
A Wearable System Composed of FBG-Based Soft Sensors for Trunk Compensatory Movements Detection in Post-Stroke Hemiplegic Patients

 ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. The Wearable System: Working Principle, Manufacturing, and Metrological Assessment
2.1. FBG’s Working Principle
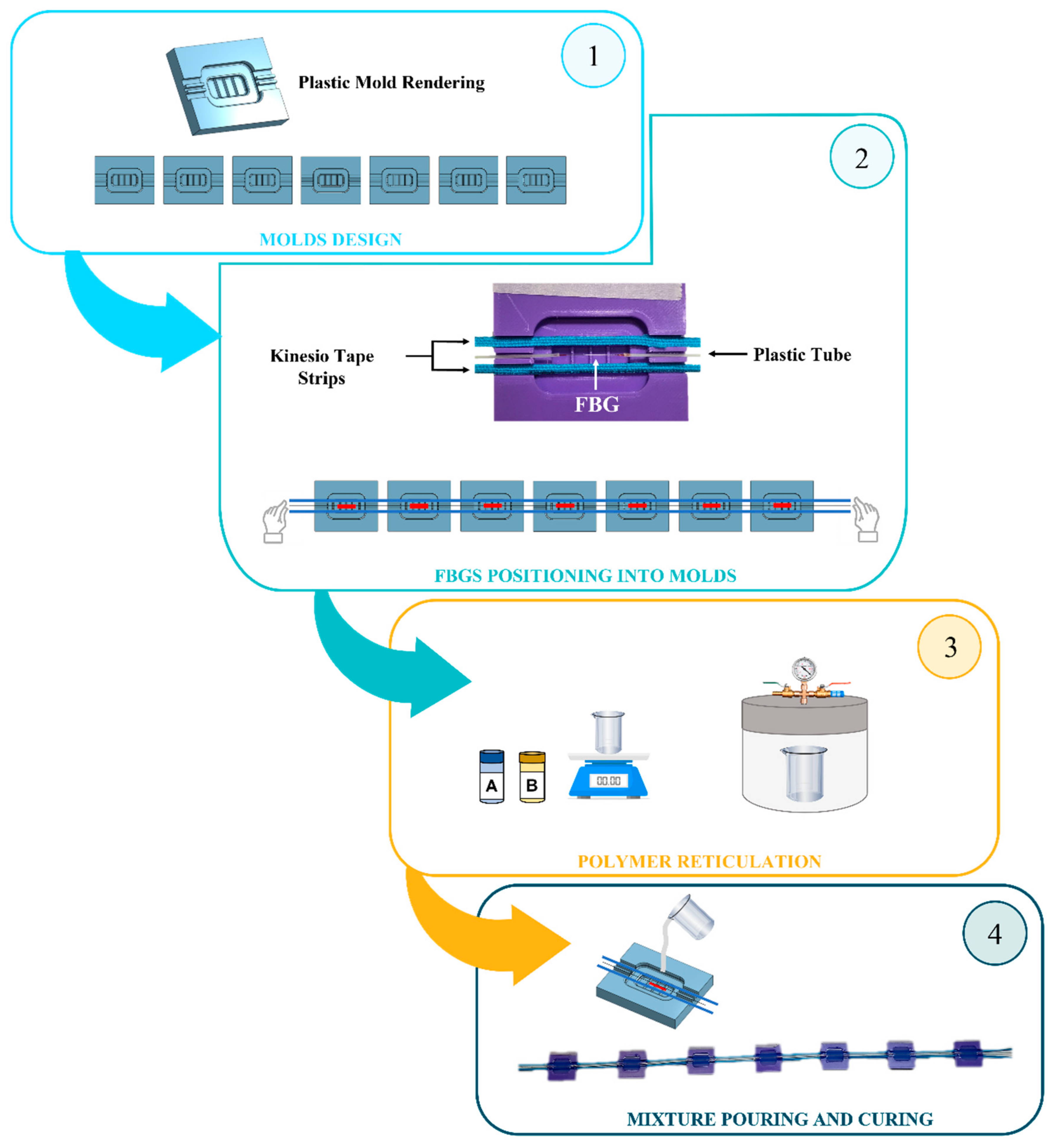
2.2. Design and Manufacturing Process
- The design and 3D-printing of seven molds;
- The FBG’s positioning at the molds’ midsection before the gratings’ encapsulation into the flexible matrices;
- The polymer reticulation by mixing part A and part B of a bi-component silicone rubber;
- The mixture pouring into the molds and curing for 24 h at room temperature before pulling out each SSE from the mold.
2.3. Response to Strain and Temperature Influence
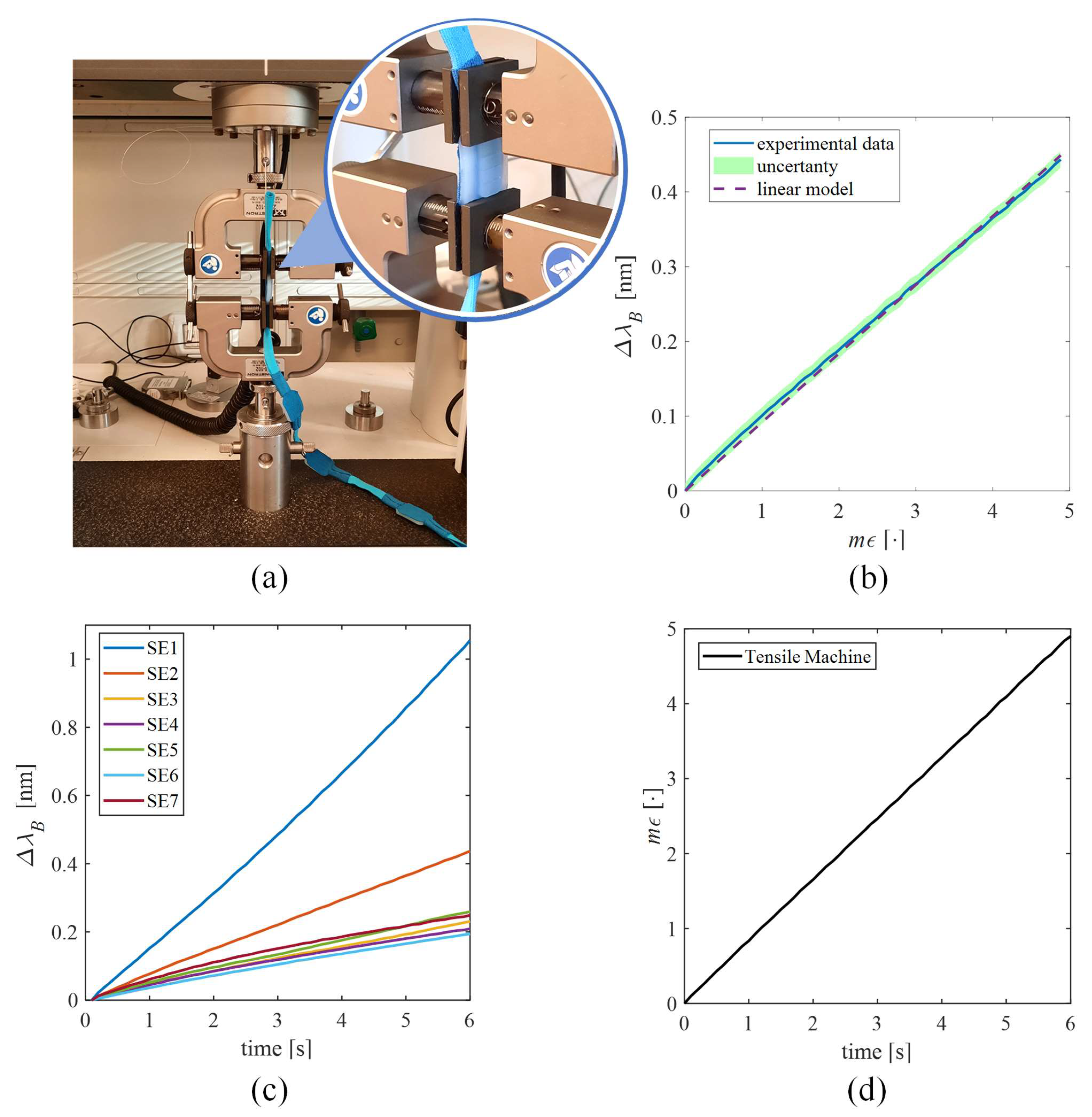
2.3.1. The Sensing Elements’ Response to Strain
2.3.2. The Sensing Elements’ Response to Temperature
3. Feasibility Assessment of the Wearable System in CTMs’ Detection
3.1. Experimental Trial on Healthy Volunteers
- Forward Movements (FM): move the object back and forth by executing a flexion–extension movement of the arm;
- Lateral Movements (LM): move the object right and left, keeping the arm outstretched;
- Circular Movements (CM): move the object, performing circular motions.
3.2. Experimental Trial on Hemiplegic Patients
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim:, J.; Thayabaranathan, T.; Donnan, G.A.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.; Norrving, B.; Owolabi, M.; Pandian, J.; et al. Global stroke statistics 2019. Int. J. Stroke 2020, 15, 819–838. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of stroke in Europe: Thirty-year projections of incidence, prevalence, deaths, and disability-adjusted life years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Lawrence, E.S.; Coshall, C.; Dundas, R.; Stewart, J.; Rudd, A.G.; Howard, R.; Wolfe, C.D.A. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 2001, 32, 1279–1284. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Oujamaa, L.; Relave, I.; Froger, J.; Mottet, D.; Pelissier, J.-Y. Rehabilitation of arm function after stroke. Literature review. Ann. Phys. Rehabil. Med. 2009, 52, 269–293. [Google Scholar] [CrossRef]
- Levin, M.F.; Kleim, J.A.; Wolf, S.L. What do motor “recovery” and “compensation” mean in patients following stroke? Neurorehabil. Neural Repair 2009, 23, 313–319. [Google Scholar] [CrossRef]
- Jones, T.A. Motor compensation and its effects on neural reorganization after stroke. Nat. Rev. Neurosci. 2017, 18, 267–280. [Google Scholar] [CrossRef]
- Cirstea, M.C.; Levin, M.F. Compensatory strategies for reaching in stroke. Brain 2000, 123, 940–953. [Google Scholar] [CrossRef]
- Lin, S.; Mann, J.; Mansfield, A.; Wang, R.H.; Harris, J.E.; Taati, B. Investigating the feasibility and acceptability of real-time visual feedback in reducing compensatory motions during self-administered stroke rehabilitation exercises: A pilot study with chronic stroke survivors. J. Rehabil. Assist. Technol. Eng. 2019, 6, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Valdés, B.A.; Van der Loos, H.F.M. Biofeedback vs. game scores for reducing trunk compensation after stroke: A randomized crossover trial. Top. Stroke Rehabil. 2018, 25, 96–113. [Google Scholar] [CrossRef] [PubMed]
- Gopura, R.A.R.C.; Kiguchi, K.; Bandara, D.S.V. A brief review on upper extremity robotic exoskeleton systems. In Proceedings of the 2011 6th international Conference on Industrial and Information Systems, Kandy, Sri Lanka, 16–19 August 2011; pp. 346–351. [Google Scholar]
- Wang, Q.; Chen, W.; Timmermans, A.A.A.; Karachristos, C.; Martens, J.B.; Markopoulos, P. Smart Rehabilitation Garment for posture monitoring. In Proceedings of the 2015 37th annual International Conference of the IEEE engineering in medicine and biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5736–5739. [Google Scholar]
- Ranganathan, R.; Wang, R.; Dong, B.; Biswas, S. Identifying compensatory movement patterns in the upper extremity using a wearable sensor system. Physiol. Meas. 2017, 38, 2222. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, R.; Wang, R.; Gebara, R.; Biswas, S. Detecting compensatory trunk movements in stroke survivors using a wearable system. In Proceedings of the 2017 Workshop on Wearable Systems and Applications, Niagara Falls, NY, USA, 19 June 2017; pp. 29–32. [Google Scholar]
- Alankus, G.; Kelleher, C. Reducing compensatory motions in video games for stroke rehabilitation. In Proceedings of the SIGCHI conference on human factors in computing systems, Austin, TX, USA, 5–10 May 2012; pp. 2049–2058. [Google Scholar]
- Delbressine, F.; Timmermans, A.; Beursgens, L.; de Jong, M.; van Dam, A.; Verweij, D.; Janssen, M.; Markopoulos, P. Motivating arm-hand use for stroke patients by serious games. In Proceedings of the 34th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, USA, 28 August–1 September 2012; pp. 3564–3567. [Google Scholar]
- Timmermans, A.A.A.; Seelen, H.A.M.; Geers, R.P.J.; Saini, P.K.; Winter, S.; Te Vrugt, J.; Kingma, H. Sensor-based arm skill training in chronic stroke patients: Results on treatment outcome, patient motivation, and system usability. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Majidi, C. Soft robotics: A perspective—current trends and prospects for the future. Soft Robot. 2014, 1, 5–11. [Google Scholar] [CrossRef]
- Trivedi, D.; Rahn, C.D.; Kier, W.M.; Walker, I.D. Soft robotics: Biological inspiration, state of the art, and future research. Appl. bionics Biomech. 2008, 5, 99–117. [Google Scholar] [CrossRef]
- Caviedes, J.E.; Li, B.; Jammula, V.C. Wearable sensor array design for spine posture monitoring during exercise incorporating biofeedback. IEEE Trans. Biomed. Eng. 2020, 67, 2828–2838. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kwon, J.; Han, S.; Park, Y.-L.; Jo, S. Deep full-body motion network for a soft wearable motion sensing suit. IEEE/ASME Trans. Mechatronics 2018, 24, 56–66. [Google Scholar] [CrossRef]
- Krohn, D.A.; MacDougall, T.; Mendez, A. Fiber optic sensors: Fundamentals and applications; SPIE: Bellingham, Washington, 2014; ISBN 1628411805. [Google Scholar]
- Presti, D.L.; Massaroni, C.; Leitão, C.S.J.; Domingues, M.D.F.; Sypabekova, M.; Barrera, D.; Floris, I.; Massari, L.; Oddo, C.M.; Sales, S.; et al. Fiber Bragg Gratings for medical applications and future challenges: A review. IEEE Access 2020, 8, 156863–156888. [Google Scholar] [CrossRef]
- Elsarnagawy, T. A simultaneous and validated wearable FBG heartbeat and respiration rate monitoring system. Sens. Lett. 2015, 13, 48–51. [Google Scholar] [CrossRef]
- Massaroni, C.; Venanzi, C.; Silvatti, A.P.; Presti, D.L.; Saccomandi, P.; Formica, D.; Giurazza, F.; Caponero, M.A.; Schena, E. Smart textile for respiratory monitoring and thoraco-abdominal motion pattern evaluation. J. Biophotonics 2018, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Massaroni, C.; Presti, D.L.; Saccomandi, P.; Caponero, M.A.; D’Amato, R.; Schena, E. Fiber Bragg grating probe for relative humidity and respiratory frequency estimation: Assessment during mechanical ventilation. IEEE Sens. J. 2018, 18, 2125–2130. [Google Scholar] [CrossRef]
- Presti, D.L.; Massaroni, C.; Zaltieri, M.; Sabbadini, R.; Carnevale, A.; Di Tocco, J.; Longo, U.G.; Caponero, M.A.; D’Amato, R.; Schena, E.; et al. A Magnetic Resonance-compatible wearable device based on functionalized fiber optic sensor for respiratory monitoring. IEEE Sens. J. 2020, 21, 14418–14425. [Google Scholar] [CrossRef]
- Das, A.; Ambastha, S.; Sen, S.; Samanta, S. Wearable system for Real-time Remote Monitoring of Respiratory Rate during Covid-19 using Fiber Bragg Grating. In Proceedings of the 2020 IEEE 17th India Council International Conference (INDICON), New Delhi, India, 10–13 December 2020; pp. 1–4. [Google Scholar]
- Massaroni, C.; Zaltieri, M.; Presti, D.L.; Nicolò, A.; Tosi, D.; Schena, E. Fiber Bragg grating sensors for cardiorespiratory monitoring: A review. IEEE Sens. J. 2020, 21, 14069–14080. [Google Scholar] [CrossRef]
- Presti, D.L.; Romano, C.; Massaroni, C.; D’Abbraccio, J.; Massari, L.; Caponero, M.A.; Oddo, C.M.; Formica, D.; Schena, E. Cardio-Respiratory Monitoring in Archery Using a Smart Textile Based on Flexible Fiber Bragg Grating Sensors. Sensors 2019, 19, 3581. [Google Scholar] [CrossRef] [Green Version]
- Leal-Junior, A.G.; Diaz, C.R.; Leitão, C.; Pontes, M.J.; Marques, C.; Frizera, A. Polymer optical fiber-based sensor for simultaneous measurement of breath and heart rate under dynamic movements. Opt. Laser Technol. 2019, 109, 429–436. [Google Scholar] [CrossRef]
- Li, L.; He, R.; Soares, M.S.; Savović, S.; Hu, X.; Marques, C.; Min, R.; Li, X. Embedded FBG-Based Sensor for Joint Movement Monitoring. IEEE Sens. J. 2021, 21, 26793–26798. [Google Scholar] [CrossRef]
- Presti, D.L.; Carnevale, A.; D’Abbraccio, J.; Massari, L.; Massaroni, C.; Sabbadini, R.; Zaltieri, M.; Tocco, J.D.; Bravi, M.; Miccinilli, S.; et al. A Multi-Parametric Wearable System to Monitor Neck Movements and Respiratory Frequency of Computer Workers. Sensors 2020, 20, 536. [Google Scholar] [CrossRef] [Green Version]
- Pant, S.; Umesh, S.; Asokan, S. Knee angle measurement device using fiber bragg grating sensor. IEEE Sens. J. 2018, 18, 10034–10040. [Google Scholar] [CrossRef]
- Zaltieri, M.; Massaroni, C.; Presti, D.L.; Bravi, M.; Sabbadini, R.; Miccinilli, S.; Sterzi, S.; Formica, D.; Schena, E. A Wearable Device Based on a Fiber Bragg Grating Sensor for Low Back Movements Monitoring. Sensors 2020, 20, 3825. [Google Scholar] [CrossRef]
- Zaltieri, M.; Presti, D.L.; Massaroni, C.; Sabbadini, R.; Schena, E.; Bravi, M.; Miccinilli, S.; Sterzi, S.; Formica, D. An FBG-based Smart Wearable Device for Monitoring Seated Posture in Video Terminal Workers. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 & IoT, Roma, Italy, 3–5 June 2020; pp. 713–717. [Google Scholar]
- Zaltieri, M.; Presti, D.L.; Massaroni, C.; Schena, E.; D’Abbraccio, J.; Massari, L.; Oddo, C.M.; Formica, D.; Caponero, M.A.; Bravi, M.; et al. Feasibility Assessment of an FBG–based Wearable System for Monitoring Back Dorsal Flexion-Extension in Video Terminal Workers. In Proceedings of the 2020 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Dubrovnik, Croatia, 25–28 May 2020; pp. 1–5. [Google Scholar]
- Erdogan, T. Fiber grating spectra. J. Light. Technol. 1997, 15, 1277–1294. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Guo, Z.; Zhang, Y.; Chiang, K.S.; Dong, X. Simultaneous pressure and temperature measurement with polymer-coated fibre Bragg grating. Electron. Lett. 2000, 36, 564–566. [Google Scholar] [CrossRef]
- JCGM, J. Evaluation of measurement data—Guide to the expression of uncertainty in measurement. Int. Organ. Stand. Geneva ISBN 2008, 50, 134. [Google Scholar]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Housman, S.J.; Scott, K.M.; Reinkensmeyer, D.J. A randomized controlled trial of gravity-supported, computer-enhanced arm exercise for individuals with severe hemiparesis. Neurorehabil. Neural Repair 2009, 23, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Van Remoortel, H.; Giavedoni, S.; Raste, Y.; Burtin, C.; Louvaris, Z.; Gimeno-Santos, E.; Langer, D.; Glendenning, A.; Hopkinson, N.S.; Vogiatzis, I. Validity of activity monitors in health and chronic disease: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Presti, D.L.; Massaroni, C.; D’Abbraccio, J.; Massari, L.; Caponero, M.; Longo, U.G.; Formica, D.; Oddo, C.; Schena, E. Wearable system based on flexible FBG for respiratory and cardiac monitoring. IEEE Sens. J. 2019, 19, 7391–7398. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # SSE. | Sε [nm·mε−1] |
|---|---|
| SSE1 | 0.21 |
| SSE2 | 0.09 |
| SSE3 | 0.05 |
| SSE4 | 0.05 |
| SSE5 | 0.06 |
| SSE6 | 0.04 |
| SSE7 | 0.06 |
| # SSE | ST [nm·°C−1] |
|---|---|
| SSE1 | 0.015 |
| SSE2 | 0.013 |
| SSE3 | 0.012 |
| SSE4 | 0.013 |
| SSE5 | 0.014 |
| SSE6 | 0.014 |
| SSE7 | 0.015 |
| # Volunteer | Age [y.o.] | Sex | Dominant Hand | Height [cm] | Body Mass [kg] |
|---|---|---|---|---|---|
| 1 | 26 | Female | Right | 168 | 52 |
| 2 | 24 | Female | Right | 165 | 60 |
| 3 | 23 | Male | Right | 179 | 72 |
| 4 | 28 | Male | Right | 177 | 76 |
| 5 | 24 | Female | Right | 154 | 48 |
| 6 | 22 | Male | Right | 186 | 81 |
| 7 | 30 | Female | Right | 170 | 60 |
| 8 | 32 | Male | Right | 163 | 61 |
| 9 | 20 | Male | Right | 180 | 72 |
| 10 | 23 | Female | Right | 160 | 52 |
| # Patient | Age [y.o.] | Sex | Affected Side | Height [cm] | Body Mass [kg] | UE-FMA * |
|---|---|---|---|---|---|---|
| 1 | 55 | Male | Left | 170 | 74 | 11 |
| 2 | 73 | Male | Left | 175 | 106 | 37 |
| 3 | 63 | Male | Right | 175 | 88 | 43 |
| 4 | 33 | Female | Right | 168 | 54 | 55 |
| 5 | 63 | Male | Left | 170 | 79 | 32 |
| 6 | 47 | Male | Left | 184 | 86 | 24 |
| 7 | 55 | Male | Right | 168 | 49 | 50 |
| 8 | 43 | Male | Left | 165 | 75 | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Presti, D.; Zaltieri, M.; Bravi, M.; Morrone, M.; Caponero, M.A.; Schena, E.; Sterzi, S.; Massaroni, C. A Wearable System Composed of FBG-Based Soft Sensors for Trunk Compensatory Movements Detection in Post-Stroke Hemiplegic Patients. Sensors 2022, 22, 1386. https://doi.org/10.3390/s22041386
Lo Presti D, Zaltieri M, Bravi M, Morrone M, Caponero MA, Schena E, Sterzi S, Massaroni C. A Wearable System Composed of FBG-Based Soft Sensors for Trunk Compensatory Movements Detection in Post-Stroke Hemiplegic Patients. Sensors. 2022; 22(4):1386. https://doi.org/10.3390/s22041386
Chicago/Turabian StyleLo Presti, Daniela, Martina Zaltieri, Marco Bravi, Michelangelo Morrone, Michele Arturo Caponero, Emiliano Schena, Silvia Sterzi, and Carlo Massaroni. 2022. "A Wearable System Composed of FBG-Based Soft Sensors for Trunk Compensatory Movements Detection in Post-Stroke Hemiplegic Patients" Sensors 22, no. 4: 1386. https://doi.org/10.3390/s22041386
APA StyleLo Presti, D., Zaltieri, M., Bravi, M., Morrone, M., Caponero, M. A., Schena, E., Sterzi, S., & Massaroni, C. (2022). A Wearable System Composed of FBG-Based Soft Sensors for Trunk Compensatory Movements Detection in Post-Stroke Hemiplegic Patients. Sensors, 22(4), 1386. https://doi.org/10.3390/s22041386