
SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images





Abstract
:1. Introduction
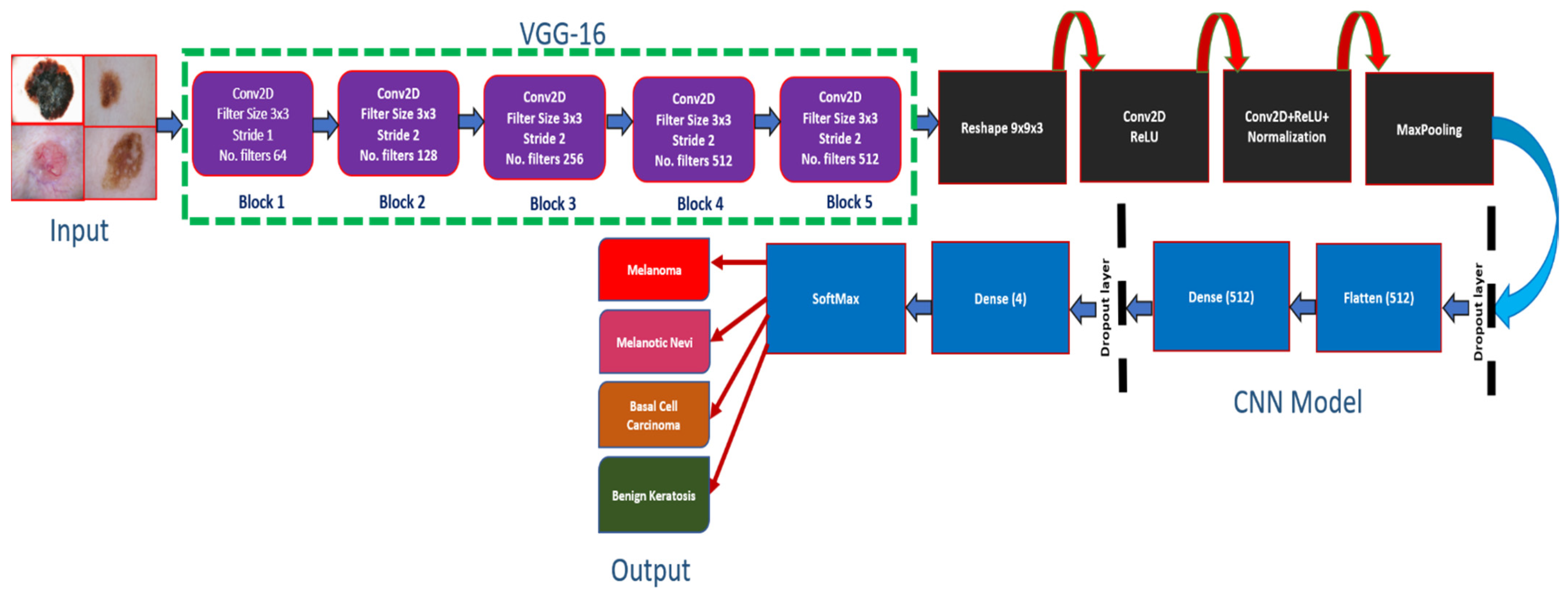
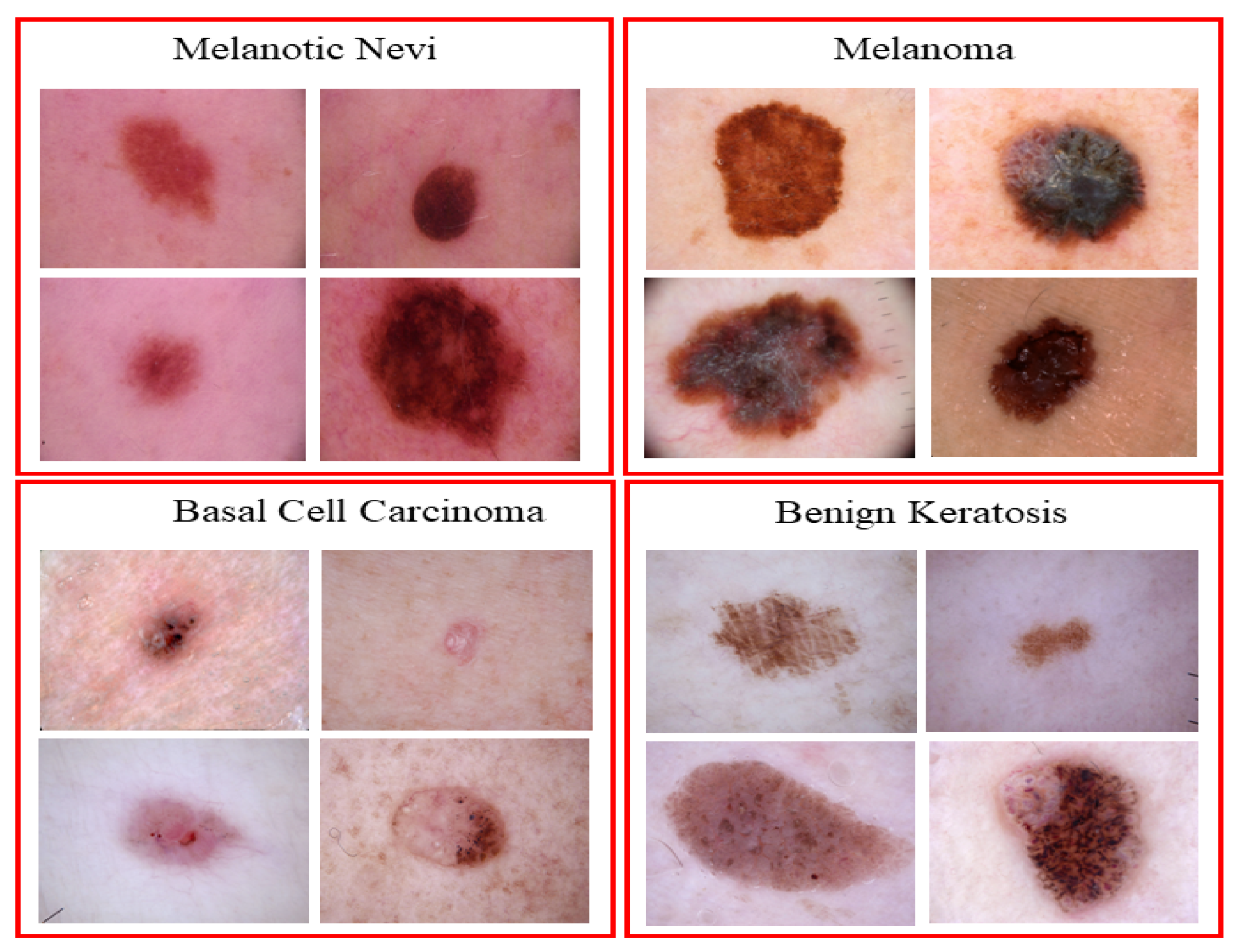
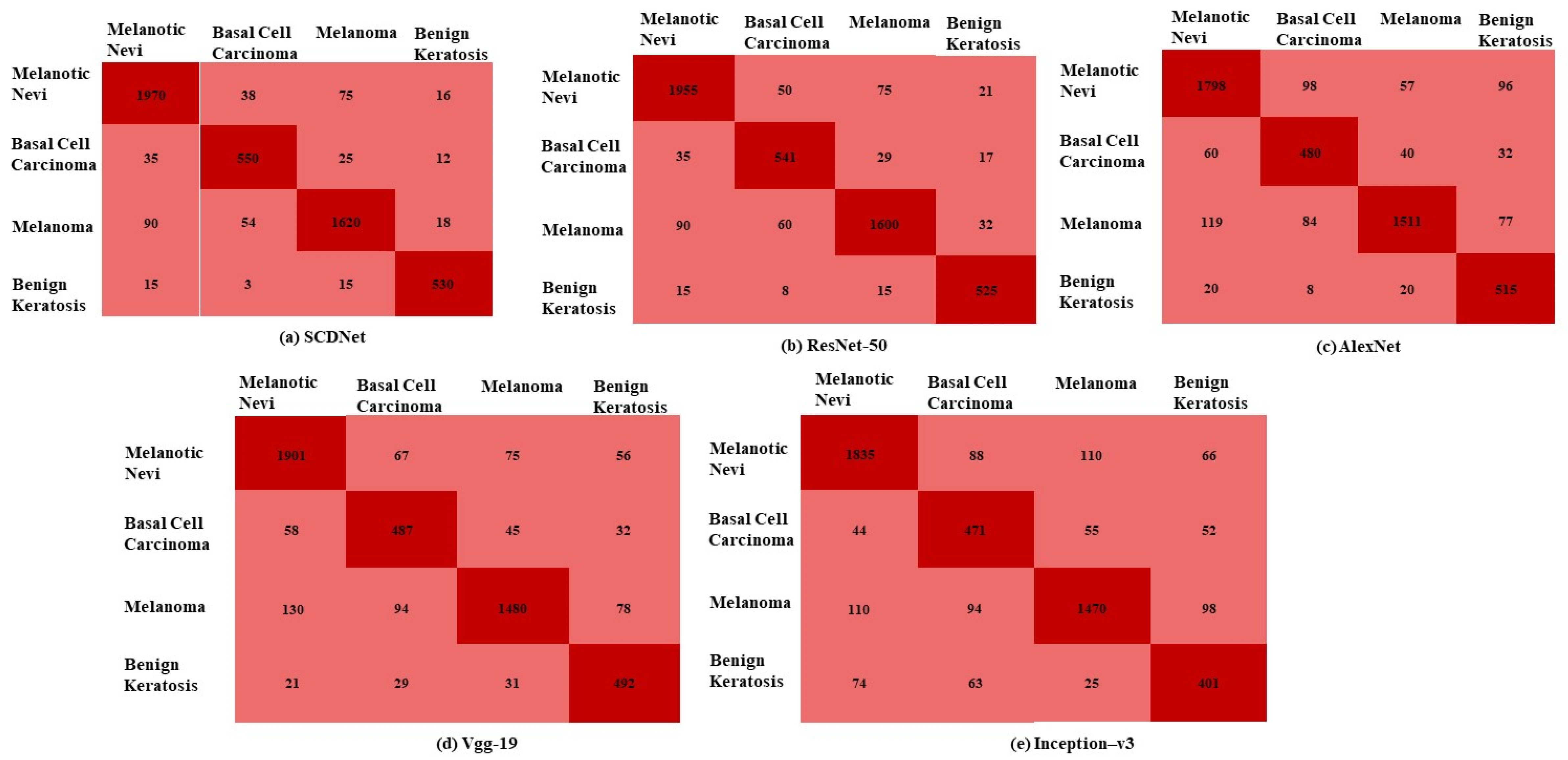
- The authors propose SCDNet which is based on CNN and Vgg16. SCDNet extracts prominent features from dermoscopic images and classifies them into four major classes of skin cancer, namely, Melanoma, Melanocytic Nevi, Basal Cell Carcinoma and Benign Keratosis. Moreover, the performance of the proposed method in terms of accuracy, f1 score, AUC, specificity and sensitivity is also compared with the four well-known classifiers in the medical domain, namely, Inception v3, Alexnet, Vgg19 and resnet50.
- The developed SCDNet was trained on dermoscopic images collected from the ISIC 2019 dataset [32] which contains images of Melanoma, Melanocytic Nevi, Basal Cell Carcinoma and Benign Keratosis. The proposed method was trained, tested, and validated using images in a 70:20:10 ratio.
- The leave one out cross validation (LOOCV) is also used to evaluate the performance of SCDNet.
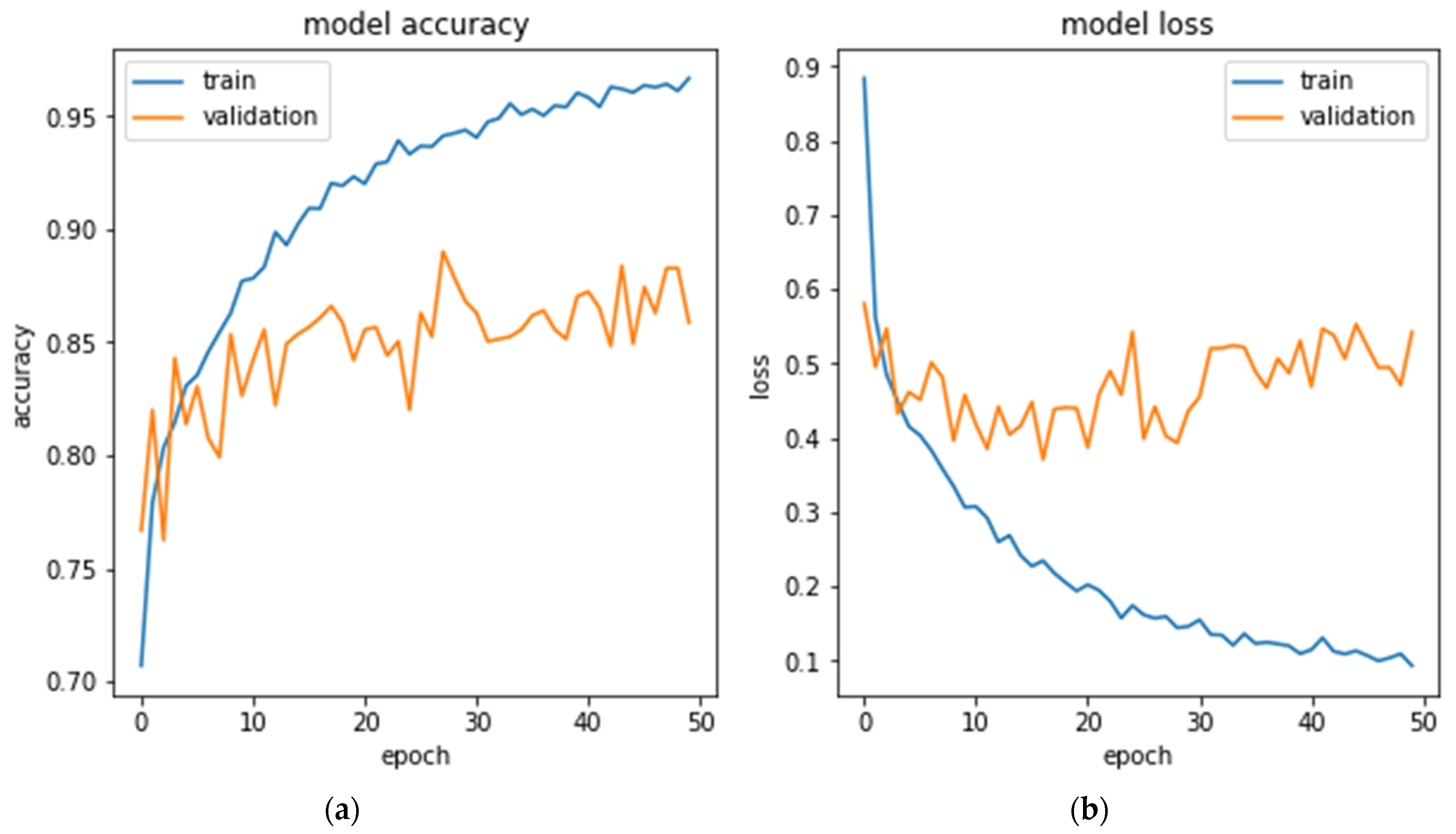
- The SCDNet showed an exceptional performance by achieving an accuracy of 96.91%, 92.18% sensitivity, 92.19% precision and 92.18% F1 score.
- AA novel deep learning framework is designed for the diagnosis of skin cancer using dermoscopic images.
2. Literature Review
3. Proposed Methodology
3.1. Dataset Description
3.2. Data Normalization and Preprocessing
3.3. Pre-Trained Classifiers
3.4. Proposed Architecture
3.5. Performance Evaluation
4. Results
4.1. Experimentation Process
4.2. SCDNet Results
4.3. Comparison with the Most Advanced Classifiers
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Basal and Squamous Cell Skin Cancer Causes Risk Factors, and Prevention. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8819.00.pdf (accessed on 19 June 2022).
- Gandhi, S.A.; Kampp, J. Skin cancer epidemiology, detection, and management. Med. Clin. 2015, 99, 1323–1335. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.C.; Bergfeld, W.F. Ultraviolet light and skin cancer in athletes. Sports Health 2009, 1, 335–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Skin Cancers. Available online: https://www.who.int/uv/faq/skincancer/en/index1.html (accessed on 19 June 2022).
- Kittler, H.; Pehamberger, H.; Wolff, K.; Binder, M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002, 3, 159–165. [Google Scholar] [CrossRef]
- Yélamos, O.; Braun, R.P.; Liopyris, K.; Wolner, Z.J.; Kerl, K.; Gerami, P.; Marghoob, A.A. Usefulness of dermoscopy to improve the clinical and histopathologic diagnosis of skin cancers. J. Am. Acad. Dermatol. 2019, 80, 365–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fee, J.A.; McGrady, F.P.; Rosendahl, C.; Hart, N.D. Training primary care physicians in dermoscopy for skin cancer detection: A scoping review. J. Cancer Educ. 2020, 35, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marra, E.; van Rijsingen, M.C.J.; Alkemade, J.A.C.; Groenewoud, J.M.M.; Hueskes, K.F.; Bijvank, C.H.M.N.; van de Laar, F.A.; Lubeek, S.F.K. The effect of a dermato-oncological training programme on the diagnostic skills and quality of referrals for suspicious skin lesions by general practitioners. Br. J. Dermatol. 2021, 184, 538–544. [Google Scholar] [CrossRef]
- Oliveira, R.B.; Papa, J.P.; Pereira, A.S.; Tavares, J.M.R.S. Computational methods for pigmented skin lesion classification in images: Review and future trends. Neural Comput. Appl. 2018, 29, 613–636. [Google Scholar] [CrossRef] [Green Version]
- Saba, T.; Khan, M.A.; Rehman, A.; Marie-Sainte, S.L. Region extraction and classification of skin cancer: A heterogeneous framework of deep CNN features fusion and reduction. J. Med. Syst. 2019, 43, 289. [Google Scholar] [CrossRef]
- Emanuelli, M.; Sartini, D.; Molinelli, E.; Campagna, R.; Pozzi, V.; Salvolini, E.; Simonetti, O.; Campanati, A.; Offidani, A. The double-edged sword of oxidative stress in skin damage and melanoma: From physiopathology to therapeutical approaches. Antioxidants 2022, 11, 612. [Google Scholar] [CrossRef]
- Nasir, M.; Khan, M.A.; Sharif, M.; Lali, I.U.; Saba, T.; Iqbal, T. An improved strategy for skin lesion detection and classification using uniform segmentation and feature selection-based approach. Microsc. Res. Tech. 2018, 81, 528–543. [Google Scholar] [CrossRef]
- Tronnier, M. Melanotic spots and melanocytic nevi. In Braun-Falco´s Dermatology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–18. [Google Scholar]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Rogers, H.W.; Weinstock, M.A.; Feldman, S.R.; Coldiron, B.M. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the US population, 2012. JAMA Dermatol. 2015, 151, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Facts and Figures. 2021. Available online: https://impactmelanoma.org/american-cancer-society-releases-2021-cancer-facts-figures-report (accessed on 13 July 2022).
- American Cancer Society. Cancer Facts and Figures. 2022. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2022/2022-cancer-facts-and-figures.pdf (accessed on 13 July 2022).
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Australian Government. Melanoma of the Skin Statistics. Available online: https://melanoma.canceraustralia.gov.au/statistics (accessed on 19 June 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, E.; Boring, C.C.; Squires, T.S. Cancer statistics, 1990. CA Cancer J. Clin. 1990, 40, 9–26. [Google Scholar] [CrossRef]
- Zhang, B.; Zhou, X.; Luo, Y.; Zhang, H.; Yang, H.; Ma, J.; Ma, L. Opportunities and challenges: Classification of skin disease based on deep learning. Chin. J. Mech. Eng. 2021, 34, 112. [Google Scholar] [CrossRef]
- Thanh, D.N.H.; Prasath, V.B.; Hieu, L.M.; Hien, N.N. Melanoma skin cancer detection method based on adaptive principal curvature, colour normalisation and feature extraction with the ABCD rule. J. Digit. Imaging 2020, 33, 574–585. [Google Scholar] [CrossRef]
- Ali, A.-R.H.; Li, J.; Yang, G. Automating the ABCD rule for melanoma detection: A survey. IEEE Access 2020, 8, 83333–83346. [Google Scholar] [CrossRef]
- Murugan, A.; Nair, S.A.H.; Kumar, K.P. Detection of skin cancer using SVM, random forest and kNN classifiers. J. Med. Syst. 2019, 43, 269. [Google Scholar] [CrossRef]
- Zawish, M.; Siyal, A.A.; Shahani, S.H.; Junejo, A.Z.; Khalil, A. Brain tumor segmentation through region-based, supervised and unsupervised learning methods: A literature survey. J. Biomed. Eng. Med. Imaging 2019, 6, 8–26. [Google Scholar]
- Abdar, M.; Samami, M.; Mahmoodabad, S.D.; Doan, T.; Mazoure, B.; Hashemifesharaki, R.; Liu, L.; Khosravi, A.; Acharya, U.R.; Makarenkov, V.; et al. Uncertainty quantification in skin cancer classification using three-way decision-based Bayesian deep learning. Comput. Biol. Med. 2021, 135, 104418. [Google Scholar] [CrossRef] [PubMed]
- Hosny, K.M.; Kassem, M.A.; Foaud, M.M. Classification of skin lesions using transfer learning and augmentation with Alex-net. PLoS ONE 2019, 14, e0217293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khamparia, A.; Singh, P.K.; Rani, P.; Samanta, D.; Khanna, A.; Bhushan, B. An internet of health things-driven deep learning framework for detection and classification of skin cancer using transfer learning. Trans. Emerg. Telecommun. Technol. 2021, 32, e3963. [Google Scholar] [CrossRef]
- Nahata, H.; Singh, S.P. Deep learning solutions for skin cancer detection and diagnosis. In Machine Learning with Health Care Perspective; Springer: Cham, Switzerland, 2020; pp. 159–182. [Google Scholar]
- Demir, A.; Yilmaz, F.; Kose, O. Early detection of skin cancer using deep learning architectures: Resnet-101 and inception-v3. In Proceedings of the 2019 Medical Technologies Congress (TIPTEKNO), Izmir, Turkey, 3–5 October 2019; pp. 1–4. [Google Scholar]
- Cassidy, B.; Kendrick, C.; Brodzicki, A.; Jaworek-Korjakowska, J.; Yap, M.H. Analysis of the ISIC image datasets: Usage, benchmarks and recommendations. Med. Image Anal. 2022, 75, 102305. [Google Scholar] [CrossRef]
- Abbas, Q.; Ramzan, F.; Ghani, M.U. Acral melanoma detection using dermoscopic images and convolutional neural networks. Vis. Comput. Ind. Biomed. Art 2021, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Sayed, G.I.; Soliman, M.M.; Hassanien, A.E. A novel melanoma prediction model for imbalanced data using optimized SqueezeNet by bald eagle search optimization. Comput. Biol. Med. 2021, 136, 104712. [Google Scholar] [CrossRef] [PubMed]
- Mijwil, M.M. Skin cancer disease images classification using deep learning solutions. Multimed. Tools Appl. 2021, 80, 26255–26271. [Google Scholar] [CrossRef]
- Nawaz, M.; Mehmood, Z.; Nazir, T.; Naqvi, R.A.; Rehman, A.; Iqbal, M.; Saba, T. Skin cancer detection from dermoscopic images using deep learning and fuzzy k-means clustering. Microsc. Res. Tech. 2022, 85, 339–351. [Google Scholar] [CrossRef]
- Dorj, U.; Lee Ke Choi, J.; Lee, M. The skin cancer classification using deep convolutional neural network. Multimed. Tools Appl. 2018, 77, 9909–9924. [Google Scholar] [CrossRef]
- Afza, F.; Sharif, M.; Mittal, M.; Khan, M.A.; Jude Hemanth, D. A hierarchical three-step superpixels and deep learning framework for skin lesion classification. Methods 2022, 202, 88–102. [Google Scholar] [CrossRef]
- Hameed, N.; Shabut, A.M.; Ghosh, M.K.; Hossain, M. Multi-class multi-level classification algorithm for skin lesions classification using machine learning techniques. Expert Syst. Appl. 2020, 141, 112961. [Google Scholar] [CrossRef]
- Singh, L.; Janghel, R.R.; Sahu, S.P. TrCSVM: A novel approach for the classification of melanoma skin cancer using transfer learning. Data Technol. Appl. 2021, 55, 64–81. [Google Scholar] [CrossRef]
- Arshad, M.; Khan, M.A.; Tariq, U.; Armghan, A.; Alenezi, F.; Javed, M.Y.; Aslam, S.M.; Kadry, S. A computer-aided diagnosis system using deep learning for multiclass skin lesion classification. Comput. Intell. Neurosci. 2021, 2021, 9619079. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Akram, T.; Zhang, Y.-D.; Sharif, M. Attributes based skin lesion detection and recognition: A mask RCNN and transfer learning-based deep learning framework. Pattern Recognit. Lett. 2021, 143, 58–66. [Google Scholar] [CrossRef]
- Abunadi, I.; Senan, E.M. Deep learning and machine learning techniques of diagnosis dermoscopy images for early detection of skin diseases. Electronics 2021, 10, 3158. [Google Scholar] [CrossRef]
- Naeem, A.; Farooq, M.S.; Khelifi, A.; Abid, A. Malignant melanoma classification using deep learning: Datasets, performance measurements, challenges and opportunities. IEEE Access 2020, 8, 110575–110597. [Google Scholar] [CrossRef]
- Malik, H.; Anees, T. BDCNet: Multi-classification convolutional neural network model for classification of COVID-19, pneumonia, and lung cancer from chest radiographs. Multimed. Syst. 2022, 28, 815–829. [Google Scholar] [CrossRef] [PubMed]
- Naeem, A.; Anees, T.; Naqvi, R.A.; Loh, W.-K. A comprehensive analysis of recent deep and federated-learning-based methodologies for brain tumor diagnosis. J. Pers. Med. 2022, 12, 275. [Google Scholar] [CrossRef] [PubMed]
- Deeba, F.; Kun, S.; Dharejo, F.A.; Zhou, Y. Sparse representation based computed tomography images reconstruction by coupled dictionary learning algorithm. IET Image Process. 2020, 14, 2365–2375. [Google Scholar] [CrossRef]
- Zawish, M.; Siyal, A.A.; Ahmed, K.; Khalil, A.; Memon, S. Brain tumor segmentation in MRI images using Chan-Vese technique in MATLAB. In Proceedings of the 2018 International Conference on Computing, Electronic and Electrical Engineering (ICE Cube), Quetta, Pakistan, 12–13 November 2018; pp. 1–6. [Google Scholar]
- Eraslan, G.; Avsec, Ž.; Gagneur, J.; Theis, F.J. Deep learning: New computational modelling techniques for genomics. Nat. Rev. Genet. 2019, 20, 389–403. [Google Scholar] [CrossRef]
- Khan, M.A.; Muhammad, K.; Sharif, M.; Akram, T.; Kadry, S. Intelligent fusion-assisted skin lesion localization and classification for smart healthcare. Neural Comput. Appl. 2021, 1–16. [Google Scholar] [CrossRef]
- Chaturvedi, S.S.; Tembhurne, J.V.; Diwan, T. A multi-class skin cancer classification using deep convolutional neural networks. Multimed. Tools Appl. 2020, 79, 28477–28498. [Google Scholar] [CrossRef]
- Deeba, F.; Kun, S.; Dharejo, F.A.; Zhou, Y. Wavelet-based enhanced medical image super resolution. IEEE Access 2020, 8, 37035–37044. [Google Scholar] [CrossRef]
- Dharejo, F.A.; Deeba, F.; Zhou, Y.; Das, B.; Jatoi, M.A.; Zawish, M.; Du, Y.; Wang, X. TWIST-GAN: Towards wavelet transform and transferred GAN for spatio-temporal single image super resolution. ACM Trans. Intell. Syst. Technol. (TIST) 2021, 12, 1–20. [Google Scholar] [CrossRef]
- Jeny, A.A.; Sakib, A.N.M.; Junayed, M.S.; Lima, K.A.; Ahmed, I.; Islam, B. SkNet: A convolutional neural networks based classification approach for skin cancer classes. In Proceedings of the 2020 23rd International Conference on Computer and Information Technology (ICCIT), Dhaka, Bangladesh, 19–21 December 2020; pp. 1–6. [Google Scholar]
- AAli, S.; Miah, S.; Haque, J.; Rahman, M.; Islam, K. An enhanced technique of skin cancer classification using deep convolutional neural network with transfer learning models. Mach. Learn. Appl. 2021, 5, 100036. [Google Scholar] [CrossRef]
- You, Y.; Zhang, Z.; Hsieh, C.; Demmel, J.; Keutzer, K. Imagenet training in minutes. In Proceedings of the 47th International Conference on Parallel Processing, Eugene, OR, USA, 13–16 August 2018; pp. 1–10. [Google Scholar]
- Quang, N.H. Automatic skin lesion analysis towards melanoma detection. In Proceedings of the 2017 21st Asia Pacific Symposium on Intelligent and Evolutionary Systems (IES), Hanoi, Vietnam, 15–17 November 2017; pp. 106–111. [Google Scholar]
- Amin, J.; Sharif, A.; Gul, N.; Anjum, M.A.; Nisar, M.W.; Azam, F.; Bukhari, S.A.C. Integrated design of deep features fusion for localization and classification of skin cancer. Pattern Recognit. Lett. 2020, 131, 63–70. [Google Scholar] [CrossRef]
- Aburaed, N.; Panthakkan, A.; Al-Saad, M.; Amin, S.A.; Mansoor, W. Deep convolutional neural network (DCNN) for skin cancer classification. In Proceedings of the 2020 27th IEEE International Conference on Electronics, Circuits and Systems (ICECS), Glasgow, UK, 23–25 November 2020; pp. 1–4. [Google Scholar]
- Zhang, J.; Xie, Y.; Xia, Y.; Shen, C. Attention residual learning for skin lesion classification. IEEE Trans. Med. Imaging 2019, 38, 2092–2103. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Mou, L.; Zhu, X.X.; Mandal, M. Automatic skin lesion classification based on mid-level feature learning. Comput. Med. Imaging Graph. 2020, 84, 101765. [Google Scholar] [CrossRef]
- Höhn, J.; Hekler, A.; Krieghoff-Henning, E.; Kather, J.N.; Utikal, J.S.; Meier, F.; Gellrich, F.F.; Hauschild, A.; French, L.; Schlager, J.G.; et al. Integrating patient data into skin cancer classification using convolutional neural networks: Systematic review. J. Med. Internet Res. 2021, 23, e20708. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Maron, R.C.; Weichenthal, M.; Utikal, J.S.; Hekler, A.; Berking, C.; Hauschild, A.; Enk, A.H.; Haferkamp, S.; Klode, J.; Schadendorf, D.; et al. Systematic outperformance of 112 dermatologists in multiclass skin cancer image classification by convolutional neural networks. Eur. J. Cancer 2019, 119, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosny, K.M.; Kassem, M.A.; Fouad, M.M. Classification of skin lesions into seven classes using transfer learning with AlexNet. J. Digit. Imaging 2020, 33, 1325–1334. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset Division | Melanoma (mel) | Melanocytic Nevi (nv) | Benign Keratosis (bk) | Basal Cell Carcinoma (bcc) | Total Images |
|---|---|---|---|---|---|
| Training Set | 3166 | 9013 | 1837 | 2327 | 17,731 |
| Validation Set | 452 | 1287 | 263 | 332 | 2533 |
| Testing Set | 904 | 2575 | 524 | 664 | 5066 |
| Total | 4522 | 12,875 | 2624 | 3323 | 25,331 |
| Types of Layers | Shape | Parameters |
|---|---|---|
| Vgg16 (layers) | (7,7,512) | 2,359,808 |
| global average pooling (Reshape) | (5,5,512) | 0 |
| dropout (Droupout) | (3,3,512) | 0 |
| dense (Dense) | 512 | 262,656 |
| Dense (Dense) | 4 | 2050 |
| 264,708 | ||
| Total params | 264,708 | |
| Train params | 2,359,808 |
| Parameters | Explanation |
|---|---|
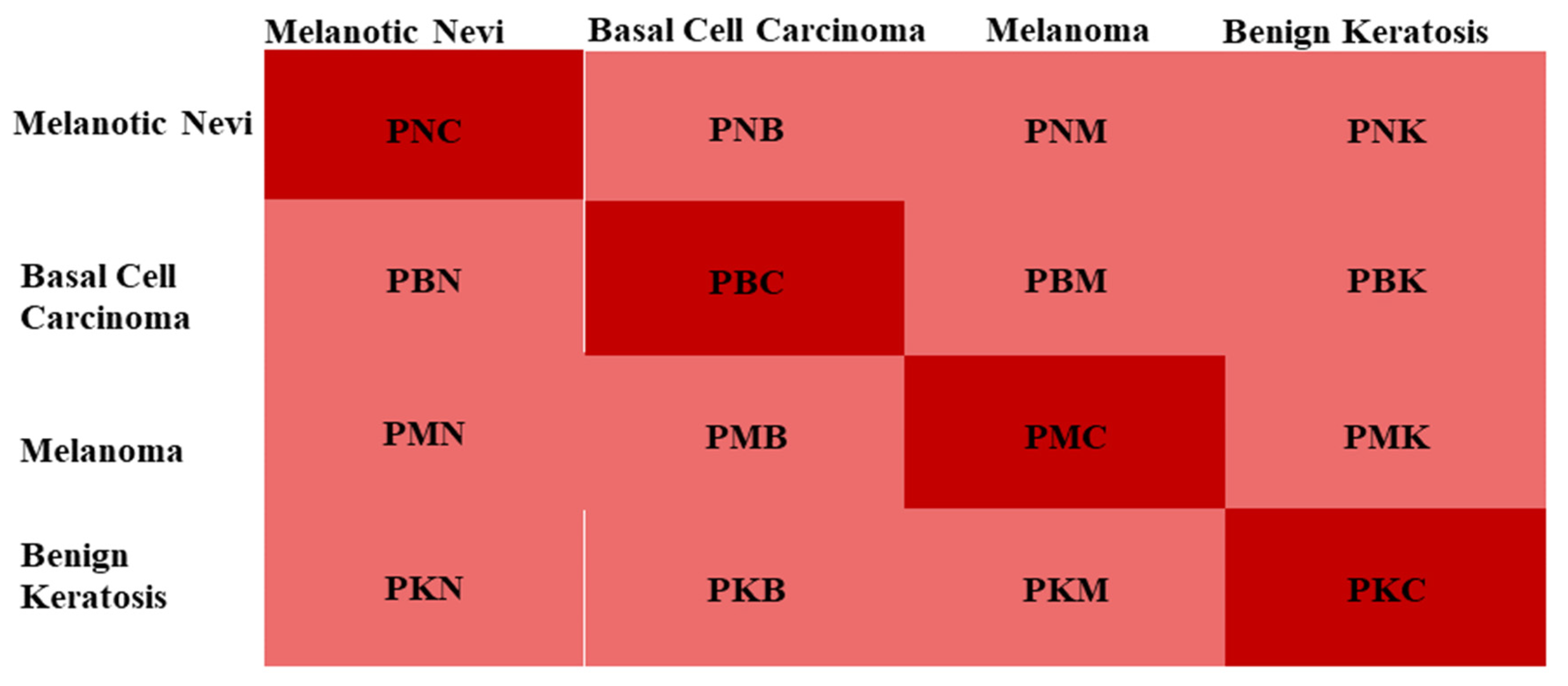
| PMC | Melanoma correctly classified as Melanoma |
| PMN | Melanoma incorrectly classified as Melanocytic nevi |
| PMB | Melanoma incorrectly classified as Basal Cell Carcinoma |
| PMK | Melanoma incorrectly classified as Benign Keratosis |
| PNC | Melanocytic nevi is correctly classified as Melanocytic nevi |
| PNM | Melanocytic nevi incorrectly classified as Melanoma |
| PNB | Melanocytic nevi is incorrectly classified as Basal Cell Carcinoma |
| PNK | Melanocytic nevi is incorrectly classified as Benign Keratosis |
| PBC | Basal Cell Carcinoma is correctly classified as Basal Cell Carcinoma |
| PBM | Basal Cell Carcinoma is incorrectly classified as Melanoma |
| PBN | Basal Cell Carcinoma is incorrectly classified as Melanocytic nevi |
| PBK | Basal Cell Carcinoma is incorrectly classified as Benign Keratosis |
| PKC | Benign Keratosis is correctly classified as Benign Keratosis |
| PKM | Benign Keratosis incorrectly classified as Melanoma |
| PKN | Benign Keratosis incorrectly classified as Melanocytic nevi |
| PKB | Benign Keratosis incorrectly classified as Basal Cell Carcinoma |
| Labels | TP | TN | FP | FN |
|---|---|---|---|---|
| Melanoma | PMC | PNM + PNB + PMB + PBM + PBN + PMN + PMC + PBC + PNC | PKM + PKN + PKB | PBK + PMK + PNK |
| Melanocytic Nevi | PNC | PKB + PKM + PBK + PMK + PKC + PMB + PBM + PMC + PBC | PNK + PNM + PNK | PBN + PMN + PKN |
| Basal Cell Carcinoma | PBC | PBC + PNB + PKN + PKN + PNC + PBN + PBK + PNK + PKC | PMK + PMN + PMB | PKM + PNM + PBM |
| Benign Keratosis | PKC | PKC + PNK + PMK + PKN + PNC + PMN + PKM + PNM + PMC | PBM + PBN + PKB | PMB + PNK + PKB |
| Classifier | Accuracy | Recall | Precision | F1-Score |
|---|---|---|---|---|
| SCDNet | 96.91% | 92.18% | 92.19% | 92.18% |
| SCDNET(LOOCV) | 94.98% | 91.35% | 91.24% | 91.30% |
| Resnet 50 | 95.50% | 91.16% | 91.18% | 91.00% |
| Vgg-19 | 94.25% | 89.71% | 89.20% | 89.44% |
| Alexnet | 93.10% | 88.41% | 88.32% | 88.36% |
| Inception-v3 | 92.54% | 87.34% | 87.36% | 87.33% |
| Model | Accuracy | Recall | Precision | F1-Score | Reference |
|---|---|---|---|---|---|
| ConvNet | 86.90% | 86.14% | 87.47% | ----- | [35] |
| ECOC SVM | 93.35% | 97.01% | 90.82% | ----- | [37] |
| 2D superpixels + MASK-RCNN | 85.50 | 83.40% | 84.50% | 85.30% | [38] |
| InceptionResnetV2 + ResNeXt101 | 88.50% | 87.40% | 88.10% | 88.30% | [42] |
| Inception-v3 | 92.83% | 84.00% | 83.00% | 84.00% | [51] |
| ARL-CNN | 86.80% | 87.80% | 86.70% | ----- | [60] |
| Densnet & Resnet | 87.00% | ----- | ----- | ----- | [61] |
| SCDNet | 96.91% | 92.18% | 92.19% | 92.18% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naeem, A.; Anees, T.; Fiza, M.; Naqvi, R.A.; Lee, S.-W. SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images. Sensors 2022, 22, 5652. https://doi.org/10.3390/s22155652
Naeem A, Anees T, Fiza M, Naqvi RA, Lee S-W. SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images. Sensors. 2022; 22(15):5652. https://doi.org/10.3390/s22155652
Chicago/Turabian StyleNaeem, Ahmad, Tayyaba Anees, Makhmoor Fiza, Rizwan Ali Naqvi, and Seung-Won Lee. 2022. "SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images" Sensors 22, no. 15: 5652. https://doi.org/10.3390/s22155652
APA StyleNaeem, A., Anees, T., Fiza, M., Naqvi, R. A., & Lee, S. -W. (2022). SCDNet: A Deep Learning-Based Framework for the Multiclassification of Skin Cancer Using Dermoscopy Images. Sensors, 22(15), 5652. https://doi.org/10.3390/s22155652