1. Introduction
Knee extensors play an essential role in human mobility [
1]. In fact, knee extensors are crucial for activities of daily living (ADL), such as climbing stairs [
2], standing up from a chair [
3]; and play a fundamental role in many sports, such as volleyball [
4], cycling, and basketball [
5]. As with every muscle, the knee extensors need continuous training to maintain their strength. However, since they are activated only during very specific movements, it is difficult to estimate the training effect of ADL without any feedback devices. According to the U.S. National Health and Nutrition Examination Survey (NHANES), 45% of US adults self-reported that their training is sufficient, while less than 5% of them actually met the national physical activity recommendation when measured with quantitative analysis using various sensors [
6]. Therefore, it was evident that quantitative muscle activity measurement during training can be useful to help people achieve their target by avoiding insufficient or excessive training.
In the past few years, the development of wearable measurement systems improved fast because people started paying more attention to their health status and had begun monitoring their own daily activity [
7,
8,
9]. As walking is a universal, very basic activity for humans, it became a very popular baseline for everyday overall training estimation. At the present, many wearable devices, such as wristwatches and ankle bands, can detect the number of steps of a user during walking. However, the number of steps can offer only limited information about the quality of walking, and on the activation of specific muscular groups in the legs. For a more detailed evaluation of the training effect of walking on single muscle groups, gait analysis should be performed using real-time muscular activity data.
In medical settings, muscular activity is usually assessed using surface electromyography (sEMG) [
10,
11,
12]. The clinical usage of sEMG sensors is often referred to as kinesiological sEMG as it involves dynamic recording of muscular activity during intentional movements in functionally relevant tasks characterized by cyclic motion of limb segments such as walking and stepping [
13,
14,
15]. In most gait analysis tests surface myoelectric signals are collected by about 10 sets of electrodes placed in a bipolar configuration connected to a preamplifier fitted a few centimeters away from the contact points. A central board is used to collect the synchronized data from all the sEMG sensors by wire cables or wireless transmission and to transfer the data to the receiving data processing unit. Muscle activity is then calculated from these surface myoelectric data. In more recent studies on gait analysis, optical motion capture systems have also been used for model-based estimation of the muscle activity [
16]. Subjects were fitted with markers on all major joints of lower limbs and walked inside a room equipped with an optical motion measurement system which recorded the motions of all markers. Gait was then reconstructed using a kinematic model of the lower human body, and leg muscle activity was then estimated from the reconstructed gait. Instead of motion capture systems, multiple inertial measurement units (IMUs) have also been used in previous studies on gait analysis [
17] and rehabilitation [
18]. An IMU can measure motion parameters, such as acceleration and angular velocity. To estimate the human lower body link model one IMU must be placed on every link of the lower limbs kinematic chain [
19]. The accuracy of IMU-based systems is comparable to the accuracy of motion capture systems [
20], albeit their usability is higher as they do not require a fitted environment.
However, all these methods for measuring leg muscle activity have severe limitations, which limit their suitability for widespread adoption as muscle activity estimation systems during ADL. sEMG sensors are invasive as they require adequate skin preparation, such as shaving and removing the sebaceous film by alcohol, to ensure good electrode contact; and the signal processing phase is critical to remove noise and interferences which can corrupt the signal and lead to calculation errors [
21]. Optical motion capture systems are expensive and require a specifically fitted room, which severely limits the workspace dimension and the situations in which they can be used. Multiple IMUs acquisition systems also require a long preparation time to fit all sensors in place and can grow very expensive due to the number of units to be used.
For this reason, in a past study, we have developed a system for kinematic model-based leg muscular activity estimation using only one IMU sensor placed on the shank. However, the preliminary results of system testing showed that knee extensors activity estimation using a traditional human lower limb kinematic model was not sufficiently accurate for real-time analysis.
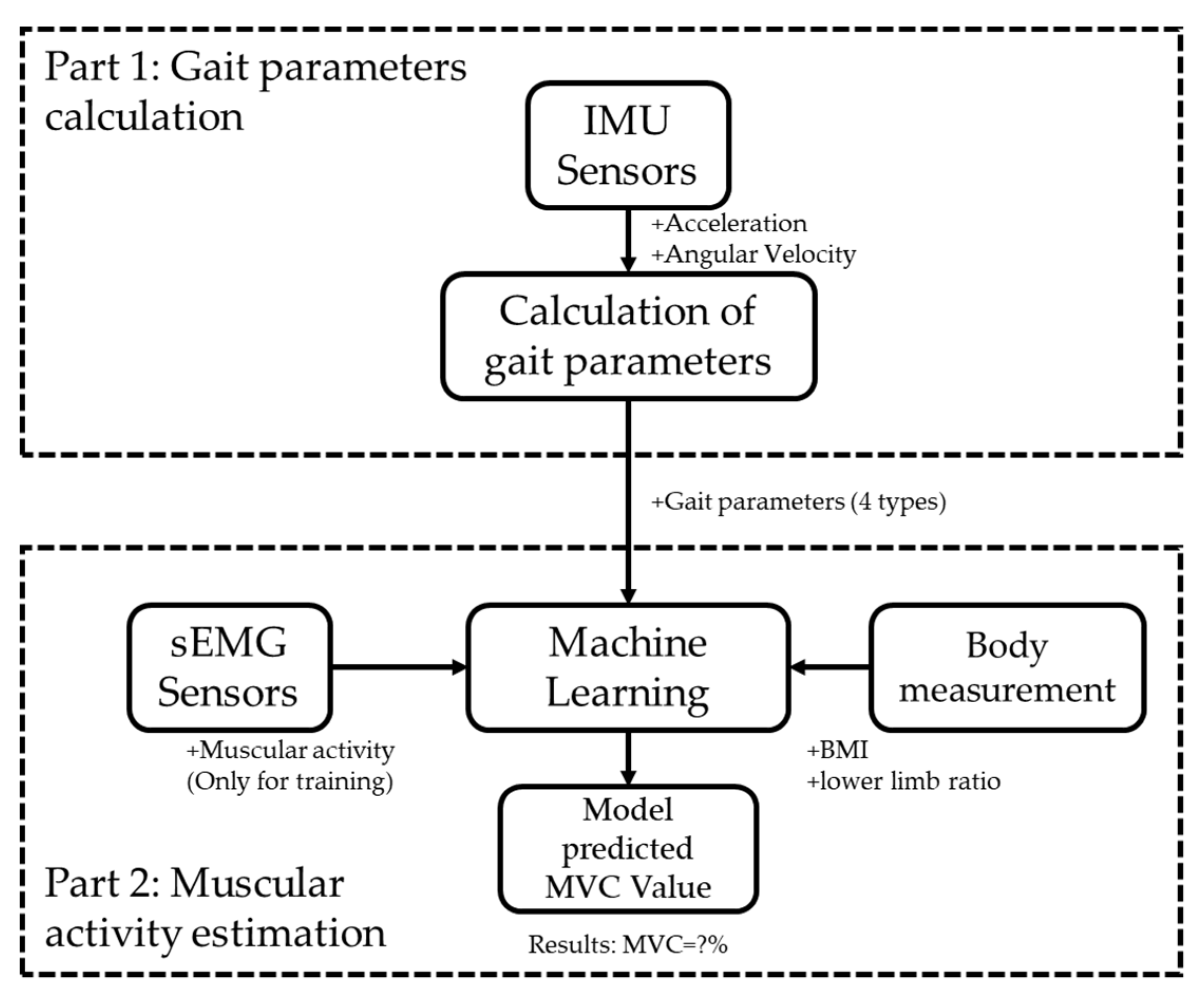
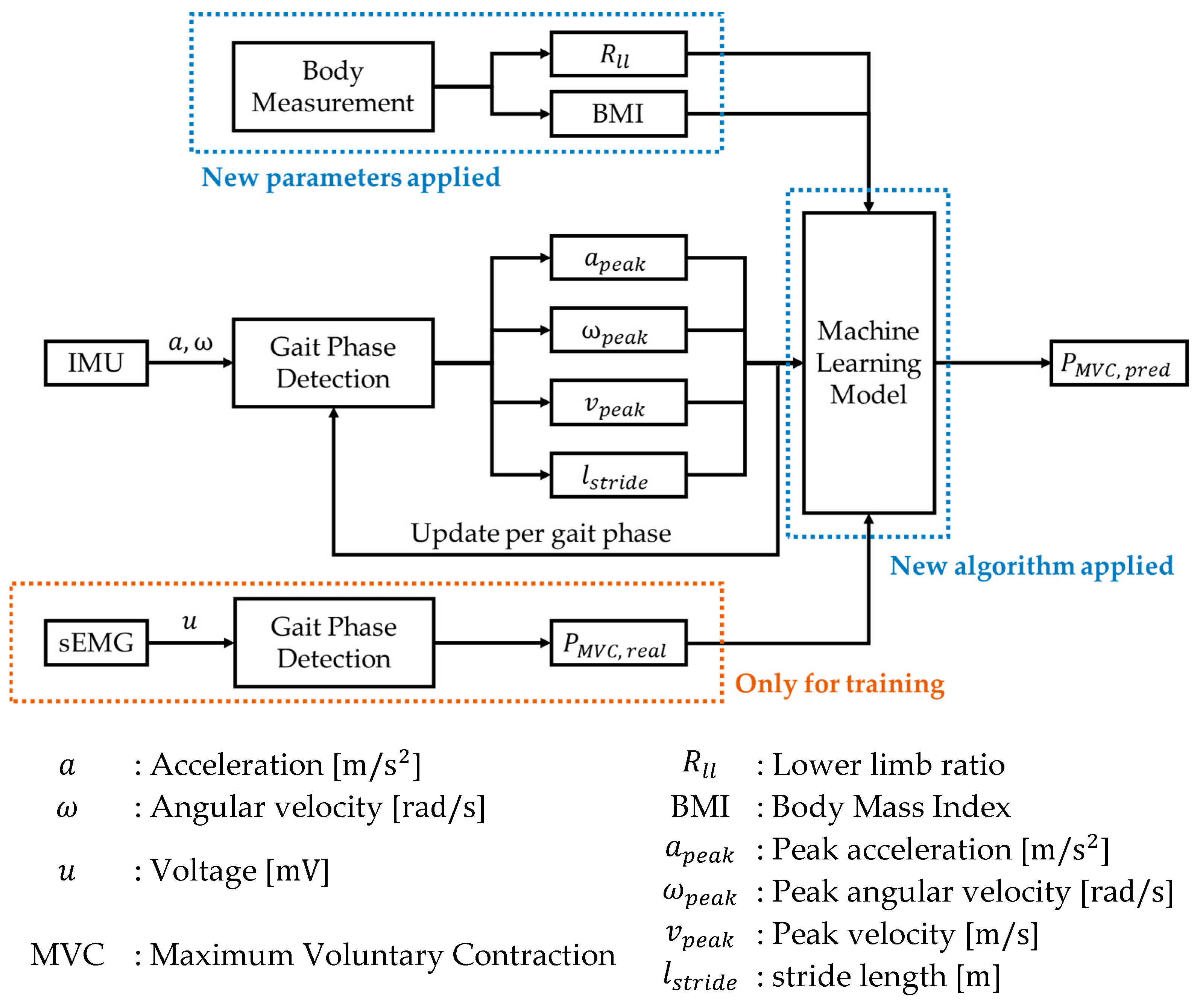
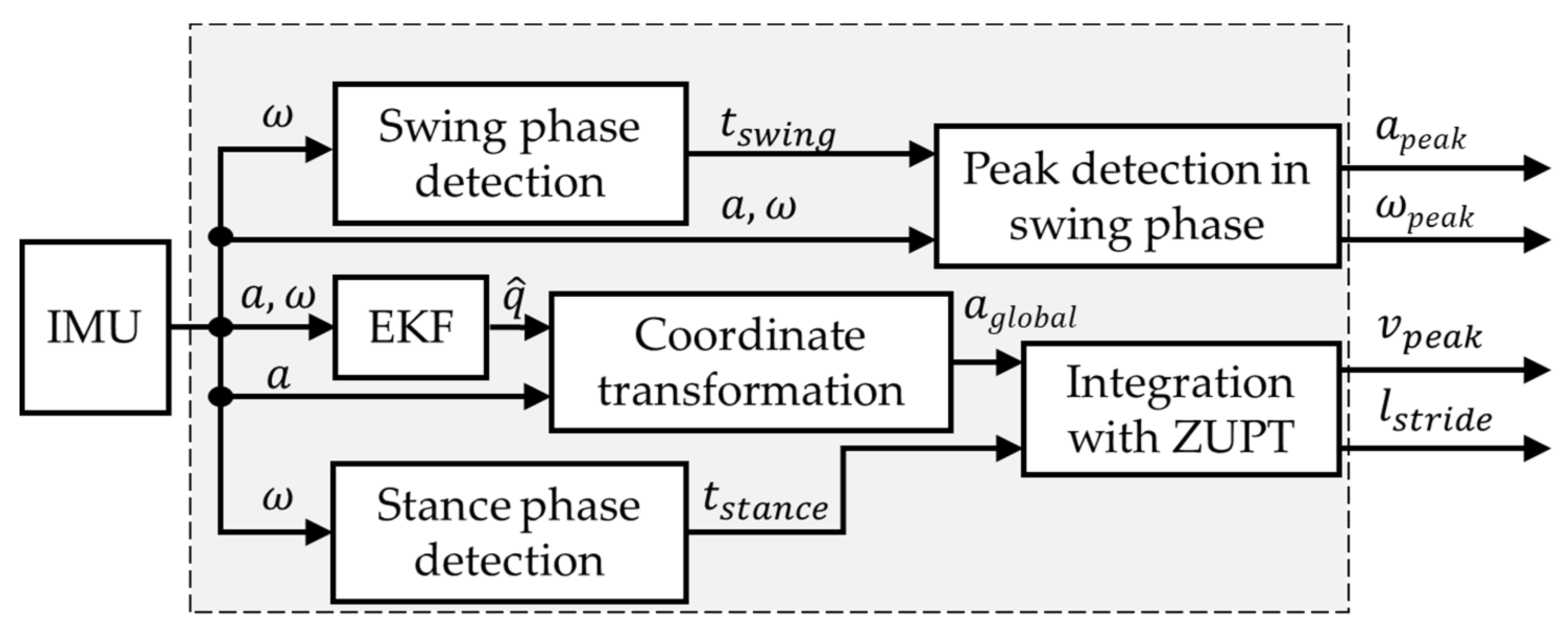
In this study, we present an updated measurement system and muscle activity estimation algorithm that overcomes all the limitations previously mentioned. The sensor system uses two IMUs, one on the shank and one on the knee joint. The IMUs collect motion data for the calculation of four gait parameters includes acceleration, velocity, angular velocity, and stride length to reconstruct a more precise gait model. ANN techniques, which are often used to solve predictive system problems [
22,
23], are embedded in the data processing algorithm, using gait parameters and individual biological data, such as BMI and the ratio between lower limb joints, to estimate the activity of the knee extensors. The muscle activity measured from sEMG sensors was used as ground truth at the training phase. We also present the results of a gait analysis experiment to evaluate both performance and reliability of this new system for estimation of knee extensors activity during walking.
This paper is structured as following:
Section 2 presents the materials and methods and introduces the system used. The experimental setup and algorithm are also described here.
Section 3 presents results and
Section 4 discusses the results and presents the future research needed to overcome the present problems.
3. Results
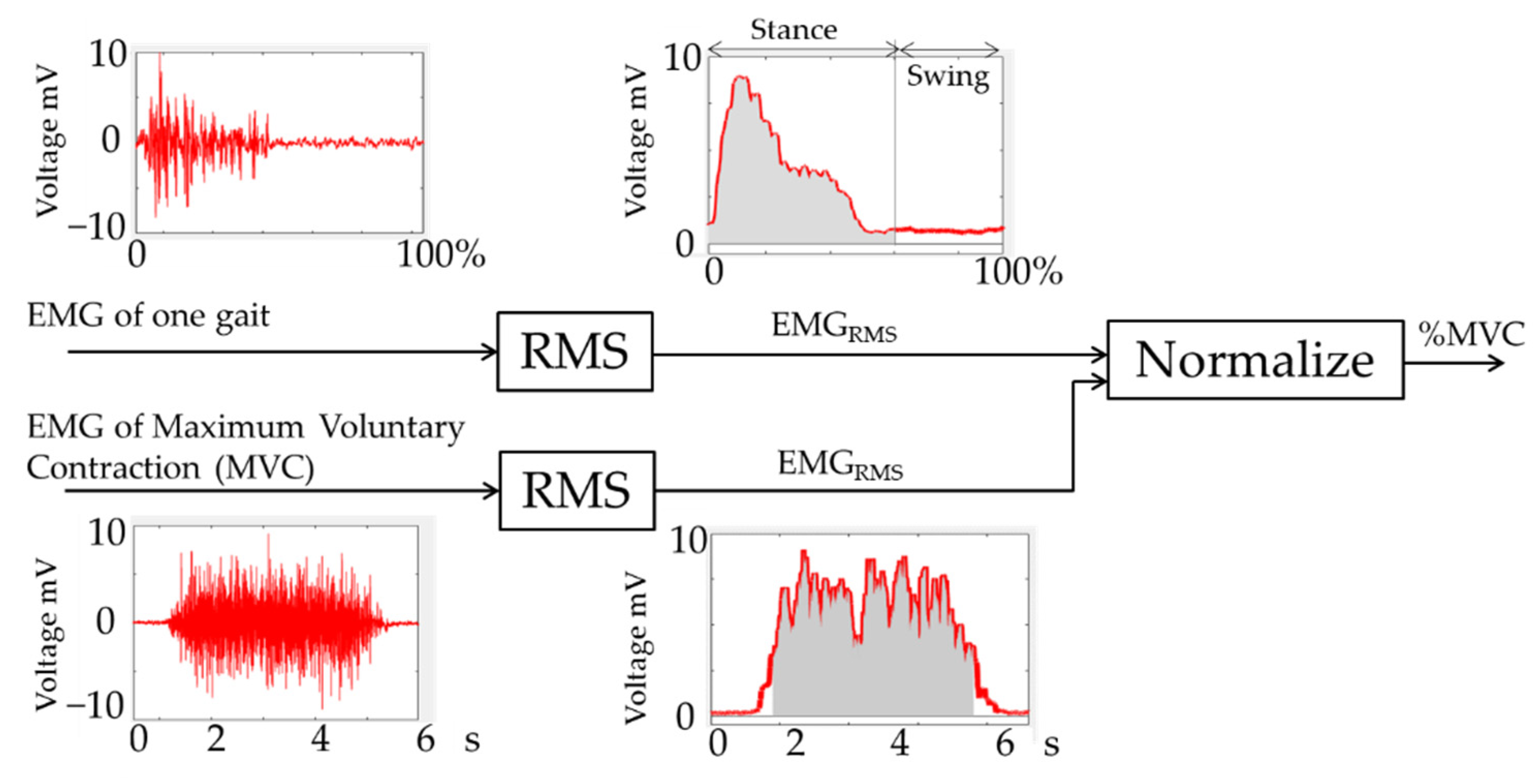
In this study, a new method to estimate muscle activity of two muscles used in walking, the rectus femoris muscle in the thigh (RFM), and the outer gastrocnemius muscle in the calf (OGM) is presented. The real-time EMG muscle activity measurement was taken as the ground truth against which the model performance was evaluated. We compared the performance of the muscle activity estimation model with the actual muscle activity measured via EMG during walking. We used the coefficient of determination
, calculated in Equation (14), as the index to evaluate the performance of the model:
where
refers to the residual sum of squares, and
refers to the total sum of squares.
For each muscle, the average muscle activity and the peak performance in one gait cycle were estimated. The results of the system performance experiment are shown in
Table 5. The comparison between the muscle activity estimated by the proposed algorithm and the actual % MVC calculated from EMG measurements showed a high estimation accuracy with a correlation efficient of
= 0.89.
The real-time performance was shown as
Table 6.
4. Discussion
By default, the hyper-parameters of the model at this stage have not been optimized. From the views of results, the accuracy of the model is notably high, but weird where accuracy testing is 30% different between the training dataset and the testing dataset. Such a situation shows that the model is with low robustness at the same time. We achieved the model optimization to improve the robustness.
For (number of the training = 3) in the given range combination, the final selected hyperparameter values are shown in
Table 7.
This set of optimized hyperparameters leads to a relatively good performance, but also to a more complex structure of the model, which indirectly increases the difficulty of model training. For this reason, the optimized model is not suitable for online learning predictions. However, the model discussed in this study is only used for offline learning.
- 2.
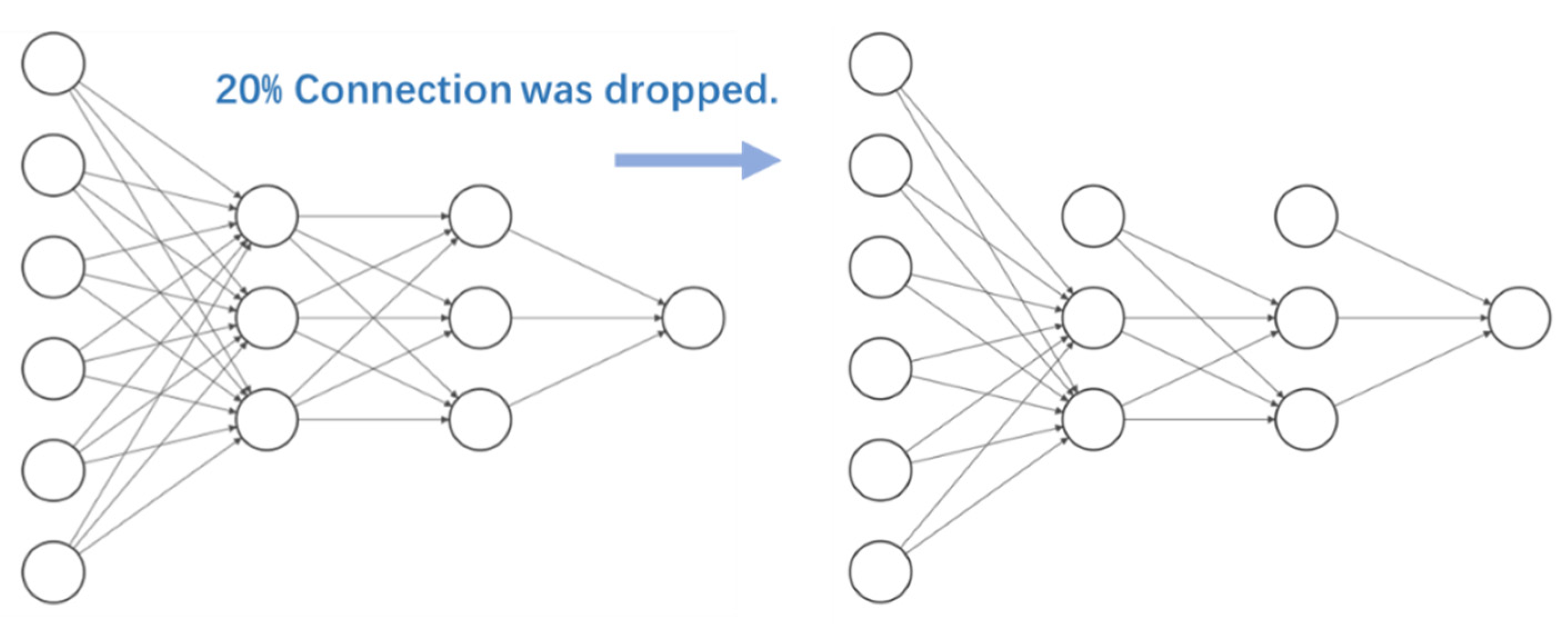
Optimization of the network structure: the most common network structure for ANN is full connection, meaning that the nodes of each layer are connected to all the nodes of the adjacent layers. The advantage of such a structure is that it can learn the training data characteristics more comprehensively. However, sometimes, a full connected ANN might give too much weight to less important or interfering features, e.g., signal processing noise. In such cases, the resulting trained model is less robust, e.g., overly sensitive to noise, and easy to overfit if trained on a small dataset, which leads to lack of practical application value of the model.
Therefore, in this study we used the “Dropout” method, to randomly discard some nodes connections (
Figure 14). This process is equivalent to noise reduction. Before using the "Dropout" method, we only need to specify the percentage of node connections required to be dropped. We compared the performances of different neural networks obtained with this process separately and selected the structure with the best performance. In this study, 20% of the original full connected neural network connections were randomly discarded based on empirical values.
The performance gap between the model on the training dataset and the test dataset is within 5%. In other words, after this optimization process, the general performance of the model has been improved.
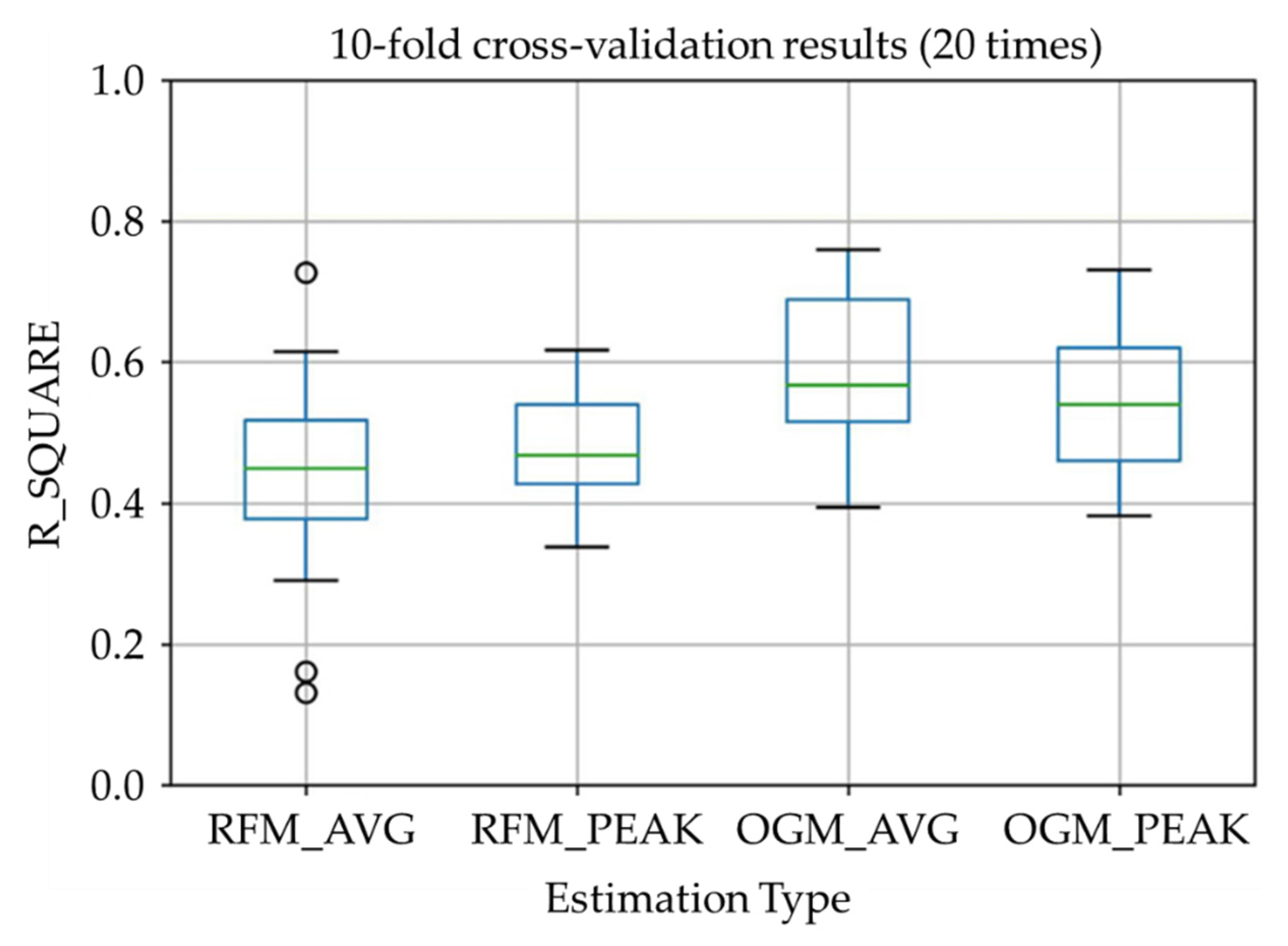
The results estimated by the proposed algorithm after optimization (in
Table 8 and
Figure 15) showed a relatively high estimation accuracy with a correlation efficient of
= 0.48 (where significant difference between distributions was confirmed using the Steel-Dwass test). For the RFM, the muscle average activity estimation and the activity peak value estimation are comparable in terms of accuracy, while the first is more scattered compared to the latter. As for the OGM, the muscle average activity estimation and the activity peak value estimation are concentrated, while the first is slightly higher than the latter.
It is important to note that the performance of real-time muscle activity estimation is affected by the signal transmission and processing delay of the current system. The measured average processing delay of the system is 72 ms, while the wireless communication average delay is 120 ms, with a total system average delay of 192 ms. Human regular walking frequency is between 1 Hz and 4 Hz [
36], which means that the average interval between different gait phases is 250–1000 ms. For this reason, a 192 ms delay is still acceptable for daily walking requirements (total delay <250 ms).
From the results,
is near 0.5 which shows to be moderate effect size. We can say that the muscle activity estimation using proposed system is working while the estimation of the rectus femoris muscle is less accurate than the muscle activity estimation of the outer gastrocnemius muscle. The reason might be due to the scarce usage of the thigh muscle during normal walking. The function of the rectus femoris during walking is raising the leg during the swing phase and lifting the upper body during stance phase. During normal walking, the upper body will only be lifted slightly. According to a previous study [
37], the activity of the rectus femoris muscle is about 26%MVC during normal walking while it is 67% MVC during stair climbing. This might also cause an error in the muscle average activity estimation, and this could explain why the activity peak value estimation of the rectus femoris muscle has better performance in comparison. As for the outer gastrocnemius muscle, both estimation results are good, and the average activity estimation is better. This is because the outer gastrocnemius muscle is frequently used in normal walking to maintain the balance of the whole body and for kicking off the ground during the stance phase.
During this study, some limitations have been discovered:
The model used in the study uses the EMG sensors measurements as the ground truth for MVC calculation. However, EMG measurement itself has intrinsic errors. For this reason, further improvements in prediction accuracy are required, possibly using more than one method to measure muscle activation and calculate the MVC;
The system in this study has data processing limitations. Before importing the model, the measured data must be filtered to remove noise and interference. As a result, the system must rely on adequate data preprocessing for correct real-time estimation of MVC values.
5. Conclusions and Future Works
In this study, a real-time muscular activity measurement system using non-contact sensors was developed. The system uses two IMU sensors to collect the motion data during normal walking to estimate the knee extensor activity. An Artificial Neural Network was used in estimation model training. An evaluation experiment was also conducted to validate the estimation algorithm.
In this study, we have shown that it is possible to estimate knee extensors activity during simple walking at different speeds, without an EMG or a Ground Reaction Force (GRF) sensor. The results of this study reveal the possibility of muscular activity estimation only by IMU.
Future works will mainly focus on the following three aspects:
Improving the accuracy of the model: subsequent research will consider using multiple sensors to estimate the MVC reference value rather than a single EMG sensor to provide the MVC reference value in model training. The fusion of multiple sensors can complement the observation results, and it is expected to raise the upper limit of prediction accuracy due to the EMG sensor;
Optimizing the effect of real-time prediction: subsequent research will consider simplifying the complexity of calculations and seeking more efficient algorithms, using feature extraction methods without gait cycle estimation, if it is possible;
Working on applications: the proposed system can not only work as measurement to offer feedback to human, but also send muscle activity data to a smart training device or exoskeleton. We have developed a knee extensor training device with active components to apply load on the knee joint during normal walking. With more detailed, real-time muscle activity data, the device can adjust its load according to the current muscle activation to avoid insufficient or excessive training.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}