
The Association between Tensiomyography and Elastography Stiffness Measurements in Lower Limb Skeletal Muscles

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
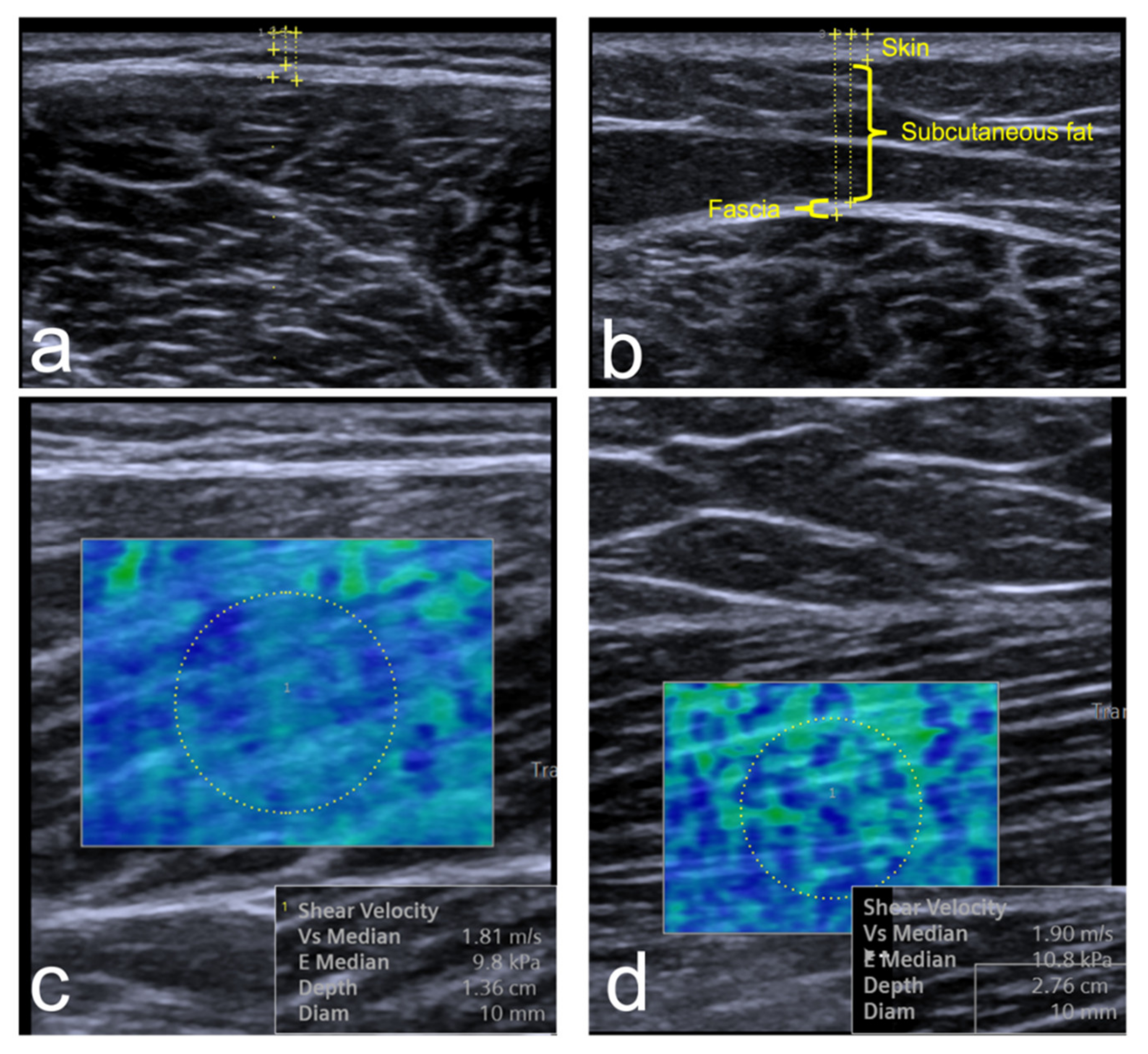
2.2. Elastography
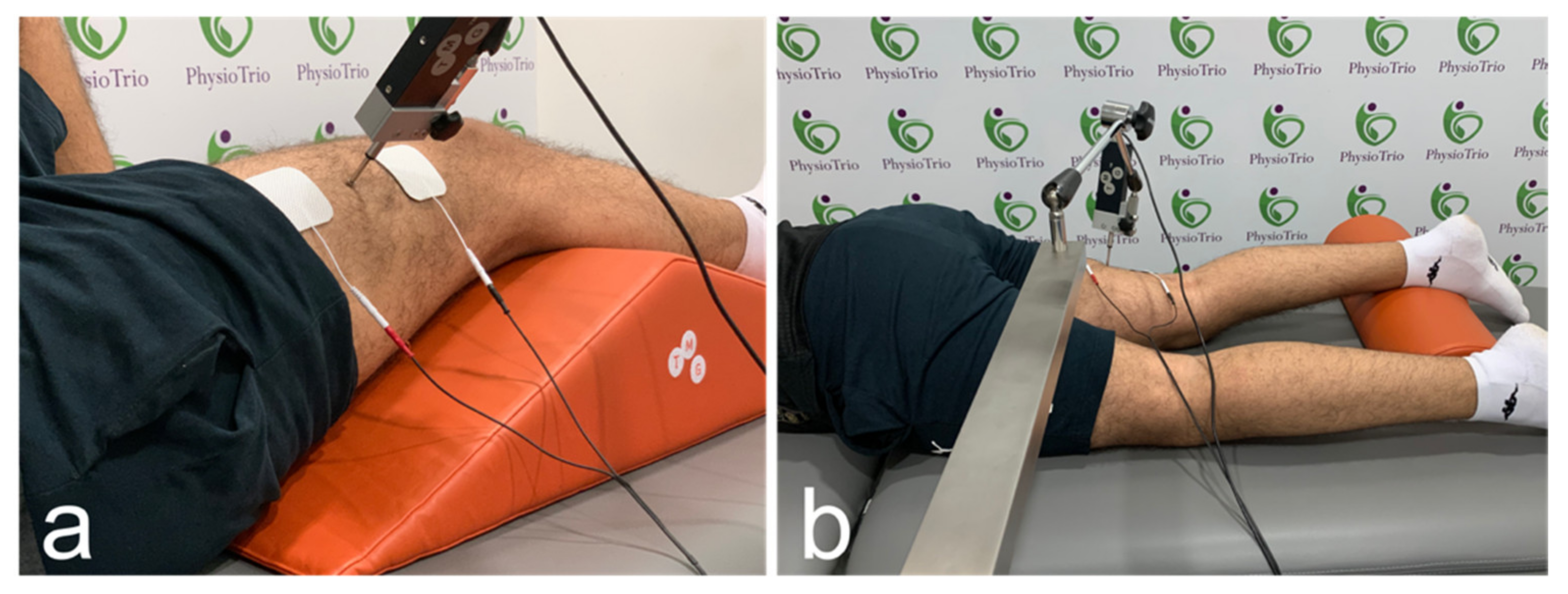
2.3. Tensiomyography
2.4. Physical Activity
2.5. Statistical Methodology
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seyfarth, A.; Geyer, H.; Günther, M.; Blickhan, R. A movement criterion for running. J. Biomech. 2002, 35, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.J.; Crowell, H.P.; Davis, I.M. Lower extremity stiffness: Implications for performance and injury. Clin. Biomech. 2003, 18, 511–517. [Google Scholar] [CrossRef]
- Pruyn, E.C.; Watsford, M.L.; Murphy, A.J.; Pine, M.J.; Spurrs, R.W.; Cameron, M.L.; Johnston, R.J. Relationship between leg stiffness and lower body injuries in professional Australian football. J. Sports Sci. 2012, 30, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Watsford, M.L.; Murphy, A.J.; McLachlan, K.A.; Bryant, A.L.; Cameron, M.L.; Crossley, K.M.; Makdissi, M. A Prospective Study of the Relationship between Lower Body Stiffness and Hamstring Injury in Professional Australian Rules Footballers. Am. J. Sports Med. 2010, 38, 2058–2064. [Google Scholar] [CrossRef]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; Tan, A.L.; O’Connor, P.; Emery, P.; Wakefield, R.J. The effect of ageing on shear wave elastography muscle stiffness in adults. Aging Clin. Exp. Res. 2019, 31, 1755–1763. [Google Scholar] [CrossRef] [Green Version]
- Taş, S.; Korkusuz, F.; Erden, Z. Neck Muscle Stiffness in Participants with and without Chronic Neck Pain: A Shear-Wave Elastography Study. J. Manip. Physiol. Ther. 2018, 41, 580–588. [Google Scholar] [CrossRef]
- Pichiecchio, A.; Alessandrino, F.; Bortolotto, C.; Cerica, A.; Rosti, C.; Raciti, M.V.; Rossi, M.; Berardinelli, A.; Baranello, G.; Bastianello, S.; et al. Muscle ultrasound elastography and MRI in preschool children with Duchenne muscular dystrophy. Neuromuscul. Disord. 2018, 28, 476–483. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; Tan, A.L.; O’Connor, P.; Emery, P.; Mackie, S.; Wakefield, R.J. Reduction in stiffness of proximal leg muscles during the first 6 months of glucocorticoid therapy for giant cell arteritis: A pilot study using shear wave elastography. Int. J. Rheum. Dis. 2019, 22, 1891–1899. [Google Scholar] [CrossRef]
- Snoj, Ž.; Wu, C.H.; Taljanovic, M.; Dumić-Čule, I.; Drakonaki, E.E.; Klauser, A.S. Ultrasound Elastography in Musculoskeletal Radiology: Past, Present, and Future. Semin. Musculoskelet. Radiol. 2020, 24, 156–166. [Google Scholar] [CrossRef]
- García-García, O.; Cuba-Dorado, A.; Álvarez-Yates, T.; Carballo-López, J.; Iglesias-Caamaño, M. Clinical utility of tensiomyography for muscle function analysis in athletes. Open Access J. Sports Med. 2019, 10, 49–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macgregor, L.; Hunter, A.M.; Orizio, C.; Fairweather, M.M.; Ditroilo, M. Assessment of Skeletal Muscle Contractile Properties by Radial Displacement: The Case for Tensiomyography. Sports Med. 2018, 48, 1607–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S. Theory and usage of tensiomyography and the analysis method for the patient with low back pain. J. Exerc. Rehabil. 2020, 16, 325–331. [Google Scholar] [CrossRef]
- García-Manso, J.M.; Rodriguez-Ruiz, D.; Rodríguez-Matoso, D.; De Saa, Y.; Sarmiento, S.; Quiroga, M. Assessment of muscle fatigue after an ultra-endurance triathlon using tensiomyography (TMG). J. Sports Sci. 2011, 29, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Alfuraih, A.; O’Connor, P.; Tan, A.L.; Hensor, E.; Emery, P.; Wakefield, R.J. An investigation into the variability between different shear wave elastography systems in muscle. Med. Ultrason. 2017, 19, 392–400. [Google Scholar] [CrossRef] [Green Version]
- Šimunič, B. Two-dimensional spatial error distribution of key tensiomyographic parameters. J. Biomech. 2019, 92, 92–97. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; O’Connor, P.; Hensor, E.; Tan, A.L.; Emery, P.; Wakefield, R.J. The effect of unit, depth, and probe load on the reliability of muscle shear wave elastography: Variables affecting reliability of SWE. J. Clin. Ultrasound 2018, 46, 108–115. [Google Scholar] [CrossRef]
- Jones, A.; Hind, K.; Wilson, H.V.; Johnson, M.I.; Francis, P. A standardised protocol for the assessment of lower limb muscle contractile properties in football players using Tensiomyography. Adv. Skelet. Muscle Funct. Assess. 2016, 1, 13–16. [Google Scholar]
- Carpenter, E.L.; Lau, H.A.; Kolodny, E.H.; Adler, R.S. Skeletal Muscle in Healthy Subjects versus Those withGNE-Related Myopathy: Evaluation with Shear-Wave US—A Pilot Study. Radiology 2015, 277, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Križaj, D.; Šimunič, B.; Žagar, T. Short-term repeatability of parameters extracted from radial displacement of muscle belly. J. Electromyogr. Kinesiol. 2008, 18, 645–651. [Google Scholar] [CrossRef]
- International Committee. Guidelines for the Data Processing and Analysis of the International Physical Activity Questionnaire, 2005. 2016. Available online: www.ipaq.ki.se (accessed on 2 September 2020).
- Helou, K.; El Helou, N.; Mahfouz, M.; Mahfouz, Y.; Salameh, P.; Harmouche-Karaki, M. Validity and reliability of an adapted arabic version of the long international physical activity questionnaire. BMC Public Health 2017, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Cè, E.; Longo, S.; Limonta, E.; Coratella, G.; Rampichini, S.; Esposito, F. Peripheral fatigue: New mechanistic insights from recent technologies. Eur. J. Appl. Physiol. 2020, 120, 17–39. [Google Scholar] [CrossRef] [PubMed]
- Ditroilo, M.; Hunter, A.; Haslam, S.; De Vito, G. The effectiveness of two novel techniques in establishing the mechanical and contractile responses of biceps femoris. Physiol. Meas. 2011, 32, 1315–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-García, O.; Cancela-Carral, J.M.; Martínez-Trigo, R.; Serrano-Gómez, V. Differences in the Contractile Properties of the Knee Extensor and Flexor Muscles in Professional Road Cyclists During the Season. J. Strength Cond. Res. 2013, 27, 2760–2767. [Google Scholar] [CrossRef] [PubMed]
- Pišot, R.; Narici, M.V.; Šimunič, B.; De Boer, M.; Seynnes, O.; Jurdana, M.; Biolo, G.; Mekjavić, I.B. Whole muscle contractile parameters and thickness loss during 35-day bed rest. Eur. J. Appl. Physiol. 2008, 104, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Eby, S.; Song, P.; Chen, S.; Chen, Q.; Greenleaf, J.F.; An, K.-N. Validation of shear wave elastography in skeletal muscle. J. Biomech. 2013, 46, 2381–2387. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Guo, J.-Y.; Cohen, J.H.; Parker, K.J. Quantifying the passive stretching response of human tibialis anterior muscle using shear wave elastography. Clin. Biomech. 2014, 29, 33–39. [Google Scholar] [CrossRef]
- Ateş, F.; Hug, F.; Bouillard, K.; Jubeau, M.; Frappart, T.; Couade, M.; Bercoff, J.; Nordez, A. Muscle shear elastic modulus is linearly related to muscle torque over the entire range of isometric contraction intensity. J. Electromyogr. Kinesiol. 2015, 25, 703–708. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; O’Connor, P.; Tan, A.L.; Hensor, E.M.A.; Ladas, A.; Emery, P.; Wakefield, R.J. Muscle shear wave elastography in idiopathic inflammatory myopathies: A case–control study with MRI correlation. Skelet. Radiol. 2019, 48, 1209–1219. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Lobo, C.; Diez-Vega, I.; Martínez-Pascual, B.; Fernández-Martínez, S.; de la Cueva-Reguera, M.; Garrosa-Martín, G.; Rodríguez-Sanz, D. Tensiomyography, sonoelastography, and mechanosensitivity differences between active, latent, and control low back myofascial trigger points: A cross-sectional study. Medicine 2017, 96, e6287. [Google Scholar] [CrossRef]
- Neamţu, M.C.; Rusu, L.; Rusu, P.F.; Neamţu, O.M.; Georgescu, D.; Iancău, M. Neuromuscular assessment in the study of structural changes of striated muscle in multiple sclerosis. Rom. J. Morphol. Embryol. 2011, 52, 1299–1303. [Google Scholar] [PubMed]
- Calvo-Lobo, C.; Díez-Vega, I.; García-Mateos, M.; Molina-Martín, J.J.; Díaz-Ureña, G.; Rodríguez-Sanz, D. Relationship of the skin and subcutaneous tissue thickness in the tensiomyography response: A novel ultrasound observational study. Rev. Da Assoc. Médica Bras. 2018, 64, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Z.; Guo, J.-Y.; Li, T.-J.; Zhou, Y.; Shi, W.; Zheng, Y.-P. Age and Sex Effects on the Active Stiffness of Vastus Intermedius under Isometric Contraction. BioMed Res. Int. 2017, 2017, 9469548. [Google Scholar] [CrossRef] [PubMed]
- Bortolotto, C.; Lungarotti, L.; Fiorina, I.; Zacchino, M.; Draghi, F.; Calliada, F. Influence of subjects’ characteristics and technical variables on muscle stiffness measured by shear wave elastosonography. J. Ultrasound 2017, 20, 139–146. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Vastus Lateralis | Biceps Femoris | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | ||
| Muscle stiffness (kPa) | 8.1 | 1.8 | 7.3, 8.9 | 10.8 | 1.5 | 10.2, 11.5 | <0.001 |
| Time of contraction (Tc) (ms) | 26.6 | 7.3 | 23.3, 29.8 | 35.9 | 18.0 | 28.9, 43.9 | 0.050 |
| Sustain time (Ts) (ms) * | 53.7 | 52.8 | 50.7, 81.6 | 159.1 | 92.3 | 128.4, 202.2 | <0.001 |
| Relaxation time (Tr) (ms) * | 20.0 | 28.9 | 16.1, 37.9 | 52.0 | 65.1 | 38.9, 89.9 | 0.007 |
| Delay time (Td) (ms) | 23.1 | 2.1 | 22.1, 24.0 | 25.1 | 5.8 | 22.6, 27.7 | 0.17 |
| Maximal displacement (Dm) (mm) | 3.7 | 1.3 | 2.1, 4.2 | 3.7 | 3.4 | 2.2, 5.2 | 0.90 |
| Muscle thickness (mm) | 22.2 | 3.6 | 20.6, 23.8 | 29.5 | 5.1 | 27.2, 31.8 | <0.001 |
| Skin thickness (mm) | 1.2 | 0.3 | 1.1, 1.4 | 1.4 | 0.4 | 1.2, 1.6 | 0.006 |
| Subcutaneous fat thickness (mm) | 6.6 | 3.2 | 5.2, 8.1 | 7.2 | 2.6 | 6.1, 8.4 | 0.129 |
| Fascia thickness (mm) | 1.2 | 0.4 | 1.0, 1.4 | 1.1 | 0.3 | 0.9, 1.2 | 0.16 |
| Total superficial layer thickness (mm) | 9.2 | 3.2 | 7.7, 10.6 | 9.8 | 2.9 | 8.5, 11.1 | 0.11 |
| Vastus Lateralis | Biceps Femoris | |||||
|---|---|---|---|---|---|---|
| Coefficient | p-Value | 95% CI | Coefficient | p-Value | 95% CI | |
| Time of contraction (Tc) (ms) | 0.213 | 0.341 | 0.213, 0.341 | −0.228 | 0.307 | −0.228, 0.307 |
| Sustain time (Ts) (ms) * | 0.043 | 0.848 | 0.043, 0.848 | 0.001 | 0.996 | 0.001, 0.996 |
| Relaxation time (Tr) (ms) * | −0.033 | 0.883 | −0.033, 0.883 | −0.187 | 0.405 | −0.187, 0.405 |
| Delay time (Td) (ms) | 0.145 | 0.521 | 0.145, 0.521 | −0.129 | 0.566 | −0.129, 0.566 |
| Maximal displacement (Dm) (mm) | −0.032 | 0.887 | −0.032, 0.887 | −0.165 | 0.463 | −0.165, 0.463 |
| Muscle thickness (mm) | 0.092 | 0.661 | 0.092, 0.661 | −0.055 | 0.792 | −0.055, 0.792 |
| Skin thickness (mm) | 0.035 | 0.867 | 0.035, 0.867 | −0.036 | 0.863 | −0.036, 0.863 |
| Subcutaneous fat thickness (mm) | −0.023 | 0.911 | −0.023, 0.911 | 0.327 | 0.11 | 0.327, 0.11 |
| Fascia thickness (mm) | 0.193 | 0.355 | 0.193, 0.355 | 0.049 | 0.817 | 0.049, 0.817 |
| Total superficial layer thickness (mm) | 0.026 | 0.903 | 0.026, 0.903 | 0.298 | 0.148 | 0.298, 0.148 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfuraih, A.M.; Alhowimel, A.; Alghanim, S.; Khayat, Y.; Aljamaan, A.; Alsobayel, H.I. The Association between Tensiomyography and Elastography Stiffness Measurements in Lower Limb Skeletal Muscles. Sensors 2022, 22, 1206. https://doi.org/10.3390/s22031206
Alfuraih AM, Alhowimel A, Alghanim S, Khayat Y, Aljamaan A, Alsobayel HI. The Association between Tensiomyography and Elastography Stiffness Measurements in Lower Limb Skeletal Muscles. Sensors. 2022; 22(3):1206. https://doi.org/10.3390/s22031206
Chicago/Turabian StyleAlfuraih, Abdulrahman M., Ahmed Alhowimel, Sara Alghanim, Yaaqoub Khayat, Abdulaziz Aljamaan, and Hana I. Alsobayel. 2022. "The Association between Tensiomyography and Elastography Stiffness Measurements in Lower Limb Skeletal Muscles" Sensors 22, no. 3: 1206. https://doi.org/10.3390/s22031206
APA StyleAlfuraih, A. M., Alhowimel, A., Alghanim, S., Khayat, Y., Aljamaan, A., & Alsobayel, H. I. (2022). The Association between Tensiomyography and Elastography Stiffness Measurements in Lower Limb Skeletal Muscles. Sensors, 22(3), 1206. https://doi.org/10.3390/s22031206