


Photoplethysmography Driven Hypertension Identification: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
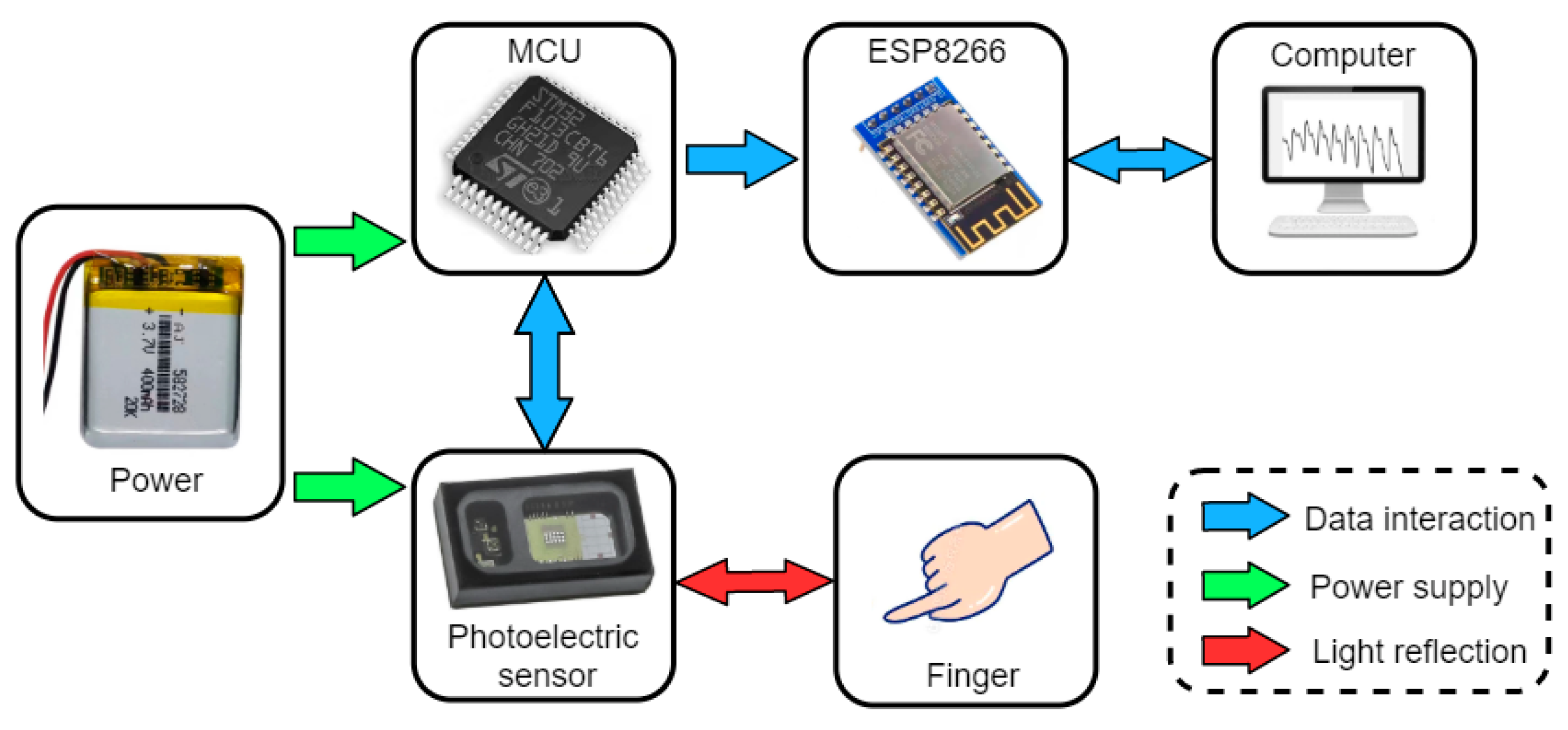
2.1. Bespoke Data Acquisition Device and Its System
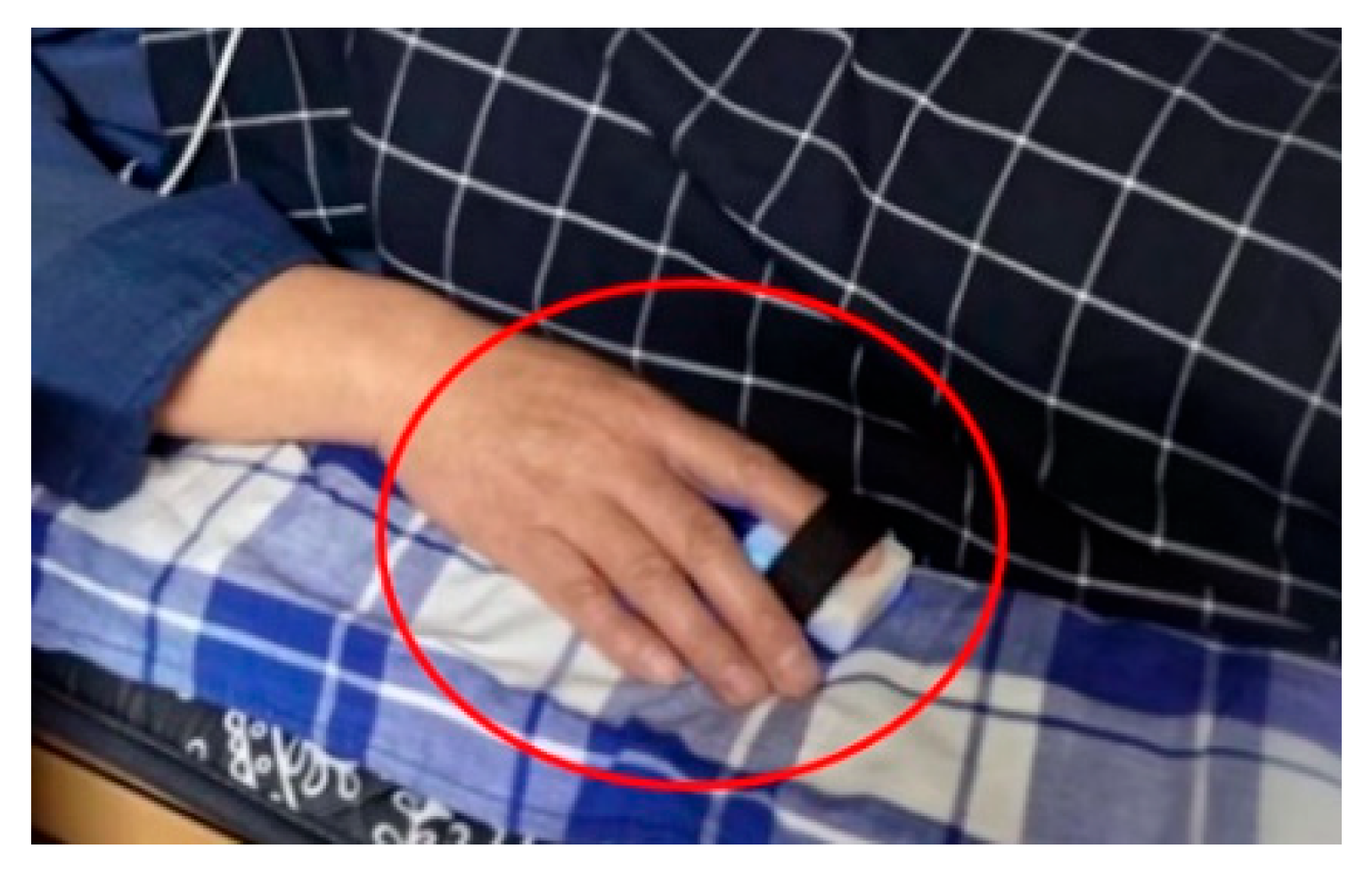
2.2. Data Acquisition
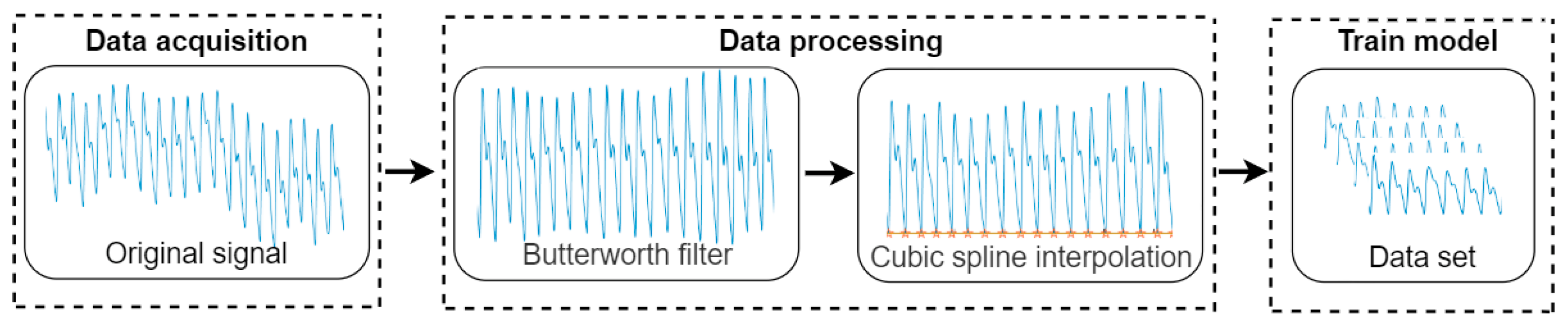
2.3. Data Preprocessing
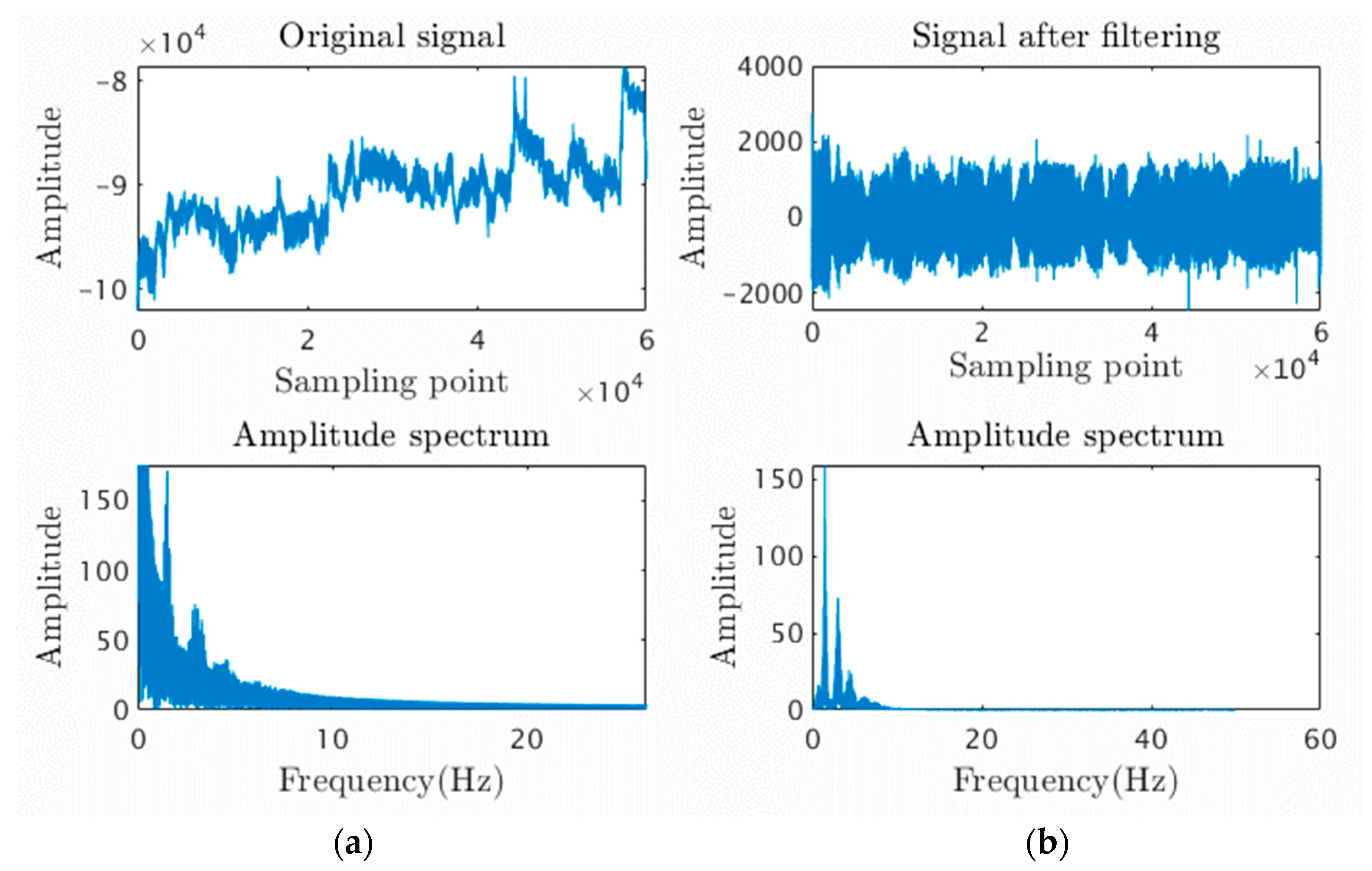
2.3.1. Butterworth Filter
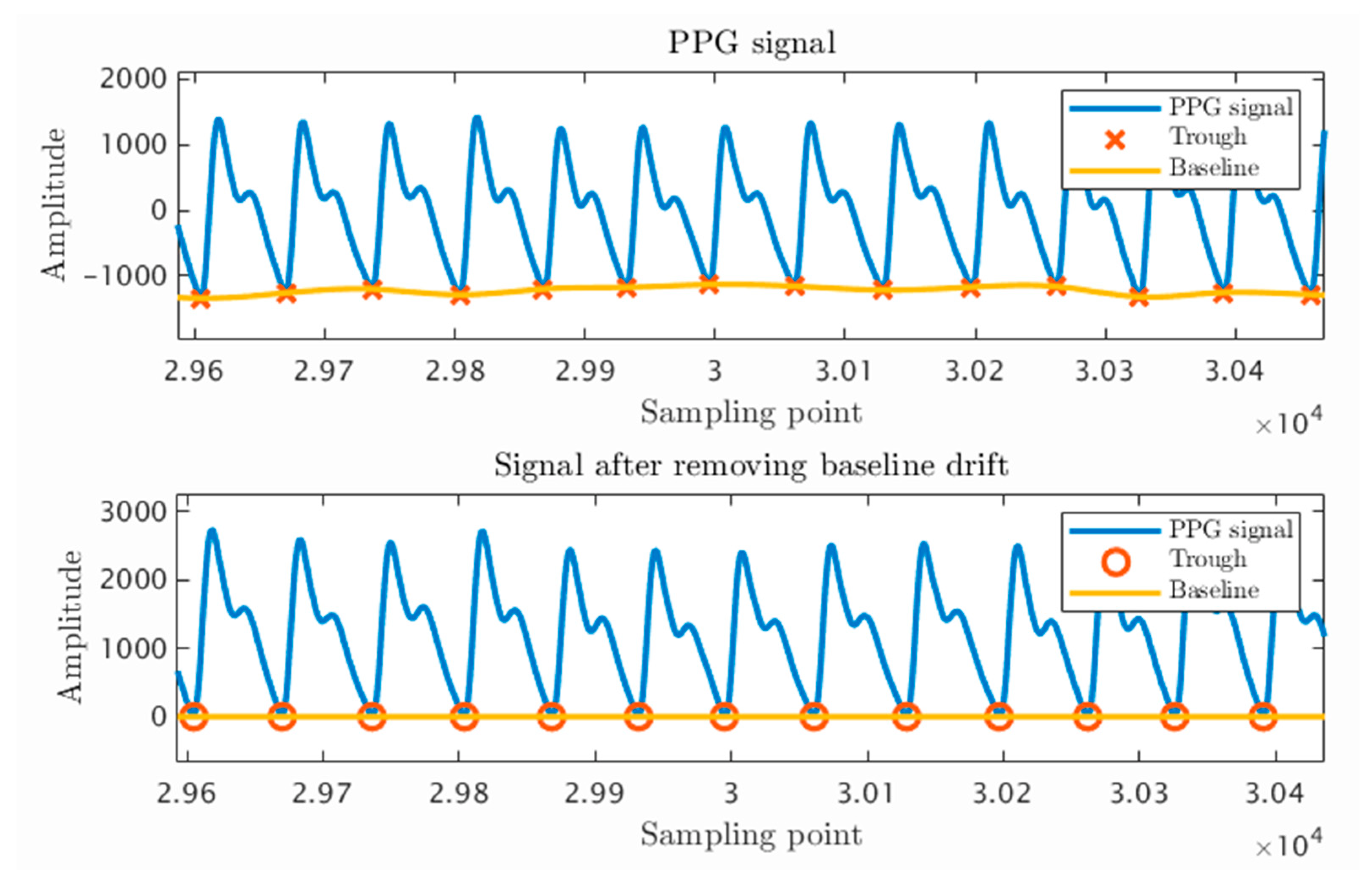
2.3.2. Cubic Spline Interpolation
2.4. LSTM-Attention Model
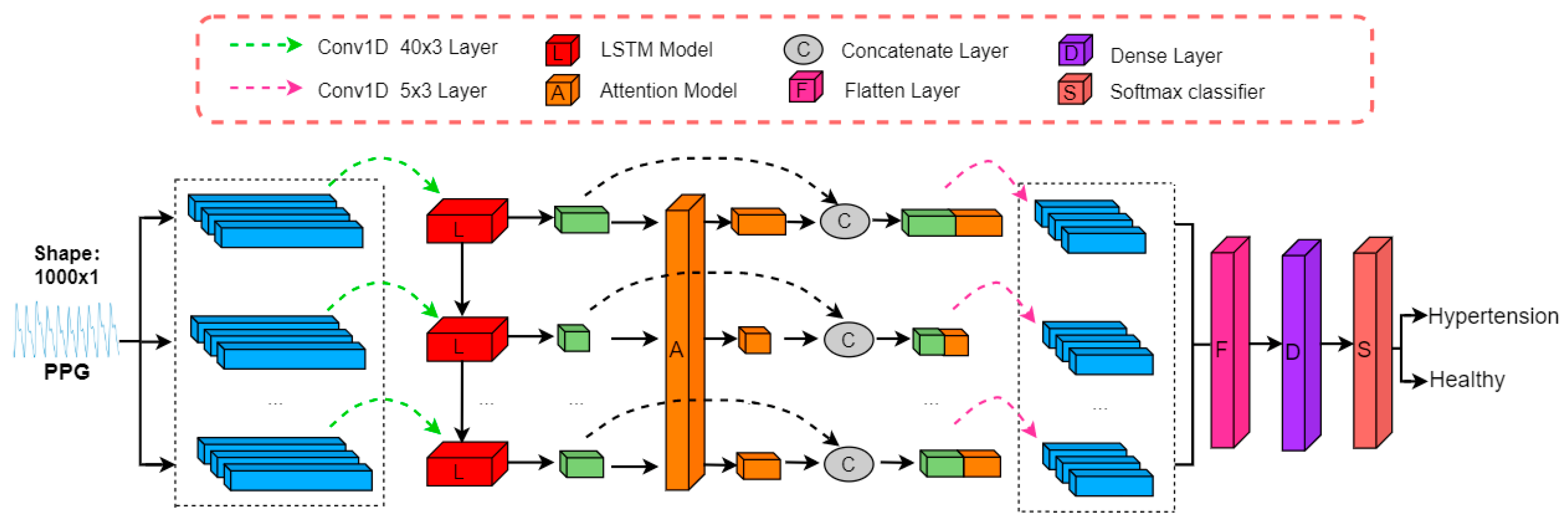
2.4.1. Model Architecture
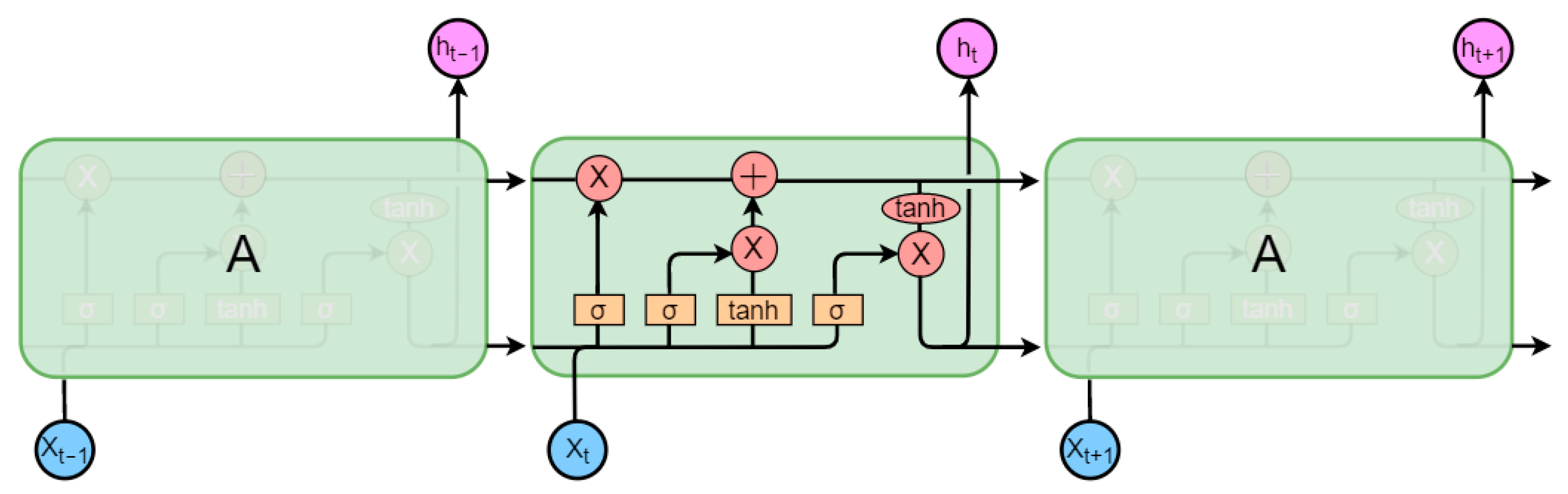
LSTM Block
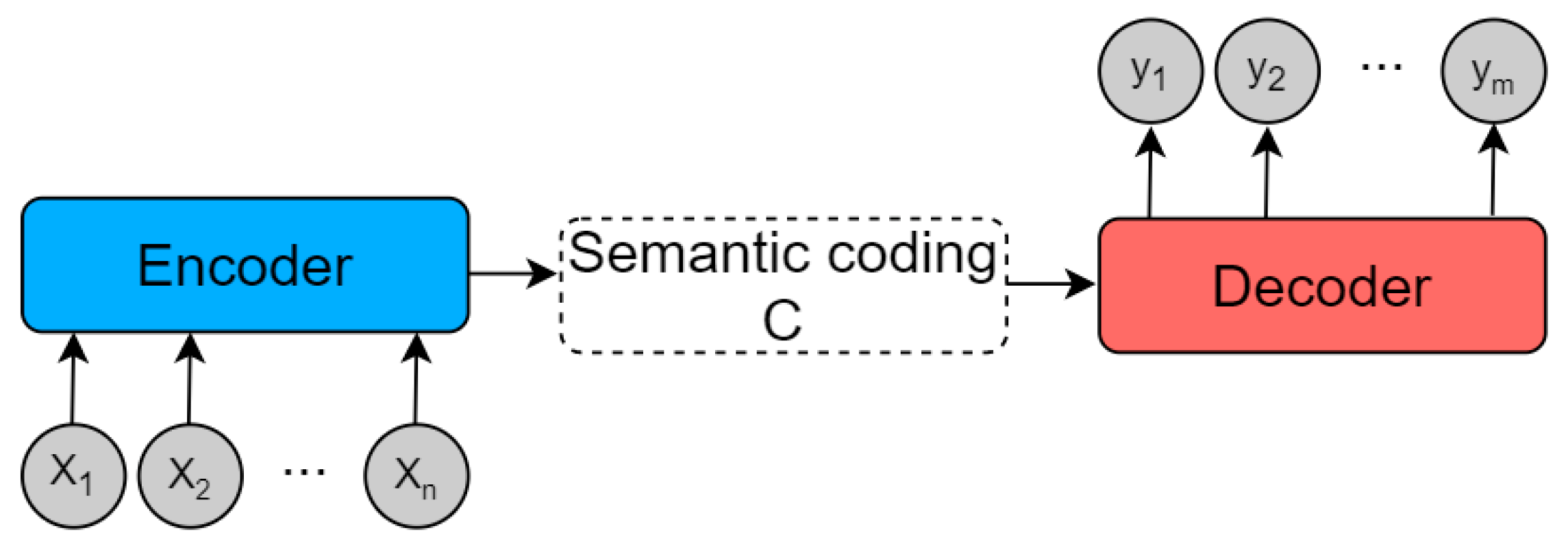
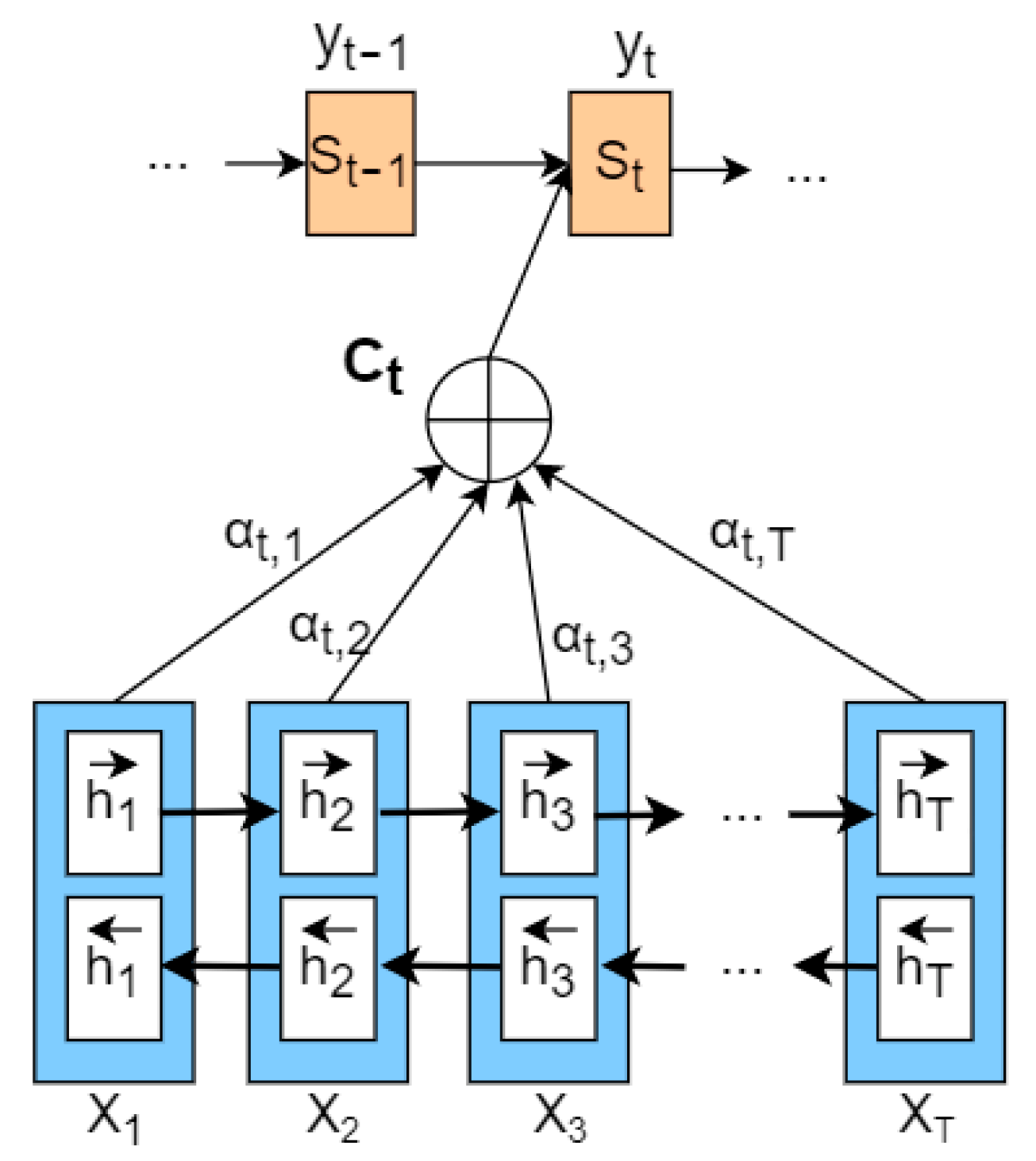
Attention Block
2.4.2. Model Parameters
2.4.3. Model Training
2.4.4. Performance Evaluation
3. Results
4. Discussion
4.1. Performance of LSTM-Attention Model
4.2. Prospect of Hypertension Identification
4.3. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Annual report on cardiovascular health and diseases in China 2020. J. Cardiovasc. Pulm. Dis. 2021, 40, 1005–1009.
- Choi, S.-K. Editorial: Diabetes, Hypertension and Cardiovascular Diseases. Front. Physiol. 2021, 12, 765767. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for Blood Pressure Measurement in Humans and Experimental Animals: Part 1: Blood pressure measurement in humans—A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Co. Circulation 2005, 111, 697–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bia, D.; Zócalo, Y.; Sánchez, R.; Lev, G.; Mendiz, O.; Pessana, F.; Ramirez, A.; Cabrera-Fischer, E.I. Aortic systolic and pulse pressure invasively and non-invasively obtained: Comparative analysis of recording techniques, arterial sites of measurement, waveform analysis algorithms and calibration methods. Front. Physiol. 2023, 14, 1113972. [Google Scholar] [CrossRef] [PubMed]
- Dart, R.A.; Alpert, B.; Quinn, D. Effect of mechanical behavior of the brachial artery on blood pressure measurement during cuff inflation and cuff deflation. Blood Press. Monit. 2014, 19, 120. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Wu, S.; Shi, J.; Huang, Z.; Zhu, C.; Du, X.; Chen, S.; Wang, G.; Cui, W. Stage 1 hypertension defined by the 2017 ACC/AHA Hypertension Guidelines and Risk of Cardiovascular Events: A Cohort Study from Northern China. Hypertens. Res. 2019, 42, 1606–1615. [Google Scholar] [CrossRef]
- Srinivasan, K.; Mahendran, N.; Vincent, D.R.; Chang, C.-Y.; Syed-Abdul, S. Realizing an Integrated Multistage Support Vector Machine Model for Augmented Recognition of Unipolar Depression. Electronics 2020, 9, 647. [Google Scholar] [CrossRef] [Green Version]
- Mahendran, N.; Vincent, P.M.D.R.; Srinivasan, K.; Sharma, V.; Jayakody, D.N.K. Realizing a Stacking Generalization Model to Improve the Prediction Accuracy of Major Depressive Disorder in Adults. IEEE Access 2020, 8, 49509–49522. [Google Scholar] [CrossRef]
- Salankar, N.; Koundal, D.; Qaisar, S.M. Stress Classification by Multimodal Physiological Signals Using Variational Mode Decomposition and Machine Learning. J. Health Eng. 2021, 2021, 2146369. [Google Scholar] [CrossRef]
- Ifeagwazi, C.M.; Egberi, H.E.; Chukwuorji, J.C. Emotional reactivity and blood pressure elevations: Anxiety as a mediator. Psychol. Health Med. 2017, 23, 585–592. [Google Scholar] [CrossRef]
- Yoon, Y.; Cho, J.H.; Yoon, G. Non-constrained Blood Pressure Monitoring Using ECG and PPG for Personal Healthcare. J. Med. Syst. 2008, 33, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Khanokh, B.; Slovik, Y. The difference in pulse transit time to the toe and finger measured by photoplethysmography. Physiol. Meas. 2001, 23, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Monte-Moreno, E. Non-invasive estimate of blood glucose and blood pressure from a photoplethysmograph by means of machine learning techniques. Artif. Intell. Med. 2011, 53, 127–138. [Google Scholar] [CrossRef]
- Nour, M.; Polat, K. Automatic Classification of Hypertension Types Based on Personal Features by Machine Learning Algorithms. Math. Probl. Eng. 2020, 2020, 2742781. [Google Scholar] [CrossRef] [Green Version]
- Avon, G.; Bucolo, M.; Buscarino, A.; Fortuna, L. Sensing Frequency Drifts: A Lookup Table Approach. IEEE Access 2022, 10, 96249–96259. [Google Scholar] [CrossRef]
- Tjahjadi, H.; Ramli, K.; Murfi, H. Noninvasive Classification of Blood Pressure Based on Photoplethysmography Signals Using Bidirectional Long Short-Term Memory and Time-Frequency Analysis. IEEE Access 2020, 8, 20735–20748. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, Z.; Ward, R.; Elgendi, M. Photoplethysmography and Deep Learning: Enhancing Hypertension Risk Stratification. Biosensors 2018, 8, 101. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Liang, H.; Ding, C.; Huang, X.; Huang, J.; Peng, Q. Improving the Accuracy in Classification of Blood Pressure from Photoplethysmography Using Continuous Wavelet Transform and Deep Learning. Int. J. Hypertens. 2021, 2021, 9938584. [Google Scholar] [CrossRef] [PubMed]
- Kong, H.; West, S.; Introduction, A. WORLD MEDICAL ASSOCIATION Ethical Principles for Medical Research Involving Human Subjects. In Proceedings of the 18th WMA General Assembly, Helsinki, Finland, June 1964; pp. 10–12. [Google Scholar]
- Mejía-Mejía, E.; Kyriacou, P.A. Effects of noise and filtering strategies on the extraction of pulse rate variability from photoplethysmograms. Biomed. Signal Process. Control. 2023, 80, 104291. [Google Scholar] [CrossRef]
- Malica, T.; Shekhar, S.; Ali, Z. Design and comparison of butterworth and chebyshev type-1 low pass filter using Matlab. Res. Cell Int. J. Eng. Sci. 2011, 4, 2229–6913. [Google Scholar]
- Huang, C.-M.; Wei, C.-C.; Liao, Y.-T.; Chang, H.-C.; Kao, S.-T.; Li, T.-C. Developing the Effective Method of Spectral Harmonic Energy Ratio to Analyze the Arterial Pulse Spectrum. Evid.-Based Complement. Altern. Med. 2011, 2011, 342462. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Wang, X.; Deller, J.R.; Fu, J. Shape-Preserving Preprocessing for Human Pulse Signals Based on Adaptive Parameter Determination. IEEE Trans. Biomed. Circuits Syst. 2013, 8, 594–604. [Google Scholar] [CrossRef]
- Hewamalage, H.; Bergmeir, C.; Bandara, K. Recurrent Neural Networks for Time Series Forecasting: Current status and future directions. Int. J. Forecast. 2020, 37, 388–427. [Google Scholar] [CrossRef]
- Zhang, X.; Zhong, C.; Zhang, J.; Wang, T.; Ng, W.W. Robust recurrent neural networks for time series forecasting. Neurocomputing 2023, 526, 143–157. [Google Scholar] [CrossRef]
- Gers, F.A.; Schmidhuber, J.; Cummins, F. Learning to Forget: Continual Prediction with LSTM. Neural Comput. 2000, 12, 2451–2471. [Google Scholar] [CrossRef] [PubMed]
- Chorowski, J.; Bahdanau, D.; Cho, K.; Bengio, Y. End-to-end Continuous Speech Recognition using Attention-based Recurrent NN: First Results. arXiv 2014, arXiv:1412.1602. [Google Scholar]
- Chen, K.; Wang, R.; Utiyama, M.; Sumita, E.; Zhao, T. Neural Machine Translation with Sentence-Level Topic Context. IEEE/ACM Trans. Audio Speech Lang. Process. 2019, 27, 1970–1984. [Google Scholar] [CrossRef]
- Zhao, H. Image Target Recognition Based on Multiregional Features under Hybrid Attention Mechanism. Trait. Signal 2022, 39, 595–601. [Google Scholar] [CrossRef]
- Huang, J.; Wu, W.; Li, J.; Wang, S. Text Summarization Method Based on Gated Attention Graph Neural Network. Sensors 2023, 23, 1654. [Google Scholar] [CrossRef]
- Lee, H.; Song, J. Introduction to convolutional neural network using Keras; an understanding from a statistician. Commun. Stat. Appl. Methods 2019, 26, 591–610. [Google Scholar] [CrossRef] [Green Version]
- Krichen, M.; Mihoub, A.; Alzahrani, M.Y.; Adoni, W.Y.H.; Nahhal, T. Are Formal Methods Applicable to Machine Learning and Artificial Intelligence? In Proceedings of the 2022 2nd International Conference of Smart Systems and Emerging Technologies, SMARTTECH 2022, Riyadh, Saudi Arabia, 9–11 May 2022; pp. 48–53. [Google Scholar] [CrossRef]
- Moscato, S.; Giudice, S.L.; Massaro, G.; Chiari, L. Wrist Photoplethysmography Signal Quality Assessment for Reliable Heart Rate Estimate and Morphological Analysis. Sensors 2022, 22, 5831. [Google Scholar] [CrossRef] [PubMed]
- Fleischhauer, V.; Feldheiser, A.; Zaunseder, S. Beat-to-Beat Blood Pressure Estimation by Photoplethysmography and Its Interpretation. Sensors 2022, 22, 7037. [Google Scholar] [CrossRef]
- Zambrana-Vinaroz, D.; Vicente-Samper, J.M.; Manrique-Cordoba, J.; Sabater-Navarro, J.M. Wearable Epileptic Seizure Prediction System Based on Machine Learning Techniques Using ECG, PPG and EEG Signals. Sensors 2022, 22, 9372. [Google Scholar] [CrossRef] [PubMed]
- Uçar, M.K.; Bozkurt, M.R.; Bilgin, C.; Polat, K. Automatic sleep staging in obstructive sleep apnea patients using photoplethysmography, heart rate variability signal and machine learning techniques. Neural Comput. Appl. 2016, 29, 1–16. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, Z.; Ward, R.; Elgendi, M. Hypertension Assessment via ECG and PPG Signals: An Evaluation Using MIMIC Database. Diagnostics 2018, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Avolio, A.; Cox, J.; Louka, K.; Shirbani, F.; Tan, I.; Qasem, A.; Butlin, M. Challenges Presented by Cuffless Measurement of Blood Pressure if Adopted for Diagnosis and Treatment of Hypertension. Pulse 2022, 10, 34–45. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Dimension (mm) | 45 × 38 × 20 |
| LED wavelength (nm) | 527/660/880 |
| Type of light source | Green/Red/Infrared light |
| PPG sampling form | Light reflection |
| LED supply voltage (V) | 3.3 |
| Working current (mA) | 1.5 |
| Sampling rate (Hz) | 100 |
| Battery capacity (mAh) | 400 |
| No. of Volunteer | Experimental Data/bpm | DB12/bpm | Error |
|---|---|---|---|
| 89 | 91 | 2% | |
| 1 | 87 | 87 | 0% |
| 90 | 89 | 1% | |
| 83 | 83 | 0% | |
| 2 | 85 | 86 | 1% |
| 81 | 82 | 1% | |
| 78 | 80 | 2% | |
| 3 | 79 | 80 | 1% |
| 76 | 76 | 0% |
| Group | No. of Males (%) | Age | BMI/(kg/m2) | SBP/(mmHg) |
|---|---|---|---|---|
| Healthy | 8 (53.3) | 54.7 ± 5.9 | 21.6 ± 2.7 | 115.4 ± 8.9 |
| Hypertension | 8 (53.3) | 55.3 ± 5.7 | 25.5 ± 2.9 | 143.6 ± 7.5 |
| Parameter | Value |
|---|---|
| Activation function | ReLU |
| Classifier | SoftMax |
| Learn-rate | 0.001 |
| LSTM-layers | 5 |
| Batch-size | 256 |
| Num-epochs | 500 |
| Dropout | 0.5 |
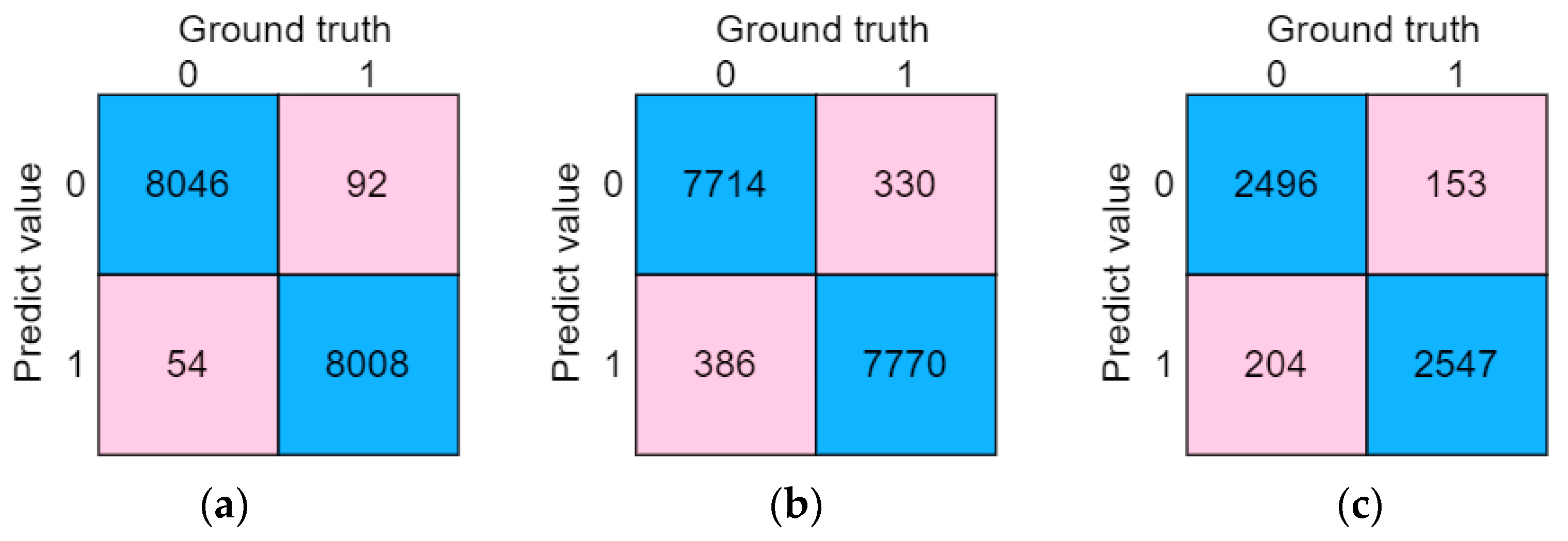
| Confusion Matrix | Ground Truth | ||
|---|---|---|---|
| Positive | Negative | ||
| Predicted value | Positive | TP | FP |
| Negative | FN | TN | |
| Characteristic | Definition |
|---|---|
| The amplitude of the dominant wave | |
| The amplitude of the dicrotic wave | |
| The amplitude of the dicrotic notch | |
| The ratio of y to x | |
| The ratio of x − y to x | |
| The duration between the main wave peaks of two adjacent PPG waveforms | |
| The duration from trough to the peak of a single PPG waveform | |
| The duration from trough to the dicrotic notch of a single PPG waveform | |
| The duration from trough to the dicrotic wave peak of a single PPG waveform | |
| The duration between the trough of two adjacent PPG waveforms | |
| The duration from principal wave peaks to dicrotic wave peak | |
| The ratio of to | |
| The ratio of to | |
| The ratio of to | |
| The ratio of to | |
| The frequency of Peak1 after the Fourier transform | |
| The frequency of Peak2 after the Fourier transform | |
| The frequency of Peak3 after the Fourier transform | |
| Shannon Entropy | |
| Information Entropy |
| Model | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| LSTM-Attention | 0.991 | 0.989 | 0.993 | 0.991 |
| LSTM | 0.953 | 0.971 | 0.934 | 0.952 |
| BiLSTM | 0.958 | 0.975 | 0.940 | 0.957 |
| SVM | 0.904 | 0.917 | 0.938 | 0.927 |
| KNN | 0.946 | 0.936 | 0.984 | 0.959 |
| Model | Time/s |
|---|---|
| LSTM-Attention | 10.3 |
| LSTM | 6.5 |
| BiLSTM | 8.6 |
| SVM | NA |
| KNN | NA |
| Model | Feature Extraction | Database | Classifier | F1-Score |
|---|---|---|---|---|
| PPG features [38] | 10 PPG features | 121 subjects (MIMIC database) | AdaBoost | 80.11% |
| PPG features [38] | 10 PPG features | 121 subjects (MIMIC database) | KNN | 86.94% |
| Raw PPG signal [17] | Short-time Fourier transform (spectrogram) | 219 subjects (Figshare database) | BLSTM with time-frequency analysis | 97.39% |
| Raw PPG signal [18] | Continuous wavelet transform (scalogram) | 219 subjects (Figshare database) | CNNs | 92.55% |
| Raw PPG signal (current study) | Raw PPG signal after preprocessing | 30 subjects (Self-collecting database) | LSTM-Attention | 99.10% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, L.; Wei, M.; Hu, S.; Sheng, B. Photoplethysmography Driven Hypertension Identification: A Pilot Study. Sensors 2023, 23, 3359. https://doi.org/10.3390/s23063359
Yan L, Wei M, Hu S, Sheng B. Photoplethysmography Driven Hypertension Identification: A Pilot Study. Sensors. 2023; 23(6):3359. https://doi.org/10.3390/s23063359
Chicago/Turabian StyleYan, Liangwen, Mingsen Wei, Sijung Hu, and Bo Sheng. 2023. "Photoplethysmography Driven Hypertension Identification: A Pilot Study" Sensors 23, no. 6: 3359. https://doi.org/10.3390/s23063359
APA StyleYan, L., Wei, M., Hu, S., & Sheng, B. (2023). Photoplethysmography Driven Hypertension Identification: A Pilot Study. Sensors, 23(6), 3359. https://doi.org/10.3390/s23063359