics and Relative Fundamental Frequency. J. Voice 2022, 3. [Google Scholar] [CrossRef] [PubMed]
- Yuceturk, A.V.; Yilmaz, H.; Egrilmez, M.; Karaca, S. Voice analysis and videolaryngostroboscopy in patients with Parkinson’s disease. Eur. Arch. Otorhinolaryngol. 2002, 259, 290–293. [Google Scholar] [CrossRef]
- Laganas, C.; Iakovakis, D.; Hadjidimitriou, S.; Charisis, V.; Dias, S.B.; Bostantzopoulou, S.; Katsarou, Z.; Klingelhoefer, L.; Reichmann, H.; Trivedi, D.; et al. Parkinson’s Disease Detection Based on Running Speech Data from Phone Calls. IEEE Trans. Biomed. Eng. 2022, 69, 1573–1584. [Google Scholar] [CrossRef]
- Yu, Q.; Zou, X.; Quan, F.; Dong, Z.; Yin, H.; Liu, J.; Zuo, H.; Xu, J.; Han, Y.; Zou, D.; et al. Parkinson’s disease patients with freezing of gait have more severe voice impairment than non-freezers during “ON state”. J. Neural Transm. 2022, 129, 277–286. [Google Scholar] [CrossRef]
- Yanovich, P.; Isenhower, R.W.; Sage, J.; Torres, E.B. Spatial-orientation priming impedes rather than facilitates the spontaneous control of hand-retraction speeds in patients with Parkinson’s disease. PLoS ONE 2013, 8, e66757. [Google Scholar] [CrossRef]
- Adamovich, S.V.; Berkinblit, M.B.; Hening, W.; Sage, J.; Poizner, H. The interaction of visual and proprioceptive inputs in pointing to actual and remembered targets in Parkinson’s disease. Neuroscience 2001, 104, 1027–1041. [Google Scholar] [CrossRef]
- Poizner, H.; Feldman, A.G.; Levin, M.F.; Berkinblit, M.B.; Hening, W.A.; Patel, A.; Adamovich, S.V. The timing of arm-trunk coordination is deficient and vision-dependent in Parkinson’s patients during reaching movements. Exp. Brain Res. 2000, 133, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Poizner, H.; Fookson, O.I.; Berkinblit, M.B.; Hening, W.; Feldman, G.; Adamovich, S. Pointing to remembered targets in 3-D space in Parkinson’s disease. Mot. Control 1998, 2, 251–277. [Google Scholar] [CrossRef] [PubMed]
- Redgrave, P.; Rodriguez, M.; Smith, Y.; Rodriguez-Oroz, M.C.; Lehericy, S.; Bergman, H.; Agid, Y.; DeLong, M.R.; Obeso, J.A. Goal-directed and habitual control in the basal ganglia: Implications for Parkinson’s disease. Nat. Rev. Neurosci. 2010, 11, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.B. Methods for the Diagnosis and Treatment of Neurological Disorders. U.S. Patent 10,176,299, 6 December 2018. [Google Scholar]
- Torres, E.B. Rethinking the Study of Volition for Clinical Use. Adv. Exp. Med. Biol. 2016, 957, 229–254. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.B.; Donnellan, A.M. Autism: The Movement Perspective; Frontiers Media SA: Lausanne, Switzerland, 2015. [Google Scholar]
- Nguyen, J.; Majmudar, U.; Papathomas, T.V.; Silverstein, S.M.; Torres, E.B. Schizophrenia: The micro-movements perspective. Neuropsychologia 2016, 85, 310–326. [Google Scholar] [CrossRef]
- Ryu, J.; Torres, E. The Autonomic Nervous System Differentiates between Levels of Motor Intent and End Effector. J. Pers. Med. 2020, 10, 76. [Google Scholar] [CrossRef]





| Parameter | Drawing | yNT 1 vs. PD | oldNT 2 vs. PD | ||
|---|---|---|---|---|---|
| Chi (1.25) | p-Value | Chi (1.10) | p-Value | ||
| Drawing Score | BCopy | 5.80 | 0.02 * | 0.72 | 0.40 |
| Trail A | 14.95 | 0.00 ** | 2.95 | 0.09 | |
| Trail B(s) | 16.54 | 0.00 ** | 2.26 | 0.13 | |
| Trail B | 7.63 | 0.01 ** | 1.05 | 0.31 | |
| Clock | 6.95 | 0.01 ** | 1.50 | 0.22 | |
| BDelay | 7.77 | 0.01 ** | 0.00 | 1.00 | |
| Gamma shape | BCopy | 7.08 | 0.01 ** | 2.95 | 0.09 |
| Trail A | 4.66 | 0.03 * | 2.95 | 0.09 | |
| Trail B(s) | 3.45 | 0.06 | 2.95 | 0.09 | |
| Trail B | 3.64 | 0.06 | 4.62 | 0.03 * | |
| Clock | 7.80 | 0.01 ** | 2.26 | 0.13 | |
| BDelay | 4.31 | 0.04 * | 4.50 | 0.03 * | |
| Gamma scale | BCopy | 6.82 | 0.01 ** | 2.26 | 0.13 |
| Trail A | 0.00 | 1.00 | 0.00 | 1.00 | |
| Trail B(s) | 0.06 | 0.80 | 0.05 | 0.83 | |
| Trail B | 0.57 | 0.45 | 1.15 | 0.28 | |
| Clock | 15.21 | 0.00 ** | 4.62 | 0.03 * | |
| BDelay | 8.63 | 0.00 ** | 4.50 | 0.03 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, J.; Torres, E.B. Motor Signatures in Digitized Cognitive and Memory Tests Enhances Characterization of Parkinson’s Disease. Sensors 2022, 22, 4434. https://doi.org/10.3390/s22124434
Ryu J, Torres EB. Motor Signatures in Digitized Cognitive and Memory Tests Enhances Characterization of Parkinson’s Disease. Sensors. 2022; 22(12):4434. https://doi.org/10.3390/s22124434
Chicago/Turabian StyleRyu, Jihye, and Elizabeth B. Torres. 2022. "Motor Signatures in Digitized Cognitive and Memory Tests Enhances Characterization of Parkinson’s Disease" Sensors 22, no. 12: 4434. https://doi.org/10.3390/s22124434
APA StyleRyu, J., & Torres, E. B. (2022). Motor Signatures in Digitized Cognitive and Memory Tests Enhances Characterization of Parkinson’s Disease. Sensors, 22(12), 4434. https://doi.org/10.3390/s22124434