
Skin Cancer Detection Using Infrared Thermography: Measurement Setup, Procedure and Equipment

 , , and
, , and 
Abstract
:1. Introduction
1.1. Today’s Screening Methodology
1.2. Biomedical Infrared Thermography
1.3. Skin Cancer and Infrared Thermography
2. Concepts of Thermography
2.1. Qualitative versus Quantitative Thermography
2.2. Passive versus Active Thermography in Biomedical Applications
2.2.1. Passive Thermography
2.2.2. Active Thermography
Thermal Excitation: Cooling vs. Heating
2.2.3. Lock-In Thermography
2.3. Infrared Cameras
- Spectral response of 5–15 m with a peak around 8–10 m.
- NETD of <80 mK
- Minimal accuracy of +/−2%.
- Spatial resolution of 1 mm at a measuring distance of 40 cm from the detector.
- Fast real-time capturing of infrared data
- Absolute resolution: >19,200 temperature points
- Instantanious Field of View: <2.5 mRad
- Emissivity set to 0.98 (human skin)
2.3.1. Spectral Range
2.3.2. Noise-Equivalent Temperature Difference (NETD)
2.3.3. Emissivity
3. State-of-the-Art Research: Overview
4. IR Thermography in Skin Cancer Research
4.1. Measurement Procedure
4.1.1. Patient Preparation, Acclimatization and Controlled Environment
4.1.2. Imaging Procedure
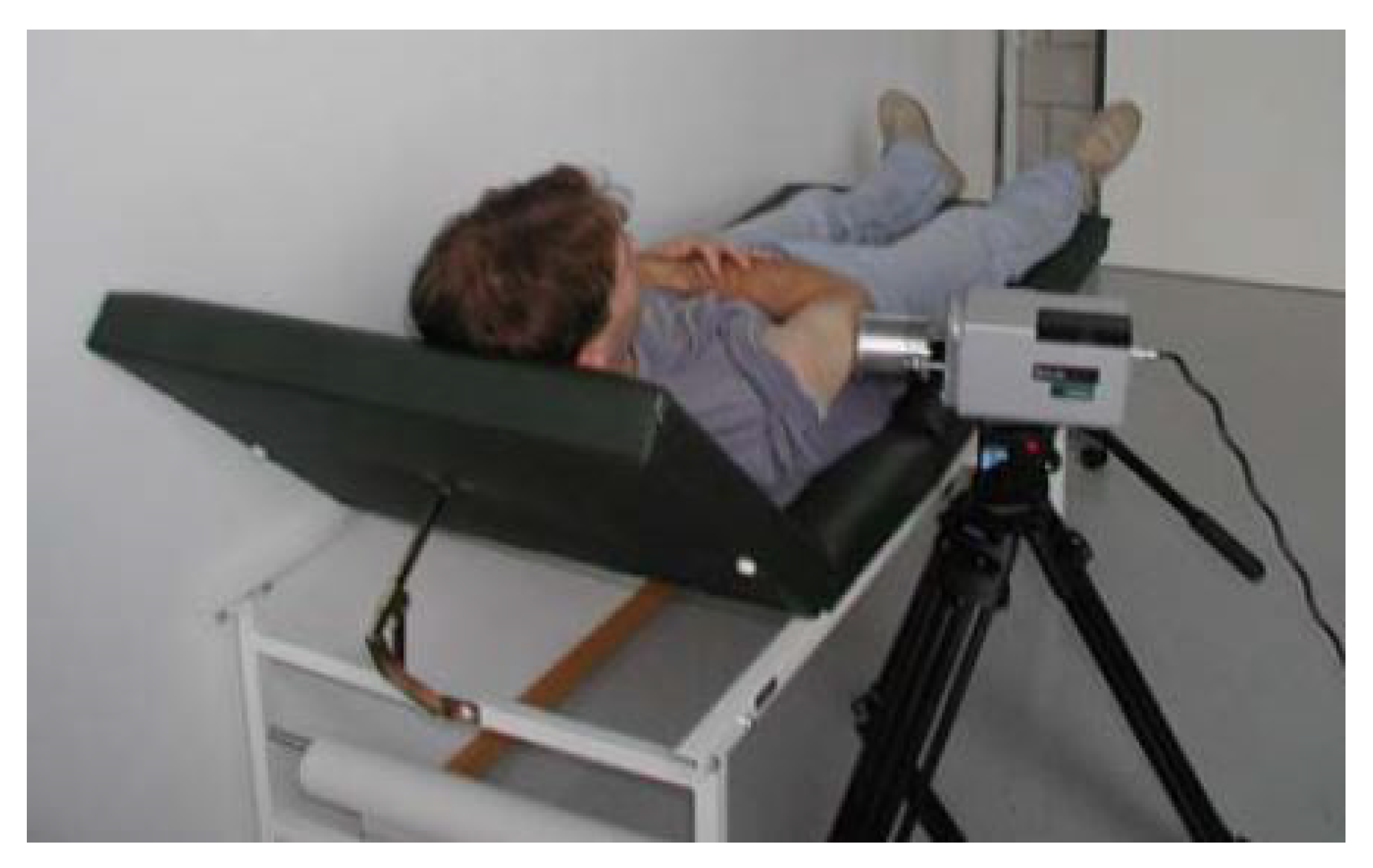
4.2. Measurement Setup
4.2.1. Skin Excitation
- T = Temperature [°C]
- = Tissue density [kg/m]
- C = Tissue specific heat [J/(kg °C)]
- k = Tissue thermal conductivity [W(m °C)]
- = Blood perfusion rate [kg/(ms)]
- = Blood specific heat [J/(kg °C)]
- = Arterial temperature [°C]
- = Metabolic heat generation rate [W/m]
- = Regional heat sources [W/m]
4.2.2. Camera Positioning System
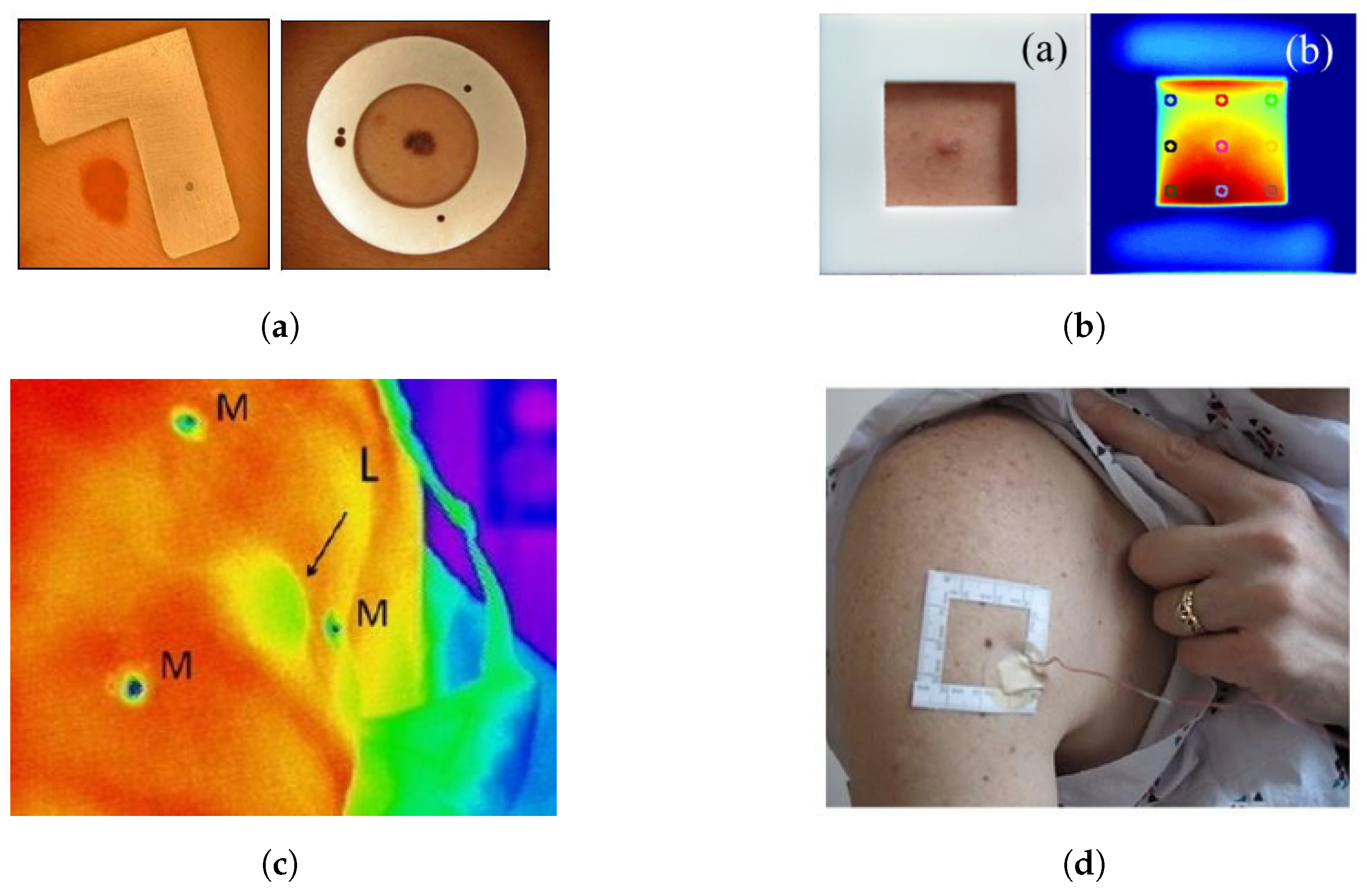
4.2.3. ROI Markers
4.3. Camera and Calibration
4.3.1. Cameras Used in Literature
4.3.2. Calibration
4.3.3. Influence of Viewing Angle on Emissivity
5. Recommendations and Future Research
6. Conclusions
6.1. Measurement Procedure
6.2. Measurement Setup
6.3. Thermal Excitation
- Biological tissue should not be heated to more than 42 °C while cooling of skin tissue is limited to 4 °C.
- Uniform thermal excitation is important to achieve a high degree of accuracy and high thermal contrast. Uneven cooling will result in differential thermal recovery of the skin lesion and surrounding healthy skin.
- Noncontact skin excitation such as convective cooling or heating is preferred in daily medical diagnostic practice. The skin excitation can be monitored for the physical limits of the patient with the thermal camera. Aseptic conditions can be easily ensured.
6.4. Camera
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TBSE | Total Body Skin Examination |
| IRT | Infrared Thermography |
| DIEP | Deep Inferior Epigastric Perforator |
| IR | Infrared |
| NIR | Near-Infrared |
| MIR | Mid-Infrared |
| FIR | Far-Infrared |
| SWIR | Short-Wave Infrared |
| MWIR | Mid-Wave Infrared |
| LWIR | Long-Wave Infrared |
| VLWIR | Very-Long Wave Infrared |
| TIR | Thermal Infrared |
| SNR | Signal-Noise Ratio |
| FMTWI | Frequency Modulated Thermal Wave Imaging |
| IACT | International Academy of Clinical Thermology |
| NETD | Noise-Equivalent Temperature Difference |
| DIRT | Dynamic Infrared Thermography |
| BNCT | Boron Neutron Capture Therapy |
| ROI | Region Of Interest |
| NUC | Nonuniformity Correction |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title | Authors | Year | Measurement Method | Analysis Scheme | Lesion types | Other Diagnosis Methods |
|---|---|---|---|---|---|---|
| Skin-tumour classification with functional infrared imaging [27] | Buzug et al. | 2006 | Quantitative | Active thermography | 1 Basal-cell carcinoma 1 dysplastic nevus | histopathology |
| Dynamic infrared imaging of cutaneous melanoma and normal skin in patients treated with BNCT [78] | Santa Cruz et al. | 2009 | Quantitative | Active thermography | 2 Malignant Melanoma | CT high resolution Doppler ultrasound |
| The Assessment of Melanoma Risk Using the Dynamic Infrared Imaging Technique [116] | Cetingül et al. | 2011 | Quantitative | Active thermography | 37 dysplastic nevi of which 2 malignant melanoma | Bright light image dermatoscopic image Confocal microscopy |
| Analysis and diagnosis of basal cell carcinoma (BCC) via infrared imaging [40] | Flores-Sahagun et al. | 2011 | Quantitative | Passive thermography | 7 basal cell carcinoma | Bright light image |
| Infrared thermography of cutaneous melanoma metastases [98] | Shada et al. | 2013 | Quantitative | Passive thermography | 123 nonmelanomas 128 malignant melanomas | N/A |
| A lock-in thermal imaging setup for dermatological applications [62] | Bonmarin et al. | 2015 | Quantitative | Lock-in thermography | 2 benign lesions | RGB image |
| Dynamic infrared imaging for skin cancer screening [76] | Godoy et al. | 2015 | Quantitative | Active thermography | 59 benign lesions 29 basal-cell carcinoma 8 squamous cell carcinoma 6 malignant melanoma | RGB image |
| Discrimination of benign-versus-malignant skin lesions by thermographic images using support vector machine classifier [100] | Stringasci et al. | 2018 | Quantitative | Passive thermography | 100 Basal-cell carcinoma 100 Normochromic intradermal nevus 35 Squamous cell carcinoma 35 Actinic keratosis 20 Pigmented Seborrheic Keratosis 20 malignant melanoma | RGB image |
| Skin neoplasms dynamic thermal assessment [96] | Magalhaes et al. | 2019 | Quantitative | Active thermography | 51 Squamous cell carcinoma 118 basal cell carcinoma 16 malignant melanomas 29 actinic keratosis 30 nevi 14 seborrheic keratosis | N/A |
| Author | Passive/Active Thermography | Acclimatization Time | Controlled Environment | Steady State Imaging | Cooling Type | Cooling Device | Cooling Temperature | Cooling Area | Cooling Time | Rewarming Time [s] | Number of Rewarming Frames | Camera Distance to Lesion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Buzug et al. [27,77] | Active | / | / | / | Direct contact (conduction) | Cooled gel packs | 20 °C | 10 cm × 10 cm | / | 300 | 300 | Directly in front |
| Santa Cruz et al. [78] | Active | 15–20 min | / | 30 s | 1. Convection 2. Forced evaporation | 1. immersion in water 2. alcohol spray and fan | 1. 15 °C 2. / | / | 1. 120 s 2. / | 180 | / | 1.5 m and 3 m |
| Cetingül et al. [12,83,86] | Active | / | 22 °C | 1 image | Convection | vortex tube | / | / | 60 s | 180–240 | 90–120 | 30 cm |
| Flores-Sahagun et al. [40] | Passive | / | / | / | N/A | N/A | N/A | N/A | N/A | N/A | N/A | 1 m |
| Shada et al. [98] | Passive | / | / | ± 14 min | N/A | N/A | N/A | N/A | N/A | N/A | N/A | / |
| Godoy et al. [9,76] | Active | / | 20–22 °C | 15 s | 1. Convection 2. Convection | 1. vortex tube 2. Airconditioning unit | / | 15–110 s | 120 s | 7200 | / | |
| Stringasci et al. [99,100] | Passive | 10 min | 22 °C | 1 image | N/A | N/A | N/A | N/A | N/A | N/A | N/A | 15 cm |
| Magalhaes et al. [94,97] | Active | 10 min | 21 ± °C relative humidity ≤50% | 1 image | Direct contact (conduction) | Aluminum medal 50 mm H 20 mm | / | 50 mm | 60 s | 300 | 5 | / |
| Author | Buzug et al. [27,77] | Santa Cruz et al. [78] | Cetingül et al. [12,83,86] | Flores-Sahagun et al. [40] | Shada et al. [98] | Godoy et al. [9,76] | Inostroza et al. [92] | Stringasci et al. [99,100] | Diaz et al. [93] | Magalhaes et al. [94,97] |
|---|---|---|---|---|---|---|---|---|---|---|
| Camera brand/type | FLIR SC3000 | Raytheon Palm IR 250 | Merlin Midwave | SAT-S160 | Raytheon Amber Radiance 1-T | / | FLIR Tau 2 | Fluke FLK-Ti400 | ThermApp | FLIR E60sc |
| Detector technology | QWIP FPA | Uncooled Ferroelectric detector FPA | InSb FPA | Uncooled Microbolometer FPA | InSb FPA | QWIP FPA | Uncooled Microbolometer FPA | Uncooled Microbolometer FPA | Uncooled Microbolometer FPA | Uncooled Microbolometer FPA |
| Resolution [pixels] | 320 × 240 | 320 × 240 | 320 × 256 | 160 × 120 | 256 × 256 | 320 × 256 | 640 × 512 | 320 × 240 | 384 × 288 | 320 × 240 |
| Spectral Band [m] | 8–9 | 7–14 | 3–5 | 8–14 | 3–5 | 8–14 | 7.5–13.5 | 7.5–14 | 7.5–14 | 7.5–13 |
| Spectral Region | LWIR | LWIR | MWIR | LWIR | MWIR | LWIR | LWIR | LWIR | LWIR | LWIR |
| Accuracy | ±1% | / | ±2 % | ±2% | / | / | / | ±2% | ±2% | ±2% |
| NETD | 20 mK at 30 °C | / | 25 mK at 30 °C | 100 mK at 30 °C | / | 20 mK at 30 °C | 60 mK at 30 °C | 50 mK at 30 °C | 70 mK at 30 °C | <50 mK at 30 °C |
| Framerate [Hz] | 50/60 | 30 | 60 | 50/60 | / | 60 | 30 | 60 | 25 | / |
| Camera Objective | Macro lens | 75 mm Germanium lens | / | / | / | 50 mm, f/2 | / | / | / | / |
| Fixed/Handheld | Fixed | Handheld | Fixed | Handheld | Fixed | Fixed | Fixed | Handheld | Handheld | Handheld |
| Calibration Method | / | Double-cavity Black body | Black body calibration image degradation correction | / | / | two-point NUC | / | / | / | Black body calibration no method described |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. World Cancer Report; Cancer Research for Cancer Prevention: Lyon, France, 2020. [Google Scholar]
- Verstockt, J.; Verspeek, S.; Thiessen, F.; Tondu, T.; Tjalma, W.A.; Brochez, L.; Steenackers, G. Dynamic Infrared Thermography (DIRT) in Biomedical Applications: DIEP Flap Breast Reconstruction and Skin Cancer. Eng. Proc. 2021, 8, 3. [Google Scholar] [CrossRef]
- Johnson, M.M.; Leachman, S.A.; Aspinwall, L.G.; Cranmer, L.D.; Curiel-Lewandrowski, C.; Sondak, V.K.; Stemwedel, C.E.; Swetter, S.M.; Vetto, J.; Bowles, T.; et al. Skin cancer screening: Recommendations for data-driven screening guidelines and a review of the US Preventive Services Task Force controversy. Melanoma Manag. 2017, 4, 13–37. [Google Scholar] [CrossRef] [PubMed]
- Kandlikar, S.G.; Perez-Raya, I.; Raghupathi, P.A.; Gonzalez-Hernandez, J.L.; Dabydeen, D.; Medeiros, L.; Phatak, P. Infrared imaging technology for breast cancer detection – Current status, protocols and new directions. Int. J. Heat Mass Transf. 2017, 108, 2303–2320. [Google Scholar] [CrossRef]
- Brunssen, A.; Waldmann, A.; Eisemann, N.; Katalinic, A. Impact of skin cancer screening and secondary prevention campaigns on skin cancer incidence and mortality: A systematic review. J. Am. Acad. Dermatol. 2017, 76, 129–139.e10. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Nachbar, F.; Stolz, W.; Merkle, T.; Cognetta, A.B.; Vogt, T.; Landthaler, M.; Bilek, P.; Braun-Falco, O.; Plewig, G. The ABCD rule of dermatoscopy: High prospective value in the diagnosis of doubtful melanocytic skin lesions. J. Am. Acad. Dermatol. 1994, 30, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Godoy, S.E.; Hayat, M.M.; Ramirez, D.A.; Myers, S.A.; Padilla, R.S.; Krishna, S. Detection theory for accurate and noninvasive skin cancer diagnosis using dynamic thermal imaging. Biomed. Opt. Express 2017, 8, 2301. [Google Scholar] [CrossRef] [Green Version]
- Vestergaard, M.; Macaskill, P.; Holt, P.; Menzies, S. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. Br. J. Dermatol. 2008, 159, 669–676. [Google Scholar] [CrossRef]
- Braun, R.P.; Oliviero, M.; Kolm, I.; French, L.E.; Marghoob, A.A.; Rabinovitz, H. Dermoscopy: What is new? Clin. Dermatol. 2009, 27, 26–34. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Herman, C. Quantification of the thermal signature of a melanoma lesion. Int. J. Therm. Sci. 2011, 50, 421–431. [Google Scholar] [CrossRef]
- Bonmarin, M.; Le Gal, F.A. Chapter 31-Thermal Imaging in Dermatology. In Imaging in Dermatology; Hamblin, M.R., Avci, P., Gupta, G.K., Eds.; Academic Press: Boston, MA, USA, 2016; pp. 437–454. [Google Scholar] [CrossRef]
- Williams, K.L. Infrared Thermometry as a Tool in Medical Research. Ann. N. Y. Acad. Sci. 1964, 121, 99–112. [Google Scholar] [CrossRef]
- Jones, B. A reappraisal of the use of infrared thermal image analysis in medicine. IEEE Trans. Med. Imaging 1998, 17, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Ring, E.F.J.; Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 2012, 33, R33–R46. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, G.J. Infrared thermography: A non-invasive window into thermal physiology. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2016, 202, 78–98. [Google Scholar] [CrossRef] [PubMed]
- Vardasca, R.; Simoes, R. Current Issues in Medical Thermography. In Topics in Medical Image Processing and Computational Vision; Tavares, J.M.R., Natal Jorge, R.M., Eds.; Lecture Notes in Computational Vision and Biomechanics; Springer: Dordrecht, The Netherlands, 2013; pp. 223–237. [Google Scholar] [CrossRef]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef]
- Thiessen, F.E.F.; Vermeersch, N.; Tondu, T.; Van Thielen, J.; Vrints, I.; Berzenji, L.; Verhoeven, V.; Hubens, G.; Verstockt, J.; Steenackers, G.; et al. Dynamic Infrared Thermography (DIRT) in DIEP flap breast reconstruction: A clinical study with a standardized measurement setup. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 166–173. [Google Scholar] [CrossRef]
- Bale, M. High-resolution infrared technology for soft-tissue injury detection. IEEE Eng. Med. Biol. Mag. 1998, 17, 56–59. [Google Scholar] [CrossRef]
- Qi, H.; Diakides, N. Infrared Imaging in Medicine; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Vollmer, M.; Möllmann, K.P. Infrared Thermal Imaging: Fundamentals, Research and Applications, 2nd ed.; Wiley-VCH: Berlin, Germany, 2017; Volume 2. [Google Scholar]
- Vollmer, M.; Möllmann, K.P. Medical Applications. In Infrared Thermal Imaging - Fundamentals, Research and Applications, 2nd ed.; Wiley-VCH: Berlin, Germany, 2018; pp. 709–721. [Google Scholar]
- Lee, Y.Y.; Md Din, M.F.; Noor, Z.Z.; Iwao, K.; Mat Taib, S.; Singh, L.; Abd Khalid, N.H.; Anting, N.; Aminudin, E. Surrogate human sensor for human skin surface temperature measurement in evaluating the impacts of thermal behaviour at outdoor environment. Measurement 2018, 118, 61–72. [Google Scholar] [CrossRef]
- Minkina, W.; Dudzik, S. Infrared Thermography—Errors and Uncertainties, 1st ed.; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Buzug, T.; Schumann, S.; Pfaffmann, L.; Reinhold, U.; Ruhlmann, J. Skin-Tumour Classification with Functional Infrared Imaging. In Proceedings of the 8th IASTED International Conference on Signal and Image Processing, SIP 2006, Honolulu, HI, USA, 14–16 August 2006. [Google Scholar]
- Togawa, T. Non-contact skin emissivity: Measurement from reflectance using step change in ambient radiation temperature. Clin. Phys. Physiol. Meas. 1989, 10, 39–48. [Google Scholar] [CrossRef]
- BuchmÜller, K. Über die ultrarote Emission, Reflexion und Durchlässigkeit der lebenden menschlichen Haut im Spektralbereich lambda = 3–15 um. Pflüger’s Arch. Für Die Gesamte Physiol. Des Menschen Und Der Tiere 1961, 272, 360–371. [Google Scholar] [CrossRef]
- Gärtner, W.; Göpfert, H. Topographische Untersuchungen über die Strahlungseigenschaften der lebenden menschlichen Haut. Pflüger’s Arch. Für Die Gesamte Physiol. Des Menschen Und Der Tiere 1964, 280, 224–235. [Google Scholar] [CrossRef]
- Hardy, J.D.; Muschenheim, C. The radiation of heat from the human body. IV. The emission, reflection, and transmission of infra-red radiation by the human skin. J. Clin. Investig. 1934, 13, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Jacquez, J.A.; Huss, J.; McKeehan, W.; Dimitroff, J.M.; Kuppenheim, H.F. Spectral Reflectance of Human Skin in the Region 0.7–2.6 µ. J. Appl. Physiol. 1955, 8, 297–299. [Google Scholar] [CrossRef]
- Mitchell, D.; Wyndham, C.H.; Hodgson, T.; Nabarro, F.R.N. Measurement of the Total Normal Emissivity of Skin Without The Need For Measuring Skin Temperature. Phys. Med. Biol. 1967, 12, 359–366. [Google Scholar] [CrossRef]
- Sanchez-Marin, F.J.; Calixto-Carrera, S.; Villaseñor-Mora, C. Novel approach to assess the emissivity of the human skin. J. Biomed. Opt. 2009, 14, 024006. [Google Scholar] [CrossRef]
- Charlton, M.; Stanley, S.A.; Whitman, Z.; Wenn, V.; Coats, T.J.; Sims, M.; Thompson, J.P. The effect of constitutive pigmentation on the measured emissivity of human skin. PLoS ONE 2020, 15, e0241843. [Google Scholar] [CrossRef]
- Bernard, V.; Staffa, E.; Mornstein, V.; Bourek, A. Infrared camera assessment of skin surface temperature—Effect of emissivity. Phys. Medica 2013, 29, 583–591. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.L. Image and Signal Processors. In Principles of Infrared Technology: A Practical Guide to the State of the Art; Miller, J.L., Ed.; Springer: Boston, MA, USA, 1994; pp. 243–283. [Google Scholar] [CrossRef]
- Faust, O.; Rajendra Acharya, U.; Ng, E.Y.K.; Hong, T.J.; Yu, W. Application of infrared thermography in computer aided diagnosis. Infrared Phys. Technol. 2014, 66, 160–175. [Google Scholar] [CrossRef]
- Ring, E.F.J. The historical development of temperature measurement in medicine. Infrared Phys. Technol. 2007, 49, 297–301. [Google Scholar] [CrossRef]
- Flores-Sahagun, J.H.; Vargas, J.V.C.; Mulinari-Brenner, F.A. Analysis and diagnosis of basal cell carcinoma (BCC) via infrared imaging. Infrared Phys. Technol. 2011, 54, 367–378. [Google Scholar] [CrossRef]
- Verstockt, J.; Thiessen, F.; Cloostermans, B.; Tjalma, W.; Steenackers, G. DIEP flap breast reconstructions: Thermographic assistance as a possibility for perforator mapping and improvement of DIEP flap quality. Appl. Opt. 2020, 59, E48. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.J.; Ng, E.Y.K.; Yeo, A.C.B.; Wu, S.; Pan, F.; Yau, W.Y.; Chen, J.H.; Yang, Y. A perspective on medical infrared imaging. J. Med Eng. Technol. 2005, 29, 257–267. [Google Scholar] [CrossRef]
- Kirimtat, A.; Krejcar, O.; Selamat, A. A Mini-review of Biomedical Infrared Thermography (B-IRT). In Bioinformatics and Biomedical Engineering; Rojas, I., Valenzuela, O., Rojas, F., Ortuño, F., Eds.; Springer International Publishing: Cham, Switzerland, 2019; Volume 11466, pp. 99–110. [Google Scholar] [CrossRef]
- Smith, R.L.; Soeters, M.R.; Wüst, R.C.I.; Houtkooper, R.H. Metabolic Flexibility as an Adaptation to Energy Resources and Requirements in Health and Disease. Endocr. Rev. 2018, 39, 489–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santulli, G. Angiogenesis: Insights from a Systematic Overview; Nova Publisher: Hauppauge, NY, USA, 2013. [Google Scholar]
- Jones, B.F.; Plassmann, P. Digital infrared thermal imaging of human skin. IEEE Eng. Med. Biol. Mag. Q. Mag. Eng. Med. Biol. Soc. 2002, 21, 41–48. [Google Scholar] [CrossRef]
- Kerbel, R.S. Tumor Angiogenesis. N. Engl. J. Med. 2008, 358, 2039–2049. [Google Scholar] [CrossRef] [Green Version]
- Elder, D. Tumor Progression, Early Diagnosis and Prognosis of Melanoma. Acta Oncol. 1999, 38, 535–548. [Google Scholar] [CrossRef] [Green Version]
- Dössel, O. Thermographie und Infrarot-Bildgebung. In Bildgebende Verfahren in der Medizin: Von der Technik zur Medizinischen Anwendung; Dössel, O., Ed.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 485–495. [Google Scholar] [CrossRef]
- González, F.; Castillo-Martínez, C.; Valdes-Rodríguez, R.; Kolosovas-Machuca, E.; Villela-Segura, U.; Moncada, B. Thermal signature of melanoma and non-melanoma skin cancers. In Proceedings of the 2012 International Conference on Quantitative InfraRed Thermography, Naples, Italy, 11–14 June 2012; Taylor & Francis: Oxfordshire, UK, 2012. [Google Scholar] [CrossRef]
- Moustafa, A.M.N.; Muhammed, H.H.; Hassan, M. Skin Cancer Detection Using Temperature Variation Analysis. Engineering 2013, 5, 18–21. [Google Scholar] [CrossRef] [Green Version]
- Zalewska, A.; Wiecek, B.; Sysa-Jedrzejowska, A.; Gralewicz, G.; Owczarek, G. Qualitative thermograhic analysis of psoriatic skin lesions. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; Volume 1, pp. 1192–1195. [Google Scholar] [CrossRef]
- Qualitative, vs. Quantitative Thermography: Understanding What Is Required and When. Available online: https://www.flir.com/discover/professional-tools/qualitative-vs.-quantitative-thermography-understanding-what-is-required-and-when/ (accessed on 9 March 2022).
- Fernández-Cuevas, I.; Marins, J.C.B.; Lastras, J.A.; Carmona, P.M.G.; Cano, S.P.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Maldague, X.P.V. Theoretical Aspects. In Nondestructive Evaluation of Materials by Infrared Thermography; Maldague, X.P.V., Ed.; Springer: London, UK, 1993; pp. 23–37. [Google Scholar] [CrossRef]
- Szentkuti, A.; Skala Kavanagh, H.; Grazio, S. Infrared thermography and image analysis for biomedical use. Period. Biol. 2011, 113, 385–392. [Google Scholar]
- Vardasca, R.; Vaz, L.; Mendes, J. Classification and Decision Making of Medical Infrared Thermal Images. In Classification in BioApps; Dey, N., Ashour, A.S., Borra, S., Eds.; Springer International Publishing: Cham, Switzerland, 2018; Volume 26, pp. 79–104. [Google Scholar] [CrossRef]
- Kaczmarek, M.; Nowakowski, A. Active Dynamic Thermography in Medical Diagnostics. In Application of Infrared to Biomedical Sciences; Ng, E.Y., Etehadtavakol, M., Eds.; Springer: Singapore, 2017; pp. 291–310. [Google Scholar] [CrossRef]
- Ammer, K.; Ring, F.J. Standard Procedures for Infrared Imaging in Medicine. In Medical Infrared Imaging; Taylor & Francis: Boca Raton, FL, USA, 2013. [Google Scholar]
- Di Carlo, A. Thermography and the possibilities for its applications in clinical and experimental dermatology. Clin. Dermatol. 1995, 13, 329–336. [Google Scholar] [CrossRef]
- Hardy, J.D.; Hammel, H.T.; Murgatroyd, D. Spectral Transmittance and Reflectance of Excised Human Skin. J. Appl. Physiol. 1956, 9, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Bonmarin, M.; Gal, F.A.L. A lock-in thermal imaging setup for dermatological applications. Skin Res. Technol. 2015, 21, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Breitenstein, O.; Warta, W.; Schubert, M.C. Lock-in Thermography: Basics and Use for Evaluating Electronic Devices and Materials; Springer Series in Advanced Microelectronics; Springer International Publishing: Cham, Switzerland, 2018; Volume 10. [Google Scholar] [CrossRef]
- Bonmarin, M.; Le Gal, F.A. Lock-in thermal imaging for the early-stage detection of cutaneous melanoma: A feasibility study. Comput. Biol. Med. 2014, 47, 36–43. [Google Scholar] [CrossRef]
- Bhowmik, A.; Repaka, R.; Mishra, S.C.; Mulaveesala, R. Detection of Subsurface Skin Lesion Using Frequency Modulated Thermal Wave Imaging: A Numerical Study; Volume 3A: Biomedical and Biotechnology Engineering; American Society of Mechanical Engineers: San Diego, CA, USA, 2013; p. V03AT03A064. [Google Scholar] [CrossRef]
- Rogalski, A. Infrared detectors: An overview. Infrared Phys. Technol. 2002, 43, 187–210. [Google Scholar] [CrossRef] [Green Version]
- Rogalski, A. History of infrared detectors. Opto-Electron. Rev. 2012, 20, 279–308. [Google Scholar] [CrossRef]
- Diakides, M.; Bronzino, J.D.; Peterson, D.R. Medical Infrared Imaging; CRC Press: Boca Raton, FL, USA; Taylor & Francis: Oxfordshire, UK, 2013. [Google Scholar]
- Jagadish, C.; Gunapala, S.D.; Rhiger, D. Advances in Infrared Photodetectors, 1st ed.; Academic Press Elsevier: Cambridge, MA, USA, 2011; Volume 84. [Google Scholar]
- Amalu, W. International Academy of Clinical Thermology Medical Infrared Imaging Standards and Guidelines; International Academy of Clinical Thermology: Foster City, CA, USA, 2018. [Google Scholar] [CrossRef]
- Babaiants, R.S.; Karpushkin, V.P.; Orlova, I.V. Diagnosis of skin neoplasms by means of thermography. Vestn. Dermatol. I Venerol. 1974, 48, 8–11. [Google Scholar]
- Brasfield, R.D.; Laughlin, J.S.; Sherman, R.S. Thermography in the Management of Cancer: A Preliminary Report. Ann. N. Y. Acad. Sci. 1964, 121, 235–247. [Google Scholar] [CrossRef]
- Hartmann, M.; Kunze, J.; Friedel, S. Telethermography in the Diagnostics and Management of Malignant Melanomas. J. Dermatol. Surg. Oncol. 1981, 7, 213–218. [Google Scholar] [CrossRef]
- Amalric, R.; Altschuler, C.; Giraud, D.; Thomassin, L.; Spitalier, J.M. Value of Infrared Thermography in the Assessment of Malignant Melanomas of the Skin. In Recent Advances in Medical Thermology; Ring, E.F.J., Phillips, B., Eds.; Springer: Boston, MA, USA; New York, NY, USA, 1984; pp. 623–629. [Google Scholar] [CrossRef]
- Bourjat, P.; Gautherie, M.; Grosshans, E. Diagnosis, follow-up and prognosis of malignant melanomas by thermography. Bibl. Radiol. 1975, 6, 115–127. [Google Scholar]
- Godoy, S.E.; Ramirez, D.A.; Myers, S.A.; von Winckel, G.; Krishna, S.; Berwick, M.; Padilla, R.S.; Sen, P.; Krishna, S. Dynamic infrared imaging for skin cancer screening. Infrared Phys. Technol. 2015, 70, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Buzug, T.M.; Schumann, S.; Pfaffmann, L.; Reinhold, U.; Ruhlmann, J. Functional infrared imaging for skin-cancer screening. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology, New York, NY, USA, 30 August–3 September 2006; pp. 2766–2769. [Google Scholar] [CrossRef]
- Santa Cruz, G.A.; Bertotti, J.; Marín, J.; González, S.J.; Gossio, S.; Alvarez, D.; Roth, B.M.C.; Menéndez, P.; Pereira, M.D.; Albero, M.; et al. Dynamic infrared imaging of cutaneous melanoma and normal skin in patients treated with BNCT. Appl. Radiat. Isot. 2009, 67, S54–S58. [Google Scholar] [CrossRef] [PubMed]
- Çetingül, M.P.; Herman, C. Identification of skin lesions from the transient thermal response using infrared imaging technique. In Proceedings of the 2008 5th IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Paris, France, 14–17 May 2008; pp. 1219–1222. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Herman, C.; Alani, R.M. Skin Imaging with Infrared Thermography and Confocal Microscopy. In Proceedings of the ASME 2009 Heat Transfer Summer Conference collocated with the InterPACK09 and 3rd Energy Sustainability Conferences, San Francisco, CA, USA, 19–23 July 2009; pp. 731–739. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Herman, C. Transient Thermal Response of Skin Tissue. In Proceedings of the ASME 2008 Heat Transfer Summer Conference collocated with the Fluids Engineering, Energy Sustainability, and 3rd Energy Nanotechnology Conferences, Jacksonville, FL, USA, 10–14 August 2008; American Society of Mechanical Engineers Digital Collection: New York, NY, USA, 2009; pp. 355–361. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Alani, R.M.; Herman, C. Quantitative Evaluation of Skin Lesions Using Transient Thermal Imaging. In Proceedings of the 2010 14th International Heat Transfer Conference, Washington, DC, USA, 8–13 August 2010; ASMEDC: Washington, DC, USA, 2010; Volume 1, pp. 31–39. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Herman, C. Using Dynamic Infrared Imaging to Detect Melanoma: Experiments on a Tissue-Mimicking Phantom. In Volume 2: Biomedical and Biotechnology Engineering; ASMEDC: Vancouver, BC, Canada, 2010; pp. 139–147. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Herman, C. A heat transfer model of skin tissue for the detection of lesions: Sensitivity analysis. Phys. Med. Biol. 2010, 55, 5933–5951. [Google Scholar] [CrossRef] [PubMed]
- Çetingül, M.P.; Alani, R.M.; Herman, C. Detection of Skin Cancer Using Transient/Thermal Imaging. In Proceedings of the ASME 2010 Summer Bioengineering Conference, Parts A and B, Naples, FL, USA, 16–19 June 2010; American Society of Mechanical Engineers: Naples, FL, USA, 2010; pp. 601–602. [Google Scholar] [CrossRef]
- Çetingül, M.P.; Çetingül, H.E.; Herman, C. Analysis of transient thermal images to distinguish melanoma from dysplastic nevi. In Proceedings of the Medical Imaging 2011: Computer-Aided Diagnosis, Lake Buena Vista (Orlando), FL, USA, 12–17 February 2011; International Society for Optics and Photonics: Bellingham, WA, USA, 2011; Volume 7963, p. 79633N. [Google Scholar] [CrossRef]
- Cheng, T.Y.; Herman, C. Optimization of Skin Cooling for Thermographic Imaging of Near-Surface Lesions. In Volume 2: Biomedical and Biotechnology Engineering; Nanoengineering for Medicine and Biology; ASMEDC: Denver, CO, USA, 2011; pp. 351–360. [Google Scholar] [CrossRef]
- Cheng, T.Y.; Deng, D.; Herman, C. Curvature effect quantification for in-vivo IR thermography. In Proceedings of the ASME 2012 International Mechanical Engineering Congress and Exposition, Houston, TX, USA, 9–15 November 2012; Volume 2, pp. 127–133. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.Y.; Herman, C. Involuntary motion tracking for medical dynamic infrared thermography using a template-based algorithm. Proc. SPIE 2013, 8669. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.Y.; Herman, C. Motion tracking in infrared imaging for quantitative medical diagnostic applications. Infrared Phys. Technol. 2014, 62, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.Y.; Herman, C. Analysis of skin cooling for quantitative dynamic infrared imaging of near-surface lesions. Int. J. Therm. Sci. 2014, 86, 175–188. [Google Scholar] [CrossRef]
- Inostroza, F.; Díaz, S.; Cárdenas, J.; Godoy, S.E.; Figueroa, M. Embedded registration of visible and infrared images in real time for noninvasive skin cancer screening. Microprocess. Microsyst. 2017, 55, 70–81. [Google Scholar] [CrossRef]
- Diaz, S.; Krohmer, T.; Moreira, A.; Godoy, S.E.; Figueroa, M. An Instrument for Accurate and Non-Invasive Screening of Skin Cancer Based on Multimodal Imaging. IEEE Access 2019, 7, 176646–176657. [Google Scholar] [CrossRef]
- Magalhaes, C.; Vardasca, R.; Mendes, J. Classifying Skin Neoplasms with Infrared Thermal Images. In Proceedings of the 14th Quantitative InfraRed Thermography Conference, Berlin, Germany, 25–29 June 2018; Taylor & Francis: Oxfordshire, UK, 2018. [Google Scholar]
- Magalhaes, C.; Vardasca, R.; Mendes, J. Recent use of medical infrared thermography in skin neoplasms. Skin Res. Technol. 2018, 24, 587–591. [Google Scholar] [CrossRef]
- Magalhaes, C.; Mendes, J.; Filipe, R.V.; Vardasca, R. Skin neoplasms dynamic thermal assessment. In Proceedings of the 2019 IEEE 6th Portuguese Meeting on Bioengineering (ENBENG), Lisbon, Portugal, 22–23 February 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Magalhaes, C.; Vardasca, R.; Rebelo, M.; Valenca-Filipe, R.; Ribeiro, M.; Mendes, J. Distinguishing melanocytic nevi from melanomas using static and dynamic infrared thermal imaging. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1700–1705. [Google Scholar] [CrossRef]
- Shada, A.L.; Dengel, L.T.; Petroni, G.R.; Smolkin, M.E.; Acton, S.; Slingluff, C.L. Infrared thermography of cutaneous melanoma metastases. J. Surg. Res. 2013, 182, e9–e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringasci, M.D.; Moriyama, L.T.; Salvio, A.G.; Bagnato, V.S.; Kurachi, C. Thermographic diagnostics to discriminate skin lesions: A clinical study. In Proceedings of the SPIE Biophotonics South America, Rio de Janeiro, Brazil, 23–25 May 2015; p. 953135. [Google Scholar] [CrossRef]
- Stringasci, M.D.; Salvio, A.G.; Sbrissa Neto, D.; Vollet-Filho, J.D.; Bagnato, V.S.; Kurachi, C. Discrimination of benign-versus-malignant skin lesions by thermographic images using support vector machine classifier. J. Appl. Phys. 2018, 124, 044701. [Google Scholar] [CrossRef]
- Khallaf, A.; Williams, R.; Ring, E.; Elvins, D. Thermographic study of heat loss from the face. Thermol. Osterreich 1994, 4, 49–54. [Google Scholar]
- Ring, F. Infrared Imaging; IOP Publishing: Bristol, UK, 2015. [Google Scholar] [CrossRef]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An Overview of Recent Application of Medical Infrared Thermography in Sports Medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef] [Green Version]
- Federspil, G.; La Grassa, E.; Giordano, F.; Macor, C.; Presacco, D.; Di Maggio, C. Study of diet-induced thermogenesis using telethermography in normal and obese subjects. Recent. Progress. Med. 1989, 80, 455–459. [Google Scholar]
- Iljaž, J.; Wrobel, L.C.; Hriberšek, M.; Marn, J. Numerical modelling of skin tumour tissue with temperature-dependent properties for dynamic thermography. Comput. Biol. Med. 2019, 112, 103367. [Google Scholar] [CrossRef]
- Kandala, S.K.; Deng, D.; Herman, C. Simulation of Discrete Blood Vessel Effects on the Thermal Signature of a Melanoma Lesion. In Proceedings of the International Mechanical Engineering Congress and Exposition. International Mechanical Engineering Congress and Exposition, San Diego, CA, USA, 15–21 November 2013; Volume 3B, pp. V03BT03A038–V03BT03A044. [Google Scholar] [CrossRef] [Green Version]
- Strąkowska, M.; Strąkowski, R.; Strzelecki, M.; De Mey, G.; Więcek, B. Thermal modelling and screening method for skin pathologies using active thermography. Biocybern. Biomed. Eng. 2018, 38, 602–610. [Google Scholar] [CrossRef]
- Silva, M.; Freitas, B.; Andrade, R.; Espregueira-Mendes, J.; Silva, F.; Carvalho, O.; Flores, P. Computational Modelling of the Bioheat Transfer Process in Human Skin Subjected to Direct Heating and/or Cooling Sources: A Systematic Review. Ann. Biomed. Eng. 2020, 48, 1616–1639. [Google Scholar] [CrossRef]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef]
- Shen, W.; Zhang, J.; Yang, F. Modeling and numerical simulation of bioheat transfer and biomechanics in soft tissue. Math. Comput. Model. 2005, 41, 1251–1265. [Google Scholar] [CrossRef]
- Gomboc, T.; Iljaž, J.; Wrobel, L.C.; Hriberšek, M.; Marn, J. Design of constant temperature cooling device for melanoma screening by dynamic thermography. Eng. Anal. Bound. Elem. 2021, 125, 66–79. [Google Scholar] [CrossRef]
- Otsuka, K.; Okada, S.; Hassan, M.; Togawa, T. Imaging of skin thermal properties with estimation of ambient radiation temperature. IEEE Eng. Med. Biol. Mag. 2002, 21, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Watmough, D.J.; Fowler, P.W.; Oliver, R. The thermal scanning of a curved isothermal surface: Implications for clinical thermography. Phys. Med. Biol. 1970, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Magalhaes, C.; Mendes, J.; Vardasca, R. Meta-Analysis and Systematic Review of the Application of Machine Learning Classifiers in Biomedical Applications of Infrared Thermography. Appl. Sci. 2021, 11, 842. [Google Scholar] [CrossRef]
- Magalhaes, C.; Tavares, J.M.R.S.; Mendes, J.; Vardasca, R. Comparison of machine learning strategies for infrared thermography of skin cancer. Biomed. Signal Process. Control 2021, 69, 102872. [Google Scholar] [CrossRef]
- Cetingul, M.P.; Herman, C. The Assessment of Melanoma Risk Using the Dynamic Infrared Imaging Technique. J. Therm. Sci. Eng. Appl. 2011, 3, 031006. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verstockt, J.; Verspeek, S.; Thiessen, F.; Tjalma, W.A.; Brochez, L.; Steenackers, G. Skin Cancer Detection Using Infrared Thermography: Measurement Setup, Procedure and Equipment. Sensors 2022, 22, 3327. https://doi.org/10.3390/s22093327
Verstockt J, Verspeek S, Thiessen F, Tjalma WA, Brochez L, Steenackers G. Skin Cancer Detection Using Infrared Thermography: Measurement Setup, Procedure and Equipment. Sensors. 2022; 22(9):3327. https://doi.org/10.3390/s22093327
Chicago/Turabian StyleVerstockt, Jan, Simon Verspeek, Filip Thiessen, Wiebren A. Tjalma, Lieve Brochez, and Gunther Steenackers. 2022. "Skin Cancer Detection Using Infrared Thermography: Measurement Setup, Procedure and Equipment" Sensors 22, no. 9: 3327. https://doi.org/10.3390/s22093327
APA StyleVerstockt, J., Verspeek, S., Thiessen, F., Tjalma, W. A., Brochez, L., & Steenackers, G. (2022). Skin Cancer Detection Using Infrared Thermography: Measurement Setup, Procedure and Equipment. Sensors, 22(9), 3327. https://doi.org/10.3390/s22093327