

A PVDF Receiver for Acoustic Monitoring of Microbubble-Mediated Ultrasound Brain Therapy



Abstract
:1. Introduction
2. Materials and Methods
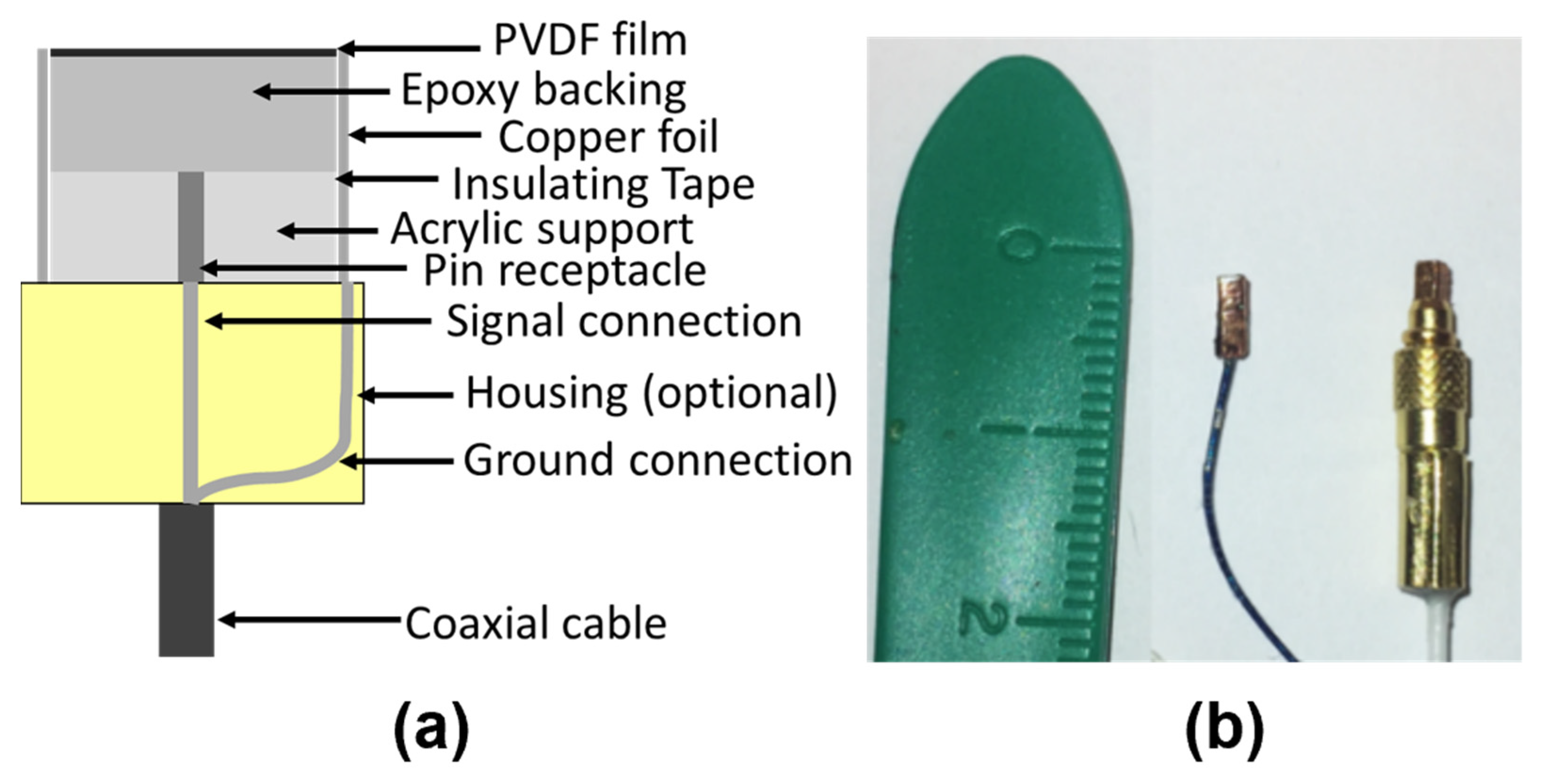
2.1. Receiver Assembly
2.2. Preamplifier Design
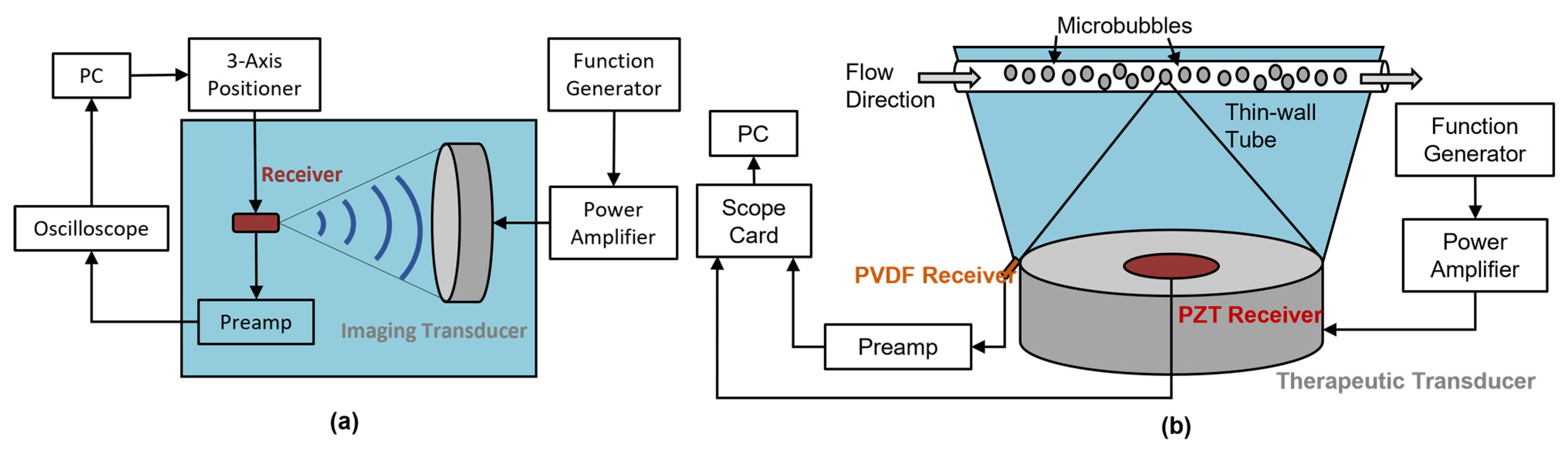
2.3. Sensitivity Characterization
2.4. Lower Dynamic Limit
2.5. Directivity Characterization
2.6. Benchtop Bubble Monitoring
3. Results
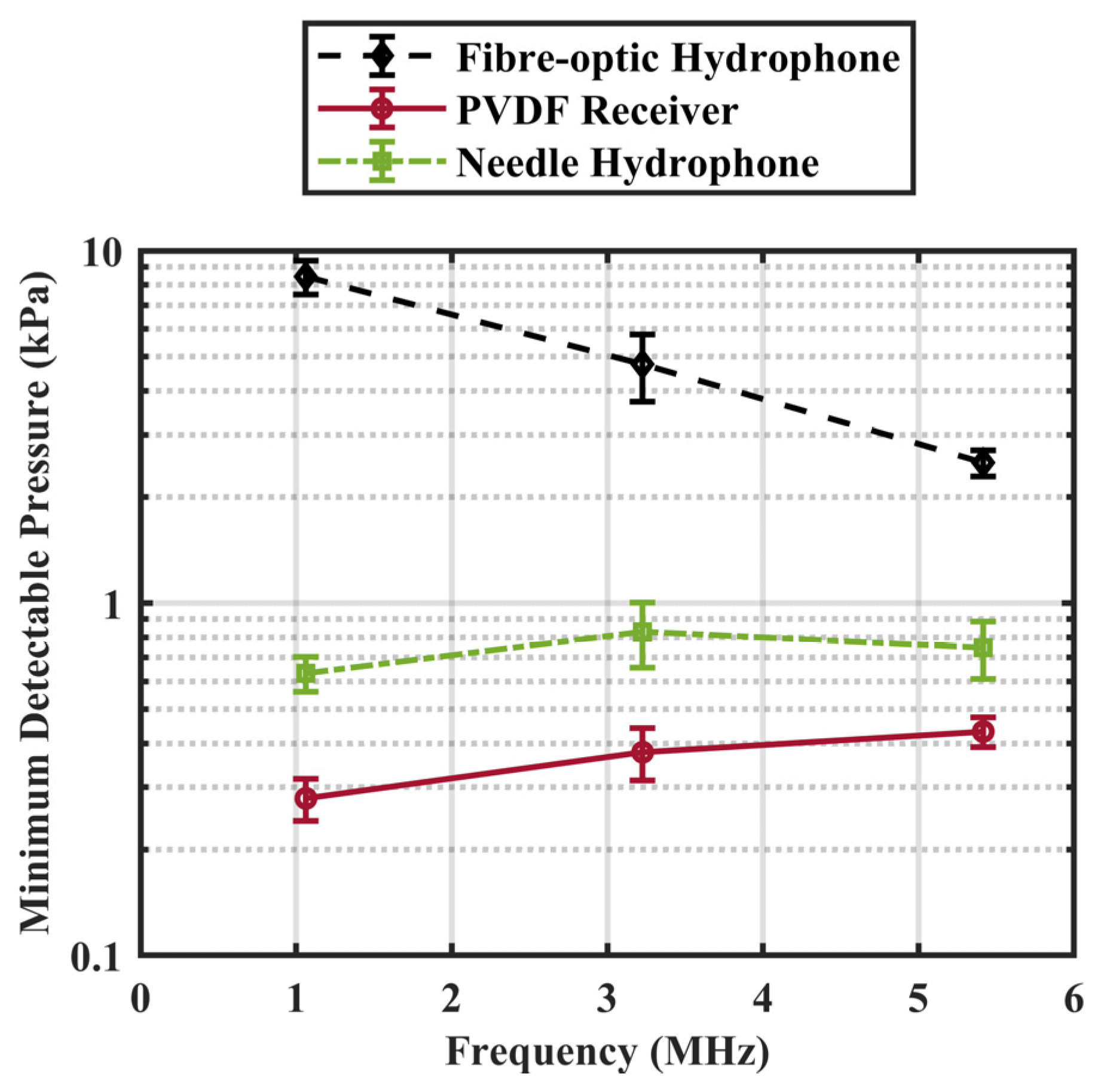
3.1. Comparison of PVDF Receiver and Commercial Hydrophones
3.2. Validation on Benchtop Bubble Monitoring
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sheikov, N.; McDannold, N.; Vykhodtseva, N.; Jolesz, F.; Hynynen, K. Cellular mechanisms of the blood-brain barrier opening induced by ultrasound in presence of microbubbles. Ultrasound Med. Biol. 2004, 30, 979–989. [Google Scholar] [CrossRef]
- Kinoshita, M.; McDannold, N.; Jolesz, F.A.; Hynynen, K. Noninvasive localized delivery of Herceptin to the mouse brain by MRI-guided focused ultrasound-induced blood–brain barrier disruption. Proc. Natl. Acad. Sci. USA 2006, 103, 11719–11723. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.-H.; Lin, Y.-T.; Chung, Y.-H.; Lin, K.-J.; Yang, L.-Y.; Yen, T.-C.; Liu, H.-L. Focused Ultrasound-Induced Blood-Brain Barrier Opening Enhances GSK-3 Inhibitor Delivery for Amyloid-Beta Plaque Reduction. Sci. Rep. 2018, 8, 12882. [Google Scholar] [CrossRef] [PubMed]
- Thévenot, E.; Jordão, J.F.; O’Reilly, M.A.; Markham, K.; Weng, Y.-Q.; Foust, K.D.; Kaspar, B.K.; Hynynen, K.; Aubert, I. Targeted Delivery of Self-Complementary Adeno-Associated Virus Serotype 9 to the Brain, Using Magnetic Resonance Imaging-Guided Focused Ultrasound. Hum. Gene Ther. 2012, 23, 1144–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, R.J.; McVeigh, P.Z.; O’Reilly, M.A.; Burrell, K.; Bebenek, M.; Smith, C.; Etame, A.B.; Zadeh, G.; Hynynen, K.; Wilson, B.C.; et al. Focused ultrasound delivery of Raman nanoparticles across the blood-brain barrier: Potential for targeting experimental brain tumors. Nanomed. Nanotechnol. Biol. Med. 2014, 10, e1075–e1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treat, L.H.; McDannold, N.; Zhang, Y.; Vykhodtseva, N.; Hynynen, K. Improved Anti-Tumor Effect of Liposomal Doxorubicin After Targeted Blood-Brain Barrier Disruption by MRI-Guided Focused Ultrasound in Rat Glioma. Ultrasound Med. Biol. 2012, 38, 1716–1725. [Google Scholar] [CrossRef] [Green Version]
- Burgess, A.; Huang, Y.; Querbes, W.; Sah, D.W.; Hynynen, K. Focused ultrasound for targeted delivery of siRNA and efficient knockdown of Htt expression. J. Control. Release 2012, 163, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Alkins, R.; Burgess, A.; Ganguly, M.; Francia, G.; Kerbel, R.; Wels, W.S.; Hynynen, K. Focused Ultrasound Delivers Targeted Immune Cells to Metastatic Brain Tumors. Cancer Res. 2013, 73, 1892–1899. [Google Scholar] [CrossRef] [Green Version]
- Carpentier, A.; Canney, M.; Vignot, A.; Reina, V.; Beccaria, K.; Horodyckid, C.; Karachi, C.; Leclercq, D.; Lafon, C.; Chapelon, J.-Y.; et al. Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci. Transl. Med. 2016, 8, 343re2. [Google Scholar] [CrossRef]
- Lipsman, N.; Meng, Y.; Bethune, A.J.; Huang, Y.; Lam, B.; Masellis, M.; Herrmann, N.; Heyn, C.; Aubert, I.; Boutet, A.; et al. Blood–brain barrier opening in Alzheimer’s disease using MR-guided focused ultrasound. Nat. Commun. 2018, 9, 2336. [Google Scholar] [CrossRef]
- Mainprize, T.; Lipsman, N.; Huang, Y.; Meng, Y.; Bethune, A.; Ironside, S.; Heyn, C.; Alkins, R.; Trudeau, M.; Sahgal, A.; et al. Blood-Brain Barrier Opening in Primary Brain Tumors with Non-invasive MR-Guided Focused Ultrasound: A Clinical Safety and Feasibility Study. Sci. Rep. 2019, 9, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konofagou, E. Non-invasive Blood-brain Barrier Opening in Alzheimer’s Disease Patients Using Focused Ultrasound Clinical Trial Identifier: NCT04118764. Available online: https://clinicaltrials.gov/ct2/show/NCT04118764 (accessed on 22 October 2022).
- Chen, K.T.; Chai, W.Y.; Lin, Y.J.; Lin, C.J.; Chen, P.Y.; Tsai, H.C.; Huang, C.Y.; Kuo, J.S.; Liu, H.L.; Wei, K.C. Neuronavigation-guided focused ultrasound for transcranial blood-brain barrier opening and im-munostimulation in brain tumors. Sci. Adv. 2021, 7, eabd0772. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.A.; Hough, O.; Hynynen, K. Blood-Brain Barrier Closure Time After Controlled Ultrasound-Induced Opening Is Independent of Opening Volume. J. Ultrasound Med. 2017, 36, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, T.; Zhang, Y.; Power, C.; Alexander, P.M.; Sutton, J.T.; Aryal, M.; Vykhodtseva, N.; Miller, E.L.; McDannold, N.J. Closed-loop control of targeted ultrasound drug delivery across the blood–brain/tumor barriers in a rat glioma model. Proc. Natl. Acad. Sci. USA 2017, 114, E10281–E10290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hynynen, K.; McDannold, N.; Martin, H.; Jolesz, F.A.; Vykhodtseva, N. The threshold for brain damage in rabbits induced by bursts of ultrasound in the presence of an ultrasound contrast agent (Optison®). Ultrasound Med. Biol. 2003, 29, 473–481. [Google Scholar] [CrossRef]
- Goldberg, B.B.; Liu, J.-B.; Forsberg, F. Ultrasound contrast agents: A review. Ultrasound Med. Biol. 1994, 20, 319–333. [Google Scholar] [CrossRef]
- Neppiras, E. Acoustic cavitation. Phys. Rep. 1980, 61, 159–251. [Google Scholar] [CrossRef]
- Emmer, M.; Borsboom, J.; van Wamel, A.; Versluis, M.; de Jong, N. Optical Investigation of Ultrasound Induced Encapsu-lated Microbubble. IEEE Int. Ultrason. Symp. 2005, 2, 981–984. [Google Scholar]
- O’Reilly, M.A.; Hynynen, K. A PVDF Receiver for Ultrasound Monitoring of Transcranial Focused Ultrasound Therapy. IEEE Trans. Biomed. Eng. 2010, 57, 2286–2294. [Google Scholar] [CrossRef] [Green Version]
- McDannold, N.; Vykhodtseva, N.; Raymond, S.; Jolesz, F.A.; Hynynen, K. MRI-guided targeted blood-brain barrier disruption with focused ultrasound: Histological findings in rabbits. Ultrasound Med. Biol. 2005, 31, 1527–1537. [Google Scholar] [CrossRef]
- McDannold, N.; Arvanitis, C.D.; Vykhodtseva, N.; Livingstone, M.S. Temporary Disruption of the Blood–Brain Barrier by Use of Ultrasound and Microbubbles: Safety and Efficacy Evaluation in Rhesus Macaques. Cancer Res. 2012, 72, 3652–3663. [Google Scholar] [CrossRef] [PubMed]
- McDannold, N.; Vykhodtseva, N.; Hynynen, K. Targeted disruption of the blood–brain barrier with focused ultrasound: Association with cavitation activity. Phys. Med. Biol. 2006, 51, 793–807. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, C.D.; Livingstone, M.S.; Vykhodtseva, N.; McDannold, N. Controlled Ultrasound-Induced Blood-Brain Barrier Disruption Using Passive Acoustic Emissions Monitoring. PLoS ONE 2012, 7, e45783. [Google Scholar] [CrossRef]
- Sun, T.; Samiotaki, G.; Wang, S.; Acosta, C.; Chen, C.C.; Konofagou, E.E. Acoustic cavitation-based monitoring of the reversibility and permeability of ultrasound-induced blood-brain barrier opening. Phys. Med. Biol. 2015, 60, 9079–9094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquet, F.; Teichert, T.; Wu, S.-Y.; Tung, Y.-S.; Downs, M.; Wang, S.; Chen, C.; Ferrera, V.; Konofagou, E.E. Real-Time, Transcranial Monitoring of Safe Blood-Brain Barrier Opening in Non-Human Primates. PLoS ONE 2014, 9, e84310. [Google Scholar] [CrossRef] [Green Version]
- Kamimura, H.A.; Flament, J.; Valette, J.; Cafarelli, A.; Badin, R.A.; Hantraye, P.; Larrat, B. Feedback control of microbubble cavitation for ultrasound-mediated blood–brain barrier disruption in non-human primates under magnetic resonance guidance. J. Cereb. Blood Flow Metab. 2018, 39, 1191–1203. [Google Scholar] [CrossRef] [Green Version]
- Sojahrood, A.J.; Earl, R.; Haghi, H.; Li, Q.; Porter, T.M.; Kolios, M.C.; Karshafian, R. Nonlinear dynamics of acoustic bubbles excited by their pressure-dependent subharmonic resonance frequency: Influence of the pressure amplitude, frequency, encapsulation and multiple bubble interactions on oversaturation and enhancement of the subharmonic signal. Nonlinear Dyn. 2021, 103, 429–466. [Google Scholar] [CrossRef]
- O’Reilly, M.A.; Hynynen, K. Blood-Brain Barrier: Real-time Feedback-controlled Focused Ultrasound Disruption by Using an Acoustic Emissions–based Controller. Radiology 2012, 263, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Alkins, R.; Schwartz, M.L.; Hynynen, K. Opening the Blood-Brain Barrier with MR Imaging–guided Focused Ultrasound: Preclinical Testing on a Trans–Human Skull Porcine Model. Radiology 2017, 282, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.M.; Deng, L.; Leung, K.; McMahon, D.; O’Reilly, M.A.; Hynynen, K. Three-dimensional transcranial microbubble imaging for guiding volumetric ultrasound-mediated blood-brain barrier opening. Theranostics 2018, 8, 2909–2926. [Google Scholar] [CrossRef]
- Tsai, C.-H.; Zhang, J.-W.; Liao, Y.-Y.; Liu, H.-L. Real-time monitoring of focused ultrasound blood-brain barrier opening via subharmonic acoustic emission detection: Implementation of confocal dual-frequency piezoelectric transducers. Phys. Med. Biol. 2016, 61, 2926–2946. [Google Scholar] [CrossRef] [PubMed]
- Lafond, M.; Asquier, N.; Mestas, J.-L.A.; Carpentier, A.; Umemura, S.-I.; Lafon, C. Evaluation of a Three-Hydrophone Method for 2-D Cavitation Localization. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2018, 65, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Xu, L.; Chien, C.-Y.; Yang, Y.; Gong, Y.; Ye, D.; Pacia, C.P.; Chen, H. 3-D Transcranial Microbubble Cavitation Localization by Four Sensors. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021, 68, 3336–3346. [Google Scholar] [CrossRef] [PubMed]
- Norton, S.; Won, I. Time exposure acoustics. IEEE Trans. Geosci. Remote Sens. 2000, 38, 1337–1343. [Google Scholar] [CrossRef]
- Arvanitis, C.D.; Livingstone, M.S.; McDannold, N. Combined ultrasound and MR imaging to guide focused ultrasound therapies in the brain. Phys. Med. Biol. 2013, 58, 4749–4761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.-Y.; Aurup, C.; Sanchez, C.S.; Grondin, J.; Zheng, W.; Kamimura, H.; Ferrera, V.P.; Konofagou, E.E. Efficient Blood-Brain Barrier Opening in Primates with Neuronavigation-Guided Ultrasound and Real-Time Acoustic Mapping. Sci. Rep. 2018, 8, 7978. [Google Scholar] [CrossRef] [Green Version]
- Pouliopoulos, A.N.; Burgess, M.T.; Konofagou, E.E. Pulse inversion enhances the passive mapping of microbubble-based ultrasound therapy. Appl. Phys. Lett. 2018, 113, 044102. [Google Scholar] [CrossRef]
- Haworth, K.J.; Bader, K.B.; Rich, K.T.; Holland, C.K.; Mast, T.D. Quantitative Frequency-Domain Passive Cavitation Imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2017, 64, 177–191. [Google Scholar] [CrossRef] [Green Version]
- Arvanitis, C.D.; Crake, C.; McDannold, N.; Clement, G.T. Passive Acoustic Mapping with the Angular Spectrum Method. IEEE Trans. Med. Imaging 2017, 36, 983–993. [Google Scholar] [CrossRef] [Green Version]
- Deng, L.; O’Reilly, M.; Jones, R.; An, R.; Hynynen, K. A Multi-frequency Sparse Hemispherical Ultrasound Phased Array for Microbubble-mediated Transcranial Therapy and Simultaneous Cavitation Mapping. Phys. Med. Biol. 2016, 61, 8476–8501. [Google Scholar] [CrossRef] [Green Version]
- Johansen, K.; Song, J.H.; Prentice, P. Performance characterisation of a passive cavitation detector optimised for subharmonic periodic shock waves from acoustic cavitation in MHz and sub-MHz ultrasound. Ultrason. Sonochem. 2018, 43, 146–155. [Google Scholar] [CrossRef]
- Jeong, J.J.; Choi, H. An impedance measurement system for piezoelectric array element transducers. Measurement 2017, 97, 138–144. [Google Scholar] [CrossRef]
- Wear, K.A. Spatiotemporal Deconvolution of Hydrophone Response for Linear and Nonlinear Beams—Part I: Theory, Spatial-Averaging Correction Formulas, and Criteria for Sensitive Element Size. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2022, 69, 1243–1256. [Google Scholar] [CrossRef] [PubMed]
- Wear, K.A.; Baker, C.; Miloro, P. Directivity and Frequency-Dependent Effective Sensitive Element Size of Needle Hy-drophone: Predictions from Four Theoretical Forms Compared with Measurements. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2018, 65, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Morse, P.M.; Ingard, K.U. Theoretical Acoustics; Princeton University Press: Princeton, NJ, USA, 1987. [Google Scholar]
- O’Reilly, M.A.; Muller, A.; Hynynen, K. Ultrasound Insertion Loss of Rat Parietal Bone Appears to Be Proportional to Animal Mass at Submegahertz Frequencies. Ultrasound Med. Biol. 2011, 37, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, A.D.; Cain, C.A.; Hall, T.L.; Fowlkes, J.B.; Xu, Z. Probability of Cavitation for Single Ultrasound Pulses Applied to Tissues and Tissue-Mimicking Materials. Ultrasound Med. Biol. 2013, 39, 449–465. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Z.; Sujarittam, K.; Yildiz, B.I.; Dickinson, R.J.; Choi, J.J. Passive Cavitation Detection with a Needle Hydrophone Array. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2022, 69, 233–240. [Google Scholar] [CrossRef]
- McDannold, N.; Vykhodtseva, N.; Hynynen, K. Blood-Brain Barrier Disruption Induced by Focused Ultrasound and Circulating Preformed Microbubbles Appears to Be Characterized by the Mechanical Index. Ultrasound Med. Biol. 2008, 34, 834–840. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.M.; O’Reilly, M.A.; Hynynen, K. Transcranial passive acoustic mapping with hemispherical sparse arrays using CT-based skull-specific aberration corrections: A simulation study. Phys. Med. Biol. 2013, 58, 4981–5005. [Google Scholar] [CrossRef] [Green Version]
- Oˈreilly, M.A.; Hynynen, K. A super-resolution ultrasound method for brain vascular mapping. Med. Phys. 2013, 40, 110701. [Google Scholar] [CrossRef] [Green Version]
- Cross, C.G.; Payne, A.H.; Hawryluk, G.W.; Haag-Roeger, R.; Cheeniyil, R.; Brady, D.; Odéen, H.; Minoshima, S.; Cross, D.J.; Anzai, Y. Technical Note: Quantification of blood-spinal cord barrier permeability after application of magnetic resonance-guided focused ultrasound in spinal cord injury. Med. Phys. 2021, 48, 4395–4401. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PZT Receiver | O’Reilly and Hynynen 2010 | PVDF Receiver | Needle Hydrophone | Fibre-Optic Hydrophone | |
|---|---|---|---|---|---|
| Active Material | PZT | PVDF | PVDF | PVDF | Fibre |
| Active Area (mm2) | 201 | 17.8 | 1.2 | 0.2 | 79 μm2 |
| Frequency Range (MHz) | 0.7–1.1 | 0.3–4.6 | 0.5–5.4 | 0.1–20 | 0.25–50 |
| Sensitivity (Order of magnitude in mV/MPa) | 106 | 103 | 103 | 102 | 102 |
| Connection | Coax | Coax | Coax | Coax | Fibre-optic system |
| Cost per receiver (USD) | N/A | N/A | 4 | 2087 * | 389 ** |
| Frequency (MHz) | Sensitivity ± 1 Standard Deviation (V/MPa) |
|---|---|
| 0.51 * | 3.87 ± 0.44 |
| 1.1 ** | 3.59 ± 0.24 |
| 1.7 * | 3.51 ± 0.14 |
| 2.9 * | 2.87 ± 0.07 |
| 3.2 ** | 2.77 ± 0.10 |
| 4.1 * | 3.08 ± 0.04 |
| 5.4 ** | 2.36 ± 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.; O’Reilly, M.A.; Hynynen, K. A PVDF Receiver for Acoustic Monitoring of Microbubble-Mediated Ultrasound Brain Therapy. Sensors 2023, 23, 1369. https://doi.org/10.3390/s23031369
Lin Y, O’Reilly MA, Hynynen K. A PVDF Receiver for Acoustic Monitoring of Microbubble-Mediated Ultrasound Brain Therapy. Sensors. 2023; 23(3):1369. https://doi.org/10.3390/s23031369
Chicago/Turabian StyleLin, Yi, Meaghan A. O’Reilly, and Kullervo Hynynen. 2023. "A PVDF Receiver for Acoustic Monitoring of Microbubble-Mediated Ultrasound Brain Therapy" Sensors 23, no. 3: 1369. https://doi.org/10.3390/s23031369
APA StyleLin, Y., O’Reilly, M. A., & Hynynen, K. (2023). A PVDF Receiver for Acoustic Monitoring of Microbubble-Mediated Ultrasound Brain Therapy. Sensors, 23(3), 1369. https://doi.org/10.3390/s23031369