



Depth-Based Measurement of Respiratory Volumes: A Review


Abstract
:1. Introduction
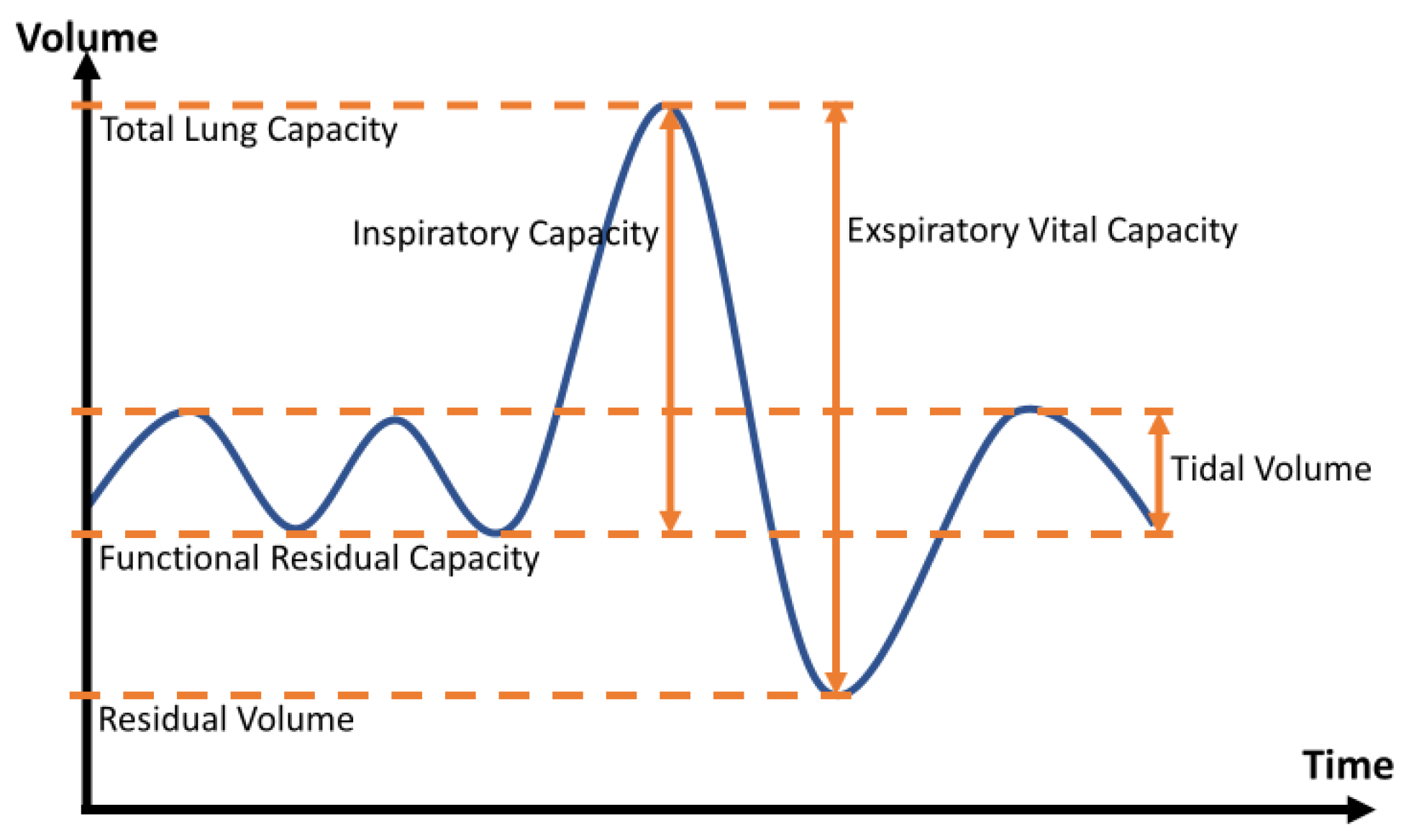
2. Fundamentals of Respiratory Measurement
3. Review on Depth-Based Respiratory Measurement
3.1. Literature Research
3.2. Methods of Depth Measurement
- marker-based methodsThis involves placing clearly visible markers on the patient’s upper body, which are then automatically registered by software. The structure of the chest can be calculated via reconstruction procedures after extensive calibration. This marker-based method is also referred to in the literature as opto-electronic plethysmography (OEP) [20] and is shown in Figure 2a. The number of markers is not fixed and can vary from 5 [21] to 89 [22] markers. Marker positioning depends on the area of the thorax being observed and is not limited to one side [23]. Another example of the application is the motion capture system in movies.
- direct methodsUsing TOF or SL methods, depth information can be inferred without applying markers. TOF measures distance by emitting laser pulses. These pulses are reflected by objects and then picked up again by a detector. Based on the required travel time, the distance can be determined via the speed of light. [24] In the structured light method, on the other hand, a known light pattern is projected onto the scene in the near-infrared range. The distance can be inferred from the deformations of the pattern on surfaces. [25] Stereoscopy is based on the use of multiple, offset cameras. The depth of information can be derived from this offset. The result of direct methods is a point cloud of depth information. The principle of these methods can be seen in Figure 2b.
- single camera systemsA single camera is used to record the subject from one side, mostly frontal.
- multi-camera systemsMultiple cameras are used to create a slightly offset stereoscopic effect or to directly view multiple sides of the patient. In particular, an effort is made to create an additional backsight of the patient.
3.3. Advantages and Application Scenarios
- The mechanics and contribution of respiratory motion are made visibleThe contributions to respiratory movement by the individual regions of the thorax can be specifically visualized and evaluated. This includes, for example, different respiratory mechanics in persons such as swimmers [26], dancers [27], or infants [28]. In addition, it is conceivable that asynchronous muscle weaknesses can be visualized, or even the failure of a lung lobe. This is not possible with traditional spirometry [29,30]. With respiration rate, respiratory volumes, and chest movements, DPG enables the measurement of three of the four classes of respiratory assessment. Only the concentration of gases cannot be measured with DPG [7].
- DPG corresponds to natural breathingNo mouthpiece is needed for non-contact measurement. Such a mouthpiece cannot be used by all patient groups. Especially in the case of facial muscle weakness, deviations in the measurements may occur [31]. Other patient groups, such as with tracheostomy, cannot use such a mouthpiece in the first place [32]. DPG can be performed without active patient participation for tidal volumes, as no mouthpiece is required. A non-contact measurement at rest can be performed straight forward, especially for children, hearing-impaired, learning-impaired, or with language barriers. Thus, breathing is not influenced by further boundary conditions.
- DPG is a potential mobile, lightweight, and low-cost methodApart from the level of development and the technology used, DPG processes offer the possibility to be used easily and everywhere, without the need for trained persons. This is not the case for multi-camera systems that require further calibration or the use of markers that need to be applied for volume extraction. Single camera systems with depth sensors, such as described in [33], which can determine respiratory volumes without calibration, offer the advantages described above. With the proliferation of depth sensors in mobile smartphone cameras [34], such technologies can potentially and in the future enable easy measurement of respiratory parameters in the everyday life of patients. Compared to the whole-body plethysmograph, with potential problems due to claustrophobia [35], DPG is not constrained by spatial constraints and can be used in a mobile manner. Used depth sensors [see Section 3.5] are cheap compared to gold standard technology, furthermore, no further consumables are needed.
3.4. Settings
3.5. Recording Systems
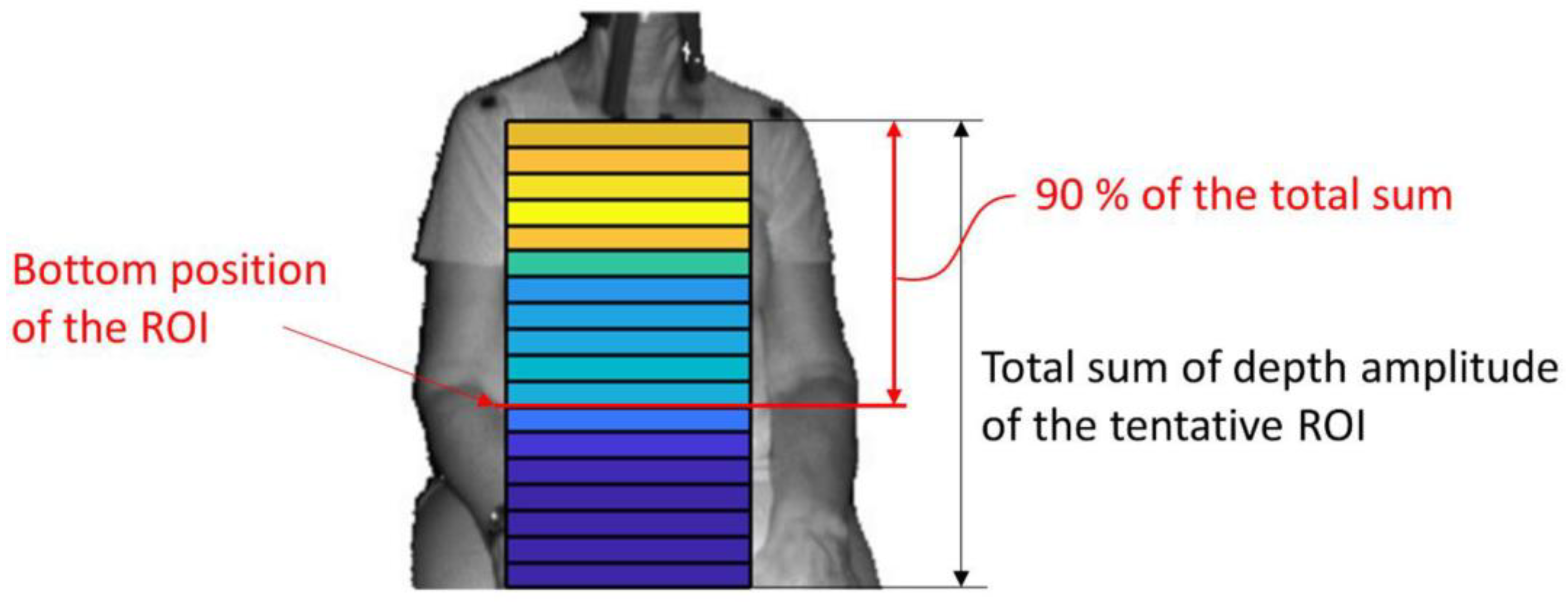
3.6. ROI-Selection
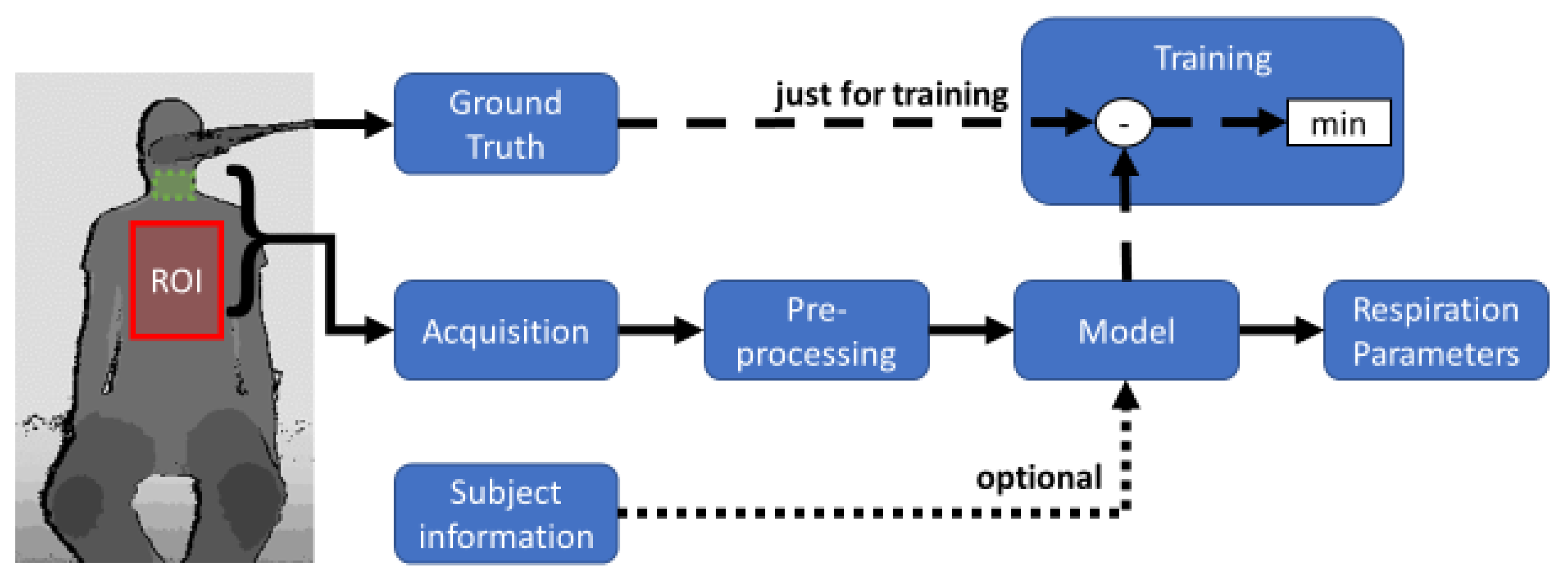
3.7. Signal Reconstruction
3.8. Accuracy of the Measuring Methods
- None: no transformation of the measured data was performed,
- Whole: the model was created with the whole data set,
- Subject: the model uses recordings of the same subject or
- Measurement: the model uses test points of the same measurement.
4. Discussion
4.1. ROI-Selection
4.2. Signal Reconstruction
4.3. Measurement Evaluation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ERS White Book. The Burden of Lung Disease. Available online: https://www.erswhitebook.org/chapters/the-burden-of-lung-disease/ (accessed on 27 September 2021).
- Krowka, M.J.; Enright, P.L.; Rodarte, J.R.; Hyatt, R.E. Effect of effort on measurement of forced expiratory volume in one second. Am. Rev. Respir. Dis. 1987, 136, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Fiz, J.A.; Haro, M.; Aguilar, J.; Alvarez, J.; Abad, J.; Monso, E.; Morera, J. Spirometry and maximal respiratory pressures in patients with facial paralysis. Chest 1993, 103, 170–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvaraju, V.; Spicher, N.; Wang, J.; Ganapathy, N.; Warnecke, J.M.; Leonhardt, S.; Swaminathan, R.; Deserno, T.M. Continuous Monitoring of Vital Signs Using Cameras: A Systematic Review. Sensors 2022, 22, 4097. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Allen, J.; Zheng, D.; Chen, F. Recent development of respiratory rate measurement technologies. Physiol. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaroni, C.; Nicolo, A.; Sacchetti, M.; Schena, E. Contactless Methods for Measuring Respiratory Rate: A Review. IEEE Sens. J. 2021, 21, 12821–12839. [Google Scholar] [CrossRef]
- Rehouma, H.; Noumeir, R.; Essouri, S.; Jouvet, P. Advancements in Methods and Camera-Based Sensors for the Quantification of Respiration. Sensors 2020, 20, 7252. [Google Scholar] [CrossRef]
- Addison, A.P.; Addison, P.S.; Smit, P.; Jacquel, D.; Borg, U.R. Noncontact Respiratory Monitoring Using Depth Sensing Cameras: A Review of Current Literature. Sensors 2021, 21, 1135. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Criée, C.P.; Sorichter, S.; Smith, H.J.; Kardos, P.; Merget, R.; Heise, D.; Berdel, D.; Köhler, D.; Magnussen, H.; Marek, W.; et al. Body plethysmography—Its principles and clinical use. Respir. Med. 2011, 105, 959–971. [Google Scholar] [CrossRef]
- Nehmeh, S.A.; Erdi, Y.E. Respiratory motion in positron emission tomography/computed tomography: A review. Semin. Nucl. Med. 2008, 38, 167–176. [Google Scholar] [CrossRef]
- Ortega, R.; Connor, C.; Kim, S.; Djang, R.; Patel, K. Monitoring ventilation with capnography. N. Engl. J. Med. 2012, 367, e27. [Google Scholar] [CrossRef]
- Muthusamy, P.D.; Sundaraj, K.; Manap, N.A. An Overview of Respiratory Airflow Estimation Techniques: Acoustic vs Non-Acoustic. In Proceedings of the 2019 IEEE International Conference on Signal and Image Processing Applications (ICSIPA), Kuala Lumpur, Malaysia, 17–19 September 2019; pp. 149–153, ISBN 978-1-7281-3377-5. [Google Scholar]
- Pacela, A.F. Impedance pneumography: A survey of instrumentation techniques. Med. Biol. Eng. 1966, 4, 1–15. [Google Scholar] [CrossRef]
- Tran, V.P.; Al-Jumaily, A.A.; Islam, S.M.S. Doppler Radar-Based Non-Contact Health Monitoring for Obstructive Sleep Apnea Diagnosis: A Comprehensive Review. BDCC 2019, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Helfenbein, E.; Firoozabadi, R.; Chien, S.; Carlson, E.; Babaeizadeh, S. Development of three methods for extracting respiration from the surface ECG: A review. J. Electrocardiol. 2014, 47, 819–825. [Google Scholar] [CrossRef]
- Monaco, V.; Stefanini, C. Assessing the Tidal Volume through Wearables: A Scoping Review. Sensors 2021, 21, 4124. [Google Scholar] [CrossRef]
- Zanuttigh, P.; Marin, G.; Dal Mutto, C.; Dominio, F.; Minto, L.; Cortelazzo, G.M. Time-of-Flight and Structured Light Depth Cameras: Technology and Applications, 1st ed.; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-30973-6. [Google Scholar]
- Massaroni, C.; Carraro, E.; Vianello, A.; Miccinilli, S.; Morrone, M.; Levai, I.K.; Schena, E.; Saccomandi, P.; Sterzi, S.; Dickinson, J.W.; et al. Optoelectronic Plethysmography in Clinical Practice and Research: A Review. Respiration 2017, 93, 339–354. [Google Scholar] [CrossRef]
- Ripka, W.L.; Ulbricht, L.; Gewehr, P.M. Application of a photogrammetric kinematic model for prediction of lung volumes in adolescents: A pilot study. BioMed. Eng. Online 2014, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- Feitosa, L.; de Britto, M.; Aliverti, A.; Noronha, J.B.; de Andrade, A.D. Accuracy of optoelectronic plethysmography in childhood exercise-induced asthma. J. Asthma 2019, 56, 61–68. [Google Scholar] [CrossRef]
- Cala, S.J.; Kenyon, C.M.; Ferrigno, G.; Carnevali, P.; Aliverti, A.; Pedotti, A.; Macklem, P.T.; Rochester, D.F. Chest wall and lung volume estimation by optical reflectance motion analysis. J. Appl. Physiol. 1996, 81, 2680–2689. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Wiede, C.; Kokozinski, R. Data Processing Approaches on SPAD-Based d-TOF LiDAR Systems: A Review. IEEE Sens. J. 2021, 21, 5656–5667. [Google Scholar] [CrossRef]
- van der Jeught, S.; Dirckx, J.J. Real-time structured light profilometry: A review. Opt. Lasers Eng. 2016, 87, 18–31. [Google Scholar] [CrossRef]
- Silvatti, A.P.; Sarro, K.J.; Cerveri, P.; Baroni, G.; Barros, R. A 3D kinematic analysis of breathing patterns in competitive swimmers. J. Sport. Sci. 2012, 30, 1551–1560. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.M.; Bernardina, G.; Sarro, K.J.; Baroni, G.; Cerveri, P.; Silvatti, A.P. Thoracoabdominal breathing motion pattern and coordination of professional ballet dancers. Sport. Biomech. 2019, 18, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Wiegandt, F.C.; Biegger, D.; Fast, J.F.; Matusiak, G.; Mazela, J.; Ortmaier, T.; Doll, T.; Dietzel, A.; Bohnhorst, B.; Pohlmann, G. Detection of breathing movements of preterm neonates by recording their abdominal movements with a time-of-flight camera. Pharmaceutics 2021, 13, 721. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, S.; Yamashiro, T.; Washko, G.R.; Kurihara, Y.; Nakajima, Y.; Hatabu, H. Quantitative CT assessment of chronic obstructive pulmonary disease. Radiographics 2010, 30, 55–66. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E. Assessment of bronchodilator efficacy in symptomatic COPD: Is spirometry useful? Chest 2000, 117, 42S–47S. [Google Scholar] [CrossRef]
- Wohlgemuth, M.; van der Kooi, E.L.; Hendriks, J.C.; Padberg, G.W.; Folgering, H.T. Face mask spirometry and respiratory pressures in normal subjects. Eur. Respir. J. 2003, 22, 1001–1006. [Google Scholar] [CrossRef]
- Boudarham, J.; Pradon, D.; Prigent, H.; Vaugier, I.; Barbot, F.; Letilly, N.; Falaize, L.; Orlikowski, D.; Petitjean, M.; Lofaso, F. Optoelectronic vital capacity measurement for restrictive diseases. Respir. Care 2013, 58, 633–638. [Google Scholar] [CrossRef] [Green Version]
- Takamoto, H.; Nishine, H.; Sato, S.; Sun, G.; Watanabe, S.; Seokjin, K.; Asai, M.; Mineshita, M.; Matsui, T. Development and Clinical Application of a Novel Non-contact Early Airflow Limitation Screening System Using an Infrared Time-of-Flight Depth Image Sensor. Front. Physiol. 2020, 11, 552942. [Google Scholar] [CrossRef]
- Breitbarth, A.; Schardt, T.; Kind, C.; Brinkmann, J.; Dittrich, P.-G.; Notni, G. Measurement accuracy and dependence on external influences of the iPhone X TrueDepth sensor. In Proceedings of the Joint TC1–TC2 International Symposium on Photonics and Education in Measurement Science, Jena, Germany, 17–19 September 2019; Rosenberger, M., Dittrich, P.-G., Zagar, B., Eds.; SPIE: Bellingham, WA, USA, 2019; p. 7. ISBN 9781510629813. [Google Scholar]
- DuBois, A.B.; Botelho, S.Y.; Comroe, J.H. A new method for measuring airway resistance in man using a body plethysmograph: Values in normal subjects and in patients with respiratory disease. J. Clin. Investig. 1956, 35, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Reyes, B.A.; Reljin, N.; Kong, Y.; Nam, Y.; Chon, K.H. Tidal Volume and Instantaneous Respiration Rate Estimation using a Volumetric Surrogate Signal Acquired via a Smartphone Camera. IEEE J. Biomed. Health Inform. 2017, 21, 764–777. [Google Scholar] [CrossRef]
- Sharp, C.; Soleimani, V.; Hannuna, S.; Camplani, M.; Damen, D.; Viner, J.; Mirmehdi, M.; Dodd, J.W. Toward respiratory assessment using depth measurements from a time-of-flight sensor. Front. Physiol. 2017, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, V.; Mirmehdi, M.; Damen, D.; Dodd, J. Markerless Active Trunk Shape Modelling for Motion Tolerant Remote Respiratory Assessment. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018. [Google Scholar] [CrossRef] [Green Version]
- Ostadabbas, S.; Bulach, C.; Ku, D.N.; Anderson, L.J.; Ghovanloo, M. A passive quantitative measurement of airway resistance using depth data. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5743–5747. [Google Scholar] [CrossRef] [Green Version]
- Ostadabbas, S.; Sebkhi, N.; Zhang, M.; Rahim, S.; Anderson, L.J.; Lee, F.-H.; Ghovanloo, M. A Vision-Based Respiration Monitoring System for Passive Airway Resistance Estimation. IEEE Trans. Biomed. Eng. 2016, 63, 1904–1913. [Google Scholar] [CrossRef]
- Kempfle, J.; van Laerhoven, K. Breathing In-Depth: A Parametrization Study on RGB-D Respiration Extraction Methods. Front. Comput. Sci. 2021, 3, 757277. [Google Scholar] [CrossRef]
- Harte, J.M.; Golby, C.K.; Acosta, J.; Nash, E.F.; Kiraci, E.; Williams, M.A.; Arvanitis, T.N.; Naidu, B. Chest wall motion analysis in healthy volunteers and adults with cystic fibrosis using a novel Kinect-based motion tracking system. Med. Biol. Eng. Comput. 2016, 54, 1631–1640. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, V.; Mirmehdi, M.; Damen, D.; Camplani, M.; Hannuna, S.; Sharp, C.; Dodd, J. Depth-based whole body photoplethysmography in remote pulmonary function testing. IEEE Trans. Biomed. Eng. 2018, 65, 1421–1431. [Google Scholar] [CrossRef] [Green Version]
- Giancola, S.; Valenti, M.; Sala, R. A Survey on 3D Cameras: Metrological Comparison of Time-of-Flight, Structured-Light and Active Stereoscopy Technologies; Springer International Publishing: Cham, Switzerland, 2018; ISBN 978-3-319-91760-3. [Google Scholar]
- Soleimani, V.; Mirmehdi, M.; Damen, D.; Hannuna, S.; Camplani, M. 3D Data Acquisition and Registration Using Two Opposing Kinects. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 128–137, ISBN 978-1-5090-5407-7. [Google Scholar]
- de Faria Júnior, N.S.; Santos, I.R.; Dias, I.S.; Urbano, J.J.; Da Palma, R.K.; Fonsêca, N.T.; Nacif, S.R.; Filho, F.; Costa, D.; Maciel, A.; et al. Opto-electronic plethysmography: Noninvasive and accurate measurement of the volume of the chest wall and its different thoraco-abdominal compartments. Med. Sci. Technol. 2013, 54, 147–150. [Google Scholar] [CrossRef]
- Meric, H.; Falaize, L.; Pradon, D.; Orlikowski, D.; Prigent, H.; Lofaso, F. 3D analysis of the chest wall motion for monitoring late-onset Pompe disease patients. Neuromuscul. Disord. 2016, 26, 146–152. [Google Scholar] [CrossRef]
- Soleimani, V.; Mirmehdi, M.; Damen, D.; Hannuna, S.; Camplani, M.; Viner, J.; Dodd, J. Remote pulmonary function testing using a depth sensor. In Proceedings of the 2015 IEEE Biomedical Circuits and Systems Conference (BioCAS), Atlanta, GA, USA, 22–24 October 2015. [Google Scholar] [CrossRef]
- Oh, K.; Shin, C.S.; Kim, J.; Yoo, S.K. Level-Set Segmentation-Based Respiratory Volume Estimation Using a Depth Camera. IEEE J. Biomed. Health Inform. 2019, 23, 1674–1682. [Google Scholar] [CrossRef]
- Arrieta, C.; Sing-Long, C.; Uribe, S.; Andia, M.E.; Irarrazaval, P.; Tejos, C. Level set segmentation with shape prior knowledge using intrinsic rotation, translation and scaling alignment. In Proceedings of the 2015 IEEE 12th International Symposium on Biomedical Imaging (ISBI 2015), Brooklyn, NY, USA, 16–19 April 2015; pp. 1568–1571, ISBN 978-1-4799-2374-8. [Google Scholar]
- Addison, P.S.; Smit, P.; Jacquel, D.; Addison, A.P.; Miller, C.; Kimm, G. Continuous non-contact respiratory rate and tidal volume monitoring using a Depth Sensing Camera. J. Clin. Monit. Comput. 2022, 36, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Seppanen, T.M.; Kananen, J.; Kai, N.; Alho, O.-P.; Seppanen, T. Accurate measurement of respiratory airflow waveforms using depth data. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 7857–7860. [Google Scholar] [CrossRef]
- Yu, M.-C.; Liou, J.-L.; Kuo, S.-W.; Lee, M.-S.; Hung, Y.-P. Noncontact respiratory measurement of volume change using depth camera. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2012, 2012, 2371–2374. [Google Scholar] [CrossRef] [PubMed]
- Bradski, G. The OpenCV Library. Dr. Dobb’s J. Softw. Tools Prof. Program. 2000, 25, 120–123. [Google Scholar]
- Imano, W.; Kameyama, K.; Hollingdal, M.; Refsgaard, J.; Larsen, K.; Topp, C.; Kronborg, S.H.; Gade, J.D.; Dinesen, B. Non-Contact Respiratory Measurement Using a Depth Camera for Elderly People. Sensors 2020, 20, 6901. [Google Scholar] [CrossRef] [PubMed]
- Zoumot, Z.; Lomauro, A.; Aliverti, A.; Nelson, C.; Ward, S.; Jordan, S.; Polkey, M.I.; Shah, P.L.; Hopkinson, N.S. Lung Volume Reduction in Emphysema Improves Chest Wall Asynchrony. Chest 2015, 148, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, V.; Mirmehdi, M.; Damen, D.; Dodd, J.; Hannuna, S.; Sharp, C.; Camplani, M.; Viner, J. Remote, Depth-Based Lung Function Assessment. IEEE Trans. Biomed. Eng. 2017, 64, 1943–1958. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.-C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. Lond. A 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Wichum, F.; Hassel, J.; Wiede, C.; Seidl, K. Contactless Measurement of Respiratory Volumes: A Calibration Free Method based on Depth Information. In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies, Online Streaming, 9–11 February 2022; SCITEPRESS—Science and Technology Publications: Setúbal, Portugal, 2022; pp. 150–158. ISBN 978-989-758-552-4. [Google Scholar]
- Transue, S.; Nguyen, P.; Vu, T.; Choi, M.-H. Real-Time Tidal Volume Estimation Using Iso-surface Reconstruction. In Proceedings of the 2016 IEEE First International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 27–29 June 2016; pp. 209–218, ISBN 978-1-5090-0943-5. [Google Scholar]
- Konno, K.; Mead, J. Measurement of the separate volume changes of rib cage and abdomen during breathing. J. Appl. Physiol. 1967, 22, 407–422. [Google Scholar] [CrossRef] [Green Version]
- Bellemare, F.; Jeanneret, A.; Couture, J. Sex differences in thoracic dimensions and configuration. Am. J. Respir. Crit. Care Med. 2003, 168, 305–312. [Google Scholar] [CrossRef]
- Kaneko, H.; Horie, J. Breathing movements of the chest and abdominal wall in healthy subjects. Respir. Care 2012, 57, 1442–1451. [Google Scholar] [CrossRef] [Green Version]
- Vogiatzis, I.; Aliverti, A.; Golemati, S.; Georgiadou, O.; Lomauro, A.; Kosmas, E.; Kastanakis, E.; Roussos, C. Respiratory kinematics by optoelectronic plethysmography during exercise in men and women. Eur. J. Appl. Physiol. 2005, 93, 581–587. [Google Scholar] [CrossRef]
- Verschakelen, J.A.; Demedts, M.G. Normal thoracoabdominal motions. Influence of sex, age, posture, and breath size. Am. J. Respir. Crit. Care Med. 1995, 151, 399–405. [Google Scholar] [CrossRef]
- Soleimani, V. Remote Depth-Based Photoplethysmography in Pulmonary Function Testing. Ph.D. Thesis, University of Bristol, Bristol, UK, 2018. [Google Scholar]
- Sharma, G.; Goodwin, J. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 2006, 1, 253–260. [Google Scholar] [CrossRef]
- Sasko, B.; Thiem, U.; Christ, M.; Trappe, H.-J.; Ritter, O.; Pagonas, N. Size matters: An observational study investigating estimated height as a reference size for calculating tidal volumes if low tidal volume ventilation is required. PLoS ONE 2018, 13, e0199917. [Google Scholar] [CrossRef]
- Littleton, S.W. Impact of obesity on respiratory function. Respirology 2012, 17, 43–49. [Google Scholar] [CrossRef]
- Lomauro, A.; Aliverti, A. Sex differences in respiratory function. Breathe 2018, 14, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Kempfle, J.; van Laerhoven, K. Towards Breathing as a Sensing Modality in Depth-Based Activity Recognition. Sensors 2020, 20, 3884. [Google Scholar] [CrossRef]
- Xu, G.; Huang, J.Z. Asymptotic optimality and efficient computation of the leave-subject-out cross-validation. Ann. Statist. 2012, 40, 3003–3030. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paper | Marker/ Direct | Cameras | Model | Calibration | Results for Respiration Parameters | #Subjects (Healthy) |
|---|---|---|---|---|---|---|
| [32] | marker | multiple | linear | whole | VC: mean: −20 ± 93 mL | 20 (0) |
| [49] | direct | single | linear | none | TV: mean: 8.41% | 10 (10) |
| [40] | direct | single | linear | none | TV: mean: 70 ± 60 mL | 14 (14) |
| [36] | direct | single | linear | subject | TV: RMSE 182 ± 107 mL | 15 (15) |
| [21] | marker | single | linear | whole | VC: mean: −30 ± 352 mL | 50 (50) |
| [37] | direct | single | linear | whole | VC: mean: 16 ± 51 mL | 100 (21) |
| [43] | direct | multiple | linear | subject | VC: mean: −300 ± 561 mL TV: mean: 0 ± 204 mL | 35 (35) |
| [57] | direct | single | linear | subject | VC: mean: −150 ± 842 mL TV: mean: 100 ± 255 mL | 35 (35) |
| [48] | direct | single | linear | meas. | VC: mean: 9 ± 39 mL TV: mean: 74 ± 88 mL | 40 (0) |
| [33] | direct | single | linear | none | VC: mean: 57 ± 716 mL | 53 (21) |
| [51] | direct | single | linear | subject | TV: mean: −213 ± 85 mL | 1 (1) |
| [52] | direct | single | non-linear | subject | TV: mean: 9.4 ± 8.4% | 8 (8) |
| [60] | direct | single | non-linear | subject | TV: max: 7.8%, min: 5.81% | 4 (4) |
| [55] | direct | single | linear | whole | TV: mean: 10.7% up to 15.5% | 39 (39) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wichum, F.; Wiede, C.; Seidl, K. Depth-Based Measurement of Respiratory Volumes: A Review. Sensors 2022, 22, 9680. https://doi.org/10.3390/s22249680
Wichum F, Wiede C, Seidl K. Depth-Based Measurement of Respiratory Volumes: A Review. Sensors. 2022; 22(24):9680. https://doi.org/10.3390/s22249680
Chicago/Turabian StyleWichum, Felix, Christian Wiede, and Karsten Seidl. 2022. "Depth-Based Measurement of Respiratory Volumes: A Review" Sensors 22, no. 24: 9680. https://doi.org/10.3390/s22249680
APA StyleWichum, F., Wiede, C., & Seidl, K. (2022). Depth-Based Measurement of Respiratory Volumes: A Review. Sensors, 22(24), 9680. https://doi.org/10.3390/s22249680