
SMART System in the Assessment of Exercise Tolerance in Adults
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
- voluntary participation: confirmed by informed consent to participate in the study;
- age: 18–65 years;
- no health contraindications to perform exercise testing. This criterion was verified by conducting a medical examination before the tests included in the SMART program.
- The first second and the following minutes of HR were taken into account. Mean HR was calculated based on SMART (Polar H10 heart rate monitor) and ECG measurements;
- The difference between SMART and ECG measurements (absolute values) was calculated;
- The difference between SMART and ECG measurements in % [(difference in absolute values/mean heart rate from SMART and ECG measurements) x 100] was calculated.
- Data were collected on the morphological parameters of the participants. Body height and waist and hip circumferences were measured to calculate the weight-to-height ratio (WHR). Body weight, BMI, and %FAT data were obtained from BIA analysis using an In Body 770 device.
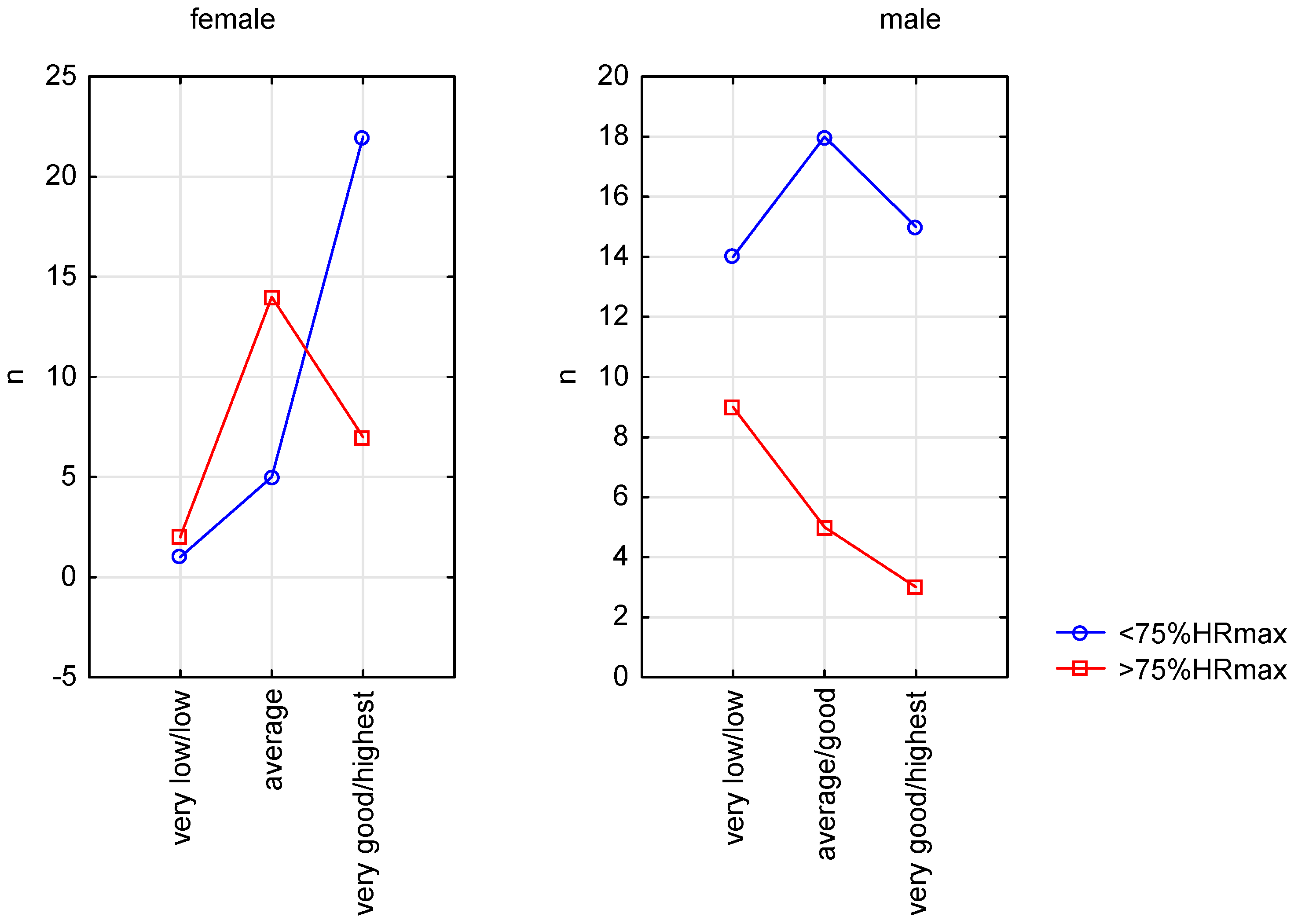
- Aerobic capacity levels were estimated using the Astrand–Rhyming step test. This indirect method of assessing the maximal oxygen uptake uses the established relationship between exercise oxygen uptake and heart rate. The qualitative VO2max assessment was made according to standardized criteria [38]. Next, for statistical analyses, the participants were divided into three groups: I—very low or low exercise performance; II—average or good exercise performance; III—very good or highest exercise performance.
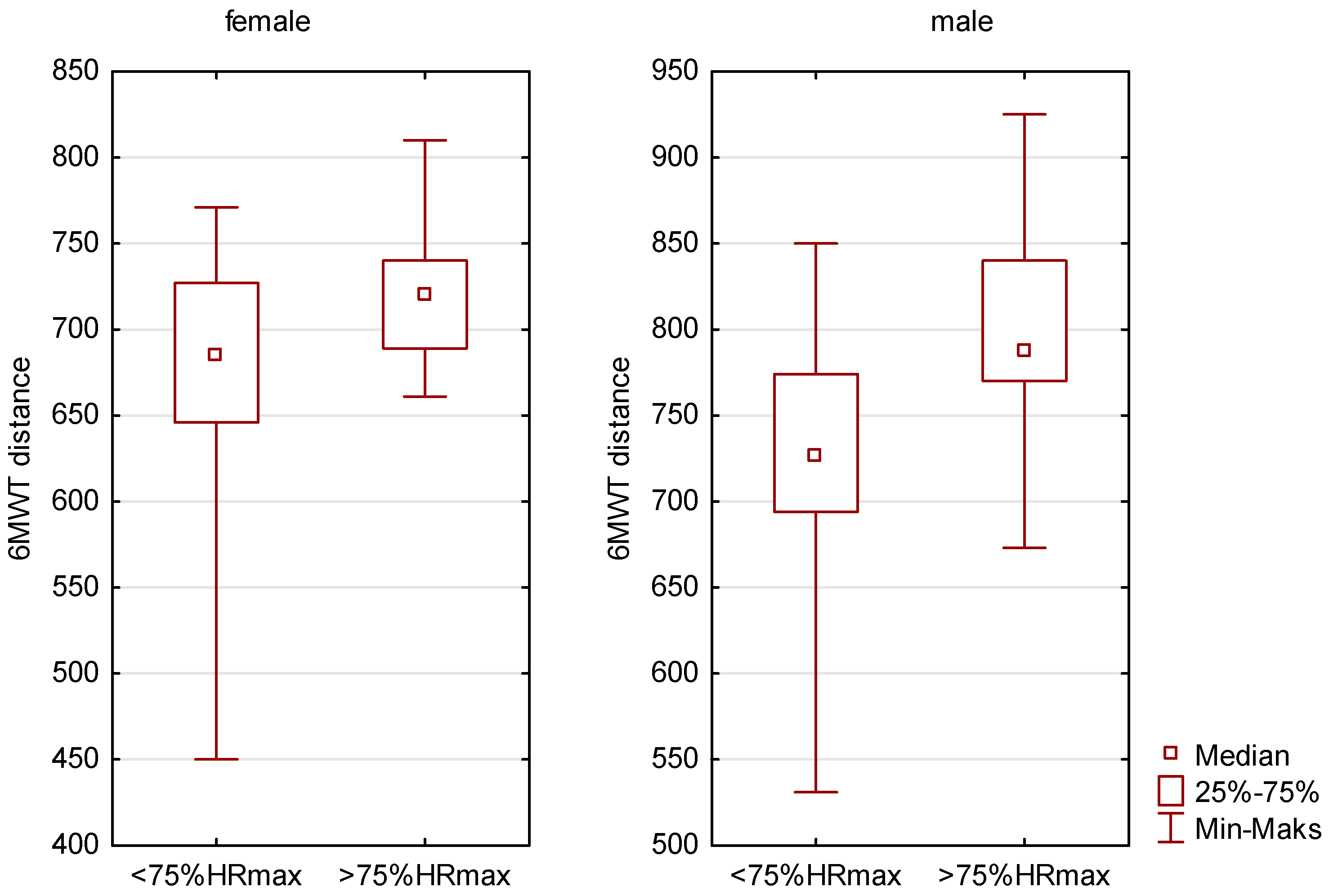
- The participants performed the 6MWT test. This test was conducted on a running track with a 400 m circumference. The distance covered was measured to the nearest 1 m using a tape measure. Step count data were collected from the SMART system. The mean step length was calculated by dividing the distance by the number of steps.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mendonca, G.V.; Pezarat-Correia, P.; Vaz, J.R.; Silva, L.; Almeida, I.D.; Heffernan, K.S. Impact of Exercise Training on Physiological Measures of Physical Fitness in the Elderly. Curr. Aging Sci. 2016, 9, 240–259. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Casu, M.; Amato, M.; Cocuzza, D.; Galofaro, V.; La Morella, A.; Paladino, S.; Pulino, K.; Raia, N.; Vella, M.C.; et al. The Effects of Physical Exercise on Mental Health: From Cognitive Improvements to Risk of Addiction. Int. J. Environ. Res. Public Health 2021, 18, 13384. [Google Scholar] [CrossRef] [PubMed]
- Dhuli, K.; Naureen, Z.; Medori, M.C.; Fioretti, F.; Caruso, P.; Perrone, M.A.; Nodari, S.; Manganotti, P.; Xhufi, S.; Bertelli, M.; et al. Physical activity for health. J. Prev. Med. Hyg. 2022, 63 (Suppl. S3), E150–E159. [Google Scholar] [CrossRef] [PubMed]
- Dimitri, P.; Joshi, K.; Jones, N. Moving Medicine for Children Working Group. Moving more: Physical activity and its positive effects on long term conditions in children and young people. Arch. Dis. Child. 2020, 105, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, S.; Li, G.; Xiao, J. Exercise Regulates the Immune System. Adv. Exp. Med. Biol. 2020, 1228, 395–408. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.S.; Kelly, M.P.; Kelly, P. Metabolomics, physical activity, exercise and health: A review of the current evidence. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165936. [Google Scholar] [CrossRef] [PubMed]
- da Costa, B.R.; Vieira, E.R. Stretching to reduce work-related musculoskeletal disorders: A systematic review. J. Rehabil. Med. 2008, 40, 321–328. [Google Scholar] [CrossRef]
- McTiernan, A.N.N.E.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Piercy, K.L.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]
- Romanowska, A.; Morawiak, A.; Woods, C.; Kelly, L.; Volf, K.; Gelius, P.; Messing, S.; Forberger, S.; Lakerveld, J.; Den Braver, N.R. Health Enhancing Physical Activity Policies in Poland: Findings from the HEPA PAT Survey. Int. J. Environ. Res. Public Health 2022, 19, 7284. [Google Scholar] [CrossRef]
- Eager, D.; Zhou, S.; Ishac, K.; Hossain, I.; Richards, A.; Sharwood, L.N. Investigation into the Trampoline Dynamic Characteristics and Analysis of Double Bounce Vibrations. Sensors 2022, 22, 2916. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Powell, K.E.; Haskell, W.L.; Janz, K.F.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease. Med. Sci. Sports Exerc. 2019, 51, 1270–1281. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Walker, M. Changes in physical activity, mortality, and incidence of coronary heart disease in older men. Lancet 1998, 351, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Hamer, M.; Lawlor, D.A. Physical activity, mortality, and cardiovascular disease: Is domestic physical activity beneficial? The Scottish Health Survey—1995, 1998, and 2003. Am. J. Epidemiol. 2009, 169, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Asif, I.M.; Maleszewski, J.J.; Owens, D.S.; Prutkin, J.M.; Salerno, J.C.; Zigman, M.L.; Ellenbogen, R.; Rao, A.L.; Ackerman, M.J.; et al. Incidence, Cause, and Comparative Frequency of Sudden Cardiac Death in National Collegiate Athletic Association Athletes: A Decade in Review. Circulation 2015, 132, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Rizzoli, G.; Schiavon, M.; Thiene, G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J. Am. Coll. Cardiol. 2003, 42, 1959–1963. [Google Scholar] [CrossRef]
- Orio, F.; Muscogiuri, G.; Ascione, A.; Marciano, F.; Volpe, A.; La Sala, G.; Savastano, S.; Colao, A.; Palomba, S. Effects of physical exercise on the female reproductive system. Minerva Endocrinol. 2013, 38, 305–319. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96, Erratum in Eur. Heart J. 2021, 42, 548–549. [Google Scholar] [CrossRef]
- Whang, W.; Manson, J.E.; Hu, F.B.; Chae, C.U.; Rexrode, K.M.; Willett, W.C.; Stampfer, M.J.; Albert, C.M. Physical exertion, exercise, and sudden cardiac death in women. JAMA 2006, 295, 1399–1403. [Google Scholar] [CrossRef]
- Reinier, K.; Sargsyan, A.; Chugh, H.S.; Nakamura, K.; Uy-Evanado, A.; Klebe, D.; Kaplan, R.; Hadduck, K.; Shepherd, D.; Young, C.; et al. Evaluation of Sudden Cardiac Arrest by Race/Ethnicity among Residents of Ventura County, California, 2015–2020. JAMA Netw. Open 2021, 4, e2118537. [Google Scholar] [CrossRef]
- Bassi, M.D.; Farina, J.M.; Bombau, J.; Maurice, M.F.; Bortman, G.; Nuñez, E.; Márquez, M.; Bornancini, N.; Baranchuk, A. Sudden Cardiac Arrest in Basketball and Soccer Stadiums, the Role of Automated External Defibrillators: A Review. For the BELTRAN Study (BaskEtbaLl and soccer sTadiums: Registry on Automatic exterNal defibrillators). Arrhythm. Electrophysiol. Rev. 2023, 12, e03. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Schlesinger, S.; Leitzmann, M.F.; Tonstad, S.; Norat, T.; Riboli, E.; Vatten, L.J. Physical activity and the risk of heart failure: A systematic review and dose-response meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 367–381. [Google Scholar] [CrossRef] [PubMed]
- American College of Cardiology Foundation/American Heart Association (ACCF/AHA). Guideline for the Management of Heart Failure. 2013. Available online: https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001063 (accessed on 5 November 2023).
- Duncan, M.J.; Mota, J.; Carvalho, J.; Nevill, A.M. Correction: An Evaluation of Prediction Equations for the 6 Minute Walk Test in Healthy European Adults Aged 50–85 Years. PLoS ONE 2015, 10, e0142463. [Google Scholar] [CrossRef] [PubMed]
- Halliday, S.J.; Wang, L.; Yu, C.; Vickers, B.P.; Newman, J.H.; Fremont, R.D.; Hemnes, A.R. Six-minute walk distance in healthy young adults. Respir. Med. 2020, 165, 105933. [Google Scholar] [CrossRef] [PubMed]
- Chirico, D.; Davidson, T.W.; Terada, T.; Scott, K.; Keast, M.L.; Reid, R.D.; Pipe, A.L.; Reed, J.L. Using the 6-min Walk Test to Monitor Peak Oxygen Uptake Response to Cardiac Rehabilitation in Patients With Heart Failure. J. Cardiopulm. Rehabil. Prev. 2020, 40, 378–382. [Google Scholar] [CrossRef]
- Brown, A.W.; Nathan, S.D. The Value and Application of the 6-Minute-Walk Test in Idiopathic Pulmonary Fibrosis. Ann. Am. Thorac. Soc. 2018, 15, 3–10. [Google Scholar] [CrossRef]
- Montes, J.; McDermott, M.P.; Martens, W.B.; Dunaway, S.; Glanzman, A.M.; Riley, S.; Quigley, J.; Montgomery, M.J.; Sproule, D.; Tawil, R.; et al. Six-Minute Walk Test demonstrates motor fatigue in spinal muscular atrophy. Neurology 2010, 74, 833–838. [Google Scholar] [CrossRef]
- Mathai, S.C.; Puhan, M.A.; Lam, D.; Wise, R.A. The minimal important difference in the 6-minute walk test for patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2012, 186, 428–433. [Google Scholar] [CrossRef]
- Martin, C.; Chapron, J.; Hubert, D.; Kanaan, R.; Honoré, I.; Paillasseur, J.-L.; Aubourg, F.; Dinh-Xuan, A.-T.; Dusser, D.; Fajac, I.; et al. Prognostic value of six minute walk test in cystic fibrosis adults. Respir. Med. 2013, 107, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, K.; Kienberger, K.; Niessner, C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2250. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Martínez, B.J.S.-A.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.; O’Connor, R.; Sivan, M. Long COVID and chronic COVID syndromes. J. Med. Virol. 2021, 93, 1242–1243. [Google Scholar] [CrossRef] [PubMed]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Herrero-Montes, M.; Fernández-de-Las-Peñas, C.; Ferrer-Pargada, D.; Izquierdo-Cuervo, S.; Abascal-Bolado, B.; Valera-Calero, J.A.; Paras-Bravo, P. Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain. Diagnostics 2023, 13, 847. [Google Scholar] [CrossRef]
- Zou, H.; Zhang, J.; Chen, X.; Wang, Y.; Lin, W.; Lin, J.; Chen, H.; Pan, J. Equations for the Six-Minute Walk Distance in the Healthy Chinese Han Population, Aged 18–30 Years. BMC Pulm. Med. 2017, 17, 119. [Google Scholar] [CrossRef]
- Cink, R.E.; Thomas, T.R. Validity of the Astrand-Ryhming nomogram for predicting maximal oxygen intake. Br. J. Sports Med. 1981, 15, 182–185. [Google Scholar] [CrossRef]
- Bautmans, I.; Lambert, M.; Mets, T. The six-minute walk test in community dwelling elderly: Influence of health status. BMC Geriatr. 2004, 4, 6. [Google Scholar] [CrossRef]
- Alison, J.A.; Kenny, P.; King, M.T.; McKinley, S.; Aitken, L.M.; Leslie, G.D.; Elliott, D. Repeatability of the six-minute walk test and relation to physical function in survivors of a critical illness. Phys. Ther. 2012, 92, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Morinder, G.; Mattsson, E.; Sollander, C.; Marcus, C.; Larsson, U.E. Six-minute walk test in obese children and adolescents: Reproducibility and validity. Physiother. Res. Int. 2009, 14, 91–104. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117, Erratum in Am. J. Respir. Crit. Care Med. 2016, 193, 1185. [Google Scholar] [CrossRef] [PubMed]
- Chetta, A.; Zanini, A.; Pisi, G.; Aiello, M.; Tzani, P.; Neri, M.; Olivieri, D. Reference values for the 6-min walk test in healthy subjects 20–50 years old. Respir. Med. 2006, 100, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Iwama, A.M.; Andrade, G.N.; Shima, P.; Tanni, S.E.; Godoy, I.; Dourado, V.Z. The six-minute walk test and body weight-walk distance product in healthy Brazilian subjects. Braz. J. Med. Biol. Res. 2009, 42, 1080–1085, Erratum in Braz. J. Med. Biol. Res. 2010, 43, 324. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T.; Gosselink, R.; Decramer, M. Six minute walking distance in healthy elderly subjects. Eur. Respir. J. 1999, 14, 270–274. [Google Scholar] [CrossRef]
- Enright, P.L.; McBurnie, M.A.; Bittner, V.; Tracy, R.P.; McNamara, R.; Arnold, A.; Newman, A.B. The 6-min walk test: A quick measure of functional status in elderly adults. Chest 2003, 123, 387–398. [Google Scholar] [CrossRef]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158 Pt 1, 1384–1387, Erratum in Am. J. Respir. Crit. Care Med. 2020, 201, 393. [Google Scholar] [CrossRef]
- Redelmeier, D.A.; Bayoumi, A.M.; Goldstein, R.S.; Guyatt, G.H. Interpreting small differences in functional status: The Six Minute Walk test in chronic lung disease patients. Am. J. Respir. Crit. Care Med. 1997, 155, 1278–1282. [Google Scholar] [CrossRef]
- O’Keeffe, S.T.; Lye, M.; Donnellan, C.; Carmichael, D.N. Reproducibility and responsiveness of quality of life assessment and six minute walk test in elderly heart failure patients. Heart 1998, 80, 377–382. [Google Scholar] [CrossRef]
- Bois, R.M.; Weycker, D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; Lancaster, L.; Noble, P.W.; Sahn, S.A.; Szwarcberg, J.; et al. Six-minute-walk test in idiopathic pulmonary fibrosis: Test validation and minimal clinically important difference. Am. J. Respir. Crit. Care Med. 2011, 183, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Bellet, R.N.; Adams, L.; Morris, N.R. The 6-minute walk test in outpatient cardiac rehabilitation: Validity, reliability and responsiveness--a systematic review. Physiotherapy 2012, 98, 277–286. [Google Scholar] [CrossRef]
- Gibbons, W.J.; Fruchter, N.; Sloan, S.; Levy, R.D. Reference values for a multiple repetition 6-minute walk test in healthy adults older than 20 years. J. Cardiopulm. Rehabil. 2001, 21, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Camarri, B.; Eastwood, P.R.; Cecins, N.M.; Thompson, P.J.; Jenkins, S. Six minute walk distance in healthy subjects aged 55–75 years. Respir. Med. 2006, 100, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Casanova, C.; Celli, B.R.; Barria, P.; Casas, A.; Cote, C.; De Torres, J.P.; Jardim, J.; Lopez, M.V.; Marin, J.M.; De Oca, M.M.; et al. The 6-min walk distance in healthy subjects: Reference standards from seven countries. Eur. Respir. J. 2011, 37, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Hachenberger, J.; Li, Y.M.; Siniatchkin, M.; Hermenau, K.; Ludyga, S.; Lemola, S. Heart Rate Variability’s Association with Positive and Negative Affect in Daily Life: An Experience Sampling Study with Continuous Daytime Electrocardiography over Seven Days. Sensors 2023, 23, 966. [Google Scholar] [CrossRef] [PubMed]
- Kraus, U.; Schneider, A.; Breitner, S.; Hampel, R.; Rückerl, R.; Pitz, M.; Geruschkat, U.; Belcredi, P.; Radon, K.; Peters, A. Individual daytime noise exposure during routine activities and heart rate variability in adults: A repeated measures study. Environ. Health Perspect. 2013, 121, 607–612. [Google Scholar] [CrossRef] [PubMed]
- No, M.; Kwak, H.B. Effects of environmental temperature on physiological responses during submaximal and maximal exercises in soccer players. Integr. Med. Res. 2016, 5, 216–222. [Google Scholar] [CrossRef]
- Schantz, P.; Salier Eriksson, J.; Rosdahl, H. The heart rate method for estimating oxygen uptake: Analyses of reproducibility using a range of heart rates from commuter walking. Eur. J. Appl. Physiol. 2019, 119, 2655–2671. [Google Scholar] [CrossRef]
- Lamberts, R.P.; Lemmink, K.A.; Durandt, J.J.; Lambert, M.I. Variation in heart rate during submaximal exercise: Implications for monitoring training. J. Strength Cond. Res. 2004, 18, 641–645. [Google Scholar] [CrossRef]
- Coyle, E.F. Physical activity as a metabolic stressor. Am. J. Clin. Nutr. 2000, 72, 512S–520S. [Google Scholar] [CrossRef] [PubMed]
- Solway, S.; Brooks, D.; Lacasse, Y.; Thomas, S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001, 119 (Suppl. S2), 256–270. [Google Scholar] [CrossRef] [PubMed]
- Noonan, V.; Dean, E. Submaximal exercise testing: Clinical application and interpretation. Phys. Ther. 2000, 80, 782–807. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Rauner, A.; Mess, F.; Woll, A. The relationship between physical activity, physical fitness and overweight in adolescents: A systematic review of studies published in or after 2000. BMC Pediatr. 2013, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Ring, K.; Pfeiffer, K.; Camhi, S.; Arredondo, E.; Pratt, C.; Pate, R.; Webber, L.S. Relationships among fitness, body composition, and physical activity. Med. Sci. Sports Exerc. 2008, 40, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Suarez, C.B.; Grimmer-Somers, K. The association of physical activity and physical fitness with pre-adolescent obesity: An observational study in Metromanila, Philippines. J. Phys. Act. Health 2011, 8, 804–810. [Google Scholar] [CrossRef]
- Riebe, D.E.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.E.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479, Erratum in Med. Sci. Sports Exerc. 2016, 48, 579. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal modeling of the relationship between age and maximal heart rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef]
- Poehling, C.P.; Llewellyn, T.L. The Effects of Submaximal and Maximal Exercise on Heart Rate Variability. Int. J. Exerc. Sci. 2019, 12, 9–14. [Google Scholar]
- Oja, P. Dose response between total volume of physical activity and health and fitness. Med. Sci. Sports Exerc. 2001, 33 (Suppl. S6), S428–S453. [Google Scholar] [CrossRef] [PubMed]
- Mora, S.; Cook, N.; Buring, J.E.; Ridker, P.M.; Lee, I.M. Physical activity and reduced risk of cardiovascular events: Potential mediating mechanisms. Circulation 2007, 116, 2110–2118. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R. Physical Activity and Cardiovascular Disease: How Much is Enough? Am. J. Lifestyle Med. 2009, 3 (Suppl. S1), 44S–49S. [Google Scholar] [CrossRef] [PubMed]
- Milewski, K.; Małecki, A.; Orszulik-Baron, D.; Kachel, M.; Hirnle, P.; Orczyk, M.; Duna, R.; Mikołajowski, G.; Janas, A.; Buszman, P.E. The use of modern telemedicine technologies in an innovative optimal cardiac rehabilitation program for patients after myocardial revascularization: Concept and design of RESTORE, a randomized clinical trial. Cardiol. J. 2019, 26, 594–603. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex | Pl | n | Age [Years] | Body Height [cm] | Body Weight [kg] | BMI | WHR | %FAT | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | |||
| female | I | 3 | 38.00 22–47 | >0.05 | 169.60 169–171 | >0.05 | 62.00 53.20–68.10 | >0.05 | 21.30 20.10–22.70 | >0.05 | 0.76 0.72–0.83 | >0.05 | 25.40 20.40–26.80 | >0.05 |
| II | 19 | 44.00 19–58 | 164.50 148–175 | 63.40 40.00–81.70 | 23.80 16.80–31.90 | 0.87 0.65–0.94 | 27.90 17.20–35.30 | |||||||
| III | 29 | 32.00 20–57 | 166 148–176 | 67.10 57.50–78.50 | 22.80 18.40–28.90 | 0.79 0.69–0.95 | 23.50 10.70–34.50 | |||||||
| male | I | 23 | 39.00 19–65 | >0.05 | 177.80 162–187 | >0.05 | 81.80 72.10–95.80 | >0.05 | 24.70 19.10–35.30 | >0.05 | 0.88 0.77–1.02 | >0.05 | 18.00 8.20–30.80 | >0.05 |
| II | 23 | 34.00 20–63 | 182.30 168–195 | 81,80 61.00–113.60 | 24.40 20.20–31.20 | 0.89 0.78–1.03 | 18.80 11.00–31.40 | |||||||
| III | 18 | 38.50 20–65 | 182.10 162–193 | 80.10 57.50–113.20 | 23.75 21.00–28.70 | 0.88 0.81–1.00 | 17.00 9.30–23.10 | |||||||
| Sex | Pl | n | Distance [m] | Number of Steps | Mean Step Length [m] | Mean HR 1–6′ | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | Median Min–Max | p | |||
| female | I | 3 | 714 667–751 | >0.05 | 819 780–828 | >0.05 | 0.87 0.86–0.91 | >0.05 | 161.00 108.17–173.50 | <0.05 |
| II | 19 | 689 573–771 | 804 653–909 | 0.85 0.71–1.12 | 146.50 73.67–170.83 | |||||
| III | 29 | 710 450–810 | 820 600–960 | 0.86 0.67–1.16 | 126.00 96.67–162.00 | |||||
| male | I | 23 | 731 600–910 | >0.05 | 767 639–902 | >0.05 | 0.93 0.78–1.11 | >0.05 | 131.67 101.83–153.17 | >0.05 |
| II | 23 | 727 531–888 | 798 724–853 | 0.92 0.73–1.05 | 125 96.83–159.17 | |||||
| III | 18 | 778.50 625–925 | 809.50 454–883 | 0.96 0.87–1.57 | 118.42 100.33–150.50 | |||||
| Sex | 6MWT Min | Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | ||||||||
| HR | % HRmax | n (%) Persons >75% HRmax | HR | % HRmax | n (%) Persons >75% HRmax | HR | % HRmax | n (%) Persons >75% HRmax | ||
| female | 1′ | 136 | 74 | 2 (67%) | 129 | 72 | 6 (32%) | 124 | 67 | 3 (10%) |
| 2′ | 144 | 78 | 2 (67%) | 136 | 76 | 14 (74%) | 129 | 70 | 7 (24%) | |
| 3′ | 147 | 80 | 2 (67%) | 139 | 78 | 14 (74%) | 130 | 71 | 7 (24%) | |
| 4′ | 152 | 83 | 2 (67%) | 147 | 83 | 15 (79%) | 131 | 71 | 9 (31%) | |
| 5′ | 153 | 83 | 2 (67%) | 147 | 82 | 15 (79%) | 131 | 71 | 8 (28%) | |
| 6′ | 154 | 84 | 2 (67%) | 145 | 81 | 16 (84%) | 127 | 69 | 5 (17%) | |
| male | 1′ | 125 | 70 | 5 (22%) | 116 | 63 | 0 | 116 | 64 | 0 |
| 2′ | 131 | 73 | 11 (48%) | 122 | 66 | 5 (22%) | 119 | 66 | 2 (11%) | |
| 3′ | 133 | 74 | 12 (52%) | 125 | 68 | 6 (26%) | 121 | 67 | 3 (17%) | |
| 4′ | 135 | 75 | 11 (48%) | 127 | 69 | 7 (30%) | 124 | 68 | 4 (22%) | |
| 5′ | 136 | 76 | 15 (65%) | 129 | 70 | 5 (22%) | 125 | 69 | 5 (28%) | |
| 6′ | 132 | 73 | 10 (43%) | 127 | 70 | 6 (26%) | 123 | 67 | 5 (28%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nierwińska, K.; Myśliwiec, A.; Konarska-Rawluk, A.; Lipowicz, A.; Małecki, A.; Knapik, A. SMART System in the Assessment of Exercise Tolerance in Adults. Sensors 2023, 23, 9624. https://doi.org/10.3390/s23249624
Nierwińska K, Myśliwiec A, Konarska-Rawluk A, Lipowicz A, Małecki A, Knapik A. SMART System in the Assessment of Exercise Tolerance in Adults. Sensors. 2023; 23(24):9624. https://doi.org/10.3390/s23249624
Chicago/Turabian StyleNierwińska, Katarzyna, Andrzej Myśliwiec, Anna Konarska-Rawluk, Anna Lipowicz, Andrzej Małecki, and Andrzej Knapik. 2023. "SMART System in the Assessment of Exercise Tolerance in Adults" Sensors 23, no. 24: 9624. https://doi.org/10.3390/s23249624
APA StyleNierwińska, K., Myśliwiec, A., Konarska-Rawluk, A., Lipowicz, A., Małecki, A., & Knapik, A. (2023). SMART System in the Assessment of Exercise Tolerance in Adults. Sensors, 23(24), 9624. https://doi.org/10.3390/s23249624