
Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review

 ,
, 

Abstract
:1. Introduction
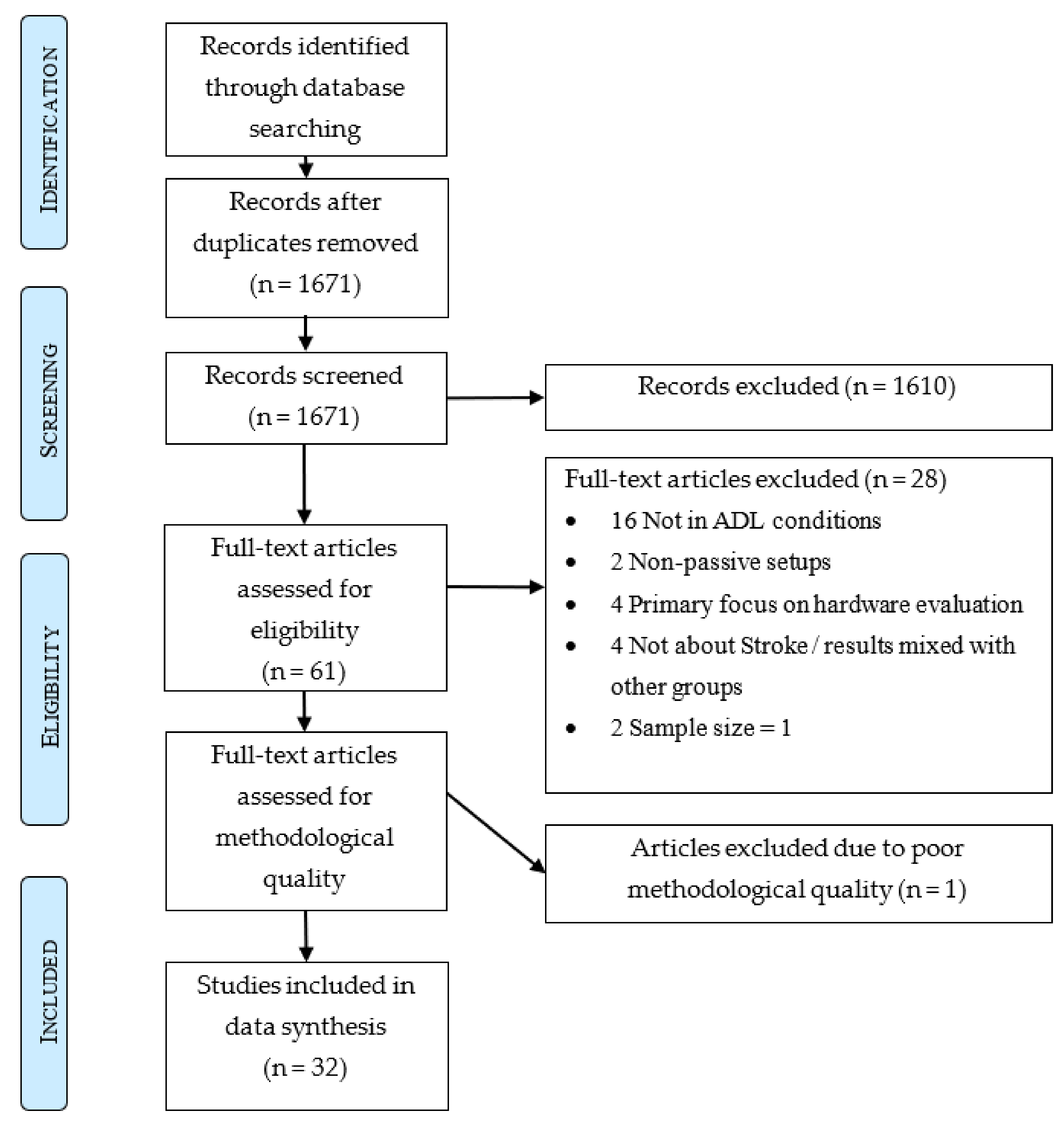
2. Materials and Methods
2.1. Search Method
- (1)
- Terms for stroke
- (2)
- Terms for movement and motor symptoms
- (3)
- Terms for wearable sensors and devices
- (4)
- Terms for activities of daily living and continuous monitoring
- (“Stroke”[Mesh] OR Cerebrovascular Accident*[tiab] OR Stroke*[tiab] OR CVA[tiab])
- AND
- (“Movement”[Mesh] OR “Motor Disorders”[Mesh] OR Move*[tiab] OR Motor Symptom*[tiab] OR Motor Disorder*[tiab])
- AND
- (Accelerometer*[tiab] OR “IMU”[tiab] OR Inertial Unit*[tiab] OR Gyroscope*[tiab] OR “Electrical Equipment and Supplies”[Mesh] OR Sensor*[tiab] OR Wearable*[tiab] OR Tracker*[tiab] OR Emg[tiab] OR Electromyograph*[tiab] OR Pressure Sens*[tiab] OR Strain Gauges Based Sens*[tiab] OR Strain Sens*[tiab] OR Strain Gauge*[tiab])
- AND
- (“Activities of Daily Living”[Mesh] OR Activities of Daily Living[tiab] OR ADL[tiab] OR Daily life*[tiab] OR “Continuous Monitoring”[tiab] OR “Remote Monitoring”[tiab] OR “Monitoring, Physiologic”[Mesh] OR “Monitoring, Ambulatory”[Mesh] OR Home-Based[tiab] OR “Environment”[Mesh] OR “Environment*”[tiab] OR “Communal*”[tiab] OR “Commune*”[tiab] OR “Community*”[tiab] OR “Communities”[tiab] OR “Free-Living”[tiab] OR “Free Living”[tiab] OR “Long Term”[tiab] OR “Real World”[tiab])
2.2. Eligibility Criteria
2.3. Assessment of Methodological Quality
2.4. Data Extraction and Synthesis
3. Results
3.1. Study Design, Sample Size and Participant Characteristics
3.2. Protocol
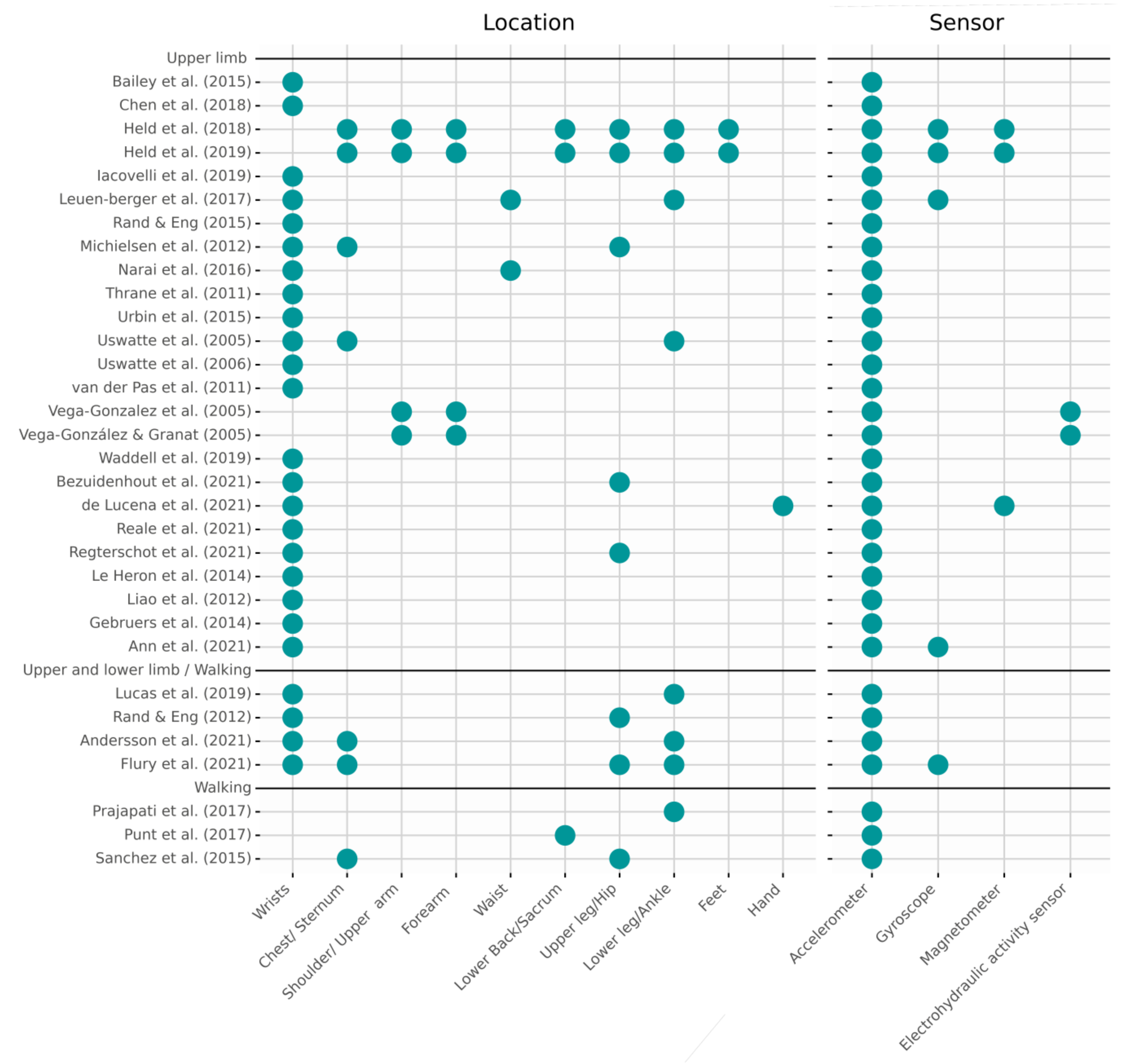
3.3. Sensor Placement and Technology
3.4. Movement Measures Derived from Sensors
3.4.1. Upper Limb Activity-Related Movement Measures
3.4.2. Measures of Quantitative Aspects of Upper Limb Movement
3.4.3. Measures of Qualitative Aspects of Upper Limb Movement
3.4.4. Hand Movement Related Measures
3.4.5. Lower Body and Gait Related Measures
3.4.6. General Measures of Quantitative Aspects of Movement
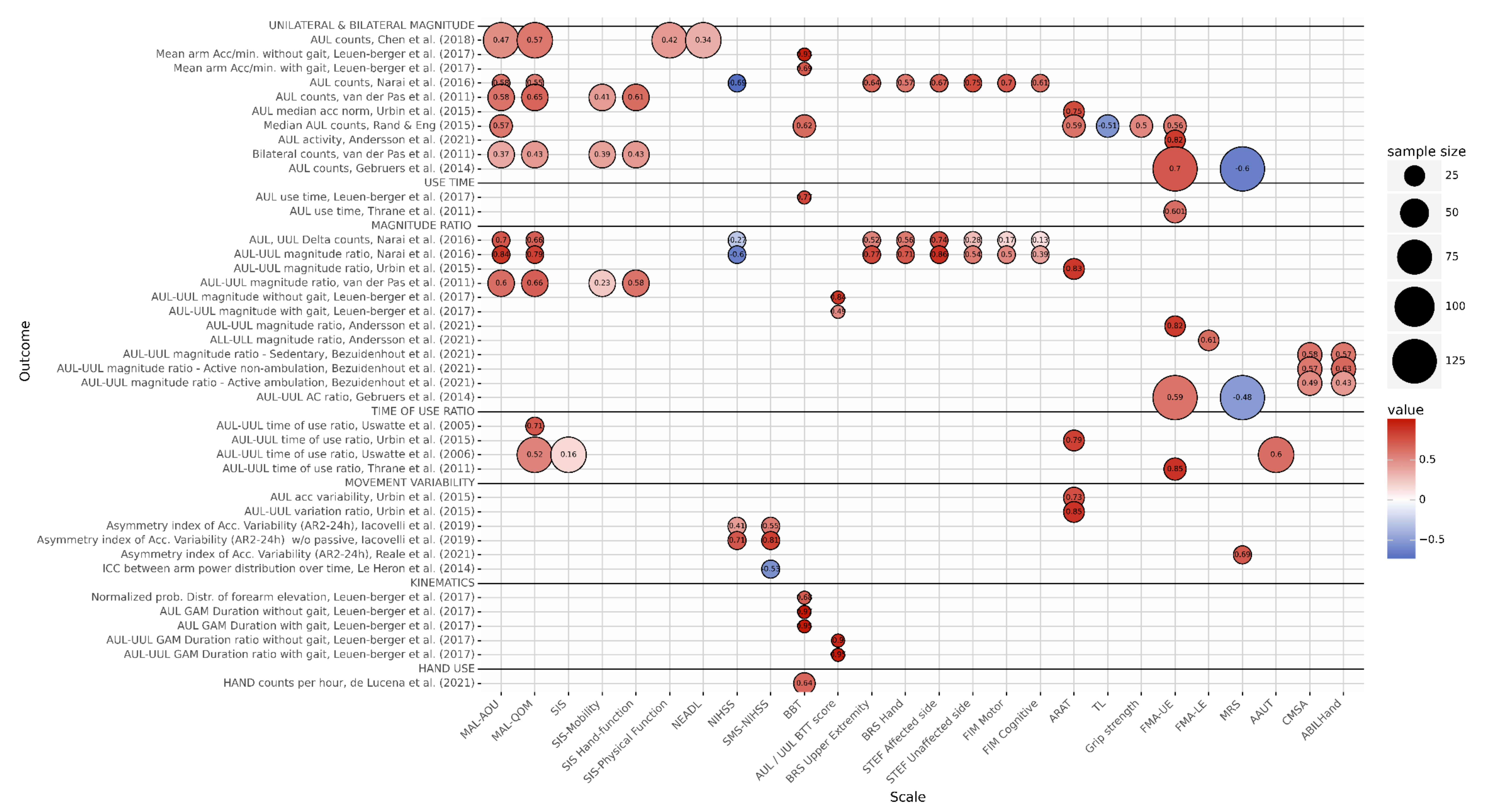
3.4.7. Comparison of Movement Measures with Clinical Assessment Tools
4. Discussion
Limitations and Future Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Reference | Experimental Design | Sensor & Placement | Measurement Task | Population (Mean ± std) | Clinical Measures | Sensor Based Measures | Results |
|---|---|---|---|---|---|---|---|
| Held et al. [31] | Observational, prospective cohort study |
| Recording during clinical assessments + 3 h recording during ADL, at: T1: 2 wks. before discharge T2: right after discharge T3: 4 wks. after discharge | Stroke: N = 4 Age: 48–55 y TAS: 5.25 ± 4.08 m. Mild-to-severe UL impairment (FMA-UE, ARAT) | FMA-UE, ARAT |
|
|
| Held et al. [32] | Observational, prospective cohort study | See [23] | See [23] | See [23] | See [23] |
|
|
| Iacovelli et al. [33] | Observational, Cross-sectional |
| 24 h continuous recording in clinic | Stroke: N = 20 Age: 69.2 ± 10.1 y TAS: 3.3 ± 1.6 d, AcuteHealthy control: N = 17 Age: 70.4 ± 7.3 y | (SMS-)NIHSS |
|
|
| Lucas et al. [43] | Observational, Cross-sectional |
| >7 d continuous recording in hospital | Stroke: N = 4 Age: 51.7 ± 13.2 y TAS: Not reported (Acute) | Oxford Grading Motor Scale |
|
|
| Narai et al. [10] | Observational, Cross-sectional |
| 24 h continuous recording in clinic | Stroke: N = 19 Age: 77 ± 6 y TAS: 17 ± 7 d | MAL-AOU and -QOL NIHSS BRS STEF FIM |
|
|
| Prajapati et al. [21] | Observational, Cross-sectional |
| 8 h continuous recording in hospital, including therapy | Stroke: N = 16 Age: 59.7 ± 15.3 y TAS: 37.8 ± 24.7 d | CMSABBS |
|
|
| Rand & Eng [5] | Observational, prospective cohort study |
| Stroke: 3 d continuous recording at: T1: first rehabilitation week, T2: 3 weeks after start rehabilitation. Healthy controls: 5 d continuous recording. | Stroke ambulant: N = 27Age: 64.3 ± 13.4 y TAS: 33.3 ± 19.2 dStroke Wheelchair users: N = 33Age: 58.2 ± 12.8 yTAS: 33.5 ± 22.1 d Healthy Controls: N = 40 Age: 71.3 ± 3.8 y | FMA-UE, ARAT BBT 10 MWT 6 MWT FIM | Mean daily use:
|
|
| Urbin et al. [25] | Observational, prospective cohort study |
| 22 h continuous recording: T1: after pre and T2: posttest inpatients T3: after 24th training session + recording during 24th training session (outpatients). | Stroke inpatients: N = 8 Age: 56 ± 10.4 y TAS: <30 d Stroke outpatients: N = 27 Age: 62 ± 9.4 y TAS: >6 m | ARAT NIHSS |
|
|
| Sanchez et al. [23] | Observational, prospective cohort study |
| 8 h continuous recording at: T1: TAS 1 w T2: TAS 12 w T3: TAS 48 w | Stroke: N = 23 Age: 58.13 ± 12.58 y TAS: ~1 w Healthy Controls: N = 20 Age: 55.35 ± 12.70 y | -- |
|
Walking
|
| Thrane et al. [24] | Observational, Cross-sectional |
| 24 h continuous recording. Car driving, sleeping data excluded. | Stroke: N = 31 Age: 65 ± 14 y TAS: 10.6 ± 6 d | FM Sunnaas ADL-index 5STS NIHSS |
| Average UUL use: 4.5 h ± 1.7 Average AUL use: 3 h ± 1.7 h Arm movement ratio: 1.5 (1.1–2.0) (Median, IQR) Correlations between 5STS and FMA rho = −0.529 ** AUL use time rho = −0.627 *** Arm movement ratio rho = −0.643 *** Correlations between FMA and AUL use time rho = 0.601 *** Arm movement ratio rho = −0.851 *** Latter supported by regression analysis: β = −0.05 ***. |
| Waddell et al. [30] | Observational, prospective cohort study |
| 24 h continuous recording at T1: TAS 2 w T2: TAS 4 w T3: TAS 6 w T4: TAS 8 w T5: TAS 12 w | Stroke: N = 22 Age: 68.7 ± 9.9 y TAS: <2 w | ARAT MoCA SAFE |
|
|
| Andersson et al. [34] | Observational, Cross-sectional |
| 2 sessions of 48 h recording in a rehabilitation clinic. Only daytime activity (8 h-20 h) was used. | Stroke: N = 26 Age: 55.4 ± 11.9 y TAS: 56 ± 24 d. Mild-to-severe impairment (FMA-UE/LE) | FMA-UE, FMA-LE, modified Ashworth Scale, 10 MWT, MRS |
| Sensor based measures correlated with with clinical measures:
|
| Reale et al. [38] | Observational, prospective cohort study |
| T1 (TAS 48–72 h): 24 h continuous recording T2 (TAS 90 d): MRS evaluation | Stroke: N = 20 Age: 69.2 ± 10.1 y TAS: 48–72 h | NIHSS MRS ASPECTS |
|
|
| Regterschot et al. [39] | Observational, prospective cohort study |
| Continuous recording for one week (only during walking hours for the wrist sensors) At: T1: TAS 3 w (rehabilitation center) T2: TAS 12 w (rehabilitation center or home depending on the patient) T3: TAS 26 w (home) | Stroke: N = 33 Age: 57.3 ± 8.5 y TAS: 3 w (NIHSS 5 A/B or 6 A/B 4 ≥ score > 0) | NIHSS FMA-UE | Using the thigh sensor to select only sitting and standing periods, mean daily values for:
| Change in time of the sensor measures:
|
| Le Heron et al. [40] | Observational, prospective cohort study |
| 1 h minimal recording in clinic at: T1: 54 h (median, 47–100) T2: T1 + 24 h. | ST: N = 20 Age: Median 77 y, IQR 59–82 y TAS: (T1) 54 h (median, range 47–100) Mild-to-moderate stroke severity (NIHSS) HC: N = 10 Age: Median 64 y, IQR 48–71 y | (SMS-)NIHSS | ICC of time-matched series of Acc. spectral power for both arms. | Correlation between NIHSS at T1 and the magnitude of ICC: rho = −0.53 *. The optimal diagnostic threshold for ICC magnitude was 0.7. At this threshold, ROC curve analysis using the ICC magnitude to distinguish stroke patients from controls yielded an AUC of 0.84 |
| Gebruers et al. [42] | Observational, prospective cohort study | Triaxial ACC (ambulatory monitoring). Both wrists. | T1: (<1 w after stroke) At least 24 h continuous recording. T2: T1 + 3 m, MRS assessment. | Stroke: N = 129 Age: 70 ± 11.4 y TAS: <1 w, median 1 d | NIHSS, FMA-UE (T1, T2), MRS (T2) | AUL AC AUL/UUL AC ratio | Correlation between: FMA-UE (T1): FMA-UE (T2) r = 0.69 * MRS: r = −0.66 * AUL AC: FMA-UE (T2) r = 0.70 * MRS: r = −0.60 * AUL/UUL AC ratio: FMA-UE (T2) r = 0.59 * MRS: r = −0.48 * |
| Reference | Experimental Design | Sensor & Placement | Measurement Task | Population (Mean ± std) | Clinical Measures | Sensor Based Measures | Results |
|---|---|---|---|---|---|---|---|
| Bailey et al. [8] | Observational, Cross-sectional |
| 24 h continuous recording during ADLHealthy vs. Stroke | Stroke: N = 48 Age: 59.7 ± 10.9 y TAS: >6 m ARAT = 31.3 ± 11.9 Healthy Controls: N = 74 Age: 54.3 ± 11.3 y | -- |
|
|
| Chen et al. [9] | Observational, prospective cohort study |
| 72 h continuous recording during ADL, except when bathing (T1) Pre and (T2) post 4-week rehabilitation intervention | Stroke: N = 82 N = Age: 55.3 ± 10.71 y TAS: 20.46 ± 13.43 m Mild-to-moderate UL impairment | MAL-AOU MAL-QOM SIS (physical function subscale) NEADL | AUL AC (Action4 software) |
|
| Leuenberger et al. [19] | Observational, Cross-sectional |
| 48 h continuous recording during ADL | Stroke: N = 10 Age: 52.7 ± 13.6 year TAS: 21.6 ± 10.6 w | BBT |
| Correlation between ratio of AUL AC and BTT incl. walking r = 0.69 * excl. walking r = 0.93 ***
|
| Michielsen et al. [20] | Observational, Cross-sectional |
| 24 h continuous recording during ADL | Stroke: N = 38 Age: 56.6 ± 12.6 y TAS: 4.5 ± 3.2 y Healthy Control: N = 18 Age: 48.1 ± 10.9 y | -- |
|
|
| Punt et al. [11] | Observational, Cross-sectional |
| 7 d continuous recording during ADL | Stroke: N = 40 of which Fall: N = 15 Age: 64.6 ± 8.5 y TAS: 113 ± 109 m NFall: N = 25 Age: 58.4 ± 14.3 y TAS: 71.8 ± 65 m | 10 MWT TUG BBS | Gait characteristics:
|
|
| Rand & Eng [22] | Observational, prospective cohort study |
| 3 d continuous recording at: T1: 4 w T2: 12 m | Stroke: N = 32 Age: 58.1 ± 12.4 y TAS (T1): 29.6 ± 15.5 d | MAL-AOU FMA-UE ARAT TL BBT Grip strength | Mean AC AUL |
|
| Uswatte et al. [26] | Observational, prospective cohort study |
| 72 h continuous recording at: CIMT rehabilitation group: (T1) Pre and (T2) post CIMT rehab (2 w).Normal rehabilitation group: T2 = T1 + 2 w. | Stroke CIMT: N = 10 Age: 61.4 ± 20.0 y TAS: >1 y Stroke normal rehabilitation group: N = 10 Age: 63.7 ± 13.5 y TAS: >1 y UL impairment: Mild to moderate (N = 19), moderate to severe (N = 1) | MAL-QOM |
|
|
| Uswatte et al. [27] | Observational, prospective cohort study |
| See 24 | Stroke intervention: N = 82 Age: 63.0 ± 12.8 y TAS: >1 y Stroke control: N = 87 Age: 64.2 ± 12.7 y TAS: >1 y Mild to moderate UL impairment | AAUT MAL-QOM SIS |
|
|
| van der Pas et al. [28] | Observational, Cross-sectional |
| 60 h continuous recording during ADL | Stroke: N = 45 Age: 59.4 ± 9.2 y TAS: 2.0 ± 1.6 y | MAL-AOU MAL-QOM SIS-mobility SIS-hand function |
|
|
| Vega-Gonzalez et al. [44] | Observational, Cross-sectional |
| 8 h continuous recording during ADL | Stroke: N = 10 Age: 55–79 y TAS: >1 y Healthy Controls: N = 10 Age: 23–57 y | -- |
|
|
| Vega-González & Granat [29] | Observational, Cross-sectional |
| 8 h continuous recording during ADL | Stroke: N = 10 Age: 56–80 y TAS: >1 y Healthy Controls: N = 10 Age: 22–35 y | -- |
|
|
| Bezuidenhout et al. [35] | Observational, Cross-sectional |
| Part 1: (HC, Stroke) Simulated ADL in a controlled environment. Part 2: (Stroke) Free ADL during waking hours for three consecutive days. | Stroke: N = 37 Age: 64.5 ± 11.7 y TAS: 3.0 ± 4.2 y (>=3 m) HC: N = 32 Age: 70.5 ± 10.4 y | MoCA ABILHand Katz ADL Index NIHSS CMSA | Vector Magnitude ratio (Wrists) |
|
| Ann et al. [45] | Observational, Cross-sectional |
| 2 Parts: Part 1: 15 scripted activities Part 2: Free ADL during waking hours for 7 (ST) and 3 (HC) days. | Part 1: Stroke: N = 5 Age: 35.4 ± 13.21 y TAS: 45.8 ± 79.1 m (>=3 m) HC: N = 10 Age: 23.2 ± 3.21 y Part 2: Stroke: N = 5 Age: range 30–60 TAS: 2.0 ± 2.5 y (>=3 m) Mild-to-moderate impairment (FMA-UE) HC: N = 5 Age: not reported | FMA-UE] MAL, AAUT | Gross arm movements |
|
| de Lucena et al. [36] | Observational, Cross-sectional (HC, Group 1), prospective (Group 2) |
| Group 0 (HC): scripted hand and arm activities. Group 1: Clinical assessments, scripted activities and one day (walking hours) of free ADL. Group 2: Three times 1 day (walking hours) of free ADL. T1: first visit T2: T1 + 4 w T3: T1 + 4 m | Group 0 HC: N = 8 Age: 26.1 ± 3.0 SD Group 1 Stroke: N = 9 Age: 68 ± 9 y TAS: 30 ± 23 m Group 2 Stroke: N = 20 Age: 57 ± 15 y TAS: 40 ± 33 | BBT, FMA-UE |
|
|
| Flury et al. [37] | Observational, Cross-sectional |
| Several hours of free ADL. (5.03 ± 1.1 h) | Stroke: N = 15 Age: 59.9 ± 9.8 y TAS: 6.5 ± 7.2 y (>3 m) | NIHSS FMA-UE MAL ARAT 10 MWT TUG BBS MRS Barthel Index | Activity time Number of steps Arm activity time Arm activity time ratio |
|
| Liao et al. [41] | Observational, Cross-sectional | Triaxial ACC (MicroMiniMotion logger, Ambulatory Monitoring). Both wrists | 6 days of continuous recording (3 before, 3 after the intervention), except when in contact with large amounts of water | Stroke: Group 1: Robot assisted therapy N = 10 Age: 55.5 ± 11.1 y TAS: 33.4 ± 13.39 m Group 2: Control N = 10 Age: 54.56 ± 8.20 y TAS: 22.20 ± 17.47 m | FMA FIM MAL-AOU MAL-QOM ABILHand | Arm activity ratio | Arm activity ratio (pre / post intervention) change: Group 1: pre: 0.71 ± 0.99, post 0.76 ± 0.10 Group 2: pre: 0.69 ± 0.12, post 0.69 ± 0.11
|
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American heart association/American stroke association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beroerte|Cijfers & Context|Sterfte. Available online: https://www.volksgezondheidenzorg.info (accessed on 1 August 2020).
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, S.-M.; Studenski, S.; Duncan, P.W.; Perera, S. Persisting Consequences of Stroke Measured by the Stroke Impact Scale. Stroke 2002, 33, 1840–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rand, D.; Eng, J.J. Disparity between functional recovery and daily use of the upper and lower extremities during subacute stroke rehabilitation. Neurorehabilit. Neural Repair 2012, 26, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, K.; Steward, J. Sroke recovery: He can but does he? Rheumatology 1979, 18, 43–48. [Google Scholar] [CrossRef]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Bailey, R.; Klaesner, J.W.; Lang, C. E Quantifying real-world upper-limb activity in nondisabled adults and adults with chronic stroke. Neurorehabilit. Neural Repair 2015, 29, 969–978. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-L.; Lin, K.-C.; Hsieh, Y.-W.; Wu, C.-Y.; Liing, R.-J.; Chen, C.-L. A study of predictive validity, responsiveness, and minimal clinically important difference of arm accelerometer in real-world activity of patients with chronic stroke. Clin. Rehabil. 2018, 32, 75–83. [Google Scholar] [CrossRef]
- Narai, E.; Hagino, H.; Komatsu, T.; Togo, F. Accelerometer-Based Monitoring of Upper Limb Movement in Older Adults with Acute and Subacute Stroke. J. Geriatr. Phys. Ther. 2016, 39, 171–177. [Google Scholar] [CrossRef]
- Punt, M.; Bruijn, S.M.; Wittink, H.; van de Port, I.G.; van Dieen, J.H. Do clinical assessments, steady-state or daily-life gait characteristics predict falls in ambulatory chronic stroke survivors? J. Rehabil. Med. 2017, 49, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Noorkõiv, M.; Rodgers, H.; Price, C.I. Accelerometer measurement of upper extremity movement after stroke: A systematic review of clinical studies. J. Neuroeng. Rehabil. 2014, 11, 144. [Google Scholar] [CrossRef] [Green Version]
- Johansson, D.; Malmgren, K.; Alt Murphy, M. Wearable sensors for clinical applications in epilepsy, Parkinson’s disease, and stroke: A mixed-methods systematic review. J. Neurol. 2018, 265, 1740–1752. [Google Scholar] [CrossRef] [Green Version]
- Gebruers, N.; Vanroy, C.; Truijen, S.; Engelborghs, S.; De Deyn, P.P. Monitoring of Physical Activity After Stroke: A Systematic Review of Accelerometry-Based Measures. Arch. Phys. Med. Rehabil. 2010, 91, 288–297. [Google Scholar] [CrossRef]
- Fini, N.A.; Holland, A.E.; Keating, J.; Simek, J.; Bernhardt, J. How is physical activity monitored in people following stroke? Disabil. Rehabil. 2014, 37, 1–15. [Google Scholar] [CrossRef]
- Peters, D.M.; O’Brien, E.S.; Kamrud, K.E.; Roberts, S.M.; Rooney, T.A.; Thibodeau, K.P.; Balakrishnan, S.; Gell, N.; Mohapatra, S. Utilization of wearable technology to assess gait and mobility post-stroke: A systematic review. J. Neuroeng. Rehabil. 2021, 18, 1–18. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Leuenberger, K.; Gonzenbach, R.; Wachter, S.; Luft, A.; Gassert, R. A method to qualitatively assess arm use in stroke survivors in the home environment. Med. Biol. Eng. Comput. 2016, 55, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Michielsen, M.E.; Selles, R.W.; Stam, H.J.; Ribbers, G.; Bussmann, J.B. Quantifying Nonuse in Chronic Stroke Patients: A Study into Paretic, Nonparetic, and Bimanual Upper-Limb Use in Daily Life. Arch. Phys. Med. Rehabil. 2012, 93, 1975–1981. [Google Scholar] [CrossRef]
- Prajapati, S.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. A novel approach to ambulatory monitoring: Investigation into the quantity and control of everyday walking in patients with subacute stroke. Neurorehabilit. Neural Repair 2010, 25, 6–14. [Google Scholar] [CrossRef]
- Rand, D.; Eng, J.J. Predicting Daily Use of the Affected Upper Extremity 1 Year after Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Bussmann, J.; Janssen, W.; Horemans, H.; Chastin, S.; Heijenbrok, M.; Stam, H. Accelerometric assessment of different dimensions of natural walking during the first year after stroke: Recovery of amount, distribution, quality and speed of walking. J. Rehabil. Med. 2015, 47, 714–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thrane, G.; Emaus, N.; Askim, T.; Anke, A. Arm use in patients with subacute stroke monitored by accelerometry: Association with motor impairment and influence on self-dependence. J. Rehabil. Med. 2011, 43, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbin, M.A.; Waddell, K.J.; Lang, C.E. Acceleration Metrics Are Responsive to Change in Upper Extremity Function of Stroke Survivors. Arch. Phys. Med. Rehabil. 2014, 96, 854–861. [Google Scholar] [CrossRef] [Green Version]
- Uswatte, G.; Foo, W.L.; Olmstead, H.; Lopez, K.; Holand, A.; Simms, L.B. Ambulatory Monitoring of Arm Movement Using Accelerometry: An Objective Measure of Upper-Extremity Rehabilitation in Persons with Chronic Stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1498–1501. [Google Scholar] [CrossRef]
- Uswatte, G.; Giuliani, C.; Winstein, C.; Zeringue, A.; Hobbs, L.; Wolf, S.L. Validity of Accelerometry for Monitoring Real-World Arm Activity in Patients with Subacute Stroke: Evidence from the Extremity Constraint-Induced Therapy Evaluation Trial. Arch. Phys. Med. Rehabil. 2006, 87, 1340–1345. [Google Scholar] [CrossRef]
- van der Pas, S.C.; Verbunt, J.A.; Breukelaar, D.E.; van Woerden, R.; Seelen, H.A. Assessment of Arm Activity Using Triaxial Accelerometry in Patients with a Stroke. Arch. Phys. Med. Rehabil. 2011, 92, 1437–1442. [Google Scholar] [CrossRef]
- Vega-González, A.; Granat, M. Continuous monitoring of upper-limb activity in a free-living environment. Arch. Phys. Med. Rehabil. 2005, 86, 541–548. [Google Scholar] [CrossRef]
- Waddell, K.J.; Strube, M.J.; Tabak, R.G.; Haire-Joshu, D.; Lang, C.E. Upper Limb Performance in Daily Life Improves Over the First 12 Weeks Poststroke. Neurorehabilit. Neural Repair 2019, 33, 836–847. [Google Scholar] [CrossRef]
- Held, J.P.O.; Klaassen, B.; Eenhoorn, A.; Van Beijnum, B.-J.F.; Buurke, J.H.; Veltink, P.H.; Luft, A.R. Inertial Sensor Measurements of Upper-Limb Kinematics in Stroke Patients in Clinic and Home Environment. Front. Bioeng. Biotechnol. 2018, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Held, J.P.O.; Veltink, P.H.; van Meulen, F.B.; Luft, A.R.; Buurke, J.H. Measurement of upper limb function during daily life after stroke. In International Conference on NeuroRehabilitation; Springer: Cham, Switzerland, 2019; Volume 21, pp. 307–311. [Google Scholar]
- Iacovelli, C.; Caliandro, P.; Rabuffetti, M.; Padua, L.; Simbolotti, C.; Reale, G.; Ferrarin, M.; Rossini, P.M. Actigraphic measurement of the upper limbs movements in acute stroke patients. J. Neuroeng. Rehabil. 2019, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Andersson, S.; Danielsson, A.; Ohlsson, F.; Wipenmyr, J.; Murphy, M. Arm impairment and walking speed explain real-life activity of the affected arm and leg after stroke. J. Rehabil. Med. 2021, 53, jrm00210. [Google Scholar] [CrossRef]
- Bezuidenhout, L.; Joseph, C.; Einarsson, U.; Thurston, C.; Hagströmer, M.; Moulaee Conradsson, D.M. Accelerometer assessed upper limb activity in people with stroke: A validation study considering ambulatory and non-ambulatory activities. Disabil. Rehabil. 2021. [Google Scholar] [CrossRef]
- de Lucena, D.S.; Rowe, J.; Chan, V.; Reinkensmeyer, D.J. Magnetically Counting Hand Movements: Validation of a Calibration-Free Algorithm and Application to Testing the Threshold Hypothesis of Real-World Hand Use after Stroke. Sensors 2021, 21, 1502. [Google Scholar] [CrossRef]
- Flury, D.; Massé, F.; Paraschiv-Ionescu, A.; Aminian, K.; Luft, A.R.; Gonzenbach, R. Clinical value of assessing motor performance in postacute stroke patients. J. Neuroeng. Rehabil. 2021, 18, 1–10. [Google Scholar] [CrossRef]
- Reale, G.; Giovannini, S.; Iacovelli, C.; Castiglia, S.; Picerno, P.; Zauli, A.; Rabuffetti, M.; Ferrarin, M.; Maccauro, G.; Caliandro, P. Actigraphic Measurement of the Upper Limbs for the Prediction of Ischemic Stroke Prognosis: An Observational Study. Sensors 2021, 21, 2479. [Google Scholar] [CrossRef]
- Regterschot, G.R.H.; Bussmann, J.B.J.; Fanchamps, M.H.J.; Meskers, C.G.M.; Ribbers, G.M.; Selles, R.W. Objectively measured arm use in daily life improves during the first 6 months poststroke: A longitudinal observational cohort study. J. Neuroeng. Rehabil. 2021, 18, 1–10. [Google Scholar] [CrossRef]
- Le Heron, C.; Fang, K.; Gubbi, J.; Churilov, L.; Palaniswami, M.S.; Davis, S.; Yan, B. Wireless Accelerometry is Feasible in Acute Monitoring of Upper Limb Motor Recovery after Ischemic Stroke. Cerebrovasc. Dis. 2014, 37, 336–341. [Google Scholar] [CrossRef]
- Liao, W.-W.; Wu, C.-Y.; Hsieh, Y.-W.; Lin, K.-C.; Chang, W.-Y. Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic stroke: A randomized controlled trial. Clin. Rehabil. 2011, 26, 111–120. [Google Scholar] [CrossRef]
- Gebruers, N.; Truijen, S.; Engelborghs, S.; De Deyn, P.P. Prediction of Upper Limb Recovery, General Disability, and Rehabilitation Status by Activity Measurements Assessed by Accelerometers or the Fugl-Meyer Score in Acute Stroke. Am. J. Phys. Med. Rehabil. 2014, 93, 245–252. [Google Scholar] [CrossRef]
- Lucas, A.; Hermiz, J.; Labuzetta, J.; Arabadzhi, Y.; Karanjia, N.; Gilja, V. Use of Accelerometry for Long Term Monitoring of Stroke Patients. IEEE J. Transl. Eng. Health Med. 2019, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Vega-Gonzalez, A.; Bain, B.J.; Granat, M.H. Measuring continuous real-world upper-limb activity. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; Volume 2005, pp. 3542–3545. [Google Scholar] [CrossRef]
- David, A.; ReethaJanetSureka, S.; Gayathri, S.; Annamalai, S.J.; Samuelkamleshkumar, S.; Kuruvilla, A.; Magimairaj, H.P.; Varadhan, S.; Balasubramanian, S. Quantification of the relative arm use in patients with hemiparesis using inertial measurement units. J. Rehabil. Assist. Technol. Eng. 2021, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, J.; Hayward, K.; Kwakkel, G.; Ward, N.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; A Boyd, L.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Taub, E.; Miller, N.E.; Novack, T.A.; Cook, E.W., III; Fleming, W.C.; Nepomuceno, C.S.; Connell, J.S.; Crago, J.E. Technique to improve chronic motor deficit after stroke. Arch. Phys. Med. Rehabil. 1993, 74, 347–354. [Google Scholar]
- Kasner, S.E. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006, 5, 603–612. [Google Scholar] [CrossRef]
- Murphy, M.A.; Resteghini, C.; Feys, P.; Lamers, I. An overview of systematic reviews on upper extremity outcome measures after stroke. BMC Neurol. 2015, 15, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Mayagoitia, R.E.; Nene, A.V.; Veltink, P. Accelerometer and rate gyroscope measurement of kinematics: An inexpensive alternative to optical motion analysis systems. J. Biomech. 2001, 35, 537–542. [Google Scholar] [CrossRef]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 1–21. [Google Scholar] [CrossRef]
- Kobsar, D.; Osis, S.T.; Phinyomark, A.; Boyd, J.E.; Ferber, R. Reliability of gait analysis using wearable sensors in patients with knee osteoarthritis. J. Biomech. 2016, 49, 3977–3982. [Google Scholar] [CrossRef]
- Zhang, W.; Smuck, M.; Legault, C.; Ith, M.A.; Muaremi, A.; Aminian, K. Gait Symmetry Assessment with a Low Back 3D Accelerometer in Post-Stroke Patients. Sensors 2018, 18, 3322. [Google Scholar] [CrossRef] [Green Version]
- Buckley, C.; Micó-Amigo, M.E.; Dunne-Willows, M.; Godfrey, A.; Hickey, A.; Lord, S.; Rochester, L.; Del Din, S.; Moore, S.A. Gait Asymmetry Post-Stroke: Determining Valid and Reliable Methods Using a Single Accelerometer Located on the Trunk. Sensors 2020, 20, 37. [Google Scholar] [CrossRef] [Green Version]
- van den Akker-Scheek, I.; Zijlstra, W.; Groothoff, J.W.; Bulstra, S.K.; Stevens, M. Physical functioning before and after total hip arthroplasty: Perception and performance. Phys. Ther. 2008, 88, 712–719. [Google Scholar] [CrossRef] [Green Version]
- Jarque-Bou, N.; Sancho-Bru, J.; Vergara, M. A Systematic Review of EMG Applications for the Characterization of Forearm and Hand Muscle Activity during Activities of Daily Living: Results, Challenges, and Open Issues. Sensors 2021, 21, 3035. [Google Scholar] [CrossRef]
- Neckel, N.; Pelliccio, M.; Nichols, D.; Hidler, J. Quantification of functional weakness and abnormal synergy patterns in the lower limb of individuals with chronic stroke. J. Neuroeng. Rehabil. 2006, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Buurke, J.H.; Nene, A.V.; Kwakkel, G.; Erren-Wolters, V.; Ijzerman, M.J.; Hermens, H.J. Recovery of Gait After Stroke: What Changes? Neurorehabilit. Neural Repair 2008, 22, 676–683. [Google Scholar] [CrossRef]
- Massé, F.; Gonzenbach, R.R.; Arami, A.; Paraschiv-Ionescu, A.; Luft, A.R.; Aminian, K. Improving activity recognition using a wearable barometric pressure sensor in mobility-impaired stroke patients. J. Neuroeng. Rehabil. 2015, 12, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Masse, F.; Gonzenbach, R.; Paraschiv-Ionescu, A.; Luft, A.R.; Aminian, K. Wearable Barometric Pressure Sensor to Improve Postural Transition Recognition of Mobility-Impaired Stroke Patients. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 1210–1217. [Google Scholar] [CrossRef] [Green Version]
- Saporito, S.; Brodie, A.M.D.; Delbaere, K.; Hoogland, J.; Nijboer, H.; Rispens, S.M.; Spina, G.; Stevens, M.; Annegarn, J. Remote timed up and go evaluation from activities of daily living reveals changing mobility after surgery. Physiol. Meas. 2019, 40, 035004. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernaldo de Quirós, M.; Douma, E.H.; van den Akker-Scheek, I.; Lamoth, C.J.C.; Maurits, N.M. Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review. Sensors 2022, 22, 1050. https://doi.org/10.3390/s22031050
Bernaldo de Quirós M, Douma EH, van den Akker-Scheek I, Lamoth CJC, Maurits NM. Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review. Sensors. 2022; 22(3):1050. https://doi.org/10.3390/s22031050
Chicago/Turabian StyleBernaldo de Quirós, Mariano, E.H. Douma, Inge van den Akker-Scheek, Claudine J. C. Lamoth, and Natasha M. Maurits. 2022. "Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review" Sensors 22, no. 3: 1050. https://doi.org/10.3390/s22031050
APA StyleBernaldo de Quirós, M., Douma, E. H., van den Akker-Scheek, I., Lamoth, C. J. C., & Maurits, N. M. (2022). Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review. Sensors, 22(3), 1050. https://doi.org/10.3390/s22031050