
Hand Motion Analysis during the Execution of the Action Research Arm Test Using Multiple Sensors

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
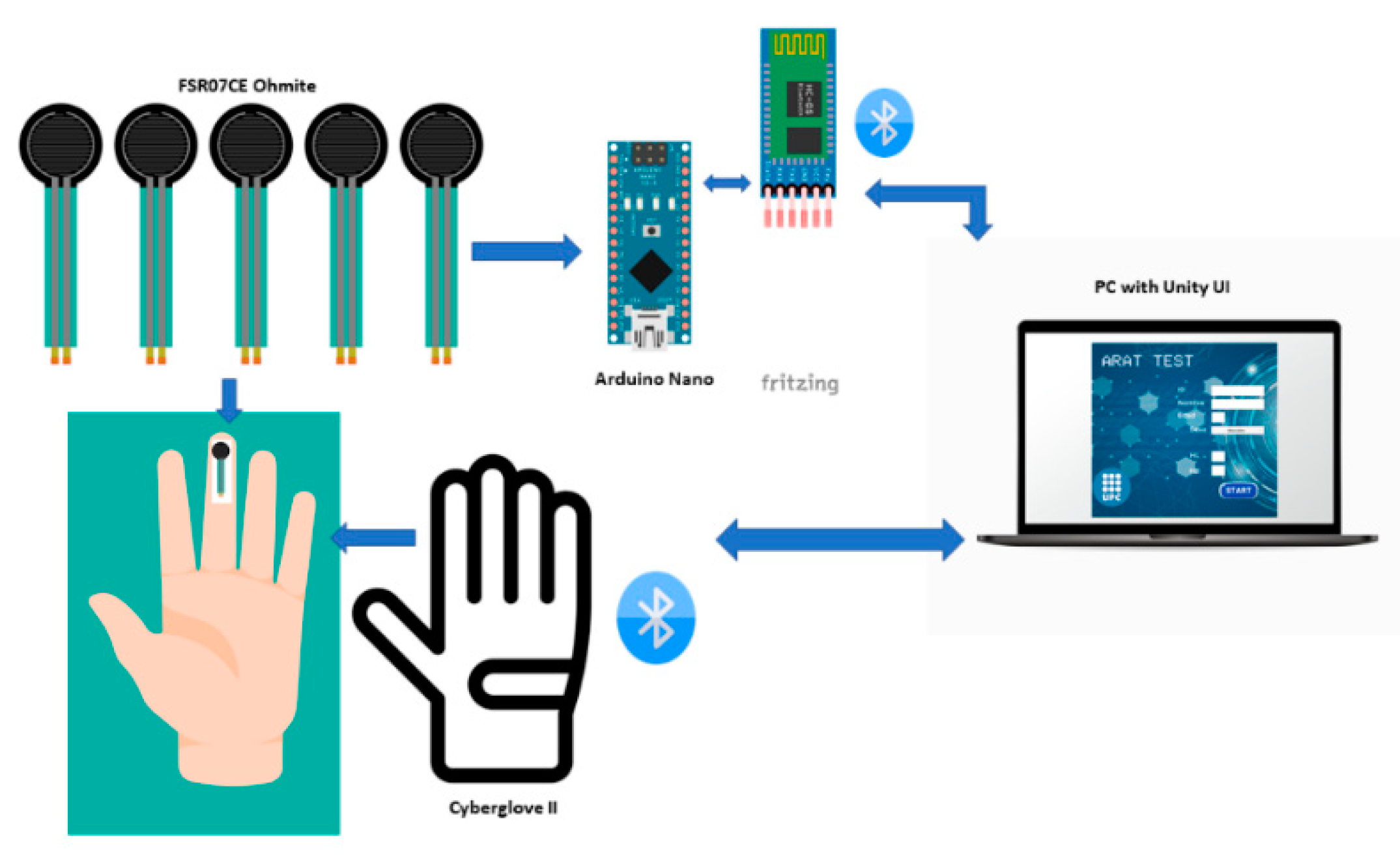
2.1. Measurement System
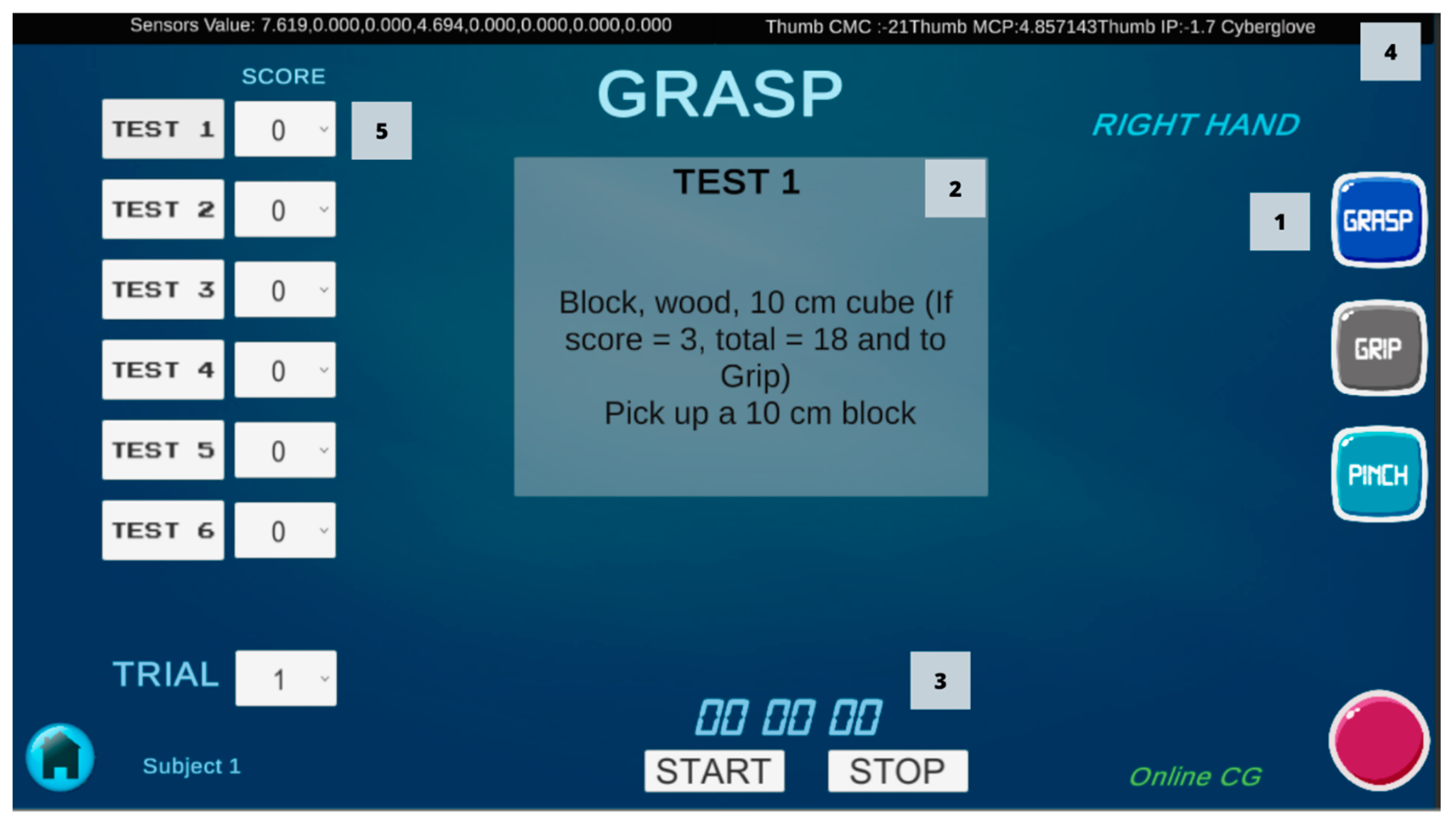
2.2. ARAT Test
2.3. Participants
2.4. Experimental Setup
2.5. Statistical Analysis
3. Results
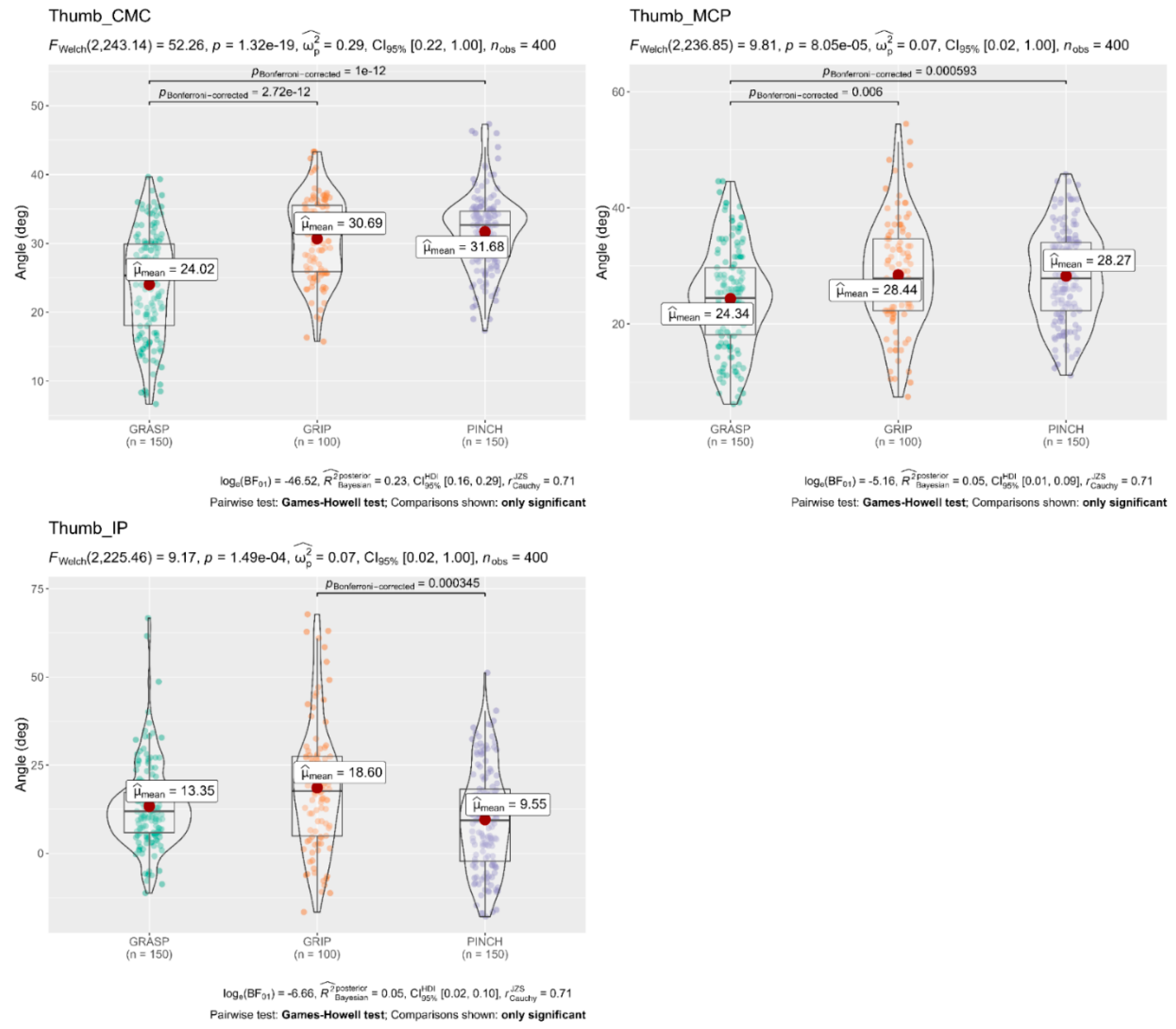
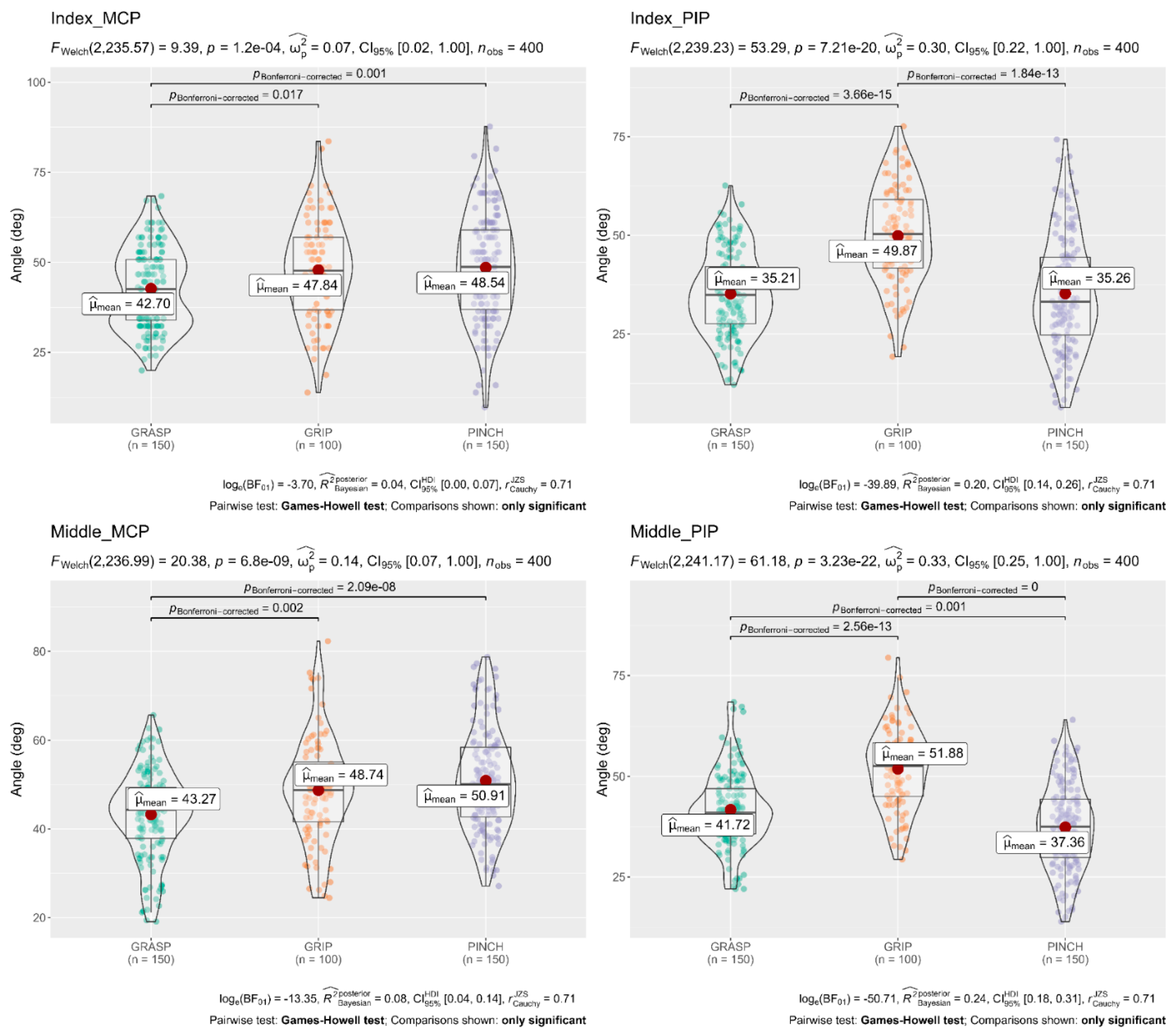
3.1. Joint Flexion Angles
3.2. Pinch Subscale t-Test
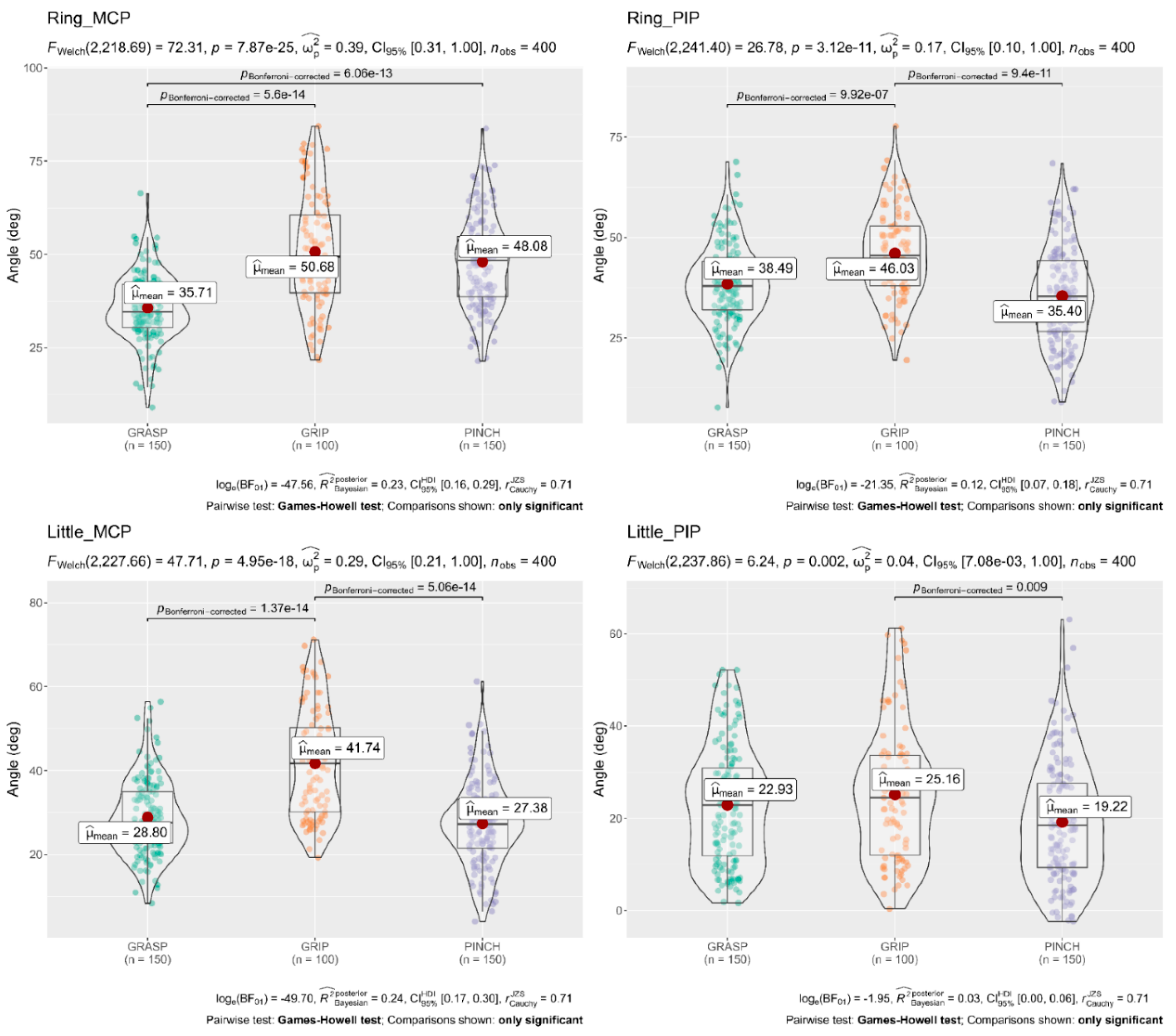
3.3. Grasp, Grip, and Pinch Subscales
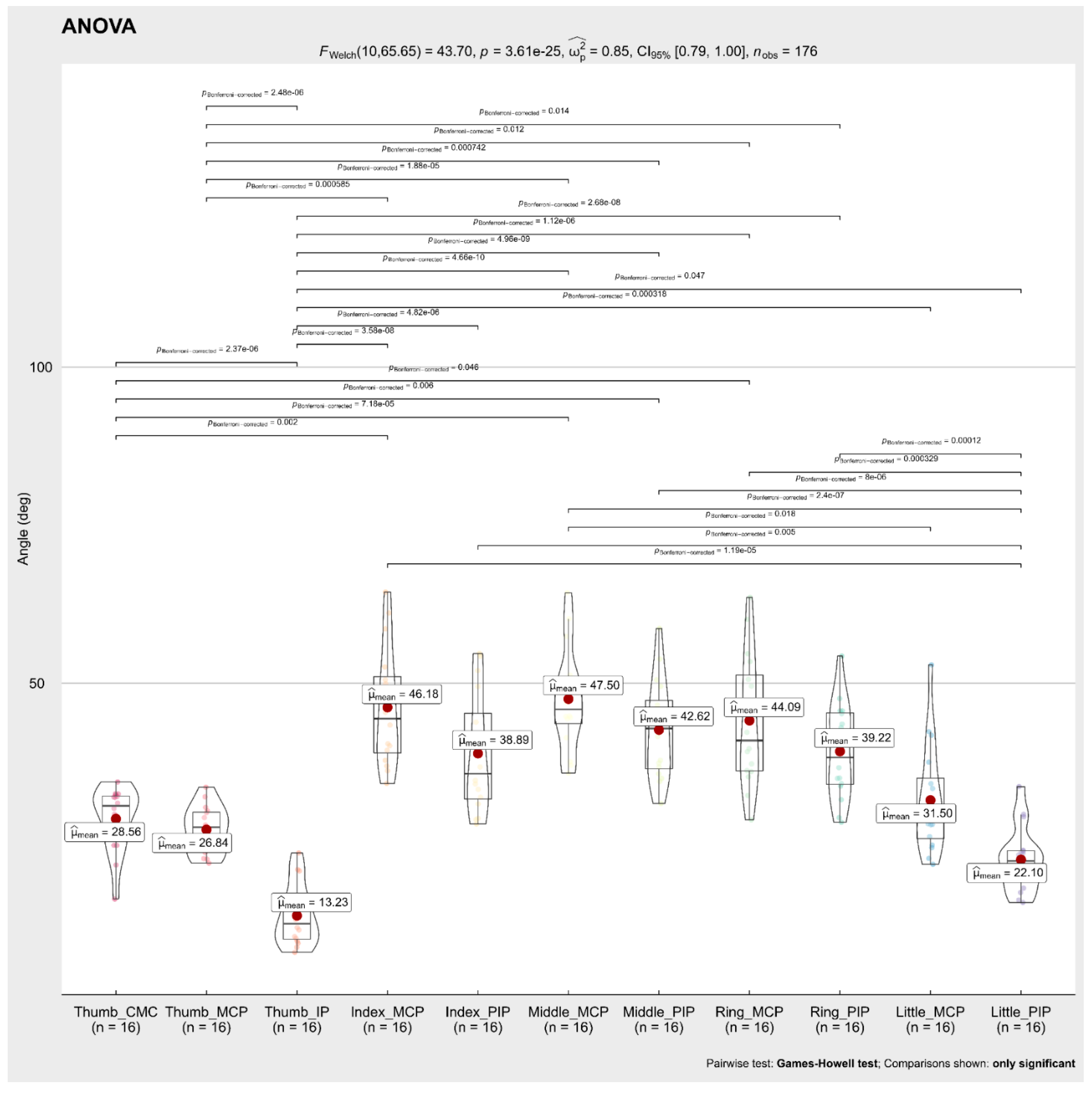
3.4. Flexion Angle of Each Finger Joint during the 16 Tests
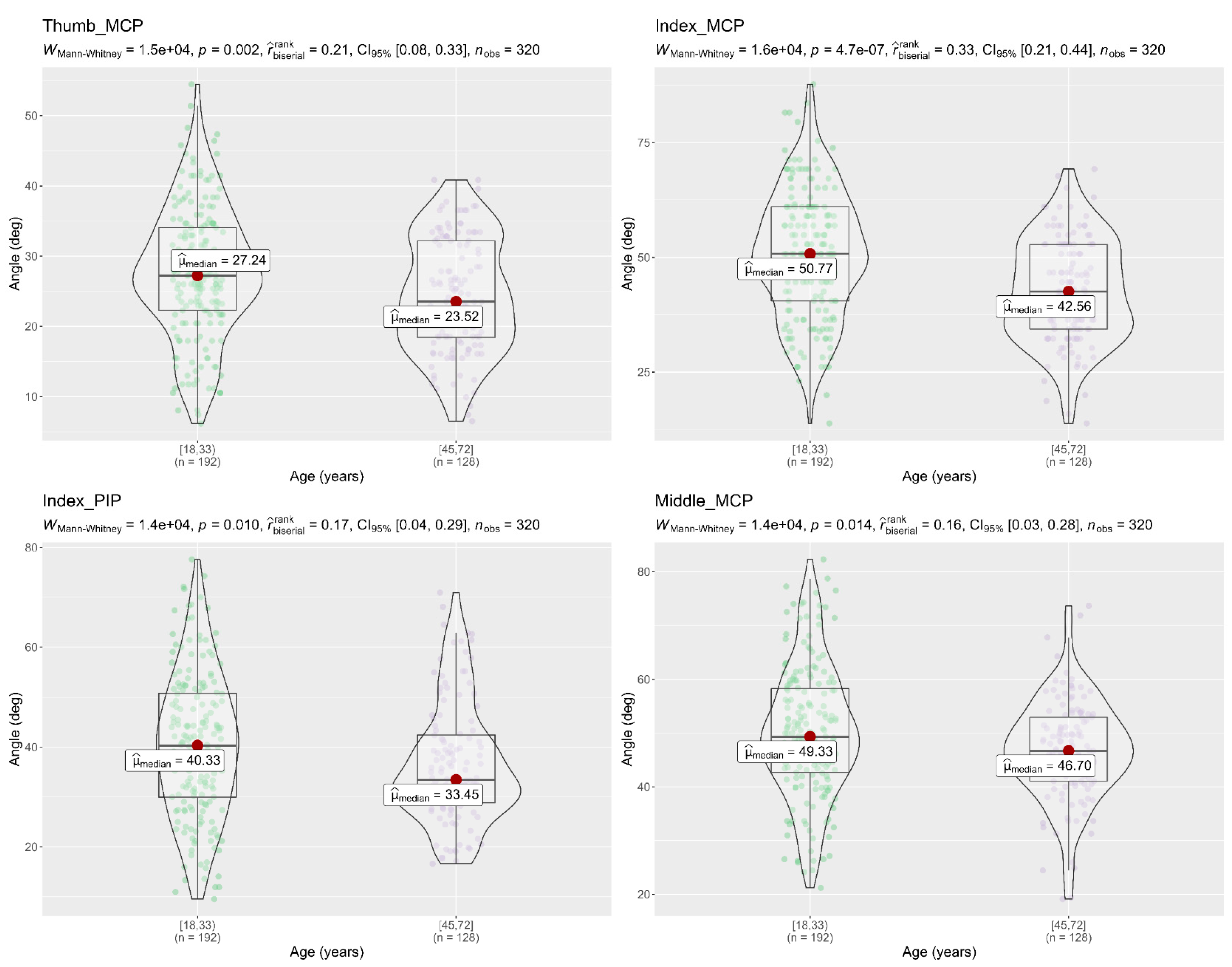
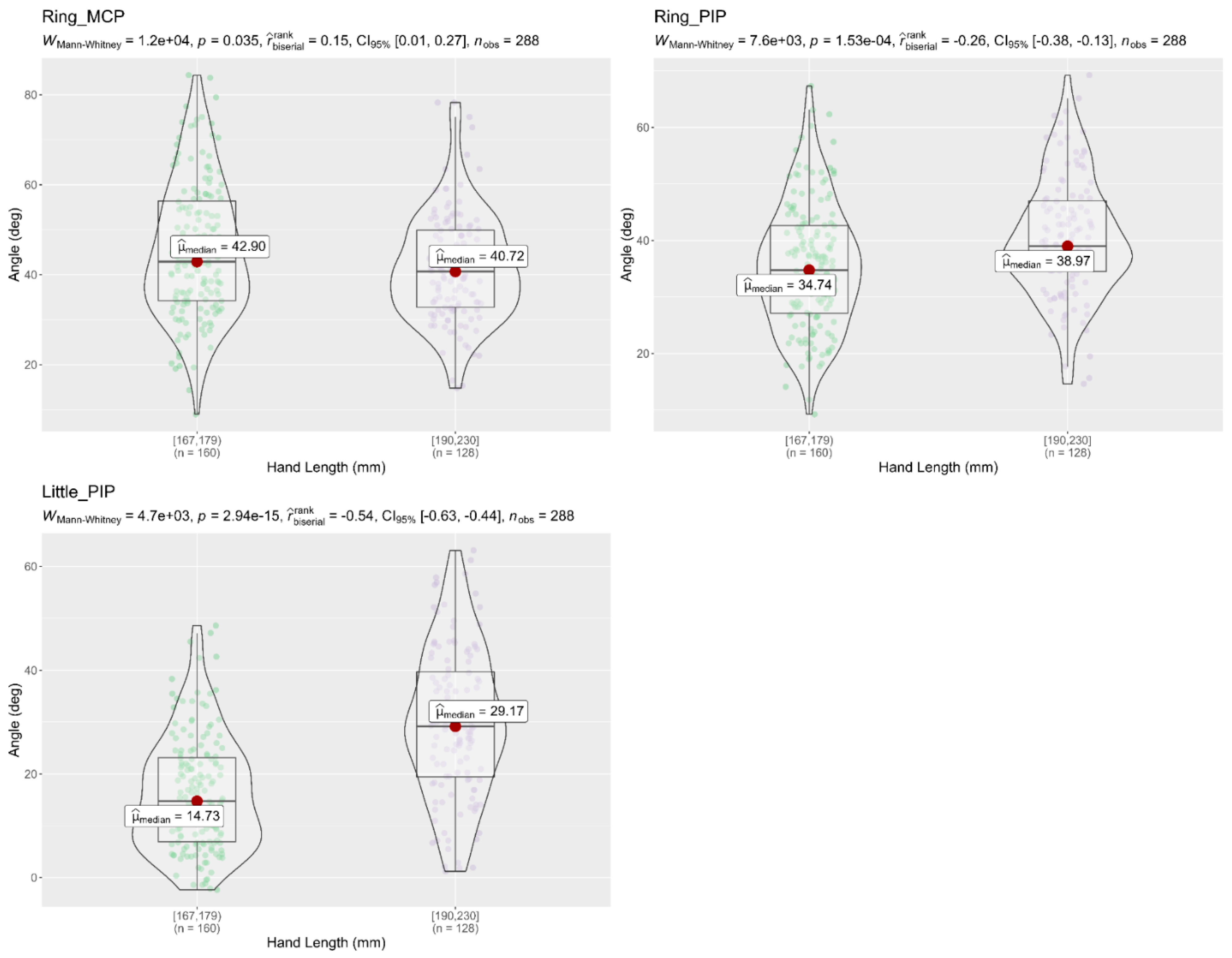
3.5. Differences in the Flexion Angles Respect to Age and Hand Length Groups
3.6. Fingertip Forces
3.7. Differences in Fingertip Force with Respect to Age Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maw, J.; Wong, K.Y.; Gillespie, P. Hand Anatomy. Br. J. Hosp. Med. 2016, 77, C34–C40. [Google Scholar] [CrossRef] [PubMed]
- Dolan, D. Hope Through Research. Neurol. Now 2014, 10, 69–71. [Google Scholar] [CrossRef]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, S.; Baalbergen, E. Post-Stroke Rehabilitation. S. Afr. Med. J. 2019, 109, 81–83. [Google Scholar] [CrossRef] [Green Version]
- Santisteban, L.; Térémetz, M.; Bleton, J.P.; Baron, J.C.; Maier, M.A.; Lindberg, P.G. Upper Limb Outcome Measures Used in Stroke Rehabilitation Studies: A Systematic Literature Review. PLoS ONE 2016, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.E.; Crowner, B.E.; Kluding, P.M.; Nichols, D.; Rose, D.K.; Yoshida, R.; Pinto Zipp, G. Outcome Measures for Individuals with Stroke: Process and Recommendations from the American Physical Therapy Association Neurology Section Task Force. Phys. Ther. 2013, 93, 1383–1396. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.; Hussein, N.; Mirkowski, M.; Vanderlaan, D.; Saikaley, M.; Longval, M.; Iruthayarajah, J. Stroke Rehabilitation Clinician Handbook 2020; Heart and Stroke Foundation: Ottawa, ON, Canada, 2020; pp. 1–60. [Google Scholar]
- Yozbatiran, N.; Der-Yeghiaian, L.; Cramer, S.C. A Standardized Approach to Performing the Action Research Arm Test. Neurorehabil. Neural Repair 2008, 22, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Y.; Ju, Z.; Xiang, K.; Chen, J.; Liu, H. Multimodal Human Hand Motion Sensing and Analysis-A Review. IEEE Trans. Cogn. Dev. Syst. 2019, 11, 162–175. [Google Scholar] [CrossRef]
- Lin, B.-S.; Hsiao, P.-C.; Yang, S.-Y.; Su, C.-S.; Lee, I.-J. Data Glove System Embedded With Inertial Measurement Units for Hand Function Evaluation in Stroke Patients. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2204–2213. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; Sazonov, E. Using Sensors to Measure Activity in People with Stroke. Top. Stroke Rehabil. 2011, 18, 746–757. [Google Scholar] [CrossRef] [PubMed]
- Ambar, R.; Ahmad, M.; Mohd Ali, A.; Abdul Jamil, M. Arduino Based Arm Rehabilitation Assistive Device. J. Eng. Technol. 2011, 1, 5–13. [Google Scholar]
- Hoda, M.; Hoda, Y.; Hafidh, B.; El Saddik, A. Predicting Muscle Forces Measurements from Kinematics Data Using Kinect in Stroke Rehabilitation. Multimed. Tools Appl. 2018, 77, 1885–1903. [Google Scholar] [CrossRef]
- Hsiao, P.C.; Yang, S.Y.; Lin, B.S.; Lee, I.J.; Chou, W. Data Glove Embedded with 9-Axis IMU and Force Sensing Sensors for Evaluation of Hand Function. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4631–4634. [Google Scholar] [CrossRef]
- Kim, W.S.; Cho, S.; Baek, D.; Bang, H.; Paik, N.J. Upper Extremity Functional Evaluation by Fugl-Meyer Assessment Scoring Using Depth-Sensing Camera in Hemiplegic Stroke Patients. PLoS ONE 2016, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Bhagubai, M.M.C.; Wolterink, G.; Held, J.P.O.; Luft, A.R.; Veltink, P.H. Assessment of Upper Limb Movement Impairments after Stroke Using Wearable Inertial Sensing. Sensors 2020, 20, 4770. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative Assessment of Upper Limb Motor Function in Multiple Sclerosis Using an Instrumented Action Research Arm Test. J. Neuroeng. Rehabil. 2014, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S.; Lee, W.H.; Seo, H.G.; Kim, Y.J.; Bang, M.S.; Kim, S. Inertial Measurement Unit Based Upper Extremity Motion Characterization for Action Research Arm Test and Activities of Daily Living. Sensors 2019, 19, 1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ticó Falguera, N. Biomecànica dels Dits de la mà com a Factor Pronòstic de la Recuperació Funcional de L’extremitat Parètica en Pacients amb Ictus Aguts; Universitat Politècnica de Catalunya: Barcelona, Spain, 2016. [Google Scholar]
- Held, J.P.O.; Klaassen, B.; Eenhoorn, A.; van Beijnum, B.J.F.; Buurke, J.H.; Veltink, P.H.; Luft, A.R. Inertial Sensor Measurements of Upper-Limb Kinematics in Stroke Patients in Clinic and Home Environment. Front. Bioeng. Biotechnol. 2018, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Repnik, E.; Puh, U.; Goljar, N.; Munih, M.; Mihelj, M. Using Inertial Measurement Units and Electromyography to Quantify Movement during Action Research Arm Test Execution. Sensors 2018, 18, 2767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CyberGlove Systems Inc.© CyberGlove II. Available online: http://www.cyberglovesystems.com/cyberglove-ii (accessed on 21 June 2019).
- Peña-Pitarch, E.; Falguera, N.T.; Yang, J. Virtual Human Hand: Model and Kinematics. Comput. Methods Biomech. Biomed. Engin. 2014, 17, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Peña-Pitarch, E.; Costa, J.V.; Martinez, J.L.; Al Omar, A.; Larrión, I.A.; Tico-Falguera, N. Introductory Analysis of Human Upper Extremity After Stroke. Int. J. Priv. Health Inf. Manag. 2018, 7, 45–60. [Google Scholar] [CrossRef] [Green Version]
- Ohmite FSR Series (Datasheet). Available online: https://www.ohmite.com/assets/docs/res_fsr.pdf (accessed on 20 July 2020).
- Flórez, J.A.; Velásquez, A. Calibration of Force Sensing Resistors (Fsr) for Static and Dynamic Applications. In Proceedings of the 2010 IEEE ANDESCON, Bogota, Colombia, 15–17 September 2010; pp. 1–6. [Google Scholar] [CrossRef]
- Hsu, W.C.; Sugiarto, T.; Chen, J.W.; Lin, Y.J. The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot. Sensors 2018, 18, 3617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, Q.; Seyedi, M.; Cai, Z.; Lai, D.T.H. Force-Sensing Glove System for Measurement of Hand Forces during Motorbike Riding. Int. J. Distrib. Sens. Netw. 2015. [Google Scholar] [CrossRef]
- ITead Studio HC—05—Bluetooth to Serial Port Module (Datasheet). Available online: https://datasheetspdf.com/pdf-file/1418730/ITead/HC-05/ (accessed on 10 July 2020).
- Unity Technologies Unity User Manual 2020.3 (LTS). Available online: https://docs.unity3d.com/Manual/index.html (accessed on 15 June 2020).
- Lyle, R.C. A Performance Test for Assessment of Upper Limb Function in Physical Rehabilitation Treatment and Research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Rijpkema, H.; Girard, M. Computer Animation of Knowledge-Based Human Grasping. In Proceedings of the 18th annual conference on Computer graphics and interactive techniques, SIGGRAPH 1991, Las Vegas, NV, USA, 28 July–2 August 1991; pp. 339–348. [Google Scholar]
- Lee, J.W.; Rim, K. Measurement of Finger Joint Angles and Maximum Finger Forces during Cylinder Grip Activity. J. Biomed. Eng. 1991, 13, 152–162. [Google Scholar] [CrossRef]
- Shimawaki, S.; Murai, T.; Nakabayashi, M.; Sugimoto, H. Measurement of Flexion Angle of the Finger Joint during Cylinder Gripping Using a Three-Dimensional Bone Model Built by X-Ray Computed Tomography. Appl. Bionics Biomech. 2019, 2019, 2839648. [Google Scholar] [CrossRef] [PubMed]
- Shimawaki, S.; Nakamura, Y.; Nakabayashi, M.; Sugimoto, H. Flexion Angles of Finger Joints in Two-Finger Tip Pinching Using 3D Bone Models Constructed from X-ray Computed Tomography (CT) Images. Appl. Bionics Biomech. 2020, 2020, 8883866. [Google Scholar] [CrossRef] [PubMed]
- Yokogawa, R.; Hara, K. Manipulabilities of the Index Finger and Thumb in Three Tip-Pinch Postures. J. Biomech. Eng. 2004, 126, 212–219. [Google Scholar] [CrossRef]
- Murai, T.; Uchiyama, S.; Nakamura, K.; Ido, Y.; Hata, Y.; Kato, H. Functional Range of Motion in the Metacarpophalangeal Joints of the Hand Measured by Single Axis Electric Goniometers. J. Orthop. Sci. 2018, 23, 504–510. [Google Scholar] [CrossRef]
- Hume, M.C.; Gellman, H.; McKellop, H.; Brumfield, R.H. Functional Range of Motion of the Joints of the Hand. J. Hand Surg. Am. 1990, 15, 240–243. [Google Scholar] [CrossRef]
- Bain, G.I.; Polites, N.; Higgs, B.G.; Heptinstall, R.J.; McGrath, A.M. The Functional Range of Motion of the Finger Joints. J. Hand Surg. Eur. Vol. 2015, 40, 406–411. [Google Scholar] [CrossRef]
- Smahel, Z.; Klímová, A. The Influence of Age and Exercise on the Mobility of Hand Joints: 1: Metacarpophalangeal Joints of the Three-Phalangeal Fingers. Acta Chir. Plast. 2004, 46, 81–88. [Google Scholar] [PubMed]
- De Smet, L.; Urlus, M.; Spriet, A.; Fabry, G. Metacarpophalangeal and Interphalangeal Flexion of the Thumb: Influence of Sex and Age, Relation to Ligamentous Injury. Acta Orthop. Belg. 1993, 59, 357–359. [Google Scholar] [PubMed]
- Peña-Pitarch, E.; Magaña, J.F.P.; Ticó-Falguera, N.; Al Omar, A.; Larrión, I.A.; Costa, J.V. Virtual Human Hand: Grasps and Fingertip Deformation. Adv. Intell. Syst. Comput. 2020, 975, 484–492. [Google Scholar]
- Cech, D.J. Chapter 14—Prehension. In Functional Movement Development Across the Life Span; Elsevier: Amsterdam, The Netherlands, 2012; pp. 309–334. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test | Item (Size) | Description |
|---|---|---|
| Grasp subscale | ||
| 1 | Block, 10 cm3 | Grasp, lift vertically, place, and release the item onto the top of the shelf. |
| 2 | Block, 2.5 cm3 | |
| 3 | Block, 5 cm3 | |
| 4 | Block, 7.5 cm3 | |
| 5 | Cricket ball (Diameter, 7 cm) | |
| 6 | Sharpening stone (10.0 × 2.5 × 1 cm) | |
| Grip Subscale | ||
| 7 | Two plastic tumblers (Upper diameter, 7 cm; lower diameter, 6 cm; height, 12 cm) | Pour water from one glass into another. |
| 8 | Displace alloy tube (Diameter,2.25 cm) | Displace from one side of the table to the other. |
| 9 | Displace alloy tube (Diameter,1 cm) | Displace from one side of the table to the other. |
| 10 | Put washer over bolt (Diameter, 0.5 cm) | Put washer over the bolt. |
| Pinch subscale | ||
| 11 | Ball-bearing (Diameter, 6 mm) | Held the ball-bearing between ring and thumb finger. |
| 12 | Marble (Diameter, 1.6 cm) | Held the marble between index and thumb finger. |
| 13 | Ball-bearing (Diameter, 6 mm) | Held the ball-bearing between middle and thumb finger. |
| 14 | Ball-bearing (Diameter, 6 mm) | Held the ball-bearing between index and thumb finger. |
| 15 | Marble (Diameter, 1.6 cm) | Held the marble between ring and thumb finger. |
| 16 | Marble (Diameter, 1.6 cm) | Held the marble between middle and thumb finger. |
| Subject Data | Descriptive Statistics | |||
|---|---|---|---|---|
| Mean | SD | Min | Max | |
| Age (years) | 40.2 | 18.1 | 18.0 | 72.0 |
| HL (mm) | 176.6 | 4.4 | 167.0 | 184.0 |
| HB (mm) | 75.4 | 3.8 | 70.0 | 84.0 |
| Test | Thumb | Index | Middle | Ring | Little | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CMC (deg) | MCP (deg) | IP (deg) | MCP (deg) | PIP (deg) | MCP (deg) | PIP (deg) | MCP (deg) | PIP (deg) | MCP (deg) | PIP (deg) | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| 1 | 15.9 | 27.6 | 20.3 | 36.1 | 33.2 | 37 | 46.5 | 28.4 | 45.6 | 22.3 | 29.3 |
| (6.0) | (9.0) | (12.0) | (9.4) | (11.9) | (10.3) | (6.7) | (9.0) | (6.4) | (6.4) | (14.3) | |
| 2 | 27.3 | 23.8 | 9.6 | 49.9 | 32 | 50.1 | 35.7 | 39.2 | 31.6 | 27.6 | 19.3 |
| (6.5) | (8.4) | (6.8) | (7.6) | (9.8) | (6.6) | (7.7) | (7.6) | (10.1) | (8.2) | (12.1) | |
| 3 | 24.4 | 22.2 | 9.9 | 40.4 | 34.6 | 44.4 | 37.8 | 36.2 | 34.9 | 27.7 | 19.6 |
| (6.4) | (9.5) | (8.0) | (9.4) | (9.6) | (7.7) | (6.5) | (5.3) | (6.8) | (7.5) | (12.4) | |
| 4 | 21.2 | 23.2 | 11.3 | 37.8 | 36.8 | 37.6 | 44.1 | 32.2 | 39.9 | 27.8 | 22.8 |
| (6.6) | (9.6) | (10.8) | (9.5) | (12.8) | (9.6) | (7.2) | (8.2) | (8.8) | (6.0) | (13.2) | |
| 5 | 24.3 | 22.3 | 13.1 | 39.4 | 34.1 | 41.4 | 36.7 | 36 | 33.7 | 34.1 | 23.5 |
| (5.8) | (8.3) | (10.2) | (10) | (7.9) | (8.9) | (5.5) | (6.0) | (6.1) | (8.7) | (10.5) | |
| 6 | 31.0 | 27.0 | 15.8 | 52.6 | 40.6 | 49.2 | 49.5 | 42.2 | 45.2 | 33.3 | 23.1 |
| (4.9) | (7.2) | (17.9) | (9.4) | (9.7) | (7.5) | (10.1) | (9.5) | (10.8) | (11.7) | (12.4) | |
| 7 | 25.7 | 21.5 | 15.5 | 34.1 | 41.1 | 35.8 | 44.5 | 35.2 | 36.6 | 30 | 20.2 |
| (5.4) | (8.3) | (12.6) | (10.1) | (9.3) | (7.8) | (6.7) | (9.7) | (7.8) | (5.0) | (11.7) | |
| 8 | 32.1 | 29.8 | 15.2 | 48.1 | 49.5 | 50.5 | 50.5 | 50.6 | 45.6 | 41.8 | 23.6 |
| (4.9) | (8.3) | (15.4) | (9.2) | (10.2) | (6.5) | (8.6) | (12.1) | (8.5) | (10.4) | (12.6) | |
| 9 | 32.5 | 30.4 | 23.1 | 50.5 | 54.2 | 51.3 | 53.8 | 53.4 | 47.6 | 42.3 | 23.2 |
| (5.5) | (8.9) | (21.4) | (10.3) | (11.1) | (7.1) | (8.8) | (12.3) | (9.1) | (11.2) | (13.4) | |
| 10 | 32.5 | 32 | 20.5 | 58.6 | 54.7 | 57.4 | 58.6 | 63.5 | 54.3 | 52.9 | 33.6 |
| (5.5) | (9.2) | (20.6) | (12.4) | (13.8) | (12.6) | (10.5) | (12.1) | (11) | (12.2) | (16.4) | |
| 11 | 34.4 | 33.5 | 9.2 | 36.9 | 28.4 | 44.7 | 41.6 | 60.1 | 43.5 | 37.5 | 28.9 |
| (6.0) | (7.4) | (14.9) | (12.7) | (12.1) | (9.7) | (10.9) | (11.5) | (11.2) | (8.5) | (15.7) | |
| 12 | 29.3 | 24.6 | 12.6 | 61.1 | 43.8 | 44.8 | 34.9 | 39.6 | 28.7 | 24.0 | 17.6 |
| (5.2) | (6.9) | (16.8) | (8.9) | (10.1) | (7.1) | (10) | (8.6) | (11.2) | (9.9) | (11.7) | |
| 13 | 32 | 28.7 | 8.9 | 45.4 | 30.9 | 64.3 | 44.8 | 59.5 | 43 | 25.7 | 16.9 |
| (5.8) | (8.6) | (14.2) | (11.2) | (11.3) | (9.2) | (11) | (9.3) | (11.8) | (9.1) | (11.8) | |
| 14 | 31.9 | 27.4 | 11.0 | 64.4 | 52 | 46.9 | 34.5 | 37.2 | 28 | 21.4 | 15.7 |
| (4.4) | (8.3) | (13.5) | (9.6) | (13.2) | (7.0) | (8.9) | (8.1) | (10.5) | (7.3) | (11.5) | |
| 15 | 32.3 | 29.5 | 8.2 | 40.1 | 27.7 | 44.6 | 31 | 54.7 | 35.0 | 31.3 | 20.9 |
| (5.4) | (7.2) | (13.5) | (11.5) | (9.8) | (8.2) | (9.1) | (8.8) | (9.8) | (8.7) | (12.5) | |
| 16 | 30.2 | 25.8 | 7.4 | 43.4 | 28.6 | 60.1 | 37.4 | 47.3 | 34.1 | 24.4 | 15.3 |
| (5.2) | (7.1) | (14.3) | (10.2) | (9.7) | (8.4) | (8.7) | (8.3) | (9.1) | (8.5) | (10.1) | |
| Finger Joints | Levene’s Test | t-Test for Equality of Means | |||
|---|---|---|---|---|---|
| F | Sig. | t | df | p-Value | |
| Thumb CMC | 0.78 | 0.383 | −1.95 | 48 | 0.58 |
| Thumb MCP | 1.14 | 0.291 | −1.27 | 48 | 0.21 |
| Thumb IP | 0.74 | 0.394 | 0.38 | 48 | 0.71 |
| Index MCP | 0.13 | 0.719 | −1.26 | 48 | 0.21 |
| Index PIP | 0.96 | 0.333 | −2.46 | 48 | 0.017 ** |
| Finger Joints | Levene’s Test | t-Test for Equality of Means | |||
|---|---|---|---|---|---|
| F | Sig. | t | df | p-Value | |
| Thumb CMC | 0.175 | 0.678 | 1.135 | 48 | 0.26 |
| Thumb MCP | 1.315 | 0.257 | 1.319 | 48 | 0.19 |
| Thumb IP | 0.08 | 0.929 | 0.353 | 48 | 0.73 |
| Middle MCP | 0.872 | 0.355 | 1.658 | 48 | 0.10 |
| Middle PIP | 2.062 | 0.157 | 2.647 | 48 | 0.011 ** |
| Finger Joints | Levene’s Test | t-Test for Equality of Means | |||
|---|---|---|---|---|---|
| F | Sig. | t | df | p-Value | |
| Thumb CMC | 0.27 | 0.60 | 1.29 | 48 | 0.20 |
| Thumb MCP | 0.08 | 0.78 | 1.95 | 48 | 0.06 |
| Thumb IP | 0.26 | 0.61 | 0.24 | 48 | 0.81 |
| Ring MCP | 1.61 | 0.21 | 1.87 | 48 | 0.07 |
| Ring PIP | 0.73 | 0.40 | 2.87 | 48 | 0.006 ** |
| Test | Thumb Force (N) | Index Force (N) | Middle Force (N) | Ring Force (N) | Little Force (N) | Total Force (N) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 1 | 4.5 | 2.1 | 2.9 | 1.5 | 3.5 | 1.7 | 2.1 | 1.1 | 1.1 | 1.3 | 14.1 |
| 2 | 2.3 | 0.7 | 2.2 | 1.1 | 1.8 | 0.7 | - | - | - | - | 6.3 |
| 3 | 2.4 | 1.1 | 1.7 | 0.6 | 1.5 | 0.6 | 0.5 | 0.7 | - | - | 6.1 |
| 4 | 2.6 | 0.9 | 1.9 | 1.0 | 1.8 | 0.7 | 1.1 | 0.8 | - | - | 7.7 |
| 5 | 2.6 | 1.2 | 1.6 | 0.8 | 1.9 | 0.6 | 0.4 | 0.6 | - | - | 6.6 |
| 6 | 2.2 | 0.9 | 2.2 | 1.1 | 2.5 | 0.7 | - | - | - | - | 6.9 |
| 7 | 3.0 | 1.8 | 2.0 | 0.7 | 2.3 | 1.1 | 0.8 | 0.8 | - | - | 8.1 |
| 8 | 2.3 | 1.1 | 2.1 | 1.0 | 1.9 | 0.8 | - | - | - | - | 6.4 |
| 9 | 2.1 | 1.0 | 1.9 | 1.1 | 1.8 | 0.8 | - | - | - | - | 6.1 |
| 10 | 2.1 | 1.0 | 1.9 | 0.9 | 1.7 | 1.0 | - | - | - | - | 5.8 |
| 11 | 1.8 | 0.2 | - | - | - | - | 1.2 | 1.0 | - | - | 3.0 |
| 12 | 2.1 | 0.7 | 2.4 | 0.9 | - | - | - | - | - | - | 4.4 |
| 13 | 1.8 | 0.2 | - | - | 1.8 | 0.5 | - | - | - | - | 3.5 |
| 14 | 2.2 | 0.5 | 1.9 | 0.6 | - | - | - | - | - | - | 4.1 |
| 15 | 2.3 | 1.0 | - | - | - | - | 1.5 | 0.9 | - | - | 3.8 |
| 16 | 2.2 | 0.9 | - | - | 2.3 | 0.8 | - | - | - | - | 4.5 |
| Fingertip | Levene’s Test | t-Test for Equality of Means | |||
|---|---|---|---|---|---|
| F | Sig. | t | df | p-Value | |
| Thumb | 1.715 | 0.193 | 0.807 | 118 | 0.421 |
| Index | 1.314 | 0.254 | 2.385 | 118 | 0.019 ** |
| Middle | 0.038 | 0.846 | 2.477 | 118 | 0.015 ** |
| Ring | 1.421 | 0.236 | 0.662 | 117 | 0.510 |
| Little | 0.013 | 0.908 | 0.051 | 118 | 0.959 |
| Fingertip | Levene’s Test | t-Test for Equality of Means | |||
|---|---|---|---|---|---|
| F | Sig. | t | df | p-Value | |
| Thumb | 3.152 | 0.080 | 1.628 | 78 | 0.108 |
| Index | 0.247 | 0.621 | 0.534 | 78 | 0.595 |
| Middle | 2.913 | 0.092 | 2.429 | 78 | 0.017 ** |
| Ring | 0.339 | 0.562 | 0.618 | 78 | 0.538 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilla-Magaña, J.F.; Peña-Pitarch, E.; Sánchez-Suarez, I.; Ticó-Falguera, N. Hand Motion Analysis during the Execution of the Action Research Arm Test Using Multiple Sensors. Sensors 2022, 22, 3276. https://doi.org/10.3390/s22093276
Padilla-Magaña JF, Peña-Pitarch E, Sánchez-Suarez I, Ticó-Falguera N. Hand Motion Analysis during the Execution of the Action Research Arm Test Using Multiple Sensors. Sensors. 2022; 22(9):3276. https://doi.org/10.3390/s22093276
Chicago/Turabian StylePadilla-Magaña, Jesus Fernando, Esteban Peña-Pitarch, Isahi Sánchez-Suarez, and Neus Ticó-Falguera. 2022. "Hand Motion Analysis during the Execution of the Action Research Arm Test Using Multiple Sensors" Sensors 22, no. 9: 3276. https://doi.org/10.3390/s22093276
APA StylePadilla-Magaña, J. F., Peña-Pitarch, E., Sánchez-Suarez, I., & Ticó-Falguera, N. (2022). Hand Motion Analysis during the Execution of the Action Research Arm Test Using Multiple Sensors. Sensors, 22(9), 3276. https://doi.org/10.3390/s22093276