
Gait Impairment in Traumatic Brain Injury: A Systematic Review

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
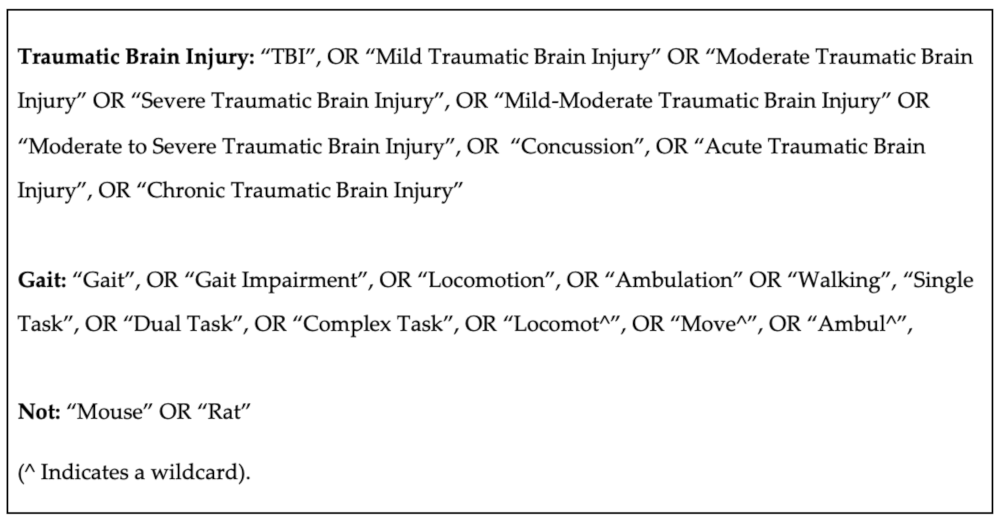
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
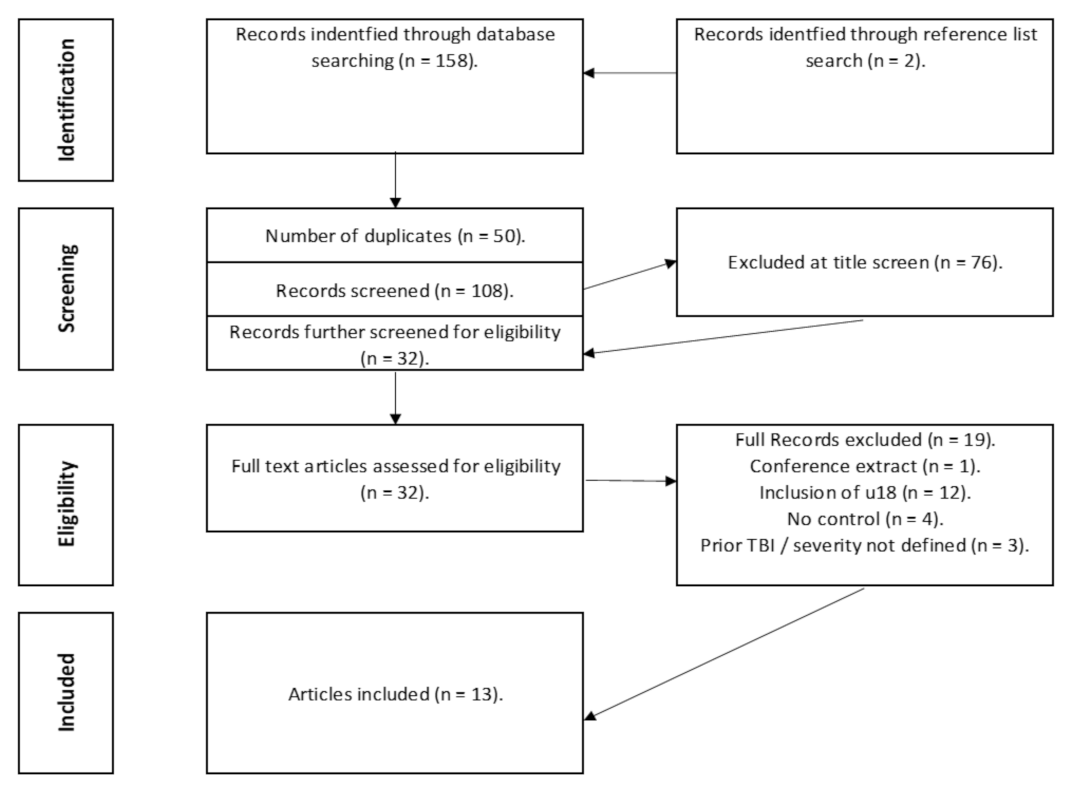
3.1. The Evidence Base
3.2. Particpants
3.3. Equipment
3.4. Procedures
3.5. Outcome Measure
3.6. Key Findings

{kind=link}
{kind=link}
| Author | TBI Population | Controls | Time Since Injury | Inclusion | Exclusion | TBI Diagnosis | |
|---|---|---|---|---|---|---|---|
| Basford et al. [26] | TBI Group: n = 10. (F:4, M:6). Age: 40.9 ± 11.3. TBI Severity: Mild: 4/10 Moderate: 2/10. Severe: 4/10. | Control Group. n = 10 (F:4, M:6). Age: 41.2 ± 11.4. Matched according to height, age (± 5 years), gender and weight (± 7.5 cm). | Time since Injury:
|
|
|
| |
| Belluscio et al. [24] | TBI Group: (19 RTA’s, 1 Fall) Severe TBI Group: >19 GCS score. n = 10 (F:2, M:8) Age: 33.2 ± 9.6. Very Severe TBI Group: ≤ 19 GCS score. n = 10. F:3, M:7) Age: 36.1 ± 13.1. | Control Group: n = 20. (F:5, M:15) Age: 33.9 ± 9.5. |
|
|
|
| |
| Fino et al. [33] | Mild TBI Group: 4 injured. (M:1, F:3) Age: 19 ± 0.8. | Control group. 4 matched control participants. (M:1, F:3) Age: 19.5 ± 1.2. |
|
|
|
| |
| Fino, [29] | Mild TBI Group: (M:2, F:3) Age: 18.8 ± 0.8. | Control group 4 matched control participants. (M:1, F:3) * No eligible control consent gained for 5th participant. Age: 19.5 ± 1.2. |
|
|
|
| |
| Martini et al. [31] | Chronic Mild TBI Group n = 65 Age: 39.6 ± 11.7. Time since TBI—1.1 years. | Control Group: n = 57. Age: 36.9 ± 12.2 Time since injury: 1.1 years. |
| Mild TBI Group.
| Control Group
|
|
|
| McFadyen et al. [25] | TBI Group: n = 8 (M:8). Post Traumatic Amnesia (Weeks): 3.9 ± 4.4.
| Control Group: n = 4 (M:4). Age: Range 22.75 to 44.3. Median: 25.9. No standard deviation or average reported. |
|
|
|
| |
| Oldham et al. [30] | Mild TBI Group: n = 50 (F:32, M: 18). Age: 20.2 ± 1.27. | Control Group: n = 25. (F: 13, M:12) 21.1 ± 2.2. | Time since injury: 72 h. |
|
|
| |
| Parker et al. [21] | University/college athletes, club sport athletes. Moderate TBI Group: n = 29 (Suffered grade 2 TBI according to the Academy of Neurology Practice). Age: 21.6 ± 3.26. (F:14, M:15) | Control Group: n = 29 Age: 21.38 ± 3.38. (F:14, M:15). |
|
|
|
| |
| Parrington et al. [32] | 53 Participants (Collegiate Athletes across 6 sporting departments in various universities). Mild TBI Group: n = 23 n = 2 did not return to play during specified 8-week period. (F:5, M:18) Age: 20.1 ± 1.3. Contact: Non-Contact Sport. 18:5. | Control Group: n = 25 (F:6, M:19) Age: 39.3 ± 13.0. Contact: Non-Contact Sport. 12:13. |
|
|
|
| |
| Pitt et al. [34] | Mild TBI Group: n = 11 (F:7, M:4). Age: 20.1 ± 1.3 | Control Group: Healthy matched—n = 11 (F:7, M:4). Age: 20.6 ± 1.9. |
|
|
|
| |
| Shan Chou et al. [27] | TBI Group: n = 10. (F:4, M:6). Age: 40.9 ± 11.3.
| Control Group: n = 10 (F:4, M:6). Age: 41.2 ± 11.4. Matched with age, gender, height, and weight. | Time since Injury:
|
|
|
| |
| Vallée et al. [23] | 18 Participants: Moderate to Severe TBI Group: n= 9(F:1, M:8) Age: 39.3 ± 13.0. | Control Group: n = 9 (F:1, M:8) Age: 39.7 ± 12.3. |
|
|
|
| |
| Williams et al. [22] | TBI Group: n = 41 (F:10, M:31) Age: 29.1 ± 9.4 Time since injury (days): 2609.4 ± 2327.3. Posttraumatic Amnesia (days): 84.9 ± 57.5. HiMAT Score: 22.7 ± 11.5. | Control Group: n = 25. (F:9, M:16) Age: 27.8 ± 7.4. |
|
|
|
| |
| Author | Aims | Procedures | Equipment | Outcome Measures | Key Findings |
|---|---|---|---|---|---|
| Basford et al. [26] | Assess the gait and dynamic balance of individuals with instability or imbalance after TBI. Examine the relationship between symptoms. |
Motion Analysis/Single Task Gait.
13 body segments. 4 upper extremities. 6 lower extremities. 1 pelvic, trunk, and head. |
|
|
|
| Belluscio et al. [24] | Quantify gait patterns in severe traumatic brain injury through wearable inertial sensors. Investigate the association of sensor-based quality of gait indices with the scores of administered scales. | Clinical Assessment:
|
|
|
|
| Fino et al. [33] | To determine the local dynamic stability of athletes who recently suffered a TBI during single and dual-task gait. |
|
|
|
|
| Fino, [29] | To determine single and dual-task turning kinematics in TBI and healthy athletes. |
|
| Stride characteristics
| Path Trajectory:
|
| Martini et al. [31] | Determine if gait domains are different without and with chronic Mild TBI. Determine if adding dual-task exacerbates differences in gait across the domains. Determine if self-reported severity scores are related to gait performance. | Single and dual-task conditions:
Audio Stroop Test:
| Inertial Sensors.
| Single Task and Dual-task.
| Individuals with chronic Mild TBI exhibit deficits across a multitude of gait characteristics.
|
| McFadyen et al. [25] | To definitively understand residual locomotor effects following a TBI on obstructed and unobstructed walking. | Locomotor Capacity and Gait:
|
|
|
|
| Oldham et al. [30] | Examine whether changes between baseline and acute post-TBI single task and dual-task tandem gait performance differed between male and female athletes. | Tandem gait measures recorded consistently with SCAT-3. Single Task:
| Time recorded using smartphone. NR of inertial sensors. |
|
|
| Parker et al. [21] | Examine the relationship between measures of dynamic motor performance (single and dual-task walking) and neuropsychological function following concussion over the course of 28 days. | Gait Stability Testing.
|
| Neuropsychological testing
Average speed of responding to
|
|
| Parrington et al. [32] | Evaluate the recovery of gait and balance in concussed athletes to account for changes in trends following return to play. |
|
|
| BESS:
|
| Pitt et al. [34] | Provide an objective description of angular velocity and acceleration profiles along orthogonal axes from one IMU situated on L5 vertebrae. Demonstrate that detectable differences could be identified in IMU metrics and be utilised to distinguish individuals with a TBI during dual-task walking. | TBI participants:
| Superlab 5 software:
| Peak velocities
| Healthy and TBI participants were distinguished across the two-month post-TBI period through.
|
| Shan Chou et al. [27] | Determine the possibility of quantitatively assessing dynamic stability that did not have an obvious neuromuscular origin in individuals who suffered a TBI. |
|
|
|
|
| Vallée et al. [23] | Establish the effects of increasingly demanding environments related to simultaneous visual tasks and physical obstructions to locomotor ability of people who have suffered TBI. | Visual Acuity:
|
|
|
|
| Williams et al. [22] | Identify the most common gait abnormalities following a TBI and determine their rate of incidence. | 25 reflective
| Kinematic: Motion Analysis: 25 small reflective markers 3DGA.
| Spatiotemporal.
|
|
| Article | Single Task | Dual-Task | Complex Task |
|---|---|---|---|
| Basford et al. [26] | ✓ | ||
| Belluscio et al. [24] | ✓ | ||
| Fino et al. [33] | ✓ | ✓ | |
| Fino, [29] | ✓ | ✓ | |
| Martini et al. [31] | ✓ | ✓ | |
| McFadyen et al. [25] | ✓ | ||
| Oldham et al. [30] | ✓ | ✓ | |
| Parker et al. [21] | ✓ | ✓ | |
| Parrington et al. [32] | ✓ | ✓ | |
| Pitt et al. [34] | ✓ | ||
| Shan Chou et al. [27] | ✓—obstacle crossing | ||
| Vallée et al. [23] | ✓—obstacle crossing | ||
| Williams et al. [22] | ✓ |
4. Discussion
4.1. Instrumentation
4.2. Outcome Measures
4.3. Protocols
4.4. Outcome Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute of Neurological Disorders Traumatic Brain Injury Information Page. National Institute of Neurological Disorders and Stroke. Available online: https://www.ninds.nih.gov/Disorders/All-Disorders/Traumatic-Brain-Injury-Information-Page (accessed on 28 February 2020).
- Shaw, N.A. The neurophysiology of concussion. Prog. Neurobiol. 2002, 67, 281–344. [Google Scholar] [CrossRef]
- Cassidy, J.D.; Carroll, L.J.; Peloso, P.M.; Borg, J.; von Holst, H.; Holm, L.; Kraus, J.; Coronado, V.G. Incidence, risk factors and prevention of mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. Suppl. 2004, 36, 28–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mild Traumatic Brain Injury Committee of the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87.
- Kay, T.; Harrington, D.E.; Adams, R.; Anderson, T.; Berrol, S.; Cicerone, K.; Dahlberg, C.; Gerber, D.; Goka, R.; Harley, P.; et al. Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87. [Google Scholar] [CrossRef]
- Lund, S.B.; Gjeilo, K.H.K.H.; Moen, K.G.; Schirmer-Mikalsen, K.; Skandsen, T.; Vik, A. Moderate traumatic brain injury, acute phase course and deviations in physiological variables: An observational study. Scand. J. Trauma. Resusc. Emerg. Med. 2016, 24, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolias, A.G.; Guilfoyle, M.R.; Helmy, A.; Allanson, J.; Hutchinson, P.J. Traumatic brain injury in adults. Pract. Neurol. 2013, 13, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, C.; Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Kleffelgaard, I.; Roe, C.; Soberg, H.L.; Bergland, A. Associations among self-reported balance problems, post-concussion symptoms and performance-based tests: A longitudinal follow-up study. Disabil. Rehabil. 2012, 34, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Alsalaheen, B.A.; Mucha, A.; Morris, L.O.; Whitney, S.L.; Furman, J.M.; Camiolo-Reddy, C.E.; Collins, M.W.; Lovell, M.R.; Sparto, P.J. Vestibular rehabilitation for dizziness and balance disorders after concussion. J. Neurol. Phys. 2010, 34, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Broglio, S.P.; Cantu, R.C.; Gioia, G.A.; Guskiewicz, K.M.; Kutcher, J.; Palm, M.; McLeod, T.C.V. National athletic trainers’ association position statement: Management of sport concussion. J. Athl. Train. 2014, 49, 245–265. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.; Kuh, D.; Hardy, R. Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, 639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.; Kuh, D.; Cooper, C.; Gale, C.R.; Lawlor, D.A.; Matthews, F.; Hardy, R. Objective measures of physical capability and subsequent health: A systematic review. Age Ageing 2011, 40, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnoff, J.T.; Peterson, V.J.; Hollman, J.H.; Smith, J. Intrarater and Interrater Reliability of the Balance Error Scoring System (BESS). PM&R 2009, 1, 50–54. [Google Scholar] [CrossRef]
- Stuart, S.; Parrington, L.; Morris, R.; Martini, D.N.; Fino, P.C.; King, L.A. Gait measurement in chronic mild traumatic brain injury: A model approach. Hum. Mov. Sci. 2020, 69, 102557. [Google Scholar] [CrossRef] [PubMed]
- Fino, P.C.; Parrington, L.; Pitt, W.; Martini, D.N.; Chesnutt, J.C.; Chou, L.S.; King, L.A. Detecting gait abnormalities after concussion or mild traumatic brain injury: A systematic review of single-task, dual-task, and complex gait. Gait Posture 2018, 62, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an Accelerometer to Quantify a Comprehensive Battery of Gait Characteristics in Healthy Older Adults and Parkinson’s Disease: Toward Clinical and at Home Use. IEEE J. Biomed. Heal. Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Head Injury: Assessment and Early Management Clinical Guideline; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Pozzato, I.; Meares, S.; Kifley, A.; Craig, A.; Gillett, M.; Van Vu, K.; Liang, A.; Cameron, I.; Gopinath, B. Challenges in the acute identification of mild traumatic brain injuries: Results from an emergency department surveillance study. BMJ Open 2020, 10, 34494. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.; Stuart, S.; Godfrey, A. Sports related concussion: An emerging era in digital sports technology. NPJ Digit. Med. 2021, 4, 1–8. [Google Scholar] [CrossRef]
- Parker, T.M.; Osternig, L.R.; van Donkelaar, P.; Chou, L.S. Balance control during gait in athletes and non-athletes following concussion. Med. Eng. Phys. 2008, 30, 959–967. [Google Scholar] [CrossRef]
- Williams, G.; Morris, M.E.; Schache, A.; McCrory, P.R. Incidence of Gait Abnormalities After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2009, 90, 587–593. [Google Scholar] [CrossRef]
- Vallée, M.; McFadyen, B.J.; Swaine, B.; Doyon, J.; Cantin, J.F.; Dumas, D. Effects of Environmental Demands on Locomotion After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2006, 87, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Belluscio, V.; Bergamini, E.; Tramontano, M.; Bustos, A.O.; Allevi, G.; Formisano, R.; Vannozzi, G.; Buzzi, M.G. Gait quality assessment in survivors from severe traumatic brain injury: An instrumented approach based on inertial sensors. Sensors 2019, 19, 5315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFadyen, B.J.; Swaine, B.; Dumas, D.; Durand, A. Residual Effects of a Traumatic Brain Injury on Locomotor Capacity: A First Study of Spatiotemporal Patterns during Unobstructed and Obstructed Walking. J. Head Trauma Rehabil. 2003, 18, 512–525. [Google Scholar] [CrossRef]
- Basford, J.R.; Chou, L.S.; Kaufman, K.R.; Brey, R.H.; Walker, A.; Malec, J.F.; Moessner, A.M.; Brown, A.W. An assessment of gait and balance deficits after traumatic brain injury. Arch. Phys. Med. Rehabil. 2003, 84, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.S.; Kaufman, K.R.; Walker-Rabatin, A.E.; Brey, R.H.; Basford, J.R. Dynamic instability during obstacle crossing following traumatic brain injury. Gait Posture 2004, 20, 245–254. [Google Scholar] [CrossRef]
- Fino, P.C.; Peterka, R.J.; Hullar, T.E.; Murchison, C.; Horak, F.B.; Chesnutt, J.C.; King, L.A. Assessment and rehabilitation of central sensory impairments for balance in mTBI using auditory biofeedback: A randomized clinical trial. BMC Neurol. 2017, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Fino, P.C. A preliminary study of longitudinal differences in local dynamic stability between recently concussed and healthy athletes during single and dual-task gait. J. Biomech. 2016, 49, 1983–1988. [Google Scholar] [CrossRef] [Green Version]
- Oldham, J.R.; Howell, D.R.; Bryk, K.N.; Lanois, C.J.; Koerte, I.K.; Meehan, W.P.; Buckley, T.A. No differences in tandem gait performance between male and female athletes acutely post-concussion. J. Sci. Med. Sport 2020, 23, 814–819. [Google Scholar] [CrossRef]
- Martini, D.N.; Parrington, L.; Stuart, S.; Fino, P.C.; King, L.A. Gait Performance in People with Symptomatic, Chronic Mild Traumatic Brain Injury. J. Neurotrauma 2021, 38, 218–224. [Google Scholar] [CrossRef]
- Parrington, L.; Fino, P.C.; Swanson, C.W.; Murchison, C.F.; Chesnutt, J.; King, L.A. Longitudinal assessment of balance and gait after concussion and return to play in collegiate athletes. J. Athl. Train. 2019, 54, 429–438. [Google Scholar] [CrossRef]
- Fino, P.C.; Nussbaum, M.A.; Brolinson, P.G. Locomotor deficits in recently concussed athletes and matched controls during single and dual-task turning gait: Preliminary results. J. Neuroeng. Rehabil. 2016, 13, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitt, W.; Chen, S.H.; Chou, L.S. Using IMU-based kinematic markers to monitor dual-task gait balance control recovery in acutely concussed individuals. Clin. Biomech. 2020, 80, 105145. [Google Scholar] [CrossRef] [PubMed]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and reliability ofwearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfrey, A.; Conway, R.; Meagher, D.; ÓLaighin, G. Direct measurement of human movement by accelerometry. Med. Eng. Phys. 2008, 30, 1364–1386. [Google Scholar] [CrossRef]
- Morris, R.; Stuart, S.; Mcbarron, G.; Fino, P.C.; Mancini, M.; Curtze, C. Validity of mobility lab (version 2) for gait assessment in young adults, older adults and Parkinson’s disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef]
- Howell, D.R.; Osternig, L.R.; Chou, L.-S. Return to Activity after Concussion Affects Dual-Task Gait Balance Control Recovery. Recover. Med. Sci. Sport. Exerc 2015, 47, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef]
- Oldham, J.R.; DiFabio, M.S.; DeWolf, R.M.; Kaminski, T.W.; Buckley, T.A. Tandem gait performance following concussion. Br. J. Sports Med. 2017, 51, A57. [Google Scholar] [CrossRef]
- Wade, D.T.; Collen, F.M.; Robb, G.F.; Warlow, C.P. Physiotherapy intervention late after stroke and mobility. Br. Med. J. 1992, 304, 609–613. [Google Scholar] [CrossRef] [Green Version]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [Green Version]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, D.A.; Leasure, J.L.; Schallert, T. The control of movement following traumatic brain injury. Compr. Physiol. 2013, 3, 121–139. [Google Scholar] [CrossRef] [PubMed]
- Von der Malsburg, T.; Angele, B. False positives and other statistical errors in standard analyses of eye movements in reading. J. Mem. Lang. 2017, 94, 119–133. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.J. Automaticity of walking: Functional significance, mechanisms, measurement and rehabilitation strategies. Front. Hum. Neurosci. 2015, 9, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, M.; El-Gohary, M.; Pearson, S.; Mcnames, J.; Schlueter, H.; Nutt, J.G.; King, L.A.; Horak, F.B. Continuous monitoring of turning in Parkinson’s disease: Rehabilitation potential. Neuro Rehabil. 2015, 37, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Stuart, S.; Parrington, L.; Martini, D.N.; Kreter, N.; Chesnutt, J.C.; Fino, P.C.; King, L.A. Analysis of Free-Living Mobility in People with Mild Traumatic Brain Injury and Healthy Controls: Quality over Quantity. J. Neurotrauma 2020, 37, 139–145. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Atsumori, H. Noninvasive imaging of prefrontal activation during attention-demanding tasks performed while walking using a wearable optical topography system. J. Biomed. Opt. 2010, 15, 046002. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA J. Am. Med. Assoc. 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Nóbrega-Sousa, P.; Gobbi, L.T.B.; Orcioli-Silva, D.; da Conceição, N.R.; Beretta, V.S.; Vitório, R. Prefrontal Cortex Activity During Walking: Effects of Aging and Associations with Gait and Executive Function. Neurorehabil. Neural Repair 2020, 34, 915–924. [Google Scholar] [CrossRef]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dever, A.; Powell, D.; Graham, L.; Mason, R.; Das, J.; Marshall, S.J.; Vitorio, R.; Godfrey, A.; Stuart, S. Gait Impairment in Traumatic Brain Injury: A Systematic Review. Sensors 2022, 22, 1480. https://doi.org/10.3390/s22041480
Dever A, Powell D, Graham L, Mason R, Das J, Marshall SJ, Vitorio R, Godfrey A, Stuart S. Gait Impairment in Traumatic Brain Injury: A Systematic Review. Sensors. 2022; 22(4):1480. https://doi.org/10.3390/s22041480
Chicago/Turabian StyleDever, Anthony, Dylan Powell, Lisa Graham, Rachel Mason, Julia Das, Steven J. Marshall, Rodrigo Vitorio, Alan Godfrey, and Samuel Stuart. 2022. "Gait Impairment in Traumatic Brain Injury: A Systematic Review" Sensors 22, no. 4: 1480. https://doi.org/10.3390/s22041480
APA StyleDever, A., Powell, D., Graham, L., Mason, R., Das, J., Marshall, S. J., Vitorio, R., Godfrey, A., & Stuart, S. (2022). Gait Impairment in Traumatic Brain Injury: A Systematic Review. Sensors, 22(4), 1480. https://doi.org/10.3390/s22041480