


An Attempt to Develop a Model of Brain Waves Using Quantitative Electroencephalography with Closed Eyes in K1 Kickboxing Athletes—Initial Concept

 ,
,  ,
, 

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. QEEG Procedure
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Marino, S. A Complete Guide to Kickboxing; Enslow Publishing: New York, NY, USA, 2018. [Google Scholar]
- Rydzik, Ł. Indices of technical and tactical training during kickboxing at different levels of competition in the K1 Formula. J. Kinesiol. Exerc. Sci. 2022, 31, 1–5. [Google Scholar] [CrossRef]
- Green, G.A.; Pollack, K.M.; D’Angelo, J.; Schickendantz, M.S.; Caplinger, R.; Weber, K.; Valadka, A.; McAllister, T.W.; Dick, R.W.; Mandelbaum, B.; et al. Mild Traumatic Brain Injury in Major and Minor League Baseball Players. Am. J. Sports Med. 2015, 43, 1118–1126. [Google Scholar] [CrossRef]
- Esser, T.; Gruber, C.; Bürkner, A.; Buchmann, N.; Minzlaff, P.; Prodinger, P.M. Das Schädel-Hirn-Trauma im Wintersport. Die Orthopädie 2022, 51, 920–928. [Google Scholar] [CrossRef]
- Georges, A.; Das, J.M. Traumatic Brain Injury; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Harmon, K.G.; Drezner, J.A.; Gammons, M.; Guskiewicz, K.M.; Halstead, M.; Herring, S.A.; Kutcher, J.S.; Pana, A.; Putukian, M.; Roberts, W.O. American Medical Society for Sports Medicine position statement: Concussion in sport. Br. J. Sports Med. 2013, 47, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Banks, R.E.; Domínguez, D.C. Sports-Related Concussion: Neurometabolic Aspects. Semin. Speech Lang. 2019, 40, 333–343. [Google Scholar] [CrossRef] [PubMed]
- McCrory, P.; Meeuwisse, W.H.; Kutcher, J.S.; Jordan, B.D.; Gardner, A. What is the evidence for chronic concussion-related changes in retired athletes: Behavioural, pathological and clinical outcomes? Br. J. Sports Med. 2013, 47, 327–330. [Google Scholar] [CrossRef]
- Pierpoint, L.A.; Collins, C. Epidemiology of Sport-Related Concussion. Clin. Sports Med. 2021, 40, 1–18. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Manley, G.T.; Abrams, M.; Åkerlund, C.; Andelic, N.; Aries, M.; Bashford, T.; Bell, M.J.; Bodien, Y.G.; et al. Traumatic brain injury: Progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022, 21, 1004–1060. [Google Scholar] [CrossRef]
- Ling, H.; Hardy, J.; Zetterberg, H. Neurological consequences of traumatic brain injuries in sports. Mol. Cell. Neurosci. 2015, 66, 114–122. [Google Scholar] [CrossRef]
- Zuckerman, S.L.; Yengo-Kahn, A.M.; Tang, A.R.; Bailes, J.E.; Beauchamp, K.; Berger, M.S.; Bonfield, C.M.; Camarata, P.J.; Cantu, R.C.; Davis, G.A.; et al. Sport-Related Structural Brain Injury and Return to Play: Systematic Review and Expert Insight. Neurosurgery 2021, 88, E495–E504. [Google Scholar] [CrossRef]
- McAllister, T.; McCrea, M. Long-Term Cognitive and Neuropsychiatric Consequences of Repetitive Concussion and Head-Impact Exposure. J. Athl. Train. 2017, 52, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodríguez, M.; García-Gómez, S.; Coterón, J.; García-Hernández, J.J.; Pérez-Tejero, J. Physical Activity and Sport for Acquired Brain Injury (PASABI): A Non-Randomized Controlled Trial. Medicina 2021, 57, 122. [Google Scholar] [CrossRef] [PubMed]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 97699. [Google Scholar] [CrossRef]
- Sagher, O.; McGillicuddy, J.E. Editorial: Brain injury in sports. J. Neurosurg. 2016, 124, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Giza, C.C.; Kutcher, J.S.; Ashwal, S.; Barth, J.; Getchius, T.S.D.; Gioia, G.A.; Gronseth, G.S.; Guskiewicz, K.; Mandel, S.; Manley, G.; et al. Summary of evidence-based guideline update: Evaluation and management of concussion in sports: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2013, 80, 2250–2257. [Google Scholar] [CrossRef]
- Schlegel, P.; Novotny, M.; Valis, M.; Klimova, B. Head injury in mixed martial arts: A review of epidemiology, affected brain structures and risks of cognitive decline. Phys. Sportsmed. 2021, 49, 371–380. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Johnston, K.; Dvorak, J.; Aubry, M.; Molloy, M.; Cantu, R. Consensus Statement on Concussion in Sport: The 3rd International Conference on Concussion in Sport Held in Zurich, November 2008. J. Athl. Train. 2009, 44, 434–448. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.H.; Aubry, M.; Cantu, B.; Dvořák, J.; Echemendia, R.J.; Engebretsen, L.; Johnston, K.; Kutcher, J.S.; Raftery, M.; et al. Consensus statement on concussion in sport: The 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br. J. Sports Med. 2013, 47, 250–258. [Google Scholar] [CrossRef]
- Laccarino, C.; Carriero, A.; Cipolloni, L.; Signoretti, S.; Frati, A.; Santoro, A.; Fineschi, V. Mild traumatic brain injury in a boxer: A neuropathological study. Int. J. Legal Med. 2017, 131, 1415–1420. [Google Scholar]
- Bledsoe, G.H.; Li, G.; Levy, F. Injury risk in professional boxing. South. Med. J. 2005, 98, 994–998. Available online: https://pubmed.ncbi.nlm.nih.gov/16295814/ (accessed on 18 April 2023).
- Casson, I.R.; Viano, D.C.; Powell, J.W.; Pellman, E.J. Twelve Years of National Football League Concussion Data. Sports Health 2010, 2, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Mez, J.; Daneshvar, D.H.; Kiernan, P.T.; Abdolmohammadi, B.; Alvarez, V.E.; Huber, B.R.; Alosco, M.L.; Solomon, T.M.; Nowinski, C.J.; McHale, L.; et al. Clinicopathological Evaluation of Chronic Traumatic Encephalopathy in Players of American Football. JAMA 2017, 318, 360. [Google Scholar] [CrossRef]
- Liu, H.; Deng, B.; Zhou, H.; Wu, Z.; Chen, Y.; Weng, G.; Zhu, S.; Xu, J.; Wang, H.; Zhou, Z.; et al. QEEG indices are associated with inflammatory and metabolic risk factors in Parkinson’s disease dementia: An observational study. eClinicalMedicine 2022, 52, 101615. [Google Scholar] [CrossRef] [PubMed]
- Rydzik, Ł.; Wąsacz, W.; Ambroży, T.; Javdaneh, N.; Brydak, K.; Kopańska, M. The Use of Neurofeedback in Sports Training: Systematic Review. Brain Sci. 2023, 13, 660. [Google Scholar] [CrossRef]
- Kopańska, M.; Ochojska, D.; Muchacka, R.; Dejnowicz-Velitchkov, A.; Banaś-Ząbczyk, A.; Szczygielski, J. Comparison of QEEG Findings before and after Onset of Post-COVID-19 Brain Fog Symptoms. Sensors 2022, 22, 6606. [Google Scholar] [CrossRef]
- De Kanda, P.A.M.; Anghinah, R.; Smidth, M.T.; Silva, J.M. The clinical use of quantitative EEG in cognitive disorders. Dement. Neuropsychol. 2009, 3, 195–203. [Google Scholar] [CrossRef]
- Babiloni, C.; Brancucci, A.; Babiloni, F.; Capotosto, P.; Carducci, F.; Cincotti, F.; Arendt-Nielsen, L.; Chen, A.C.N.; Rossini, P.M. Anticipatory cortical responses during the expectancy of a predictable painful stimulation. A high-resolution electroencephalography study. Eur. J. Neurosci. 2003, 18, 1692–1700. [Google Scholar] [CrossRef]
- Başar, E.; Schürmann, M.; Başar-Eroglu, C.; Karakaş, S. Alpha oscillations in brain functioning: An integrative theory. Int. J. Psychophysiol. 1997, 26, 5–29. [Google Scholar] [CrossRef]
- Safinia, C.; Bershad, E.M.; Clark, H.B.; SantaCruz, K.; Alakbarova, N.; Suarez, J.I.; Divani, A.A. Chronic Traumatic Encephalopathy in Athletes Involved with High-impact Sports. J. Vasc. Interv. Neurol. 2016, 9, 34–48. [Google Scholar]
- Siepmann, M.; Kirch, W. Effects of Caffeine on Topographic Quantitative EEG. Neuropsychobiology 2002, 45, 161–166. [Google Scholar] [CrossRef]
- Fetz, E.E. Volitional control of neural activity: Implications for brain-computer interfaces. J. Physiol. 2007, 579, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Jurewicz, K.; Paluch, K.; Kublik, E.; Rogala, J.; Mikicin, M.; Wróbel, A. EEG-neurofeedback training of beta band (12–22 Hz) affects alpha and beta frequencies—A controlled study of a healthy population. Neuropsychologia 2018, 108, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Zamysłowski, S. Schemes of EEG electrode placement in humans. In Licensing Training for a Biofeedback Specialist and Therapist, 2nd ed.; Kubik, A., Ed.; Polish Society of Clinical Neurophysiology: Warszawa, Poland, 2015; pp. 47–51. [Google Scholar]
- Barrett Stephen, M.D. How Useful Is a Quantitative Electroencephalogram (qEEG)? Quackwatch: Amherst, NY, USA, 2015. [Google Scholar]
- Gudmundsson, S.; Runarsson, T.P.; Sigurdsson, S.; Eiriksdottir, G.; Johnsen, K. Reliability of quantitative EEG features. Clin. Neurophysiol. 2007, 118, 2162–2171. [Google Scholar] [CrossRef] [PubMed]
- Marzbani, H.; Marateb, H.; Mansourian, M. Methodological Note: Neurofeedback: A Comprehensive Review on System Design, Methodology and Clinical Applications. Basic Clin. Neurosci. J. 2016, 7, 2. [Google Scholar] [CrossRef]
- Gorgoni, M.; Ferlazzo, F.; Ferrara, M.; Moroni, F.; D’Atri, A.; Fanelli, S.; Gizzi Torriglia, I.; Lauri, G.; Marzano, C.; Rossini, P.M.; et al. Topographic electroencephalogram changes associated with psychomotor vigilance task performance after sleep deprivation. Sleep Med. 2014, 15, 1132–1139. [Google Scholar] [CrossRef]
- Vyazovskiy, V.V.; Olcese, U.; Hanlon, E.C.; Nir, Y.; Cirelli, C.; Tononi, G. Local sleep in awake rats. Nature 2011, 472, 443–447. [Google Scholar] [CrossRef]
- Krueger, J.M.; Rector, D.M.; Roy, S.; Van Dongen, H.P.A.; Belenky, G.; Panksepp, J. Sleep as a fundamental property of neuronal assemblies. Nat. Rev. Neurosci. 2008, 9, 910–919. [Google Scholar] [CrossRef]
- Reilly, T.; Ekblom, B. The use of recovery methods post-exercise. J. Sports Sci. 2005, 23, 619–627. [Google Scholar] [CrossRef]
- Jensen, O.; Tesche, C.D. Frontal theta activity in humans increases with memory load in a working memory task. Eur. J. Neurosci. 2002, 15, 1395–1399. [Google Scholar] [CrossRef]
- Rydzik, Ł. The Comparison of the Level of Aggressiveness of Oyama Karate and Mixed Martial Art Fighters. Appl. Sci. 2022, 12, 8446. [Google Scholar] [CrossRef]
- Thompson, M.; Thompson, L. Neurofeedback. Wprowadzenie do Podstawowych Koncepcji Psychofizjologii Stosowanej; Biomed Neurotechnologie: Wrocław, Poland, 2012. [Google Scholar]
- Barry, R.J.; De Blasio, F.M. EEG differences between eyes—Closed and eyes-open resting conditions. Clin. Neurophysiol. 2007, 118, 2765–2773. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, E.; da Silva, F.L. Electroencephalography: Basic Principles, Clinical Applications, and Related Fields; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Klimesch, W. EEG alpha and theta oscillations reflect cognitive and memory performance: A review and analysis. Brain Res. Rev. 1999, 29, 169–195. [Google Scholar] [CrossRef] [PubMed]
- Barry, R.J.; Clarke, A.R.; Johnstone, S.J. A review of electrophysiology in attention-deficit/hyperactivity disorder: I. Qualitative and quantitative electroencephalography. Clin. Neurophysiol. 2003, 114, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Haufler, A.J.; Spalding, T.W.; Santa Maria, D.L.; Hatfield, B.D. Neuro-cognitive activity during a self-paced visuospatial task: Comparative EEG profiles in marksmen and novice shooters. Biol. Psychol. 2000, 53, 131–160. [Google Scholar] [CrossRef] [PubMed]
- Domingos, C.; da Silva, C.M.; Antunes, A.; Prazeres, P.; Esteves, I.; Rosa, A.C. The Influence of an Alpha Band Neurofeedback Training in Heart Rate Variability in Athletes. Int. J. Environ. Res. Public Health 2021, 18, 12579. [Google Scholar] [CrossRef]
- Schreckenberger, M.; Lange-Asschenfeld, C.; Lochmann, M.; Mann, K.; Siessmeier, T.; Buchholz, H.-G.; Bartenstein, P.; Gründer, G. The thalamus as the generator and modulator of EEG alpha rhythm: A combined PET/EEG study with lorazepam challenge in humans. Neuroimage 2004, 22, 637–644. [Google Scholar] [CrossRef]
- Vernon, D.; Egner, T.; Cooper, N.; Compton, T.; Neilands, C.; Sheri, A.; Gruzelier, J. The effect of training distinct neurofeedback protocols on aspects of cognitive performance. Int. J. Psychophysiol. 2003, 47, 75–85. [Google Scholar] [CrossRef]
- Egner, T.; Gruzelier, J.H. EEG Biofeedback of low beta band components: Frequency-specific effects on variables of attention and event-related brain potentials. Clin. Neurophysiol. 2004, 115, 131–139. [Google Scholar] [CrossRef]
- Budde, H.; Voelcker-Rehage, C.; Pietraßyk-Kendziorra, S.; Ribeiro, P.; Tidow, G. Acute coordinative exercise improves attentional performance in adolescents. Neurosci. Lett. 2008, 441, 219–223. [Google Scholar] [CrossRef]
- Rydzik, Ł.; Ambroży, T. Physical Fitness and the Level of Technical and Tactical Training of Kickboxers. Int. J. Environ. Res. Public Health 2021, 18, 3088. [Google Scholar] [CrossRef]
- Del Percio, C.; Brancucci, A.; Bergami, F.; Marzano, N.; Fiore, A.; Di Ciolo, E.; Aschieri, P.; Lino, A.; Vecchio, F.; Iacoboni, M.; et al. Cortical alpha rhythms are correlated with body sway during quiet open-eyes standing in athletes: A high-resolution EEG study. Neuroimage 2007, 36, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Rydzik, Ł.; Wąsacz, W.; Ambroży, T.; Pałka, T.; Sobiło-Rydzik, E.; Kopańska, M. Comparison of Head Strike Incidence under K1 Rules of Kickboxing with and without Helmet Protection—A Pilot Study. Int. J. Environ. Res. Public Health 2023, 20, 4713. [Google Scholar] [CrossRef] [PubMed]
- Azouvi, P.; Arnould, A.; Dromer, E.; Vallat-Azouvi, C. Neuropsychology of traumatic brain injury: An expert overview. Rev. Neurol. 2017, 173, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Ide, J.S.; Li, C.R. Resting-State Functional Connectivity of the Medial Superior Frontal Cortex. Cereb. Cortex 2012, 22, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, J.; Reinecke, K.; Liesen, H.; Weiss, M. Cortical activity of skilled performance in a complex sports related motor task. Eur. J. Appl. Physiol. 2008, 104, 625–631. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Training experience of at least 10 years | Neurological disorders |
| Current medical examinations | Skin diseases of the head |
| Participation in at least 5 competitions per year (having medal from national championship) | Cranio-Cerebral Injuries |
| Taking psychotropic drugs | |
| Injuries and severe knockouts |
| Delta 0.5–4 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 19.54 | 13.03 | 33.78 | 13.84 | 22.19 | 7.50 |
| F3 | 14.01 | 11.48 | 22.84 | 12.19 | 14.21 | 3.01 |
| F4 | 15.10 | 10.62 | 26.35 | 12.28 | 16.00 | 4.33 |
| p < 0.001 ES = 0.23 | ||||||
| Cz | 16.85 | 9.13 | 24.98 | 13.03 | 19.45 | 4.47 |
| C3 | 16.24 | 12.19 | 23.23 | 13.98 | 19.43 | 3.54 |
| C4 | 16.14 | 10.62 | 26.35 | 13.28 | 18.62 | 3.87 |
| p = 0.86 ES = 0.00 | ||||||
| Pz | 16.88 | 10.62 | 26.35 | 12.28 | 22.28 | 5.32 |
| P3 | 17.34 | 11.48 | 34.21 | 12.83 | 21.99 | 6.78 |
| P4 | 15.96 | 10.62 | 26.35 | 13.28 | 19.45 | 4.13 |
| p = 0.61 ES = 0.03 | ||||||
| Theta 4–8 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 13.83 | 9.19 | 27.55 | 11.77 | 14.91 | 4.20 |
| F3 | 12.56 | 9.88 | 17.19 | 11.78 | 13.70 | 1.86 |
| F4 | 12.99 | 9.90 | 18.37 | 11.91 | 14.37 | 2.14 |
| p = 0.34 ES = 0.06 | ||||||
| Cz | 9.08 | 6.69 | 11.67 | 7.38 | 10.10 | 1.66 |
| C3 | 8.58 | 6.59 | 11.10 | 7.63 | 10.59 | 1.69 |
| C4 | 8.91 | 5.78 | 11.78 | 6.71 | 11.78 | 2.48 |
| p = 0.51 ES = 0.04 | ||||||
| Pz | 8.53 | 5.14 | 10.62 | 6.85 | 10.62 | 2.11 |
| P3 | 8.99 | 6.01 | 10.93 | 7.54 | 10.12 | 1.68 |
| P4 | 8.38 | 5.08 | 10.08 | 7.25 | 10.08 | 1.85 |
| p = 0.36 ES = 0.06 | ||||||
| Alpha 8–12 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 8.77 | 6.31 | 14.34 | 6.87 | 9.31 | 2.77 |
| F3 | 7.81 | 5.45 | 11.56 | 6.77 | 7.58 | 1.89 |
| F4 | 10.13 | 5.58 | 35.37 | 6.11 | 10.12 | 7.33 |
| p = 0.27 ES = 0.08 | ||||||
| Cz | 10.30 | 5.58 | 18.58 | 7.53 | 10.70 | 4.17 |
| C3 | 11.02 | 5.34 | 19.79 | 8.34 | 16.71 | 4.42 |
| C4 | 10.64 | 7.01 | 19.88 | 7.14 | 16.18 | 4.40 |
| p = 0.71 ES = 0.03 | ||||||
| Pz | 8.26 | 4.69 | 12.07 | 6.18 | 9.94 | 2.32 |
| P3 | 9.22 | 4.68 | 13.09 | 7.68 | 11.69 | 2.62 |
| P4 | 8.43 | 4.60 | 11.98 | 7.08 | 9.94 | 2.33 |
| p = 0.21 ES = 0.08 | ||||||
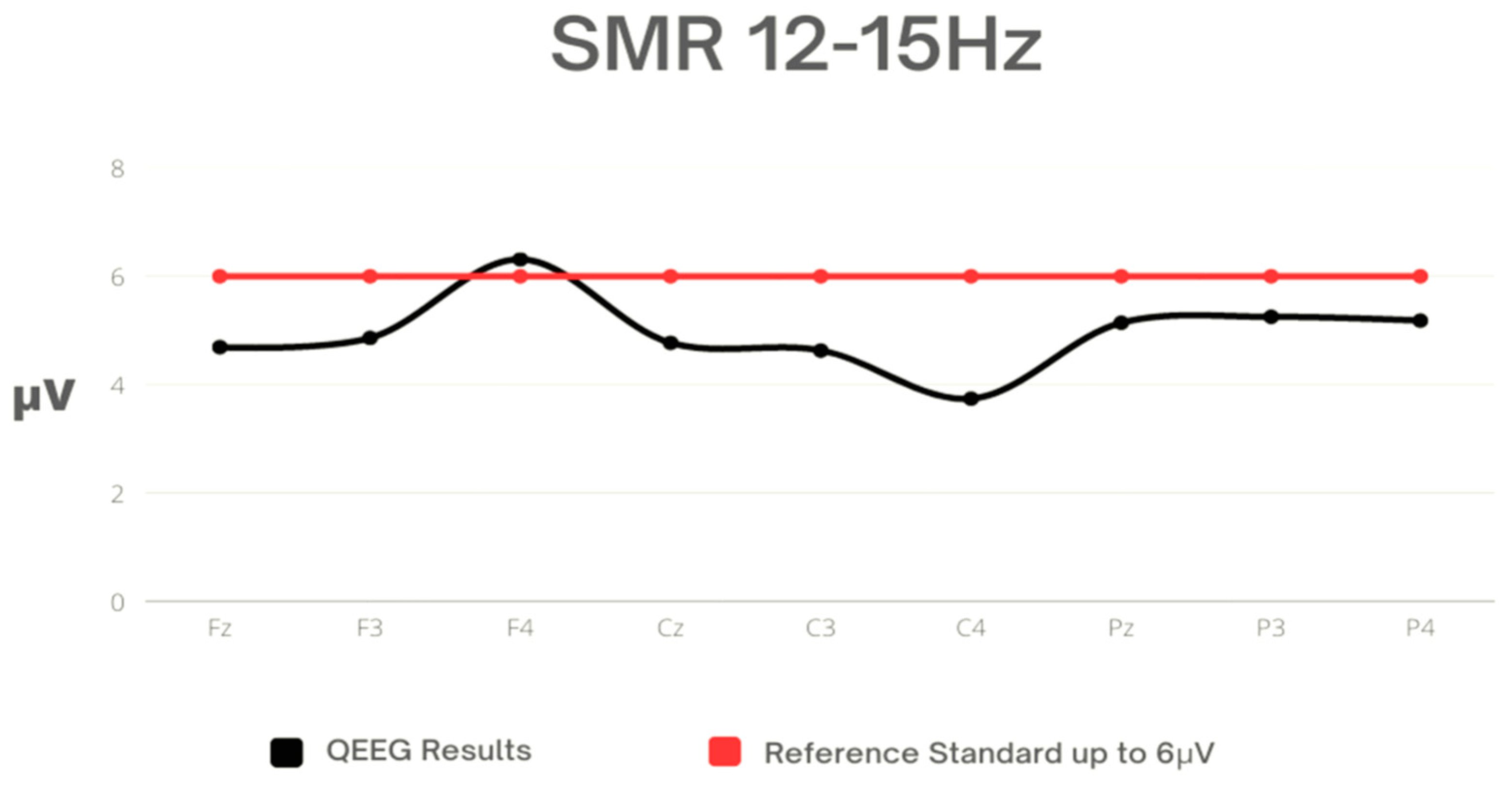
| SMR 12–15 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 4.69 | 3.74 | 6.14 | 4.00 | 5.08 | 0.81 |
| F3 | 4.86 | 0.87 | 3.67 | 6.11 | 3.83 | 5.31 |
| F4 | 6.31 | 4.37 | 3.12 | 15.64 | 3.58 | 5.25 |
| p = 0.60 ES = 0.03 | ||||||
| Cz | 4.77 | 3.02 | 7.02 | 3.68 | 5.39 | 1.11 |
| C3 | 4.63 | 4.21 | 7.58 | 4.27 | 4.59 | 0.76 |
| C4 | 3.74 | 3.21 | 5.41 | 3.45 | 3.92 | 0.49 |
| p = 0.002 ES = 0.29 | ||||||
| Pz | 5.14 | 3.47 | 7.38 | 4.18 | 5.76 | 1.28 |
| P3 | 5.25 | 3.47 | 8.80 | 4.39 | 5.80 | 1.45 |
| P4 | 5.18 | 3.18 | 9.18 | 3.58 | 5.66 | 1.76 |
| p = 0.97 ES = 0.001 | ||||||
| Beta 15–20 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 5.33 | 4.50 | 6.59 | 5.03 | 5.63 | 0.67 |
| F3 | 6.48 | 4.98 | 9.77 | 5.60 | 6.77 | 1.61 |
| F4 | 8.05 | 4.09 | 19.30 | 5.58 | 6.69 | 5.25 |
| p = 0.02 ES = 0.20 | ||||||
| Cz | 5.76 | 4.81 | 7.59 | 5.20 | 6.19 | 0.94 |
| C3 | 6.04 | 4.80 | 7.83 | 5.38 | 6.93 | 1.06 |
| C4 | 5.44 | 4.21 | 6.88 | 4.82 | 6.27 | 0.92 |
| p < 0.001 ES = 0.61 | ||||||
| Pz | 5.59 | 4.21 | 7.51 | 4.44 | 6.35 | 1.06 |
| P3 | 6.49 | 4.91 | 7.96 | 5.89 | 7.44 | 1.04 |
| P4 | 5.66 | 4.43 | 7.51 | 4.44 | 6.35 | 1.11 |
| p = 0.01 ES = 0.22 | ||||||
| Beta2 20–35 Hz | Mean | Min | Max | Q1 | Q3 | SD |
|---|---|---|---|---|---|---|
| Fz | 6.70 | 5.66 | 7.96 | 6.16 | 7.31 | 0.77 |
| F3 | 8.39 | 6.06 | 14.67 | 7.31 | 9.41 | 2.01 |
| F4 | 9.40 | 5.21 | 15.27 | 7.08 | 11.17 | 2.70 |
| p < 0.001 ES = 0.43 | ||||||
| Cz | 6.97 | 5.18 | 9.25 | 6.25 | 7.49 | 0.86 |
| C3 | 7.40 | 6.14 | 9.82 | 6.40 | 7.64 | 1.00 |
| C4 | 7.63 | 6.38 | 9.28 | 6.69 | 7.89 | 0.86 |
| p = 0.04 ES = 0.17 | ||||||
| Pz | 7.35 | 6.18 | 9.28 | 6.69 | 7.81 | 0.83 |
| P3 | 8.21 | 6.79 | 9.29 | 7.46 | 8.79 | 0.80 |
| P4 | 8.21 | 5.85 | 9.56 | 7.15 | 8.79 | 0.94 |
| p = 0.002 ES = 0.31 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rydzik, Ł.; Pałka, T.; Sobiło-Rydzik, E.; Tota, Ł.; Ambroży, D.; Ambroży, T.; Ruzbarsky, P.; Czarny, W.; Kopańska, M. An Attempt to Develop a Model of Brain Waves Using Quantitative Electroencephalography with Closed Eyes in K1 Kickboxing Athletes—Initial Concept. Sensors 2023, 23, 4136. https://doi.org/10.3390/s23084136
Rydzik Ł, Pałka T, Sobiło-Rydzik E, Tota Ł, Ambroży D, Ambroży T, Ruzbarsky P, Czarny W, Kopańska M. An Attempt to Develop a Model of Brain Waves Using Quantitative Electroencephalography with Closed Eyes in K1 Kickboxing Athletes—Initial Concept. Sensors. 2023; 23(8):4136. https://doi.org/10.3390/s23084136
Chicago/Turabian StyleRydzik, Łukasz, Tomasz Pałka, Ewa Sobiło-Rydzik, Łukasz Tota, Dorota Ambroży, Tadeusz Ambroży, Pavel Ruzbarsky, Wojciech Czarny, and Marta Kopańska. 2023. "An Attempt to Develop a Model of Brain Waves Using Quantitative Electroencephalography with Closed Eyes in K1 Kickboxing Athletes—Initial Concept" Sensors 23, no. 8: 4136. https://doi.org/10.3390/s23084136
APA StyleRydzik, Ł., Pałka, T., Sobiło-Rydzik, E., Tota, Ł., Ambroży, D., Ambroży, T., Ruzbarsky, P., Czarny, W., & Kopańska, M. (2023). An Attempt to Develop a Model of Brain Waves Using Quantitative Electroencephalography with Closed Eyes in K1 Kickboxing Athletes—Initial Concept. Sensors, 23(8), 4136. https://doi.org/10.3390/s23084136