

Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements

Abstract
:1. Introduction
1.1. Background
1.2. Current Dysphagia Evaluation Approaches
1.3. Alternative Approaches to Assessment
2. Materials and Methods
2.1. Participants and Ethical Considerations
2.2. VFSS
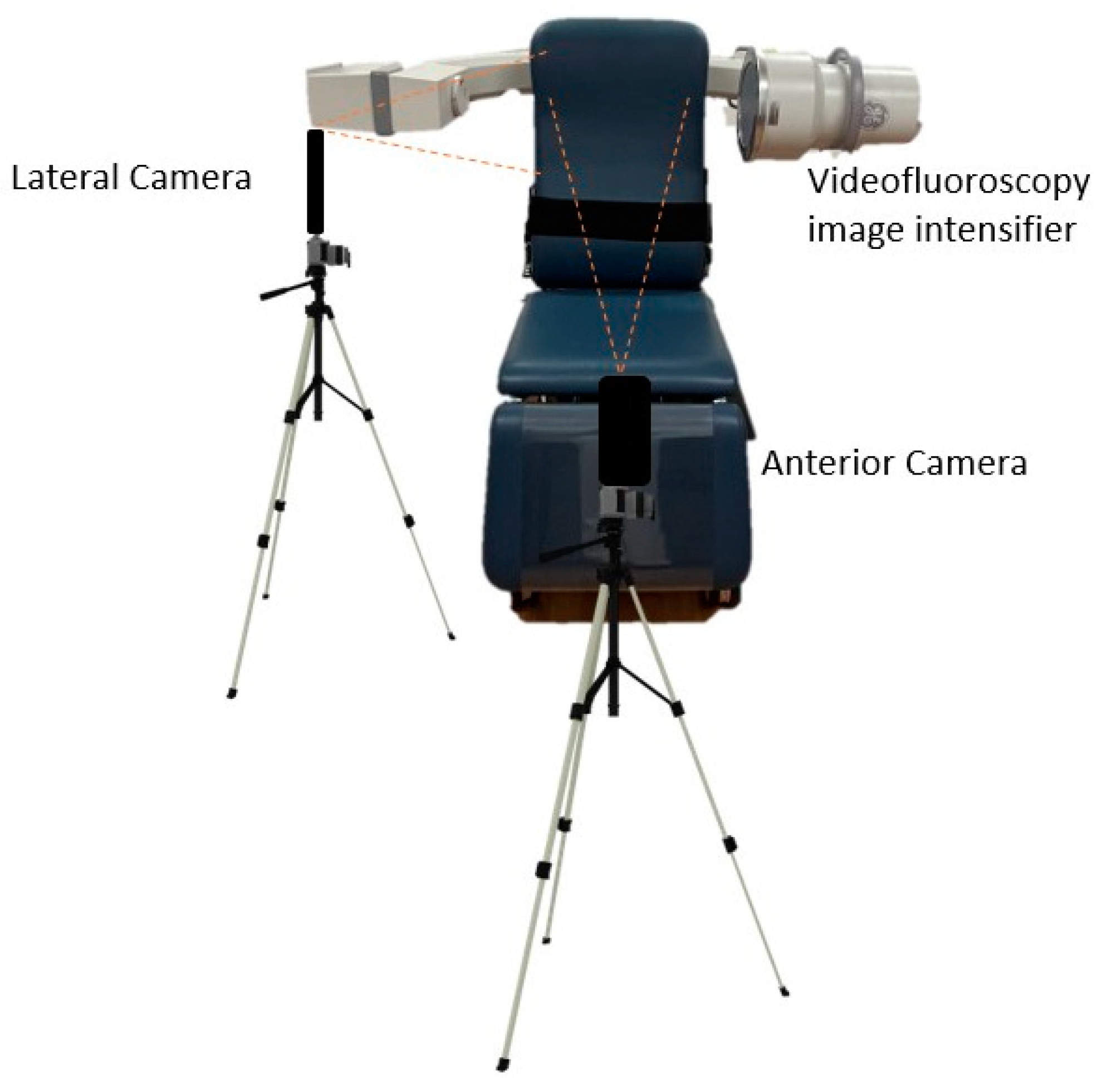
2.3. Video Recording
2.4. Data Extraction
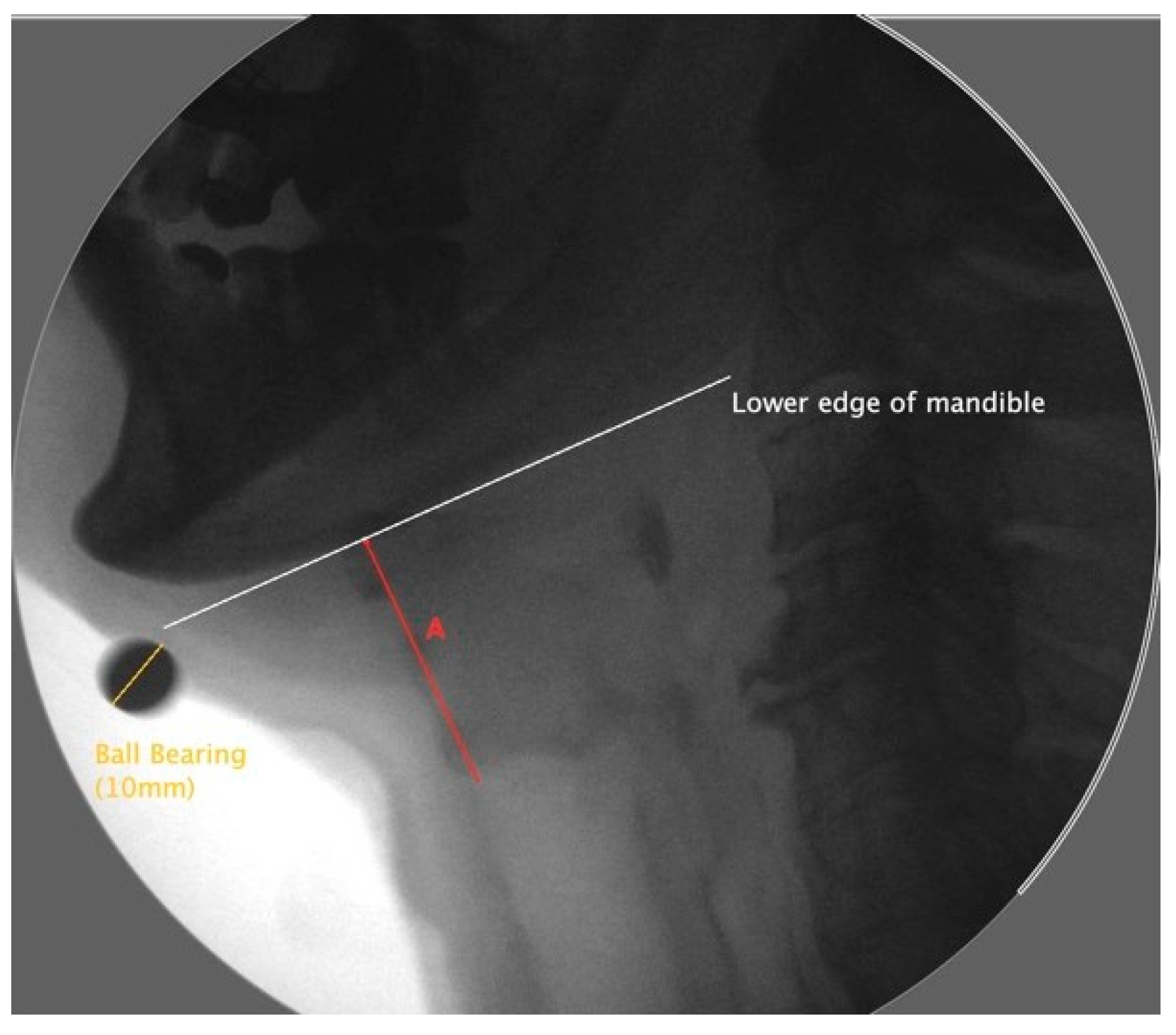
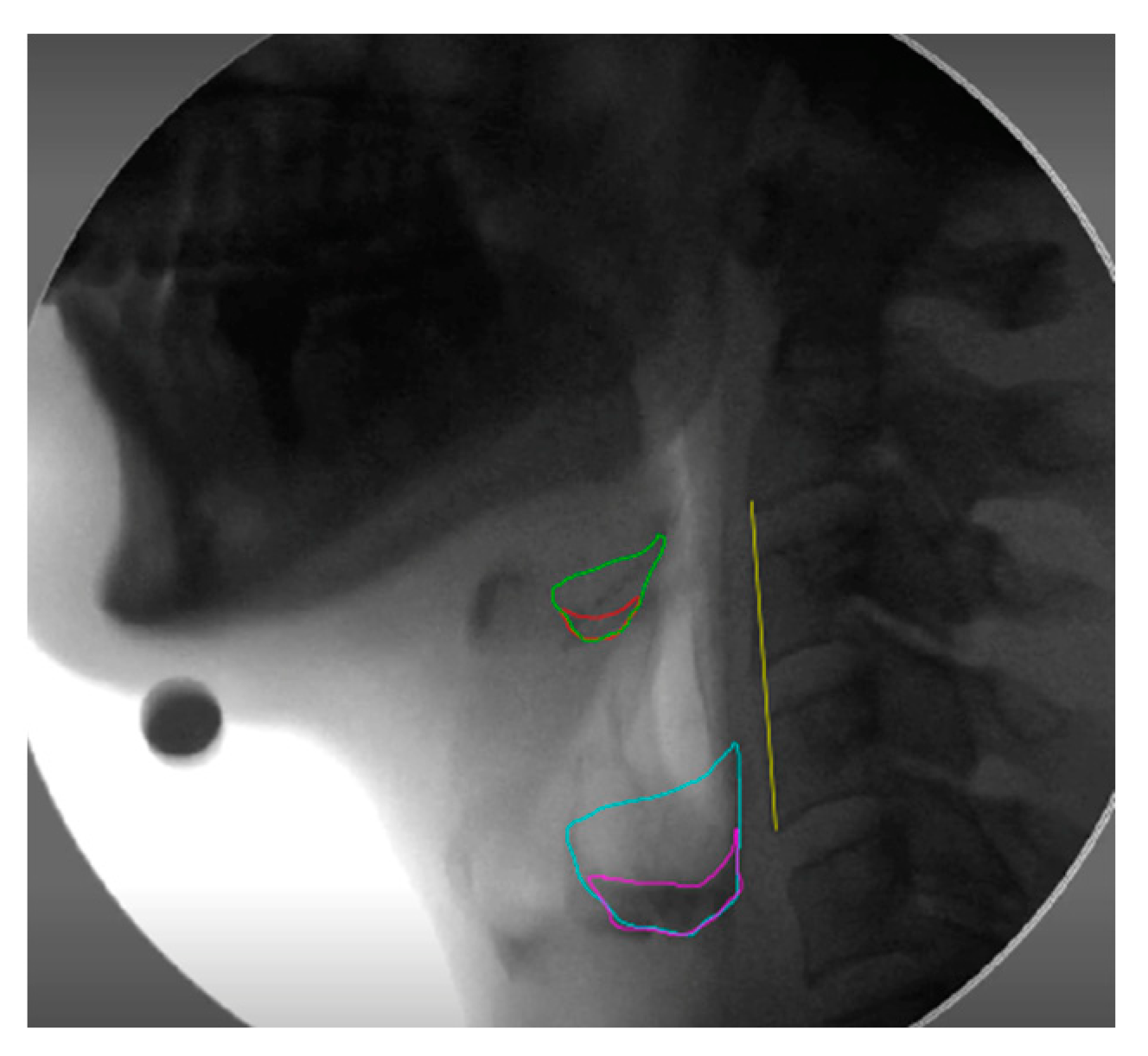
2.4.1. Hyoid Bone Displacement
2.4.2. Hyoid Bone Displacement Velocity
2.4.3. Laryngeal Excursion
2.4.4. Velocity of Laryngeal Elevation
2.4.5. Analysis of Aspiration
2.4.6. Residue Severity Ratings (RSV)
2.4.7. NRRS Residue Measures
2.5. Skin Displacements
2.6. Inter-Rater Reliability
2.7. Statistical Analysis
3. Results
3.1. Hyolaryngeal Excursion
3.2. Clinical Measures of Dysphagia Severity
3.2.1. Penetration-Aspiration
3.2.2. Post-Swallow Residue
3.3. Inter-Rater Reliability
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carucci, L.R.; Turner, M.A. Dysphagia revisited: Common and unusual causes. RadioGraphics 2015, 35, 105–122. [Google Scholar] [CrossRef]
- Cohen, D.L.; Roffe, C.; Beavan, J.; Blackett, B.; Fairfield, C.A.; Hamdy, S.; Bath, P.M. Post-stroke dysphagia: A review and design considerations for future trials. Int. J. Stroke 2016, 11, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Medin, J.; Larson, J.; von Arbin, M.; Wredling, R.; Tham, K. Elderly persons’ experience and management of eating situations 6 months after stroke. Disabil. Rehabil. 2010, 32, 1346–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, K.W.; Yu, G.P.; Schaefer, S.D. Consequence of dysphagia in the hospitalized patient: Impact on prognosis and hospital resources. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 784–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, D.A.; Krishnaswami, S.; Steger, E.; Conover, E.; Vaezi, M.F.; Ciucci, M.R.; Francis, D.O. Economic and survival burden of dysphagia among inpatients in the United States. Dis. Esophagus 2017, 31, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.P.; Frank, C.; Moltz, C.C.; Vos, P.; Smith, H.J.; Karlsson, U.; Sallah, S. Impact of dysphagia on quality of life after treatment of head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 772–778. [Google Scholar] [CrossRef]
- Wilson, R.D. Mortality and cost of pneumonia after stroke for different risk groups. J. Stroke Cerebrovasc. Dis. 2012, 21, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Feng, M.C.; Lin, Y.C.; Chang, Y.H.; Chen, C.H.; Chiang, H.C.; Huang, L.C.; Hung, C.H. The mortality and the risk of aspiration pneumonia related with dysphagia in Stroke Patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1381–1387. [Google Scholar] [CrossRef]
- Pearson, W.G.; Molfenter, S.M.; Smith, Z.M.; Steele, C.M. Image-based measurement of post-swallow residue: The normalized residue ratio scale. Dysphagia 2013, 28, 167–177. [Google Scholar] [CrossRef] [Green Version]
- Carbo, A.; Brown, M.; Nakrour, N. Fluoroscopic Swallowing Examination: Radiologic Findings and Analysis of Their Causes and Pathophysiologic Mechanisms. RadioGraphics 2021, 41, 1733–1749. [Google Scholar] [CrossRef]
- Lind, C.D. Dysphagia: Evaluation and treatment. Gastroenterol. Clin. N. Am. 2003, 32, 553–575. [Google Scholar] [CrossRef]
- Deborah, J.C.; Ramsey, M.R.C.P.; David, G.; Smithard, M.D.; Lalit, K. Early Assessments of Dysphagia and Aspiration Risk in Acute Stroke Patients. Stroke 2003, 34, 1252–1257. [Google Scholar] [CrossRef]
- Guan, X.-L.; Wang, H.; Huang, H.-S.; Meng, L. Prevalence of dysphagia in multiple sclerosis: A systematic review and meta-analysis. Neurol. Sci. 2015, 36, 671–681. [Google Scholar] [CrossRef]
- Wilson, R.D.; Howe, E.C. A cost-effectiveness analysis of screening methods for dysphagia after stroke. PMR 2012, 4, 273–282. [Google Scholar] [CrossRef]
- Yoon, J.A.; Kim, S.H.; Jang, M.H.; Kim, S.D.; Shin, Y.B. Correlations between aspiration and pharyngeal residue scale scores for fibreoptic endoscopic evaluation and videofluoroscopy. Yonsei Med. J. 2019, 60, 1181–1186. [Google Scholar] [CrossRef]
- Rumbach, A.; Coombes, C.; Doeltgen, S. A survey of australian dysphagia practice patterns. Dysphagia 2017, 33, 216–226. [Google Scholar] [CrossRef]
- Kendall, K.; McKenzie, S.; Leonard, R. Timing of Events in Normal Swallowing: A Videofluoroscopic Study. Dysphagia 2000, 15, 74–83. [Google Scholar] [CrossRef]
- Choi, K.H.; Ryu, J.S.; Kim, M.Y. Kinematic Analysis of Dysphagia: Significant Parameters of Aspiration Related to Bolus Viscosity. Dysphagia 2011, 26, 392–398. [Google Scholar] [CrossRef]
- Leonard, R.; Kendall, K.; McKenzie, S. Structural Displacements in Normal Swallowing: A Videofluoroscopic Study. Dysphagia 2000, 15, 146–152. [Google Scholar] [CrossRef]
- Perlman, A.L.; Booth, B.; Grayhack, J. Videofluoroscopic predictors of aspiration in patients with oropharyngeal dysphagia. Dysphagia 1994, 9, 90–95. [Google Scholar] [CrossRef]
- Cichero, J.; Murdoch, B. Applied anatomy and physiology of the normal swallow. In Dysphagia: Foundation, Theory and Practice; John Wiley & Sons, Ltd.: Chichester, UK, 2006; pp. 3–25. [Google Scholar]
- Hsiao, M.Y.; Chang, Y.C.; Chen, W.S.; Chang, H.-Y.; Wang, T.-G. Application of ultrasonography in assessing oropharyngeal dysphagia in stroke patients. Ultrasound Med. Biol. 2012, 38, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Nordin, N.A.; Miles, A.; Allen, J. Measuring competency development in objective evaluation of videofluoroscopic swallowing studies. Dysphagia 2017, 32, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Donohue, C.; Khalifa, Y.; Perera, S.; Sejdić, E.; Coyle, J.L. A Preliminary Investigation of Whether HRCA Signals Can Differentiate Between Swallows from Healthy People and Swallows from People with Neurodegenerative Diseases. Dysphagia 2021, 36, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Arafa, H.M.; Yoo, J.Y. Soft skin-interfaced mechano-acoustic sensors for real-time monitoring and patient feedback on respiratory and swallowing biomechanics. NPJ Digit. Med. 2022, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Gilmour, S.; Hoshino, E.; Nakayama, E.; Momosaki, R.; Sakata, N.; Yoneoka, D. A machine learning-based screening test for sarcopenic dysphagia using image recognition. Nutrients 2021, 13, 4009. [Google Scholar] [CrossRef]
- Lam Po Tang, E.J.; HajiRassouliha, A.; Nash, M.P.; Nielsen, P.M.F.; Taberner, A.J.; Cakmak, Y.O. Non-contact quantification of jugular venous pulse waveforms from skin displacements. Sci. Rep. 2018, 8, 17236. [Google Scholar] [CrossRef] [Green Version]
- HajiRassouliha, A.; Taberner, A.J.; Nash, M.P.; Nielsen, P.M.F. Subpixel measurement of living skin deformation using intrinsic features. In Computational Biomechanics for Medicine; Wittek, A., Joldes, G., Nielsen, P., Doyle, B., Miller, K., Eds.; Springer: Cham, Switzerland, 2017; pp. 91–99. [Google Scholar] [CrossRef]
- HajiRassouliha, A.; Taberner, A.J.; Nash, M.P.; Nielsen, P.M.F. Subpixel phase-based image registration using Savitzky–Golay differentiators in gradient-correlation. Comput. Vis. Image Underst. 2018, 170, 28–39. [Google Scholar] [CrossRef]
- Molfenter, S.M.; Brates, D.; Herzberg, E.; Noorani, M.; Lazarus, C. The swallowing profile of healthy aging adults: Comparing noninvasive swallow tests to videofluoroscopic measures of safety and efficiency. J. Speech Lang. Hear. Res. 2018, 61, 1603–1612. [Google Scholar] [CrossRef]
- Rosenbek, J.C.; Robbins, J.A.; Roecker, E.B.; Coyle, J.L.; Wood, J.L. A penetration-aspiration scale. Dysphagia 1996, 11, 93–98. [Google Scholar] [CrossRef]
- Eisenhuber, E.; Schima, W.; Schober, E.; Pokieser, P.; Stadler, A.; Scharitzer, M.; Oschatz, E. Videofluoroscopic assessment of patients with dysphagia. Am. J. Roentgenol. 2002, 178, 393–398. [Google Scholar] [CrossRef]
- Kim, Y.; McCullough, G.H. Maximal hyoid excursion in poststroke patients. Dysphagia 2010, 25, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhou, Y.; Wei, N.; Yang, B.; Wang, A.; Zhou, H.; Groher, M. Laryngeal elevation velocity and aspiration in acute ischemic stroke patients. PLoS ONE 2016, 11, e0162257. [Google Scholar] [CrossRef] [Green Version]
- Cullins, M.J.; Gill, J.P.; McManus, J.M.; Lu, H.; Shaw, K.M.; Chiel, H.J. Sensory feedback reduces individuality by increasing variability within Subjects. Curr. Biol. 2015, 25, 2672–2676. [Google Scholar] [CrossRef] [Green Version]
- Söder, N.; Miller, N. Using ultrasound to investigate intrapersonal variability in durational aspects of tongue movement during swallowing. Dysphagia 2002, 17, 288–297. [Google Scholar] [CrossRef]
- Robbins, J.; Coyle, J.; Rosenbek, J.; Roecker, E.; Wood, J. Differentiation of normal and abnormal airway protection during swallowing using the penetration–aspiration scale. Dysphagia 1999, 14, 228–232. [Google Scholar] [CrossRef]
- Wechsler, S. Statistics at Square One, 9th ed.; Campbell, M.J.T., Swinscow, D.V., Eds.; BMJ Publishing Group: London, UK, 1996; Volume 16, pp. 2629–2630. [Google Scholar] [CrossRef]
- Ishida, R.; Palmer, J.B.; Hiiemae, K.M. Hyoid motion during swallowing: Factors affecting forward and upward displacement. Dysphagia 2002, 17, 262–272. [Google Scholar] [CrossRef]
- Molfenter, S.M.; Steele, C.M. Physiological variability in the deglutition literature: Hyoid and laryngeal kinematics. Dysphagia 2011, 26, 67–74. [Google Scholar] [CrossRef]
- Steele, C.M.; Cichero, J.A.Y. Physiological factors related to aspiration risk: A systematic review. Dysphagia 2014, 29, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Ueda, N.; Nohara, K.; Kotani, Y.; Tanaka, N.; Okuno, K.; Sakai, T. Effects of the bolus volume on hyoid movements in normal individuals. J. Oral. Rehabil. 2013, 40, 491–499. [Google Scholar] [CrossRef]
- Ertekin, C.; Aydogdu, I. Neurophysiology of swallowing. Clin. Neurophysiol. 2003, 114, 2226–2244. [Google Scholar] [CrossRef]
- Warshafsky, D.; Goldenberg, D.; Kanekar, S.G. Imaging anatomy of deep neck spaces. Otolaryngol. Clin. N. Am. 2012, 45, 1203–1221. [Google Scholar] [CrossRef] [PubMed]
- Mitz, V.; Peyronie, M. The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plast. Reconst. Surg. 1976, 58, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Humbert, I.A.; Poletto, C.J.; Saxon, K.G.; Kearney, P.R.; Crujido, L.; Wright-Harp, W.; Ludlow, C.L. The effect of surface electrical stimulation on hyolaryngeal movement in normal individuals at rest and during swallowing. J. Appl. Physiol. 2006, 101, 1657–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, W.G.; Langmore, S.E.; Zumwalt, A.C. Evaluating the structural properties of suprahyoid muscles and their potential for moving the hyoid. Dysphagia 2011, 26, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Jung, B.; Bhutta, S. Anatomy, Head and Neck, Neck Movements. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: https://www-ncbi-nlm-nih-gov.cmezproxy.chmeds.ac.nz/books/NBK557555/ (accessed on 15 June 2022).
- Kohan, E.J.; Wirth, G.A. Anatomy of the neck. Clin. Plast. Surg. 2014, 41, 1–6. [Google Scholar] [CrossRef]
- Malone, J.C.; Arya, N.R. Anatomy, Head and Neck, Swallowing. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: https://www.ncbi.nlm.nih.gov/books/NBK554405/ (accessed on 15 June 2022).
- Leonard, R. Predicting aspiration risk in patients with dysphagia: Evidence from fluoroscopy. Laryngoscope Investig. Otolaryngol. 2019, 4, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Stokely, S.L.; Peladeau-Pigeon, M.; Leigh, C.; Molfenter, S.M.; Steele, C.M. The relationship between pharyngeal constriction and post-swallow residue. Dysphagia 2015, 30, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Zhang, T.; Sun, X.; Xu, J.; Jiang, G. Quantitative videofluoroscopic analysis of penetration-aspiration in post-stroke patients. Neurol. India 2010, 58, 42–47. [Google Scholar] [CrossRef]
- Perlman, A.L.; VanDaele, D.J.; Otterbacher, M.S. Quantitative assessment of Hyoid bone displacement from video images during swallowing. J. Speech Lang. Hear. Res. 1995, 38, 579–585. [Google Scholar] [CrossRef]
- Zhang, Z.; Perera, S.; Donohue, C.; Kurosu, A.; Mahoney, A.S.; Coyle, J.L.; Sejdić, E. The prediction of risk of penetration–aspiration via hyoid bone displacement features. Dysphagia 2020, 35, 66–72. [Google Scholar] [CrossRef]
- Zhang, Z.; Kurosu, A.; Coyle, J.L.; Perera, S.; Sejdić, E. A generalized equation approach for hyoid bone displacement and penetration–aspiration scale analysis. SN Appl. Sci. 2021, 3, 688. [Google Scholar] [CrossRef]
- Friedman, B.; Frazier, J.B. Deep laryngeal penetration as a predictor of aspiration. Dysphagia 2000, 15, 153–158. [Google Scholar] [CrossRef]
- Gurberg, J.; Birnbaum, R.; Daniel, S.J. Laryngeal penetration on videofluoroscopic swallowing study is associated with increased pneumonia in children. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1827–1830. [Google Scholar] [CrossRef]
- Nakamura, T.; Kita, Y.; Fujimoto, J.; Ayuzawa, K.; Ozawa, H. Hyoid bone movement during swallowing and mechanism of pharyngeal residue in patients with profound intellectual and multiple disabilities. Int. J. Pediatr. Otorhinolaryngol. 2021, 149, 110849. [Google Scholar] [CrossRef]
- Steele, C.M.; Bailey, G.L.; Chau, T.; Molfenter, S.M.; Oshalla, M.; Waito, A.A.; Zoratto, D.C. The relationship between hyoid and laryngeal displacement and swallowing impairment. Clin. Otolaryngol. 2011, 36, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Molfenter, S.M.; Steele, C.M. The relationship between residue and aspiration on the subsequent swallow: An application of the normalized residue ratio scale. Dysphagia 2013, 28, 494–500. [Google Scholar] [CrossRef]
- Dejaeger, E.; Pelemans, W.; Ponette, E.; Joosten, E. Mechanisms involved in postdeglutition retention in the elderly. Dysphagia 1997, 12, 63–67. [Google Scholar] [CrossRef]
- Troche, M.S.; Huebner, I.; Rosenbek, J.C.; Okun, M.S.; Sapienza, C.M. Respiratory-swallowing coordination and swallowing safety in patients with parkinson’s disease. Dysphagia 2011, 26, 218–224. [Google Scholar] [CrossRef]
- Ellerston, J.K.; Heller, A.C.; Houtz, D.R.; Kendall, K.A. Quantitative measures of swallowing deficits in patients with parkinson’s disease. Ann. Otol. Rhinol. 2016, 125, 385–392. [Google Scholar] [CrossRef]
- Han, T.R.; Paik, N.-J.; Park, J.W. Quantifying swallowing function after stroke: A functional dysphagia scale based on videofluoroscopic studies. Arch. Phys. Med. Rehabil. 2001, 82, 677–682. [Google Scholar] [CrossRef]
- Gaeckle, M.; Domahs, F.; Kartmann, A.; Tomandl, B.; Frank, U. Predictors of penetration-aspiration in parkinson’s disease patients with dysphagia: A retrospective analysis. Ann. Otol. Rhinol. Laryngol. 2019, 128, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Shin, G.; Jun, A.; Park, T.; Ko, D.; Choi, E.; Kim, Y. The relation between the presence of aspiration or penetration and the clinical indicators of dysphagia in poststroke survivors. Ann. Rehabil. Med. 2016, 40, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, J.A.; Molfenter, S.; Troche, M.S. Predictors of residue and airway invasion in parkinson’s disease. Dysphagia 2020, 35, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabré, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail. J. Neurogastroenterol. Motil. 2010, 22, e230. [Google Scholar] [CrossRef]
- Tarricone, R.; Petracca, F.; Ciani, O.; Cucciniello, M. Distinguishing features in the assessment of mHealth apps. Expert. Rev. Pharmacoecon. Outcomes Res. 2021, 21, 521–526. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 20–80 years |
| Sex | 11 Male, 12 Female |
| Diagnosis | Huntington gene positive (2); inclusion body myositis (1); esophageal motility disorder (1); diffuse idiopathic skeletal hyperostosis (1); stroke (3); listeria rhombencephalitis (1); muscular dystrophy (1); traumatic brain injury (2); head and neck cancer (2); cerebral palsy (1); Parkinson’s disease (1); multiple sclerosis (1); rigid spine (1); diagnosis unknown (5). |
| Hyoid | Larynx | |||
|---|---|---|---|---|
| Skin Displacements of Corresponding ROA | 3 mL | 20 mL | 3 mL | 20 mL |
| X displacement (%) | −0.25 (0.11) | 0.67 *** (0.0001) | 0.08 (0.6) | 0.17 (0.42) |
| Y displacement (%) | 0.07 (0.66) | 0.04 (0.81) | 0.17 (0.29) | 0.34 (0.09) |
| Xdisplacement velocity (%/s) | −0.21 (0.20) | 0.14 (0.48) | 0.29 (0.07) | −0.34 (0.09) |
| Y displacement velocity (%/s) | 0.22 (0.16) | −0.30 (0.12) | 0.04 (0.8) | −0.11 (0.72) |
| Hyoid | Larynx | |||
|---|---|---|---|---|
| Skin Displacements of Corresponding ROA | 3 mL | 20 mL | 3 mL | 20 mL |
| X displacement (%) | −0.06 (0.77) | −0.05 (0.85) | 0.01 (0.92) | −0.002 (0.99) |
| Y displacement (%) | −0.15 (0.35) | 0.02 (0.9) | 0.27 (0.09) | −0.18 (0.42) |
| X displacement velocity (%/s) | −0.44 ** (0.04) | −0.16 (0.61) | 0.023 (0.90) | −0.37 (0.11) |
| Y displacement velocity (%/s) | −0.15 (0.35) | 0.02 (0.90) | 0.23 (0.18) | −0.05 (0.81) |
| Skin Displacements | PAS (all n = 61) | PAS (scores of 2+) (n = 26) | PAS (3+) (n = 11) | PAS (2–5, Penetration only = 25) | |
|---|---|---|---|---|---|
| X displacement (%) | 0.16 (0.23) | 0.35 (0.09) | 0.33 (0.34) | 0.35 (0.09) | |
| Hyoid ROA | Y displacement (%) | −0.06 (0.65) | 0.02 (0.92) | 0.31 (0.35) | 0.02 (0.9) |
| X velocity (%/s) | 0.13 (0.31) | 0.40 (0.053) | 0.58 (0.07) | 0.41 (0.053) | |
| Y velocity (%/s) | −0.07 (0.56) | 0.06 (0.76) | 0.48 (0.15) | 0.06 (0.76) | |
| Larynx ROA | X displacement (%) | 0.02 (0.88) | 0.53 (0.09) | 0.77 (0.22) | 0.53 (0.09) |
| Y displacement (%) | −0.09 (0.54) | 0.39 (0.23) | 0.97 (0.78) | 0.39 (0.23) | |
| X velocity (%/s) | −0.09 (0.55) | 0.30 (0.37) | 0.77 (0.22) | 0.3 (0.37) | |
| Y velocity (%/s) | −0.09 (0.71) | −0.08 (0.80) | −0.44 (0.55) | −0.08 (0.80) | |
| Anterior ROA | X displacement (%) | 0.100 (0.47) | 0.18 (0.48) | 0.55 (0.12) | 0.18 (0.48) |
| Y displacement (%) | 0.07 (0.62) | 0.15 (0.56) | −0.56 (0.14) | 0.15 (0.56) | |
| X velocity (%/s) | 0.12 (0.39) | 0.14 (0.56) | 0.42 (0.29) | 0.14 (0.56) | |
| Y velocity (%/s) | 0.09 (0.51) | 0.16 (0.51) | −0.80 *** (0.01) | 0.17 (0.51) |
| Skin Displacements | RSRv (n = 61) | RSRp (n = 61) | NRRS v (n = 61) | NRRS p (n = 61) | RSRv (Exhibit Residue n = 37) | RSRp (Exhibit Residue n = 37) | NRRS v (Exhibit Residue n = 37) | NRRS p (Exhibit Residue n = 37) | |
|---|---|---|---|---|---|---|---|---|---|
| Hyoid ROA | X displacement (%) | −0.22 (0.08) | −0.10 (0.43) | −0.08 (0.52) | −0.06 (0.65) | −0.20 (0.26) | −0.08 (0.57) | −0.34 (0.22) | −0.05 (0.78) |
| Y displacement (%) | 0.01 (0.91) | 0.03 (0.83) | 0.06 (0.64) | 0.01 (0.93) | −0.01 (0.53) | 0.07 (0.66) | −0.21 (0.41) | 0.41 ** (0.047) | |
| X velocity (%/s) | −0.16 (0.20) | −0.08 (0.53) | −0.15 (0.23) | −0.11 (0.4) | −0.11 (0.40) | 0.01 (0.53) | −0.27 (0.34) | 0.47 ** (0.010) | |
| Y velocity (%/s) | 0.05 (0.70) | 0.06 (0.62) | 0.06 (0.64) | 0.03 (0.47) | −0.12 (0.80) | 0.15 (0.31) | −0.13 (0.59) | 0.57 ** (0.001) | |
| Larynx ROA | X displacement (%) | 0.04 (0.77) | 0.04 (0.79) | −0.23 (0.13) | 0.004 (0.77) | −0.04 (0.83) | −0.33 * (0.04) | −0.33 (0.28) | 0.62 *** (0.03) |
| Y displacement (%) | −0.22 (0.12) | −0.13 (0.38) | −0.15 (0.29) | −0.17 (0.22) | −0.11 (0.55) | −0.32 (0.05) | −0.32 (0.29) | −0.48 ** (0.03) | |
| X velocity (%/s) | 0.15 (0.31) | 0.07 (0.65) | −0.16 (0.30) | 0.07 (0.66) | 0.04 (0.85) | −0.23 (0.18) | −0.10 (0.74) | −0.05 (0.83) | |
| Y velocity (%/s) | −0.11 (0.47) | −0.02 (0.87) | 0.0009 (0.99) | 0.01 (0.9) | 0.13 (0.50) | −0.23 (0.16) | −0.32 (0.31) | −0.17 (0.2) | |
| Anterior ROA | X displacement (%) | −0.16 (0.23) | −0.08 (0.58) | 0.11 (0.49) | 0.07 (0.64) | −0.32 (0.07) | −0.01 (0.55) | −0.45 (0.050) | 0.37 (0.16) |
| Y displacement (%) | −0.0782 (0.57) | 0.123 (0.36) | 0.03 (0.82) | 0.04 (0.77) | 0.05 (0.74) | 0.08 (0.59) | −0.20 (0.53) | −0.08 (0.74) | |
| X velocity (%/s) | −0.13 (0.33) | 0.03 (0.82) | 0.10 (0.54) | 0.05 (0.73) | −0.28 (0.12) | 0.009 (0.95) | −0.36 (0.16) | 0.46 (0.07) | |
| Y velocity (%/s) | −0.008 (0.95) | 0.17 (0.22) | 0.07 (0.65) | 0.04 (0.79) | 0.12 (0.50) | 0.057 (0.72) | −0.26 (0.43) | −0.17 (0.52) |
| Parameters | ICC Value | Interpretation |
|---|---|---|
| Internal Hyoid displacement | 0.95 | Excellent reliability |
| Internal Laryngeal displacement | 0.97 | Excellent reliability |
| PAS rating | 0.99 | Excellent reliability |
| Residue Severity ratings | 0.97 | Excellent reliability |
| NRRSv | 0.34 | Poor reliability |
| NRRSp | 0.23 | Poor reliability |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chesney, N.; Khwaounjoo, P.; Huckabee, M.-L.; Cakmak, Y.O. Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements. Sensors 2023, 23, 5392. https://doi.org/10.3390/s23125392
Chesney N, Khwaounjoo P, Huckabee M-L, Cakmak YO. Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements. Sensors. 2023; 23(12):5392. https://doi.org/10.3390/s23125392
Chicago/Turabian StyleChesney, Nikyta, Prashanna Khwaounjoo, Maggie-Lee Huckabee, and Yusuf Ozgur Cakmak. 2023. "Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements" Sensors 23, no. 12: 5392. https://doi.org/10.3390/s23125392
APA StyleChesney, N., Khwaounjoo, P., Huckabee, M.-L., & Cakmak, Y. O. (2023). Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements. Sensors, 23(12), 5392. https://doi.org/10.3390/s23125392