
Wearable Systems for Unveiling Collective Intelligence in Clinical Settings


 ,
,  ,
,  and
and 
Abstract
:1. Introduction
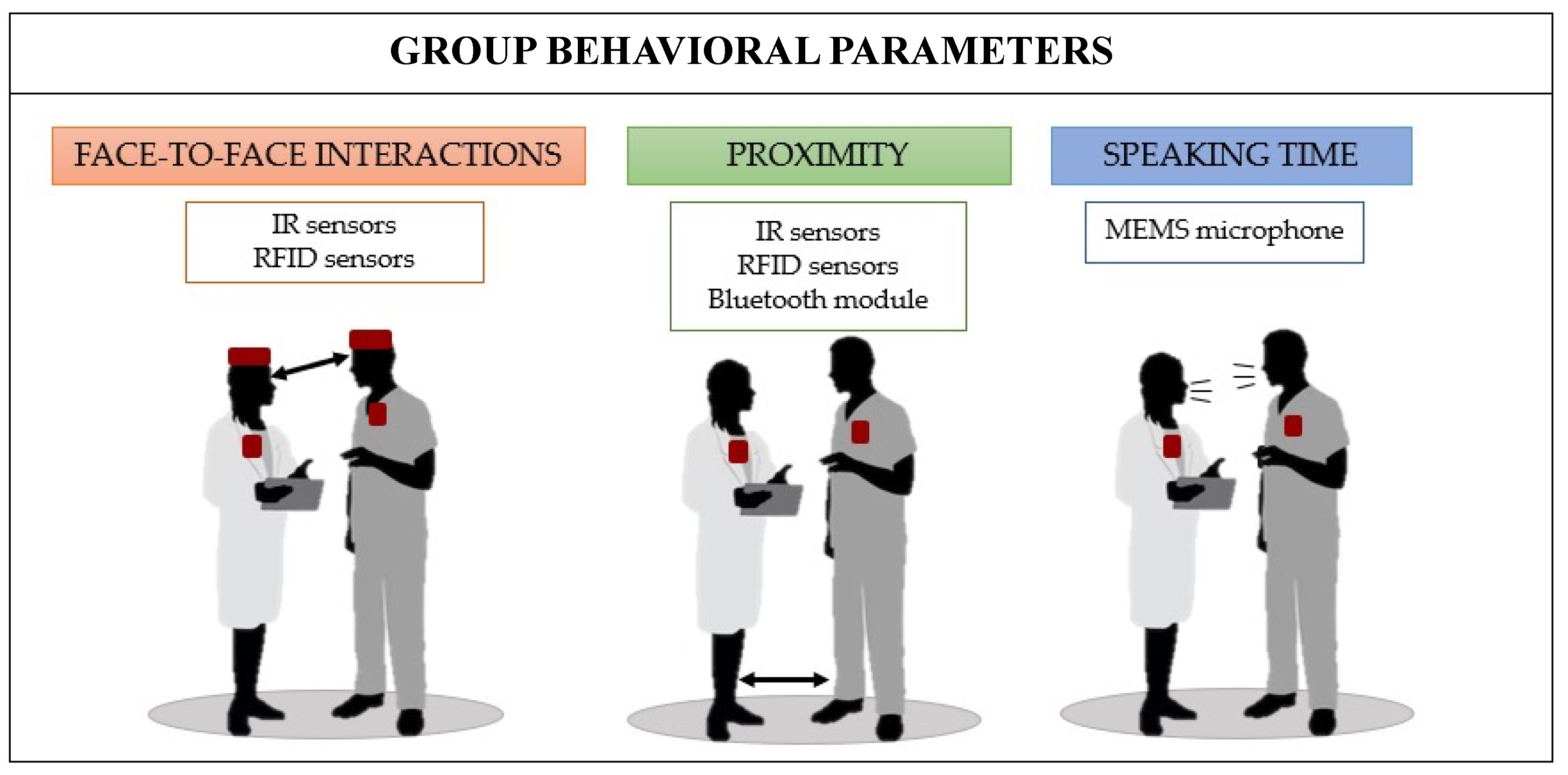
2. Wearables for Monitoring Group Behaviors
2.1. Face-to-Face Interactions
2.2. Proximity
2.3. Speaking Time

{kind=link}
{kind=link}
| Paper | Parameter | Working Principle | Wearable | Scenario | Pros | Cons |
|---|---|---|---|---|---|---|
| Hachisu T. et al., 2018 [22] | F2F: starting time and duration of each F2F | IR sensor | FaceLooks: headband-type wearable device 1 | Children with intellectual disabilities and/or ASD |
|
|
| Olguin D. et al., 2009 [36] | F2F: T-F2F 2 per person and NP-F2F 3 | IR sensor | Sociometric Badge, worn around the neck 1 | Nurses of a post-anaesthesia care unit (PACU) |
|
|
| Kawamoto E. et al., 2020 [41] | F2F: T-F2F 2 per person | IR sensor | The Business Microscope: wearable badge, attached to the participants’ front pockets 1 | Staff members of an intensive care unit (ICU) |
|
|
| Yu D. et al., 2016 [35] | F2F: T-F2F 2 for each actor pair | IR sensor | Sociometric Badge, worn around the neck 1 | Simulated team communication and patient care scenarios at an emergency department’s pediatric ward |
|
|
| Yu et al., 2015 [56] | F2F: T-F2F 2 for each actor pair | IR sensor | Sociometer Badge, worn around the neck 1 | Simulated hand-off scenarios at an emergency care environment |
|
|
| Isella et al., 2011 [24] | F2F: N-F2F 4 | RFID technology: exchanging of low-power radio packets | Active RFID badge 1 | Health care personnel, patients, and their caregivers at the pediatric ward of a hospital to study infectious disease transmissions |
|
|
| Vanhems et al., 2013 [55] | F2F-Ps 5: number and duration of F2F-Ps 5 | RFID technology: exchanging of ultra-low-power radio packets | Active RFID badge, worn with a lanyard on the chest 1 | Professional staff and patients at an acute care geriatric unit of a university hospital |
|
|
| Yu et al., 2015 [56] | Proximity: ND-Ps 6 | Bluetooth module | Sociometric badge, worn around the neck 1 | Simulated hand-off scenarios at an emergency care environment |
|
|
| Obadia et al., 2015 [65] | F2F-Ps 5: number and duration of F2F-Ps 5 | RFID technology: exchanging of low-power radio packets | Wireless sensor that the healthcare workers keep in the overcoat pocket and the patients keep in a pocket, or wear as a watch or around the ankle 1 | Patients and healthcare workers in a hospital in northern France |
|
|
| Yu et al., 2016 [35] | Proximity: detection vs. no detection and D-P 7 | Both IR and Bluetooth sensors | Sociometric Badge, worn around the neck 1 | Simulated team communication and patient care scenarios at an emergency department’s pediatric ward |
|
|
| Stefanini et al., 2020 [39] | Proximity: D-Ps 7 | Bluetooth module | Sociometric Badge, worn around the neck 1 | Surgical team of the Breast Unit of an Italian university hospital |
|
|
| Stefanini et al., 2021 [40] | Proximity: D-Ps 7 | Bluetooth module | Sociometric Badge, worn around the neck 1 | Doctors and nurses of an emergency department of a hospital |
|
|
| Isella et al., 2011 [24] | F2F-Ps 5: number and duration of F2F-Ps 5 | RFID technology: exchanging of ultra-low-power radio packets | Active RFID badge 1 | Healthcare personnel, patients, and their caregivers at the pediatric ward of a hospital to study infectious disease transmissions |
|
|
| Olguin D. et al., 2009 [36] | F2F-Ps 5: duration of F2F-Ps 5 | RFID technology: exchanging of power radio packets | Sociometric Badge, worn around the neck 1 | Nurses of a post-anaesthesia care unit (PACU) |
|
|
| Endedijk M. et al., 2018 [38] | Speech activity:
| Microphone | Sociometric Badge, worn around the neck 1 | Master’s students of a ‘Technical Medicine’ Master’s program during simulated medical emergencies |
|
|
| Yu et al., 2016 [35] | Speech activity:
| Microphone | Sociometric Badge, worn around the neck 1 | Simulated procedures of care assistance at an emergency department’s pediatric ward |
|
|
| Stefanini et al., 2020 [39] | Speech activity:
| Microphone | Sociometric Badge, worn around the neck 1 | Surgical team at a university hospital |
| |
| Stefanini et al., 2021 [40] | Speech activity:
| Microphone | Sociometric Badge, worn around the neck 1 | Doctors and nurses of an emergency department of a hospital |
| |
| Olguin D. et al., 2009 [36] | Speech activity:
| Microphone | Sociometric Badge, worn around the neck 1 | Nurses of a post-anaesthesia care unit (PACU) |
|
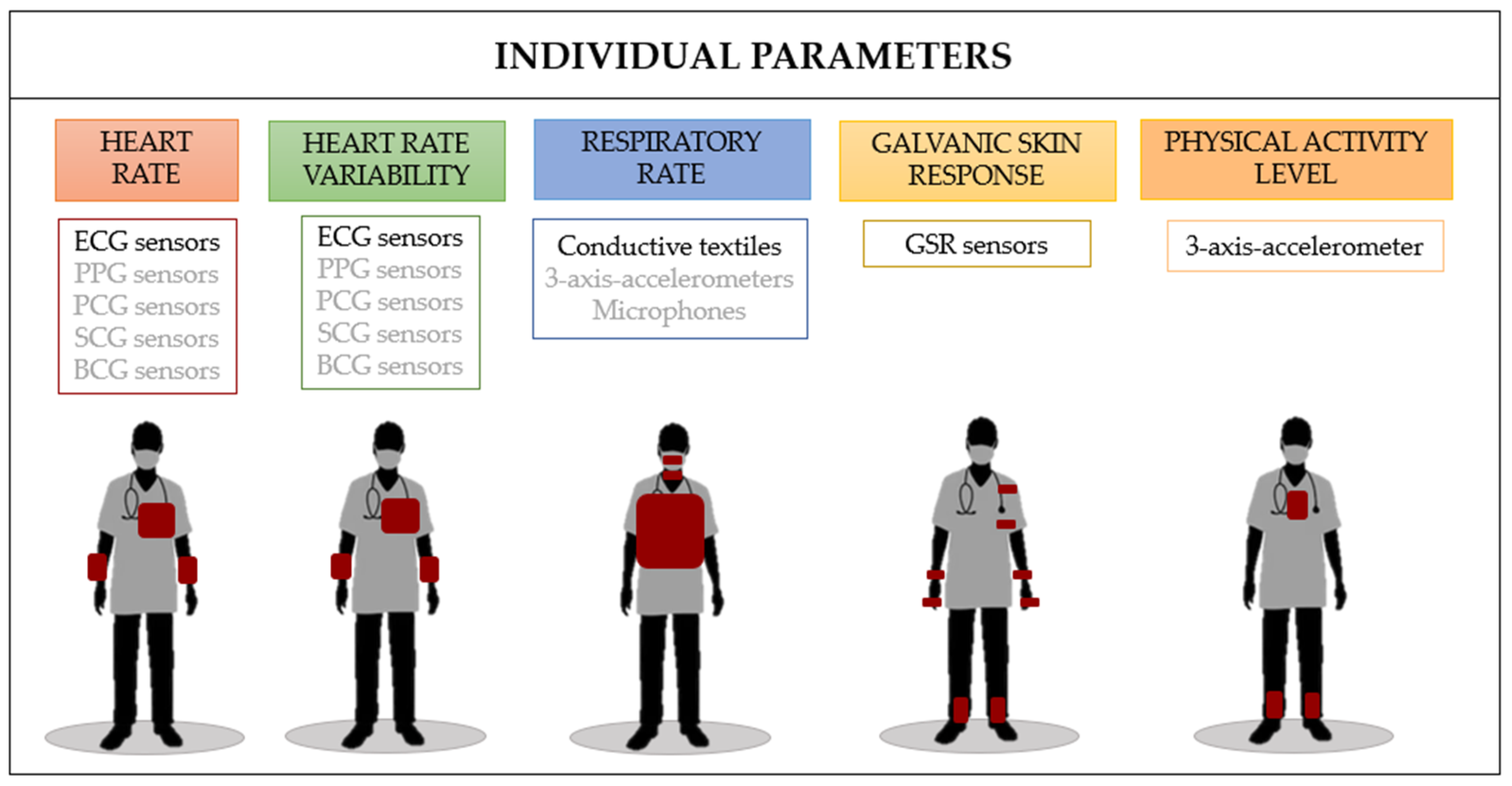
3. Wearables for Monitoring Individual Traits
3.1. Heart Rate
3.2. Heart Rate Variability
3.3. Respiratory Rate
3.4. Galvanic Skin Response
3.5. Physical Activity Level
| Paper | Parameter | Working Principle | Wearable | Scenario | Pros | Cons |
|---|---|---|---|---|---|---|
| Rieger et al. [108] | HR, HRV | 3-channel ECG-recording | The Equivital sensor system EQ-01 (Hidalgo Ltd., Cambridge, UK) 1 | Intraoperative monitoring of 20 surgeons, 6 residents, 5 fellows, 5 attending, and 4 chiefs of medicine to assess surgeons’ stress level |
|
|
| Lo Presti et al. [5] | HR, HRV | Single-lead ECG trace | Zephyr BioHarness (Medtronic, The Netherlands) 4 | Monitoring of an anesthesiologist and a medical trainee during the execution of an epidural procedure on a patient afflicted by chronic back pain |
|
|
| Joseph et al., 2016 [85] | HR, HRV | Single-lead ECG trace | Zephyr BioHarness (Medtronic, The Netherlands) 4 | Monitoring of a trauma team composed of an attending trauma surgeon, a junior trainee, and a senior trainee during trauma activation and emergency surgeries |
|
|
| Lo Presti et al. [109] | HR, HRV | Single-lead ECG trace | Zephyr BioHarness (Medtronic, The Netherlands) 4 | Monitoring of a subject invited to engage in unrestricted upper body motions to replicate common actions performed in OR |
|
|
| Pimentel et al., 2019 [21] | HRV | Single-lead ECG trace | VitalJacket® (Biodevices, Setubal, Portugal S.A) 6 | Monitoring of stress and fatigue among 2 neurosurgeons during intracranial aneurism procedures |
|
|
| Yamada et al. [110] | HR | Photopletismography | Apple Watch Series 8 worn on upper arm | Monitoring of surgeons during robotic-assisted surgery |
|
|
| Lo Presti et al. [5] | RR | Breathing waveform by the chest wall excursions | Zephyr BioHarness (Medtronic, The Netherlands) 4 | Monitoring of an anesthesiologist and a medical trainee during the execution of an epidural procedure on a patient afflicted by chronic back pain |
|
|
| Lo Presti et al. [109] | RR | Breathing waveform by the chest wall excursions | Zephyr BioHarness (Medtronic, The Netherlands) 4 | Monitoring of a subject invited to engage in unrestricted upper body motions to replicate common actions performed in OR |
|
|
| Endedijk et al., 2018 [38] | GSR: SCR signal, N-SCR-Ps 7 and A-SCR-Ps 8 | GSR signal | Empatica E4 9 | Monitoring of Master’s students of the ‘Technical Medicine’ Master’s program during simulated medical emergencies |
|
|
| Phitayakorn et al., 2015 [81] | GSR | GSR signal | GSR device (Manufactured by Neumitra, Inc, Boston, MA, USA) 10 | Monitoring of 17 OR teams, composed by 2 anesthesiology residents, 2 general surgery residents and 2 practicing OR nurses during high-fidelity surgical simulations |
|
|
| Lo Presti et al. [109] | GSR | GSR signal | Shimmer GSR+ sensor (Shimmer sensing, Dublin, Ireland) applying two electrodes on two fingers of the subject | Monitoring of a subject invited to engage in unrestricted upper body motions to replicate common actions performed in OR |
|
|
| Van Houwelingen et al., 2020 [150] | GSR | GSR signal | SenseWear Pro 3 armband | Monitoring of expert and novice surgeons during 21 surgical procedures to study the effect of surgical flow irregularities on their cognitive, emotional, and physiological state |
|
|
| Jacob et al., 2017 [151] | GSR, SCL, SCR | GSR signal | A GSR sensor (Affectiva Q Sensor, Affectiva Inc., Waltham, MA, USA) 11 | Monitoring of 14 general surgery residents during laparoscopic cholecystectomy |
|
|
| Yu et al., 2015 [56] | Physical activity level:
| Three-axis accelerometer | Sociometric badge, worn around the neck | Simulated hand-off scenarios at an emergency care environment |
|
|
| Yu et al., 2016 [35] | Physical activity level:
| Three-axis accelerometer | Sociometric badge, worn around the neck | Simulated patient care scenarios at an emergency department’s pediatric ward |
| • SW 5 |
| Stefanini et al., 2020 [39] | Physical activity level:
| Three-axis accelerometer | Sociometric Badge, worn around the neck | Surgical team of the Breast Unit of an Italian university hospital |
| - |
| Stefanini et al., 2021 [40] | Physical activity level:
| Three-axis accelerometer | Sociometric Badge, worn around the neck | Doctors and nurses of an emergency department of a hospital |
| - |
| Olguin D. et al., 2009 [36] | Physical activity level:
| Three-axis accelerometer | Sociometric Badge, worn around the neck | Nurses of a post-anaesthesia care unit (PACU) |
| - |
| Rosen M. et al., 2018 [37] |
| RFID technology: exchanging of power radio packets | Sociometric wearable badge | Nurses of a surgical intensive care unit (ICU) |
| - |
4. Discussions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woolley, A.W.; Chabris, C.F.; Pentland, A.; Hashmi, N.; Malone, T.W. Evidence for a Collective Intelligence Factor in the Performance of Human Groups. Science 2010, 330, 686–688. [Google Scholar] [CrossRef] [PubMed]
- Woolley, A.W.; Aggarwal, I.; Malone, T.W. Collective Intelligence and Group Performance. Curr. Dir. Psychol. Sci. 2015, 24, 420–424. [Google Scholar] [CrossRef]
- Spearman, C. ‘General Intelligence,’ Objectively Determined and Measured. Am. J. Psychol. 1904, 15, 201–292. [Google Scholar] [CrossRef]
- Manser, T. Teamwork and patient safety in dynamic domains of healthcare: A review of the literature. Acta Anaesthesiol. Scand. 2009, 53, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Presti, D.L.; De Tommasi, F.; Romano, C.; Pulcinelli, M.; Pinnelli, M.; Massaroni, C.; Lanni, B.; Carassiti, M.; Fortino, G.; Schena, E. A quantitative assessment of team members physiological traits and interactions for the development of Collective In-telligence in a clinical scenario. In Proceedings of the 2022 IEEE Intl Conf on Dependable, Autonomic and Secure Computing, Intl Conf on Pervasive Intelligence and Computing, Intl Conf on Cloud and Big Data Computing, Intl Conf on Cyber Science and Technology Congress (DASC/PiCom/CBDCom/CyberSciTech), Falerna, Italy, 12–15 September 2022. [Google Scholar]
- Buljac-Samardzic, M.; Doekhie, K.D.; van Wijngaarden, J.D.H. Interventions to improve team effectiveness within health care: A systematic review of the past decade. Hum. Resour. Health 2020, 18, 2. [Google Scholar] [CrossRef]
- Salas, E.; Klein, C.; King, H.; Salisbury, M.; Augenstein, J.S.; Birnbach, D.J.; Robinson, D.W.; Upshaw, C. Debriefing Medical Teams: 12 Evidence-Based Best Practices and Tips. Jt. Comm. J. Qual. Patient Saf. 2008, 34, 518–527. [Google Scholar] [CrossRef]
- Tan, S.B.; Pena, G.; Altree, M.; Maddern, G.J. Multidisciplinary team simulation for the operating theatre: A review of the literature. ANZ J. Surg. 2014, 84, 515–522. [Google Scholar] [CrossRef]
- Neily, J.; Mills, P.D.; Young-Xu, Y.; Carney, B.T.; West, P.; Berger, D.H.; Mazzia, L.M.; Paull, D.E.; Bagian, J.P. Association between Implementation of a Medical Team Training Program and Surgical Mortality. JAMA 2010, 304, 1693–1700. [Google Scholar] [CrossRef]
- Murphy, M.; Curtis, K.; McCloughen, A. What is the impact of multidisciplinary team simulation training on team performance and efficiency of patient care? An integrative review. Australas. Emerg. Nurs. J. 2016, 19, 44–53. [Google Scholar] [CrossRef]
- Hughes, A.M.; Gregory, M.E.; Joseph, D.L.; Sonesh, S.C.; Marlow, S.L.; Lacerenza, C.N.; Benishek, L.E.; King, H.B.; Salas, E. Saving lives: A meta-analysis of team training in healthcare. J. Appl. Psychol. 2016, 101, 1266–1304. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Attitudes to teamwork and safety among Italian surgeons and operating room nurses. Work 2014, 49, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Flin, R.; Yule, S.; McKenzie, L.; Paterson-Brown, S.; Maran, N. Attitudes to teamwork and safety in the operating theatre. Surgeon 2006, 4, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Undre, S.; Healey, A.N.; Darzi, A.; Vincent, C.A. Observational Assessment of Surgical Teamwork: A Feasibility Study. World J. Surg. 2006, 30, 1774–1783. [Google Scholar] [CrossRef] [PubMed]
- Healey, A.N.; Undre, S.; Sevdalis, N.; Koutantji, M.; Vincent, C.A. The complexity of measuring interprofessional teamwork in the operating theatre. J. Interprof. Care 2006, 20, 485–495. [Google Scholar] [CrossRef]
- Olguín, D.O.; Pentland, A. Sociometric Badges: State of the Art and Future Applications. In Proceedings of the IEEE 11th International Symposium on Wearable Computers, Boston, MA, USA, 11 October 2007. [Google Scholar]
- Olguin, D.O.; Waber, B.N.; Kim, T.; Mohan, A.; Ara, K.; Pentland, A. Sensible Organizations: Technology and Methodology for Automatically Measuring Organizational Behavior. IEEE Trans. Syst. Man Cybern. Part B 2009, 39, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Olguín, D.O.; Pentland, A. Assessing Group Performance from Collective Behavior. In Proceedings of the CSCW Workshop on Collective Intelligence in Organizations, Savannah, GA, USA, 6–10 February 2010. [Google Scholar]
- Kim, T.; McFee, E.; Olguin, D.O.; Waber, B.; Pentland, A. Sociometric badges: Using sensor technology to capture new forms of collaboration. J. Organ. Behav. 2012, 33, 412–427. [Google Scholar] [CrossRef]
- Ito-Masui, A.; Kawamoto, E.; Esumi, R.; Imai, H.; Shimaoka, M. Sociometric wearable devices for studying human behavior in corporate and healthcare workplaces. BioTechniques 2021, 71, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, G.; Rodrigues, S.; Silva, P.A.; Vilarinho, A.; Vaz, R.; Cunha, J.P.S. A wearable approach for intraoperative physiological stress monitoring of multiple cooperative surgeons. Int. J. Med. Inform. 2019, 129, 60–68. [Google Scholar] [CrossRef]
- Hachisu, T.; Pan, Y.; Matsuda, S.; Bourreau, B.; Suzuki, K. FaceLooks: A Smart Headband for Signaling Face-to-Face Behavior. Sensors 2018, 18, 2066. [Google Scholar] [CrossRef]
- Cattuto, C.; Van den Broeck, W.; Barrat, A.; Colizza, V.; Pinton, J.-F.; Vespignani, A. Dynamics of Person-to-Person Interactions from Distributed RFID Sensor Networks. PLoS ONE 2010, 5, e11596. [Google Scholar] [CrossRef]
- Isella, L.; Romano, M.; Barrat, A.; Cattuto, C.; Colizza, V.; Van den Broeck, W.; Gesualdo, F.; Pandolfi, E.; Ravà, L.; Rizzo, C.; et al. Close Encounters in a Pediatric Ward: Measuring Face-to-Face Proximity and Mixing Patterns with Wearable Sensors. PLoS ONE 2011, 6, e17144. [Google Scholar] [CrossRef] [PubMed]
- Presti, D.L.; Bianchi, D.; Massaroni, C.; Gizzi, A.; Schena, E. A Soft and Skin-Interfaced Smart Patch Based on Fiber Optics for Cardiorespiratory Monitoring. Biosensors 2022, 12, 363. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Liu, J. Network-Based Modeling for Characterizing Human Collective Behaviors During Extreme Events. IEEE Trans. Syst. Man Cybern. Syst. 2017, 47, 171–183. [Google Scholar] [CrossRef]
- Presti, D.L.; Massaroni, C.; Leitao, C.S.J.; Domingues, M.D.F.; Sypabekova, M.; Barrera, D.; Floris, I.; Massari, L.; Oddo, C.M.; Sales, S.; et al. Fiber Bragg Gratings for Medical Applications and Future Challenges: A Review. IEEE Access 2020, 8, 156863–156888. [Google Scholar] [CrossRef]
- Undre, S.; London, F. Team Performance in the Operating Theatre. Ph.D. Thesis, University of London, London, UK, 2007. [Google Scholar]
- Olguín, D.O.; Gloor, P.A.; Pentland, A. Capturing Individual and Group Behavior with Wearable Sensors. In Proceedings of the AAAI Spring Symposium—Technical Report, Palo Alto, CA, USA, 23–25 March 2009; Volume SS-09-04, pp. 68–74. [Google Scholar]
- Wu, L.; Waber, B.; Aral, S.; Brynjolfsson, E.; Sandy, A. Pentland Mining Face-to-Face Interaction Networks Using Sociometric Badges: Predicting Productivity in an it Configuration TASK. Available online: http://ssrn.com/abstract=1130251 (accessed on 1 October 2023).
- Dietz, A.S.; Pronovost, P.J.; Mendez-Tellez, P.A.; Wyskiel, R.; Marsteller, J.A.; Thompson, D.A.; Rosen, M.A. A systematic review of teamwork in the intensive care unit: What do we know about teamwork, team tasks, and improvement strategies? J. Crit. Care 2014, 29, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Higo, N.; Ogawa, K.-I.; Minemura, J.; Xu, B.; Nozawa, T.; Ogata, T.; Ara, K.; Yano, K.; Miyake, Y. Interpersonal Similarity between Body Movements in Face-To-Face Communication in Daily Life. PLoS ONE 2014, 9, e102019. [Google Scholar] [CrossRef] [PubMed]
- Ara, K.; Akitomi, T.; Sato, N.; Takahashi, K.; Maeda, H.; Yano, K.; Yanagisawa, M. Integrating Wearable Sensor Technology into Project-management Process. J. Inf. Process. 2012, 20, 406–418. [Google Scholar] [CrossRef]
- Olguín, D.O. Sensor-Based Organizational Design and Engineering. Int. J. Organ. Des. Eng. 2010, 1, 69–97. [Google Scholar]
- Yu, D.; Blocker, R.C.; Sir, M.Y.; Hallbeck, M.S.; Hellmich, T.R.; Cohen, T.; Nestler, D.M.; Pasupathy, K.S. Intelligent Emergency Department: Validation of Sociometers to Study Workload. J. Med. Syst. 2016, 40, 1–12. [Google Scholar] [CrossRef]
- Olguin, D.O.; Gloor, P.A.; Pentland, A. Wearable sensors for pervasive healthcare management. In Proceedings of the 3d International ICST Conference on Pervasive Computing Technologies for Healthcare, London UK, 1–3 April 2009. [Google Scholar]
- Rosen, M.A.; Dietz, A.S.; Lee, N.; Wang, I.-J.; Markowitz, J.; Wyskiel, R.M.; Yang, T.; Priebe, C.E.; Sapirstein, A.; Gurses, A.P.; et al. Sensor-based measurement of critical care nursing workload: Unobtrusive measures of nursing activity complement traditional task and patient level indicators of workload to predict perceived exertion. PLoS ONE 2018, 13, e0204819. [Google Scholar] [CrossRef]
- Endedijk, M.; Hoogeboom, M.; Groenier, M.; de Laat, S.; van Sas, J. Using sensor technology to capture the structure and content of team interactions in medical emergency teams during stressful moments. Frontline Learn. Res. 2018, 6, 123–147. [Google Scholar] [CrossRef]
- Stefanini, A.; Aloini, D.; Gloor, P. Silence is golden: The role of team coordination in health operations. Int. J. Oper. Prod. Manag. 2020, 40, 1421–1447. [Google Scholar] [CrossRef]
- Stefanini, A.; Aloini, D.; Gloor, P.; Pochiero, F. Patient satisfaction in emergency department: Unveiling complex interactions by wearable sensors. J. Bus. Res. 2020, 129, 600–611. [Google Scholar] [CrossRef]
- Kawamoto, E.; Ito-Masui, A.; Esumi, R.; Imai, H.; Shimaoka, M. How ICU Patient Severity Affects Communicative Interactions between Healthcare Professionals: A Study Utilizing Wearable Sociometric Badges. Front. Med. 2020, 7, 606987. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, E.; Ito-Masui, A.; Esumi, R.; Ito, M.; Mizutani, N.; Hayashi, T.; Imai, H.; Shimaoka, M. Social Network Analysis of Intensive Care Unit Health Care Professionals Measured by Wearable Sociometric Badges: Longitudinal Observational Study. J. Med. Internet Res. 2020, 22, e23184. [Google Scholar] [CrossRef] [PubMed]
- Elmer, T.; Chaitanya, K.; Purwar, P.; Stadtfeld, C. The validity of RFID badges measuring face-to-face interactions. Behav. Res. Methods 2019, 51, 2120–2138. [Google Scholar] [CrossRef] [PubMed]
- Pachucki, M.C.; Ozer, E.J.; Barrat, A.; Cattuto, C. Mental health and social networks in early adolescence: A dynamic study of objectively-measured social interaction behaviors. Soc. Sci. Med. 2015, 125, 40–50. [Google Scholar] [CrossRef]
- Hoegl, M.; Proserpio, L. Team member proximity and teamwork in innovative projects. Res. Policy 2004, 33, 1153–1165. [Google Scholar] [CrossRef]
- Martinez-Maldonado, R.; Yacef, K.; Dos Santos, A.D.P.; Shum, S.B.; Echeverria, V.; Santos, O.C.; Pechenizkiy, M. Towards Proximity Tracking and Sensemaking for Supporting Teamwork and Learning. In Proceedings of the 2017 IEEE 17th International Conference on Advanced Learning Technologies (ICALT), Timisoara, Romania, 3–7 July 2017; pp. 89–91. [Google Scholar]
- Pentland, A. Collective intelligence. IEEE Comput. Intell. Mag. 2006, 1, 9–12. [Google Scholar] [CrossRef]
- Chong, D.S.F.; van Eerde, W.; Rutte, C.G.; Chai, K.H. Bringing Employees Closer: The Effect of Proximity on Communication When Teams Function under Time Pressure. J. Prod. Innov. Manag. 2012, 29, 205–215. [Google Scholar] [CrossRef]
- Bian, S.; Zhou, B.; Bello, H.; Lukowicz, P. A wearable magnetic field based proximity sensing system for monitoring COVID-19 social distancing. In Proceedings of the 2020 International Symposium on Wearable Computers, Online, Mexico, 12–16 September 2020; Association for Computing Machinery: New York, NY, USA, 2020; pp. 1–5. [Google Scholar]
- Jeong, S.; Kuk, S.; Kim, H. A Smartphone Magnetometer-Based Diagnostic Test for Automatic Contact Tracing in Infectious Disease Epidemics. IEEE Access 2019, 7, 20734–20747. [Google Scholar] [CrossRef]
- Stopczynski, A.; Sekara, V.; Sapiezynski, P.; Cuttone, A.; Madsen, M.M.; Larsen, J.E.; Lehmann, S. Measuring Large-Scale Social Networks with High Resolution. PLoS ONE 2014, 9, e95978. [Google Scholar] [CrossRef] [PubMed]
- Polastre, J.; Szewczyk, R.; Culler, D. Telos: Enabling ultra-low power wireless research. In Proceedings of the IPSN 2005. Fourth International Symposium on Information Processing in Sensor Networks, Boise, ID, USA, 15 April 2005. [Google Scholar]
- Kiti, M.C.; Tizzoni, M.; Kinyanjui, T.M.; Koech, D.C.; Munywoki, P.K.; Meriac, M.; Cappa, L.; Panisson, A.; Barrat, A.; Cattuto, C.; et al. Quantifying social contacts in a household setting of rural Kenya using wearable proximity sensors. EPJ Data Sci. 2016, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Salathé, M.; Kazandjieva, M.; Lee, J.W.; Levis, P.; Feldman, M.W.; Jones, J.H. A high-resolution human contact network for infectious disease transmission. Proc. Natl. Acad. Sci. USA 2010, 107, 22020–22025. [Google Scholar] [CrossRef] [PubMed]
- Vanhems, P.; Barrat, A.; Cattuto, C.; Pinton, J.-F.; Khanafer, N.; Régis, C.; Kim, B.-A.; Comte, B.; Voirin, N. Estimating Potential Infection Transmission Routes in Hospital Wards Using Wearable Proximity Sensors. PLoS ONE 2013, 8, e73970. [Google Scholar] [CrossRef]
- Yu, D.; Blocker, R.; Hallbeck, S.; Sir, M.; Hellmich, T.; Pasupathy, K. Application of sociometer badges in simulated health environments. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2015, 59, 538–542. [Google Scholar] [CrossRef]
- Ohashi, K.; Ota, S.; Ohno-Machado, L.; Tanaka, H. Comparison of RFID systems for tracking clinical interventions at the bedside. Am. Med. Inform. Assoc. 2008, 2008, 525–529. [Google Scholar]
- Ni, L.M.; Liu, Y.; Lau, Y.C.; Patil, A.P. LANDMARC: Indoor location sensing using active RFID. In Proceedings of the First IEEE International Conference on Pervasive Computing and Communications, Fort Worth, TX, USA, 26 March 2003; pp. 407–415. [Google Scholar]
- Jin, G.-Y.; Lu, X.-Y.; Park, M.-S. An Indoor Localization Mechanism Using Active RFID Tag. In Proceedings of the IEEE International Conference on Sensor Networks, Ubiquitous, and Trustworthy Computing (SUTC’06), Taichung, Taiwan, 5–7 June 2006. [Google Scholar]
- Iqbal, Z.; Luo, D.; Henry, P.; Kazemifar, S.; Rozario, T.; Yan, Y.; Westover, K.; Lu, W.; Nguyen, D.; Long, T.; et al. Accurate real time localization tracking in a clinical environment using Bluetooth Low Energy and deep learning. PLoS ONE 2018, 13, e0205392. [Google Scholar] [CrossRef] [PubMed]
- Madhavapeddy, A.; Tse, A. A Study of Bluetooth Propagation Using Accurate Indoor Location Mapping. In International Conference on Ubiquitous Computing; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Bekkelien, A.; Deriaz, M.; Marchand-Maillet, S. Bluetooth Indoor Positioning. Master’s Thesis, University of Geneva, Geneva, Switzerland, 2012. [Google Scholar]
- Lin, Q.; Son, J. Analysis of Bluetooth RSSI for Proximity Detection of Ship Passengers. Appl. Sci. 2022, 12, 517. [Google Scholar] [CrossRef]
- He, T.; Tan, J.; Zhuo, W.; Printz, M.; Chan, S.-H.G. Tackling Multipath and Biased Training Data for IMU-Assisted BLE Proximity Detection. In Proceedings of the IEEE INFOCOM 2022-IEEE Conference on Computer Communications, London, UK, 2–5 May 2022; pp. 1259–1268. [Google Scholar]
- Obadia, T.; Silhol, R.; Opatowski, L.; Temime, L.; Legrand, J.; Thiébaut, A.C.M.; Herrmann, J.-L.; Fleury, E.; Guillemot, D.; Boëlle, P.-Y.; et al. Detailed Contact Data and the Dissemination of Staphylococcus aureus in Hospitals. PLoS Comput. Biol. 2015, 11, e1004170. [Google Scholar] [CrossRef]
- Zetterholm, M.V.; Nilsson, L.; Jokela, P. Using a Proximity-Detection Technology to Nudge for Physical Distancing in a Swedish Workplace During the COVID-19 Pandemic: Retrospective Case Study. JMIR Form. Res. 2022, 6, e39570. [Google Scholar] [CrossRef] [PubMed]
- Tomprou, M.; Kim, Y.J.; Chikersal, P.; Woolley, A.W.; Dabbish, L.A. Speaking out of turn: How video conferencing reduces vocal synchrony and collective intelligence. PLoS ONE 2021, 16, e0247655. [Google Scholar] [CrossRef] [PubMed]
- Dirks, K.T. Effects of Interpersonal Trust 1 The Effects of Interpersonal Trust on Work Group Performance. J. Appl. Psychol. 1999, 84, 445. [Google Scholar] [CrossRef] [PubMed]
- Lindskold, S. Trust Development, the GRIT Proposal, and the Effects of Conciliatory Acts on Conflict and Cooperation. Psychol. Bull. 1978, 85, 772. [Google Scholar] [CrossRef]
- Kayhan, V.O.; Chen, Z.; French, K.A.; Allen, T.D.; Salomon, K.; Watkins, A. How honest are the signals? A protocol for validating wearable sensors. Behav. Res. Methods 2018, 50, 57–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Seong, J.J.; Ozlu, B.; Shim, B.S.; Marakhimov, A.; Lee, S. Biosignal Sensors and Deep Learning-Based Speech Recognition: A Review. Sensors 2021, 21, 1399. [Google Scholar] [CrossRef] [PubMed]
- Pentland, A. On the Collective Nature of Human Intelligence. Adapt. Behav. 2007, 15, 189–198. [Google Scholar] [CrossRef]
- Fiscella, K.; Meldrum, S.; Franks, P.; Shields, C.G.; Duberstein, P.; McDaniel, S.H.; Epstein, R.M. Patient Trust Is It Related to Patient-Centered Behavior of Primary Care Physicians? Med. Care 2004, 42, 1049–1055. [Google Scholar] [CrossRef]
- Gleichgerrcht, E.; Decety, J. Empathy in Clinical Practice: How Individual Dispositions, Gender, and Experience Moderate Empathic Concern, Burnout, and Emotional Distress in Physicians. PLoS ONE 2013, 8, e61526. [Google Scholar] [CrossRef]
- Rouse, W.; Cannon-Bowers, J.; Salas, E. The role of mental models in team performance in complex systems. IEEE Trans. Syst. Man Cybern. 1992, 22, 1296–1308. [Google Scholar] [CrossRef]
- LeBlanc, V.R.; Tabak, D.; Kneebone, R.; Nestel, D.; MacRae, H.; Moulton, C.-A. Psychometric properties of an integrated assessment of technical and communication skills. Am. J. Surg. 2009, 197, 96–101. [Google Scholar] [CrossRef]
- Chrouser, K.L.; Xu, J.; Hallbeck, S.; Weinger, M.B.; Partin, M.R. The influence of stress responses on surgical performance and outcomes: Literature review and the development of the surgical stress effects (SSE) framework. Am. J. Surg. 2018, 216, 573–584. [Google Scholar] [CrossRef]
- Wheelock, A.M.; Suliman, A.M.; Wharton, R.B.; Babu, E.D.F.; Hull, L.; Vincent, C.; Sevdalis, N.; Arora, S. The Impact of Operating Room Distractions on Stress, Workload, and Teamwork. Ann. Surg. 2015, 261, 1079–1084. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Hull, L.; Sevdalis, N.; Tierney, T.; Nestel, D.; Woloshynowych, M.; Darzi, A.; Kneebone, R. Factors compromising safety in surgery: Stressful events in the operating room. Am. J. Surg. 2010, 199, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, K.; Larentzakis, A.; Papavassiliou, A.G. Surgeons’ and surgical trainees’ acute stress in real operations or simulation: A systematic review. Surgeon 2017, 15, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Phitayakorn, R.; Minehart, R.; Pian-Smith, M.; Hemingway, M.; Petrusa, E. Practicality of using galvanic skin response to measure intraoperative physiologic autonomic activation in operating room team members. Surgery 2015, 158, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Phitayakorn, R.; Minehart, R.D.; Hemingway, M.W.; Pian-Smith, M.C.; Petrusa, E. Relationship between physiologic and psychological measures of autonomic activation in operating room teams during a simulated airway emergency. Am. J. Surg. 2015, 209, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, I.; Tsiamyrtzis, P.; Shastri, D.; Wesley, A.; Zhou, Y.; Lindner, P.; Buddharaju, P.; Joseph, R.; Mandapati, A.; Dunkin, B.; et al. Fast by Nature-How Stress Patterns Define Human Experience and Performance in Dexterous Tasks. Sci. Rep. 2012, 2, 305. [Google Scholar] [CrossRef]
- Sanchez-Comas, A.; Synnes, K.; Molina-Estren, D.; Troncoso-Palacio, A.; Comas-González, Z. Correlation Analysis of Different Measurement Places of Galvanic Skin Response in Test Groups Facing Pleasant and Unpleasant Stimuli. Sensors 2021, 21, 4210. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Parvaneh, S.; Swartz, T.; Haider, A.A.; Hassan, A.; Kulvatunyou, N.; Tang, A.; Latifi, R.; Najafi, B.; Rhee, P. Stress among surgical attending physicians and trainees. J. Trauma Inj. Infect. Crit. Care 2016, 81, 723–728. [Google Scholar] [CrossRef]
- Rai, D.; Thakkar, H.K.; Rajput, S.S.; Santamaria, J.; Bhatt, C.; Roca, F. A Comprehensive Review on Seismocardiogram: Current Advancements on Acquisition, Annotation, and Applications. Mathematics 2021, 9, 2243. [Google Scholar] [CrossRef]
- Lukkarinen, S. Phonocardiography: Development of a Clinical System and Its Application to Screening for Paediatric Heart Murmurs. Available online: http://lib.tkk.fi/Diss/2012/isbn9789526045511/isbn9789526045511.pdf (accessed on 1 October 2023).
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed]
- Hogewind, F.; Zwaaredemaker, H.; Huygens Institute-Royal Netherlands Academy of Arts and Sciences (KNAW). On Spray-Electricity and Waterfall-Electricity. Huygens Inst. R. Neth. Acad. Arts Sci. Proc. 1919, 1919–1920, 429–437. [Google Scholar]
- Inan, O.T.; Migeotte, P.-F.; Park, K.-S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [PubMed]
- Starr, I.; Rawson, A.J.; Schroeder, H.A.; Joseph, N.R. Studies on the estimation of cardiac ouptut in man, and of abnormalities in cardiac function, from the heart’s recoil and the blood’s impacts; the ballistocardiogram. Am. J. Physiol.-Leg. Content 1939, 127, 1–28. [Google Scholar] [CrossRef]
- Choudhary, T.; Sharma, L.N.; Bhuyan, M.K. Automatic Detection of Aortic Valve Opening Using Seismocardiography in Healthy Individuals. IEEE J. Biomed. Health Inform. 2019, 23, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Bour, J.; Kellett, J. Impedance cardiography—A rapid and cost-effective screening tool for cardiac disease. Eur. J. Intern. Med. 2008, 19, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Tadi, M.J.; Lehtonen, E.; Pankaala, M.; Saraste, A.; Vasankari, T.; Teras, M.; Koivisto, T. Gyrocardiography: A new non-invasive approach in the study of mechanical motions of the heart. Concept, method and initial observations. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016. [Google Scholar] [CrossRef]
- Iliev, I.T.; Jekova, I.I.; Tabakov, S.D.; Koshtikova, K.G.; Iovev, S.T. Telemetry of Hospitalized High-Risk Patients with Cardiovascular Diseases. In Proceedings of the 2019 IEEE XXVIII International Scientific Conference Electronics (ET), Sozopol, Bulgaria, 12–14 September 2019; pp. 1–4. [Google Scholar]
- Iliev, I.; Jekova, I.; Tabakov, S.; Koshtikova, K.; Runev, N.; Manov, E. High-Risk Cardiac Patients’ Follow-Up via Portable Telemonitoring Personal Analyzer: Applicability, Reliability and Accuracy. In Proceedings of the International Symposium on Bioinformatics and Biomedicine, Burgas, Bulgaria, 8–10 October 2023; Springer: Cham, Switzerland, 2022; pp. 312–321. [Google Scholar] [CrossRef]
- Soroudi, A.; Hernández, N.; Berglin, L.; Nierstrasz, V. Electrode placement in electrocardiography smart garments: A review. J. Electrocardiol. 2019, 57, 27–30. [Google Scholar] [CrossRef]
- López, G.; Custodio, V.; I Moreno, J. LOBIN: E-Textile and Wireless-Sensor-Network-Based Platform for Healthcare Monitoring in Future Hospital Environments. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1446–1458. [Google Scholar] [CrossRef]
- Yoo, J.; Yan, L.; Lee, S.; Kim, H.; Yoo, H.-J. A Wearable ECG Acquisition System with Compact Planar-Fashionable Circuit Board-Based Shirt. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 897–902. [Google Scholar] [CrossRef]
- Pollonini, L.; Rajan, N.O.; Xu, S.; Madala, S.; Dacso, C.C. A Novel Handheld Device for Use in Remote Patient Monitoring of Heart Failure Patients—Design and Preliminary Validation on Healthy Subjects. J. Med. Syst. 2012, 36, 653–659. [Google Scholar] [CrossRef]
- Han, X.; Wu, X.; Wang, J.; Li, H.; Cao, K.; Cao, H.; Zhong, K.; Yang, X. The Latest Progress and Development Trend in the Research of Ballistocardiography (BCG) and Seismocardiogram (SCG) in the Field of Health Care. Appl. Sci. 2021, 11, 8896. [Google Scholar] [CrossRef]
- Taebi, A.; Solar, B.E.; Bomar, A.J.; Sandler, R.H.; Mansy, H.A. Recent Advances in Seismocardiography. Vibration 2019, 2, 64–86. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Meriggi, P.; Rizzo, F.; Vaini, E.; Faini, A.; Merati, G.; Parati, G.; Castiglioni, P. A wearable system for the seismocardiogram assessment in daily life conditions. In Proceedings of the 2011 33rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4263–4266. [Google Scholar] [CrossRef]
- Etemadi, M.; Inan, O.T.; Heller, J.A.; Hersek, S.; Klein, L.; Roy, S. A Wearable Patch to Enable Long-Term Monitoring of Environmental, Activity and Hemodynamics Variables. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Santucci, F.; Presti, D.L.; Massaroni, C.; Schena, E.; Setola, R. Precordial Vibrations: A Review of Wearable Systems, Signal Processing Techniques, and Main Applications. Sensors 2022, 22, 5805. [Google Scholar] [CrossRef] [PubMed]
- Giovangrandi, L.; Inan, O.T.; Wiard, R.M.; Etemadi, M.; Kovacs, G.T. Ballistocardiography—A Method Worth Revisiting. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar] [CrossRef]
- Castiglioni, P.; Meriggi, P.; Rizzo, F.; Vaini, E.; Faini, A.; Parati, G.; Merati, G.; Di Rienzo, M. Cardiac Sounds from a Wearable Device for Sternal Seismocardiography. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar] [CrossRef]
- Rieger, A.; Stoll, R.; Kreuzfeld, S.; Behrens, K.; Weippert, M. Heart rate and heart rate variability as indirect markers of surgeons’ intraoperative stress. Int. Arch. Occup. Environ. Health 2014, 87, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Presti, D.L.; Gravina, R.; Massaroni, C.; Formica, D.; Schena, E.; Fortino, G. A Multisensory Platform for Maximizing Collective Intelligence in the Operating Room. In Proceedings of the 2021 IEEE/ACM Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 16–17 December 2021; pp. 174–178. [Google Scholar] [CrossRef]
- Yamada, K.; Enokida, Y.; Kato, R.; Imaizumi, J.; Takada, T.; Ojima, H. The Feasibility and Reliability of Upper Arm–Worn Apple Watch Heart Rate Monitoring for Surgeons During Surgery: Observational Study. JMIR Hum. Factors 2023, 10, e50891. [Google Scholar] [CrossRef]
- Natalicio, D.S. Development of The Spanish Edition of The State-Trait Anxiety Inventory. Interam. J. Psychol. 1971, 5, 145–158. [Google Scholar]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Preejith, S.P.; Dhinesh, R.; Joseph, J.; Sivaprakasam, M. Wearable ECG platform for continuous cardiac monitoring. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016. [Google Scholar] [CrossRef]
- Yuan, G.; Drost, N.A.; McIvor, R.A. Respiratory rate and breathing pattern. McMaster Univ. Med. J. 2013, 10, 23–25. [Google Scholar]
- Al-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration rate monitoring methods: A review. Pediatr. Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory Rate: The Neglected Vital Sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Yuen, T.C.B.; Park, S.Y.; Meltzer, D.O.; Hall, J.B.; Edelson, D.P. Derivation of a cardiac arrest prediction model using ward vital signs*. Crit. Care Med. 2012, 40, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Nicolò, A.; Bazzucchi, I.; Haxhi, J.; Felici, F.; Sacchetti, M. Comparing Continuous and Intermittent Exercise: An “Isoeffort” and “Isotime” Approach. PLoS ONE 2014, 9, e94990. [Google Scholar] [CrossRef] [PubMed]
- Homma, I.; Masaoka, Y. Breathing rhythms and emotions. Exp. Physiol. 2008, 93, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Gorman, J.M.; Kent, J.; Martinez, J.; Browne, S.; Coplan, J.; Papp, L.A. Physiological Changes During Carbon Dioxide Inhalation in Patients with Panic Disorder, Major Depression, and Premenstrual Dysphoric Disorder Evidence for a Central Fear Mechanism. Arch. Gen. Psychiatry 2001, 58, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.L.; Khuvis, S.; Yeagle, E.; Cerf, M.; Mehta, A.D. Breathing above the brain stem: Volitional control and attentional modulation in humans. J. Neurophysiol. 2018, 119, 145–159. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Ley, M.; Hanke, S. Emotion Recognition from Physiological Signal Analysis: A Review. Electron. Notes Theor. Comput. Sci. 2019, 343, 35–55. [Google Scholar] [CrossRef]
- Dzedzickis, A.; Kaklauskas, A.; Bucinskas, V. Human Emotion Recognition: Review of Sensors and Methods. Sensors 2020, 20, 592. [Google Scholar] [CrossRef]
- Nicolò, A.; Massaroni, C.; Schena, E.; Sacchetti, M. The Importance of Respiratory Rate Monitoring: From Healthcare to Sport and Exercise. Sensors 2020, 20, 6396. [Google Scholar] [CrossRef]
- Massaroni, C.; Nicolò, A.; Presti, D.L.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-Based Methods for Measuring Respiratory Rate. Sensors 2019, 19, 908. [Google Scholar] [CrossRef] [PubMed]
- Presti, D.L.; Carnevale, A.; D’abbraccio, J.; Massari, L.; Massaroni, C.; Sabbadini, R.; Zaltieri, M.; Di Tocco, J.; Bravi, M.; Miccinilli, S.; et al. A Multi-Parametric Wearable System to Monitor Neck Movements and Respiratory Frequency of Computer Workers. Sensors 2020, 20, 536. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Liu, T.; Li, G.; Li, T.; Inoue, Y. Wearable Sensor Systems for Infants. Sensors 2015, 15, 3721–3749. [Google Scholar] [CrossRef] [PubMed]
- Folke, M.; Cernerud, L.; Ekström, M.; Hök, B. Critical review of non-invasive respiratory monitoring in medical care. Med. Biol. Eng. Comput. 2003, 41, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Storck, K.; Karlsson, M.; Ask, P.; Loyd, D. Heat transfer evaluation of the nasal thermistor technique. IEEE Trans. Biomed. Eng. 1996, 43, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Lee-Chiong, T. Sleep: A Comprehensive Handbook; John Wiley and Sons: Hoboken, NJ, USA, 2005; ISBN 047168371X. [Google Scholar]
- Chuo, Y.; Kaminska, B. Sensor Layer of a Multiparameter Single-Point Integrated System. IEEE Trans. Biomed. Circuits Syst. 2009, 3, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A. Clinical Validation of the ECG-Derived Respiration (EDR) Technique Fractal Physiology View Project Non-Linear Dynamics of Blood Pressure View project. Available online: https://www.researchgate.net/publication/245671704 (accessed on 1 October 2023).
- Mazzanti, B.; Lamberti, C.; De Bie, J. Validation of an ECG-derived respiration monitoring method. In Proceedings of the Computers in Cardiology, Thessaloniki Chalkidiki, Greece, 21–24 September 2003. [Google Scholar]
- Khanam, F.-T.-Z.; Al-Naji, A.; Chahl, J. Remote Monitoring of Vital Signs in Diverse Non-Clinical and Clinical Scenarios Using Computer Vision Systems: A Review. Appl. Sci. 2019, 9, 4474. [Google Scholar] [CrossRef]
- Wei, B.; He, X.; Zhang, C.; Wu, X. Non-contact, synchronous dynamic measurement of respiratory rate and heart rate based on dual sensitive regions. Biomed. Eng. Online 2017, 16, 17. [Google Scholar] [CrossRef]
- Janssen, R.J.M.; Wang, W.; Janssen, R.; Wang, W.; Moço, A.; De Haan, G.-A. Video-based Respiration Monitoring with Automatic Region of Interest Detection. Physiol. Meas. 2015, 37, 100. [Google Scholar] [CrossRef]
- Nazari, G.; Bobos, P.; MacDermid, J.C.; Sinden, K.E.; Richardson, J.; Tang, A. Psychometric properties of the Zephyr bioharness device: A systematic review. BMC Sports Sci. Med. Rehabil. 2018, 10, 6. [Google Scholar] [CrossRef]
- Nepi, D.; Sbrollini, A.; Agostinelli, A.; Maranesi, E.; Di Nardo, F.; Fioretti, S.; Pierleoni, P.; Pernini, L.; Valenti, S.; Burattini, L. Validation of the Heart: Rate Signal Provided by the Zephyr BioHarness 3.0. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016. [Google Scholar]
- Tarvainen, M.; Koistinen, A.; Valkonen-Korhonen, M.; Partanen, J.; Karjalainen, P. Analysis of galvanic skin responses with principal components and clustering techniques. IEEE Trans. Biomed. Eng. 2001, 48, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Ayata, D.; Yaslan, Y.; Kamasak, M. Emotion Recognition via Galvanic Skin Response: Comparison of Machine Learning Algorithms and Feature Extraction Methods. IU-J. Electr. Electron. Eng. 2017, 17, 3147–3156. [Google Scholar]
- Setyohadi, D.B.; Kusrohmaniah, S.; Gunawan, S.B.; Pranowo, P. Galvanic skin response data classification for emotion detection. Int. J. Electr. Comput. Eng. IJECE 2018, 8, 31–41. [Google Scholar] [CrossRef]
- Tarvainen, M.; Karjalainen, P.; Koistinen, A.; Valkonen-Korhonen, M. Principal component analysis of galvanic skin responses. In Proceedings of the 22nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 23–28 July 2000; pp. 3011–3014. [Google Scholar] [CrossRef]
- Topoglu, Y.; Watson, J.; Suri, R.; Ayaz, H. Electrodermal Activity in Ambulatory Settings: A Narrative Review of Literature. In Advances in Intelligent Systems and Computing; Springer: Cham, Switzerland, 2019; pp. 91–102. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Florian, J.P.; Orjuela-Cañón, A.D.; Chon, K.H. Electrodermal Activity Is Sensitive to Cognitive Stress under Water. Front. Physiol. 2018, 8, 1128. [Google Scholar] [CrossRef] [PubMed]
- Posada-Quintero, H.F.; Florian, J.P.; Orjuela-Cañón, A.D.; Aljama-Corrales, T.; Charleston-Villalobos, S.; Chon, K.H. Power Spectral Density Analysis of Electrodermal Activity for Sympathetic Function Assessment. Ann. Biomed. Eng. 2016, 44, 3124–3135. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, T.; Takagi, K. Two Components Involved in Galvanic Skin Response. Jpn. J. Physiol. 1958, 8, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, A.; Nivedha, R.; Vani, C. Galvanic Skin Response Measurement and Analysis. Int. J. Appl. Eng. Res. 2015, 10, 12447–12452. [Google Scholar]
- Villarejo, M.V.; Zapirain, B.G.; Zorrilla, A.M. A Stress Sensor Based on Galvanic Skin Response (GSR) Controlled by ZigBee. Sensors 2012, 12, 6075–6101. [Google Scholar] [CrossRef]
- van Houwelingen, B.C.G.; Rutkowski, A.-F.; Ganni, S.; Stepaniak, P.S.; Jakimowicz, J.J. Effects of surgical flow disruptions on surgeons’ resources: A pilot study. Surg. Endosc. 2020, 34, 4525–4535. [Google Scholar] [CrossRef]
- Quick, J.A.; Bukoski, A.D.; Doty, J.; Bennett, B.J.; Crane, M.; Barnes, S.L. Objective measurement of clini-cal competency in surgical education using electrodermal activity. J. Surg. Educ. 2017, 74, 674–680. [Google Scholar] [CrossRef]
- Sun, F.; Zang, W.; Gravina, R.; Fortino, G.; Li, Y. Gait-based identification for elderly users in wearable healthcare systems. Inf. Fusion 2020, 53, 134–144. [Google Scholar] [CrossRef]
- Yang, C.-C.; Hsu, Y.-L.; Yang, C.-C.; Hsu, Y.-L. A Review of Accelerometry-Based Wearable Motion Detectors for Physical Activity Monitoring. Sensors 2010, 10, 7772–7788. [Google Scholar] [CrossRef]
- Green, B. Testing and Quantifying Collective Intelligence. In Proceedings of the Collective Intelligence Conference, Santa Clara, CA, USA, 31 May–2 June 2015. [Google Scholar]
- Riedl, C.; Kim, Y.J.; Gupta, P.; Malone, T.W.; Woolley, A.W. Quantifying collective intelligence in human groups. Proc. Natl. Acad. Sci. USA 2021, 118, e2005737118. [Google Scholar] [CrossRef]
- Pace, P.; Aloi, G.; Gravina, R.; Caliciuri, G.; Fortino, G.; Liotta, A. An Edge-Based Architecture to Support Efficient Applications for Healthcare Industry 4.0. IEEE Trans. Ind. Inform. 2018, 15, 481–489. [Google Scholar] [CrossRef]
- Fortino, G.; Galzarano, S.; Gravina, R.; Li, W. A framework for collaborative computing and multi-sensor data fusion in body sensor networks. Inf. Fusion 2015, 22, 50–70. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulcinelli, M.; Pinnelli, M.; Massaroni, C.; Lo Presti, D.; Fortino, G.; Schena, E. Wearable Systems for Unveiling Collective Intelligence in Clinical Settings. Sensors 2023, 23, 9777. https://doi.org/10.3390/s23249777
Pulcinelli M, Pinnelli M, Massaroni C, Lo Presti D, Fortino G, Schena E. Wearable Systems for Unveiling Collective Intelligence in Clinical Settings. Sensors. 2023; 23(24):9777. https://doi.org/10.3390/s23249777
Chicago/Turabian StylePulcinelli, Martina, Mariangela Pinnelli, Carlo Massaroni, Daniela Lo Presti, Giancarlo Fortino, and Emiliano Schena. 2023. "Wearable Systems for Unveiling Collective Intelligence in Clinical Settings" Sensors 23, no. 24: 9777. https://doi.org/10.3390/s23249777
APA StylePulcinelli, M., Pinnelli, M., Massaroni, C., Lo Presti, D., Fortino, G., & Schena, E. (2023). Wearable Systems for Unveiling Collective Intelligence in Clinical Settings. Sensors, 23(24), 9777. https://doi.org/10.3390/s23249777