
Experimental Verification of Micro-Doppler Radar Measurements of Fall-Risk-Related Gait Differences for Community-Dwelling Elderly Adults


Abstract
:1. Introduction
- The effectiveness of the classification model constructed based on simulated MDR data was verified using actual MDR data. Thus, this study experimentally verified our previous simulation study.
- The actual MDR data of elderly fallers were collected via experiments in a community setting (not in a laboratory setting). In other words, similar data on the practical use of monitoring systems for community-dwelling elderly adults were collected.
- A classification accuracy of 78.8% was achieved for the actual data through the training and validation process of the classification model using only the simulated data.
- The comparison of the results of gait parameter extraction and classification based on the simulated and actual data indicated the validity of both types of data.
2. Methods
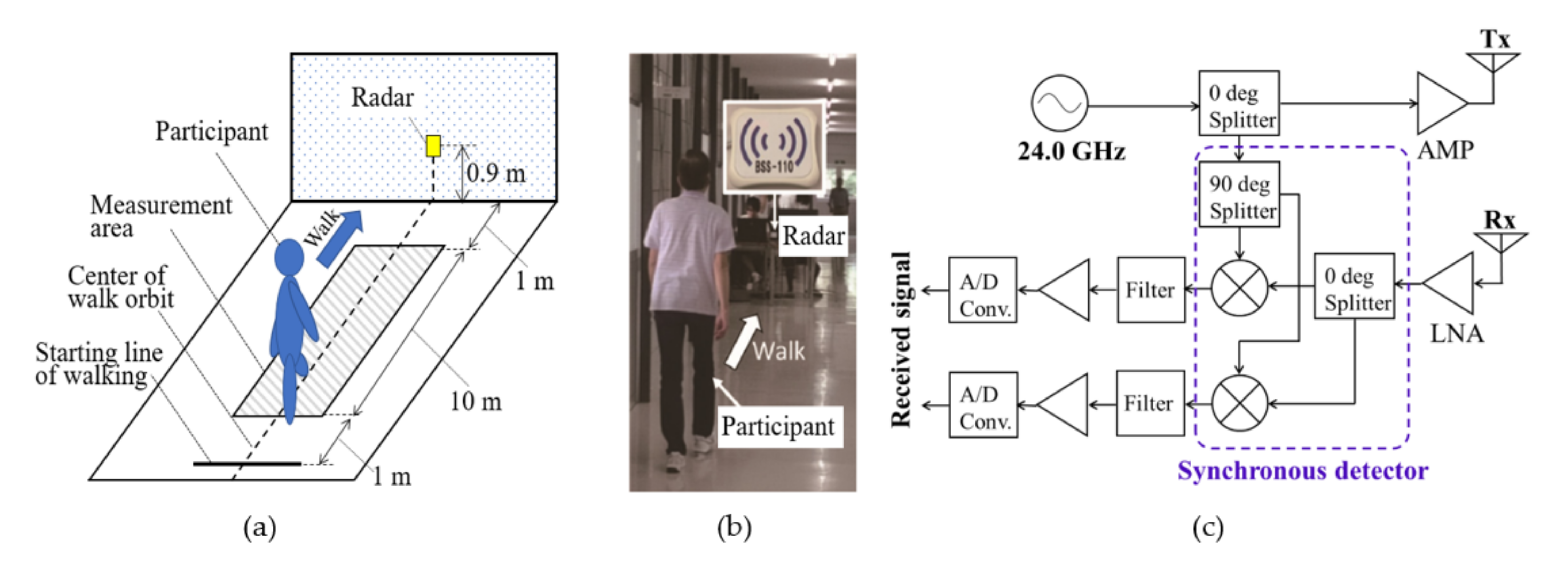
2.1. Participants and Experimental Protocol
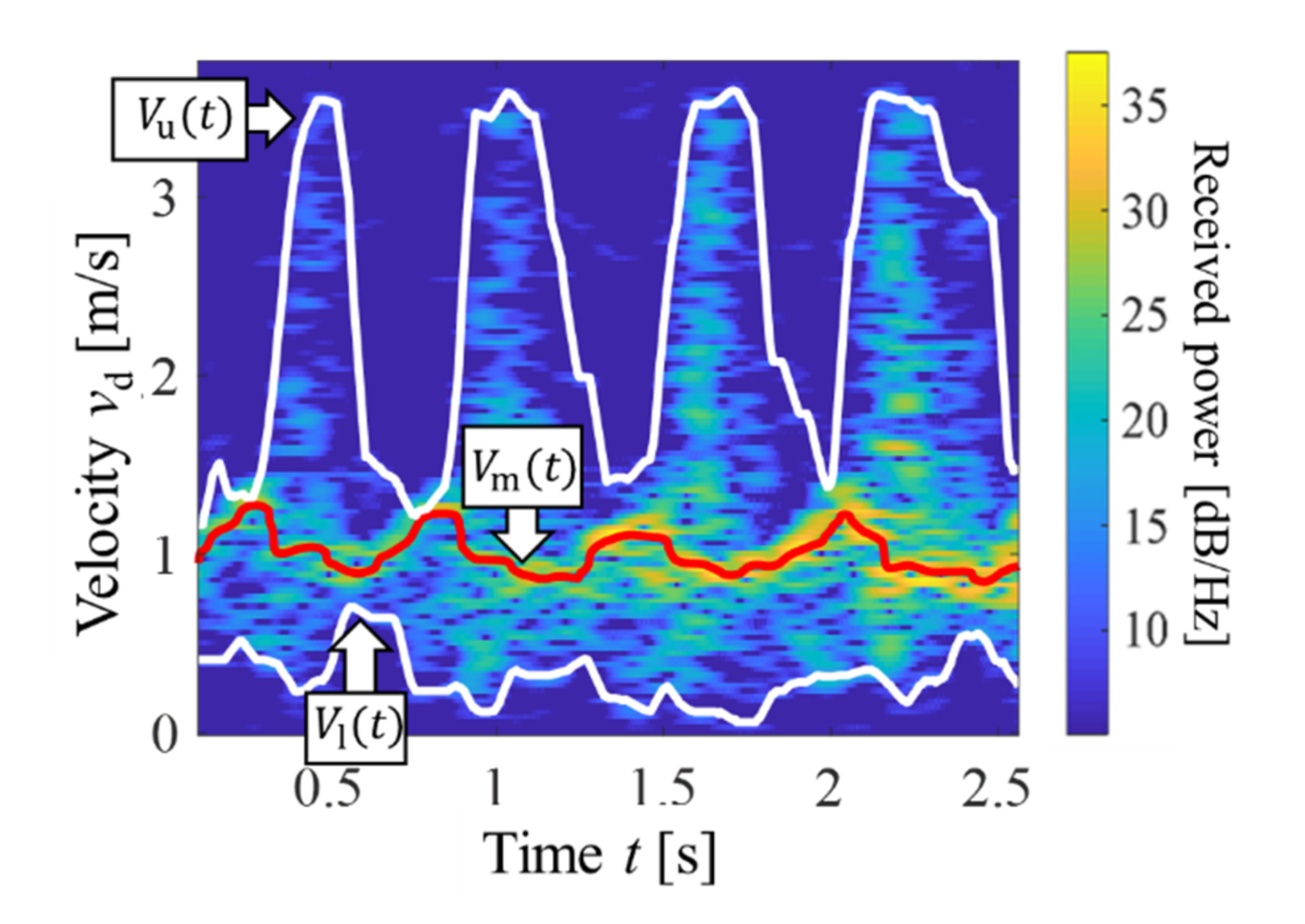
2.2. MDR Gait Measurement and Gait Parameter Extraction
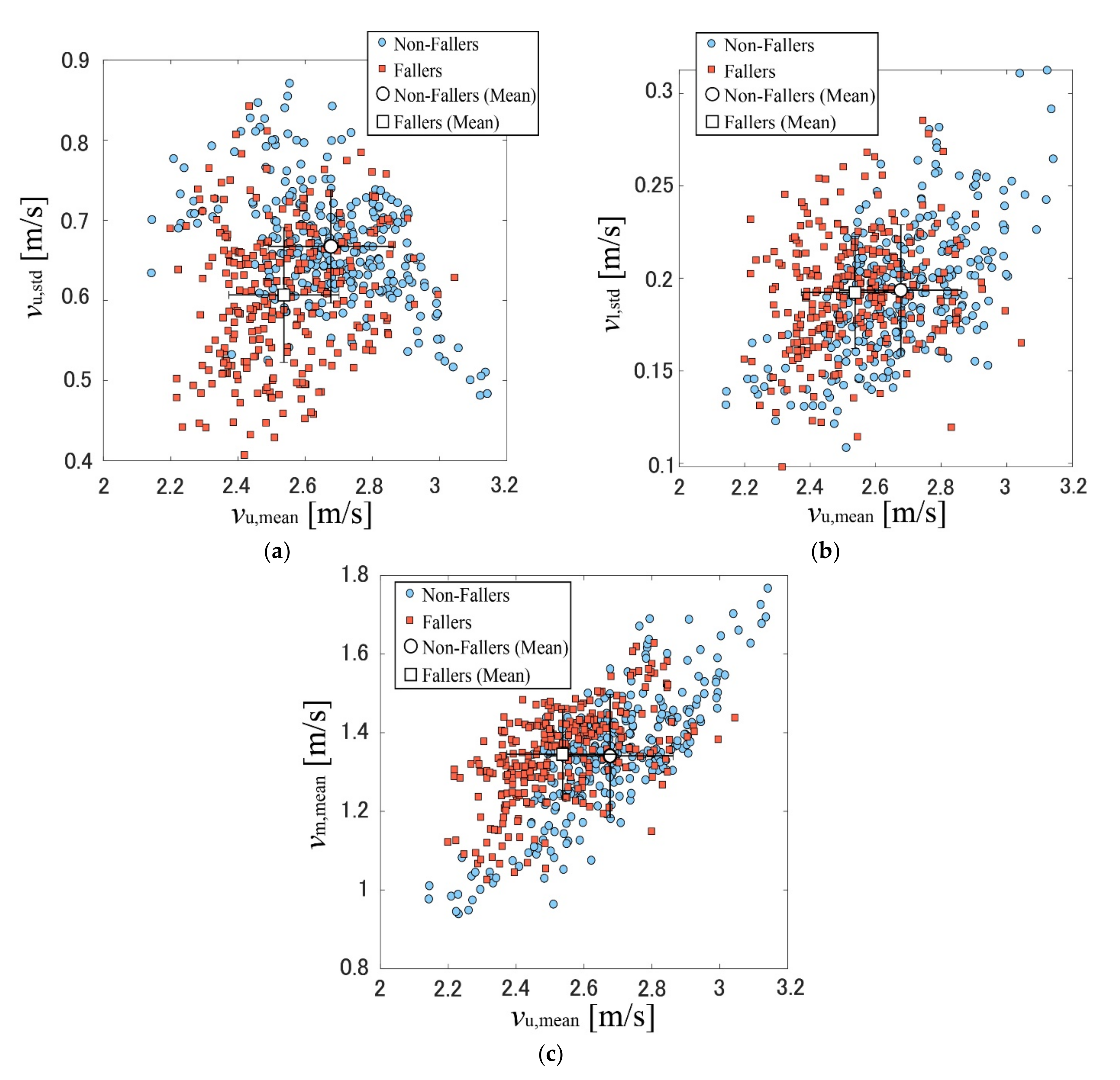
- The mean body velocity, vm,mean = E[vm(t)], where E[ ] indicates the mean with respect to t.
- The mean leg velocity during the leg-forward motion, vu,mean = E[vu(t)].
- The degree of variation in leg velocities during the leg-forward motion, vu,std = STD[vu(t)], where STD[ ] indicates the standard deviation with respect to t.
- The degree of variation in leg velocities in the stance phase, vl,std = STD[vl(t)].
2.3. Gait Classification Based on SVM Model Constructed Using Simulated MDR Dataset
3. Results and Discussion
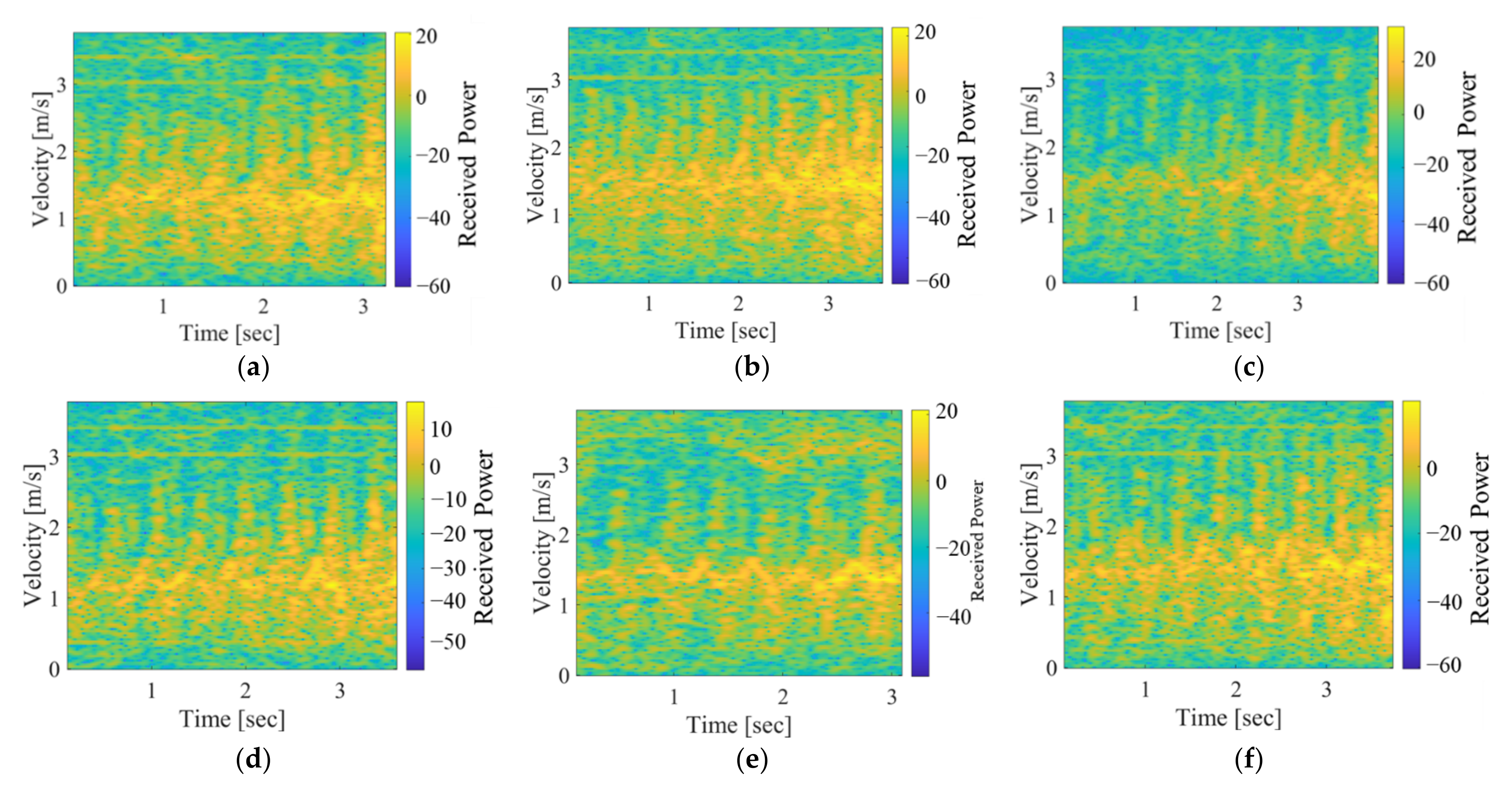
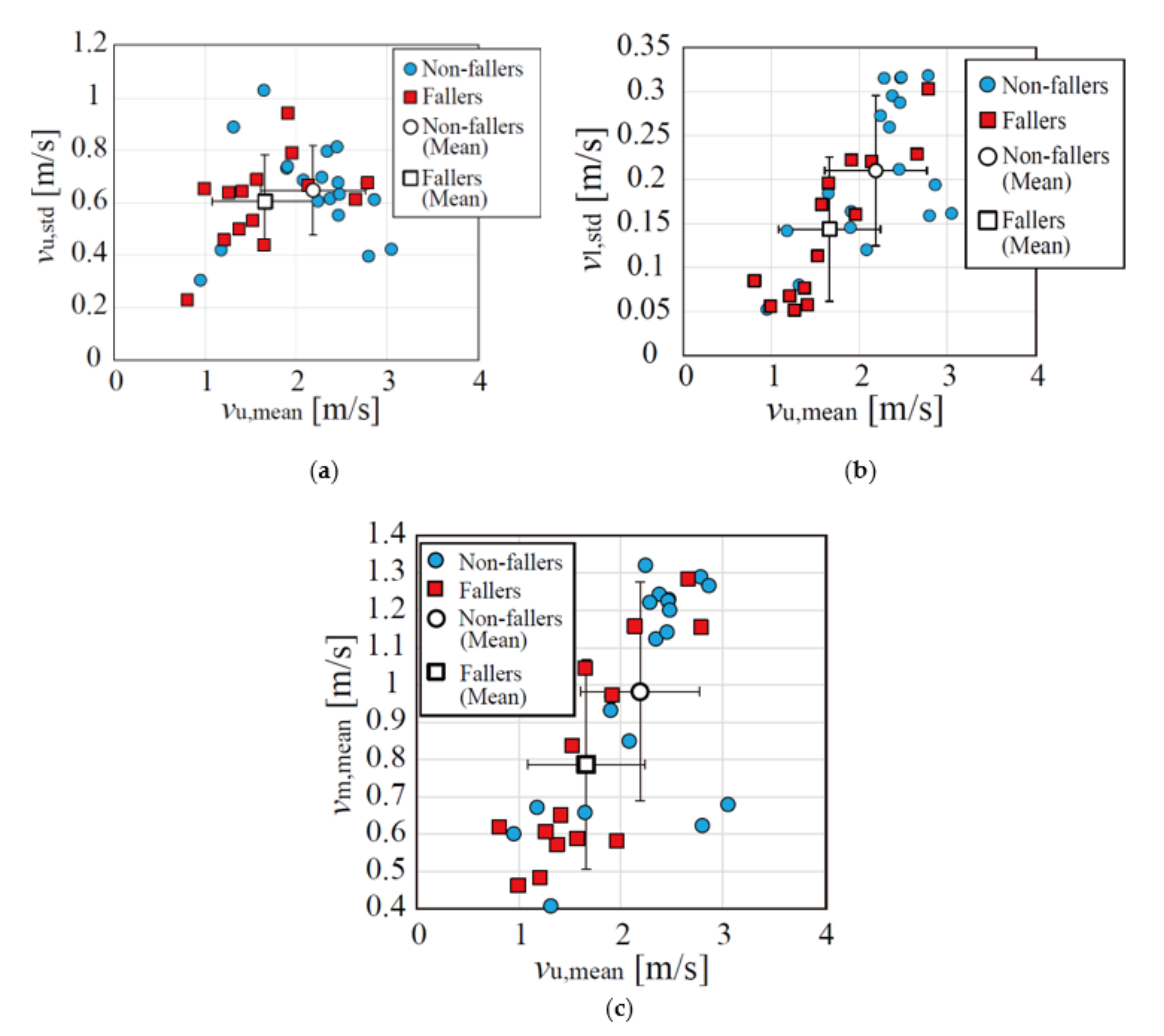
3.1. Gait Parameter Extraction
3.2. Classification Results
3.3. Comparison with Other Studies
- The conventional radar-based techniques including these conventional studies did not deal with the faller classification problem. Thus, the novelty of our previous and present studies is in performing the faller classification using the radar gait measurement.
- The radar data of the actual community-dwelling elderly adults collected in the real environments (not in the laboratory settings) were used to show the feasibility of radar-based monitoring for daily healthcare applications.
3.4. Limitation of the Study
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, W.; Keegan, T.H.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P., Jr.; Kelsey, J.L. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, M.; Chou, L.-S. Sagittal plane momentum control during walking in elderly fallers. Gait Posture 2016, 45, 121–126. [Google Scholar] [CrossRef]
- Drover, D.; Howcroft, J.; Kofman, J.; Lemaire, E.D. Faller classification in older adults using wearable sensors based on turn and straight-walking accelerometer-based features. Sensors 2017, 17, 1321. [Google Scholar] [CrossRef] [PubMed]
- Tromp, A.M.; Pluijm, S.M.F.; Smit, J.H.; Deeg, D.J.H.; Bouter, L.M.; Lips, P.T.A.M. Fall-risk screening test: A prospective study on predictors for falls in community-dwelling elderly. J. Clin. Epidemiol. 2001, 54, 837–844. [Google Scholar] [CrossRef] [Green Version]
- Anwary, A.R.; Yu, H.; Callaway, A.; Vassallo, M. Validity and consistency of concurrent extraction of gait features using inertial measurement units and motion capture system. IEEE Sens. J. 2020, 21, 1625–1634. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Thorpe, S.K.; O’Malley, M.J.; Vaughan, C.L. Automatic detection of gait events using kinematic data. Gait Posture 2007, 25, 469–474. [Google Scholar] [CrossRef]
- Daines, K.J.; Baddour, N.; Burger, H.; Bavec, A.; Lemaire, E.D. Fall risk classification for people with lower extremity amputations using random forests and smartphone sensor features from a 6-minute walk test. PLoS ONE 2021, 16, e0247574. [Google Scholar] [CrossRef]
- Meyer, B.M.; Tulipani, L.J.; Gurchiek, R.D.; Allen, D.A.; Adamowicz, L.; Larie, D.; Solomon, A.J.; Cheney, N.; McGinnis, R.S. Wearables and deep learning classify fall risk from gait in multiple sclerosis. IEEE J. Biomed. Health Inform. 2020, 25, 1824–1831. [Google Scholar] [CrossRef]
- Bet, P.; Castro, P.C.; Ponti, M.A. Foreseeing future falls with accelerometer features in active community-dwelling older persons with no recent history of falls. Exp. Gerontol. 2021, 143, 111139. [Google Scholar] [CrossRef]
- Esfahani, M.I.M.; Maury, A.N. Using smart garments to differentiate among normal and simulated abnormal gaits. J. Biomech. 2019, 93, 70–76. [Google Scholar] [CrossRef]
- Bergmann, J.H.M.; Chandaria, V.; McGregor, A. Wearable and implantable sensors: The patient’s perspective. Sensors 2012, 12, 16695–16709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmann, J.H.M.; McGregor, A. Body-worn sensor design: What do patients and clinicians want? Ann. Biomed. Eng. 2011, 39, 2299–2312. [Google Scholar] [CrossRef] [PubMed]
- Latorre, J.; Colomer, C.; Alcañiz, M.; Llorens, R. Gait analysis with the Kinect v2: Normative study with healthy individuals and comprehensive study of its sensitivity, validity, and reliability in individuals with stroke. J. Neuroeng. Rehabil. 2019, 16, 97. [Google Scholar] [CrossRef] [Green Version]
- Latorre, J.; Llorens, R.; Colomer, C.; Alcaiz, M. Reliability and comparison of Kinect-based methods for estimating spatiotemporal gait parameters of healthy and post-stroke individuals. J. Biomech. 2018, 72, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Akbari, G.; Nikkhoo, M.; Wang, L.; Chen, C.P.; Han, D.S.; Lin, Y.H.; Chen, H.-B.; Cheng, C.H. Frailty level classification of the community elderly using Microsoft Kinect-based skeleton pose: A machine learning approach. Sensors 2021, 21, 4017. [Google Scholar] [CrossRef]
- Steinert, A.; Sattler, I.; Otte, K.; Röhling, H.; Mansow-Model, S.; Müller-Werdan, U. Using new camera-based technologies for gait analysis in older adults in comparison to the established GAITRite system. Sensors 2020, 20, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandomkar, Z.; Bahrami, F. Method to classify elderly subjects as fallers and non-fallers based on gait energy image. Healthc. Technol. Lett. 2014, 1, 110–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardillo, E.; Li, C.; Caddemi, A. Radar-Based Monitoring of the Worker Activities by Exploiting Range-Doppler and Micro-Doppler Signatures. In Proceedings of the 2021 IEEE International Workshop on Metrology for Industry 4.0 & IoT (MetroInd4. 0&IoT), Rome, Italy, 7–9 June 2021. [Google Scholar] [CrossRef]
- Li, X.; He, Y.; Fioranelli, F.; Jing, X.; Yarovoy, A.; Yang, Y. Human motion recognition with limited radar micro-Doppler signatures. IEEE Trans. Geosci. Remote Sens. 2020, 59, 6586–6599. [Google Scholar] [CrossRef]
- Saho, K.; Sakamoto, T.; Sato, T.; Inoue, K.; Fukuda, T. Pedestrian imaging using UWB Doppler radar interferometry. IEICE Trans. Commun. 2013, 96, 613–623. [Google Scholar] [CrossRef]
- Seifert, A.K.; Amin, M.G.; Zoubir, A.M. Toward unobtrusive in-home gait analysis based on radar micro-Doppler signatures. IEEE Trans. Biomed. Eng. 2019, 66, 2629–2640. [Google Scholar] [CrossRef] [Green Version]
- Nazaroff, M.J.; Kong, H.J.; Kim, Y. Tracking bedridden patient positions using micro-Doppler signatures. IEEE Sens. Lett. 2021, 5, 3500504. [Google Scholar] [CrossRef]
- Shah, S.A.; Fioranelli, F. RF sensing technologies for assisted daily living in healthcare: A comprehensive review. IEEE Aerosp. Electron. Syst. Mag. 2019, 34, 26–44. [Google Scholar] [CrossRef] [Green Version]
- Seifert, A.K.; Grimmer, M.; Zoubir, A.M. Doppler radar for the extraction of biomechanical parameters in gait analysis. IEEE J. Biomed. Health Inform. 2020, 25, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Alshamaa, D.; Soubra, R.; Chkeir, A. A Radar Sensor for Automatic Gait Speed Analysis in Walking Tests. IEEE Sens. J. 2021, 21, 13886–13894. [Google Scholar] [CrossRef]
- Gurbuz, S.Z.; Amin, M.G. Radar-based human-motion recognition with deep learning: Promising applications for indoor monitoring. IEEE Signal Process. Mag. 2019, 36, 16–28. [Google Scholar] [CrossRef]
- Le, H.T.; Phung, S.L.; Bouzerdoum, A. A fast and compact deep Gabor network for micro-Doppler signal processing and human motion classification. IEEE Sens. J. 2021, 21, 23085–23097. [Google Scholar] [CrossRef]
- Singh, A.; Rehman, S.U.; Yongchareon, S.; Chong, P.H.J. Sensor technologies for fall detection systems: A review. IEEE Sens. J. 2020, 20, 6889–6919. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Vaughan, R. Deep learning radar design for breathing and fall detection. IEEE Sens. J. 2020, 20, 5072–5085. [Google Scholar] [CrossRef]
- Taylor, W.; Dashtipour, K.; Shah, S.A.; Hussain, A.; Abbasi, Q.H.; Imran, M.A. Radar sensing for activity classification in elderly people exploiting micro-Doppler signatures using machine learning. Sensors 2021, 21, 3881. [Google Scholar] [CrossRef]
- Hayashi, S.; Saho, K.; Shioiri, K.; Fujimoto, M.; Masugi, M. Utilization of micro-Doppler radar to classify gait patterns of young and elderly adults: An approach using long short-term memory network. Sensors 2021, 21, 3643. [Google Scholar] [CrossRef]
- Saho, K.; Fuijimoto, M.; Masugi, M.; Chou, L.-S. Gait classification of young adults, elderly non-fallers, and elderly fallers using micro-Doppler radar signals: Simulation study. IEEE Sens. J. 2017, 17, 2320–2321. [Google Scholar] [CrossRef]
- Saho, K.; Shioiri, K.; Fujimoto, M.; Kobayashi, Y. Micro-Doppler radar gait measurement to detect age- and fall risk-related differences in gait: A simulation study on comparison of deep learning and gait parameter-based approaches. IEEE Access 2021, 9, 18518–18526. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Hida, N.; Nakajima, K.; Fujimoto, M.; Mochimaru, M. AIST Gait Database. 2019. Available online: https://unit.aist.go.jp/harc/ExPART/GDB2019_e.html (accessed on 1 December 2021).
- Luts, J.; Ojeda, F.; Van de Plas, R.; De Moor, B.; Van Huffel, S.; Suykens, J.A. A tutorial on support vector machine-based methods for classification problems in chemometrics. Anal. Chim. Acta 2010, 665, 129–145. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.L.; Chen, M.C.; Wang, C.J. Credit scoring with a data mining approach based on support vector machines. Expert Syst. Appl. 2007, 33, 847–856. [Google Scholar] [CrossRef]
- Patterson, M.R.; Whelan, D.; Reginatto, B.; Caprani, N.; Walsh, L.; Smeaton, A.F.; Inomata, A.; Caulfield, B. Does External Walking Environment Affect Gait Patterns? In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transmitting frequency | 24 GHz |
| Transmitting waveform | Sinusoidal |
| Detector for received signals | Synchronous detector |
| Sampling frequency of received signals | 600 Hz |
| Effective isotropic radiated power | 40 mW |
| 3 dB beamwidth | ±35° (H-plane), ±14° (E-plane) |
| Physical size | 6 cm (W), 2 cm (D), 7 cm (H) |
| Parameter | Fallers (Mean ± SD) | Non-Fallers (Mean ± SD) | p from Welch’s t-Test |
|---|---|---|---|
| vm,mean (m/s) | 0.787 ± 0.281 | 0.982 ± 0.293 | 0.0630 |
| vu,mean (m/s) | 1.66 ± 0.578 | 2.19 ± 0.581 | 0.0151 |
| vu,std (m/s) | 0.605 ± 0.170 | 0.647 ± 0.178 | 0.493 |
| vl,std (m/s) | 0.144 ± 0.0817 | 0.210 ± 0.0854 | 0.0308 |
| True\Predicted | Fallers | Non-Fallers |
|---|---|---|
| Fallers | 9 | 5 |
| Non-fallers | 2 | 17 |
| True\Predicted | Fallers | Non-Fallers |
|---|---|---|
| Fallers | 10 | 4 |
| Non-fallers | 5 | 14 |
| Study | Sensor (Other Conditions) | Sensor Type | Accuracy | Sensitivity |
|---|---|---|---|---|
| Daines et al. (2021) [7] | Accelerometer (smartphone, 6 min walk test) | Contact | 81.3% | 57.2% |
| Meyer et al. (2020) [8] | Accelerometer and gyro sensor (deep learning model, 1 min walk data) | Contact | 86% | 88% |
| Bet et al. (2021) [9] | Accelerometer ((measuring the timed up and go test) | Contact | 75% | 71% |
| Latorre et al. (2019) [13] | Depth sensor (Microsoft Kinect, 10 m walk test) | Remote | N.A. (Results of paired t-tests were only presented) | |
| Gandomkar et al. (2014) [17] | Video camera (measuring the timed up and go test) | Remote | 62.5% | N.A. |
| This study | Doppler radar (model was tuned for the accuracy, 10 m walk test) | Remote | 78.9% | 63.2% |
| Doppler radar (model was tuned for the sensitivity, 10 m walk test) | 72.7% | 71.4% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saho, K.; Fujimoto, M.; Kobayashi, Y.; Matsumoto, M. Experimental Verification of Micro-Doppler Radar Measurements of Fall-Risk-Related Gait Differences for Community-Dwelling Elderly Adults. Sensors 2022, 22, 930. https://doi.org/10.3390/s22030930
Saho K, Fujimoto M, Kobayashi Y, Matsumoto M. Experimental Verification of Micro-Doppler Radar Measurements of Fall-Risk-Related Gait Differences for Community-Dwelling Elderly Adults. Sensors. 2022; 22(3):930. https://doi.org/10.3390/s22030930
Chicago/Turabian StyleSaho, Kenshi, Masahiro Fujimoto, Yoshiyuki Kobayashi, and Michito Matsumoto. 2022. "Experimental Verification of Micro-Doppler Radar Measurements of Fall-Risk-Related Gait Differences for Community-Dwelling Elderly Adults" Sensors 22, no. 3: 930. https://doi.org/10.3390/s22030930
APA StyleSaho, K., Fujimoto, M., Kobayashi, Y., & Matsumoto, M. (2022). Experimental Verification of Micro-Doppler Radar Measurements of Fall-Risk-Related Gait Differences for Community-Dwelling Elderly Adults. Sensors, 22(3), 930. https://doi.org/10.3390/s22030930