


Feasibility of 3D Body Tracking from Monocular 2D Video Feeds in Musculoskeletal Telerehabilitation

 ,
, 
Abstract
:1. Introduction
2. Background
3. Materials and Methods
3.1. Experimental Design
3.2. Experimental Data Acquisition
3.3. Data Preprocessing
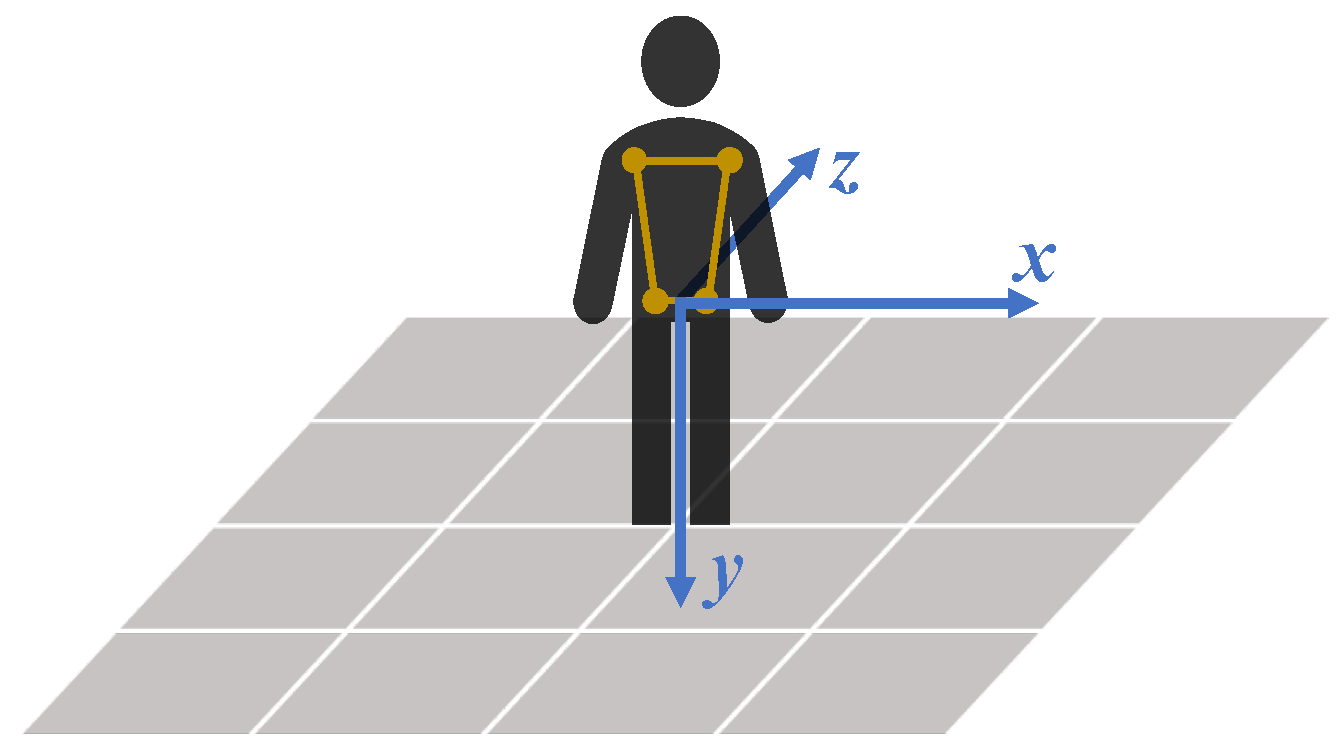
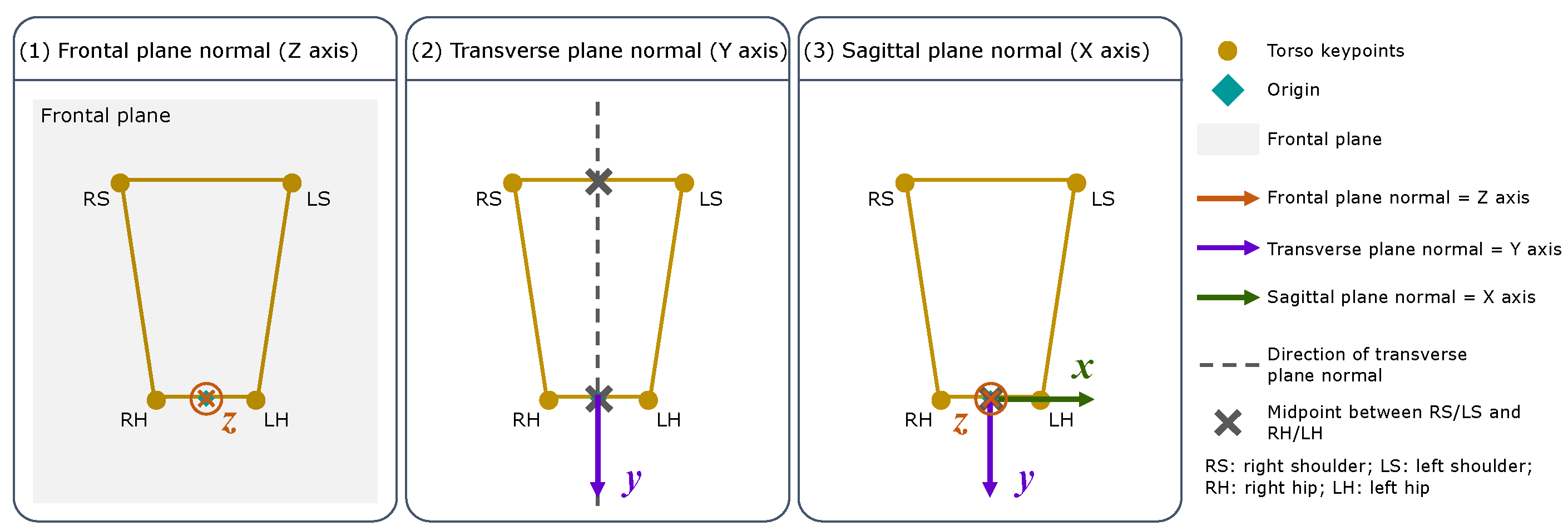
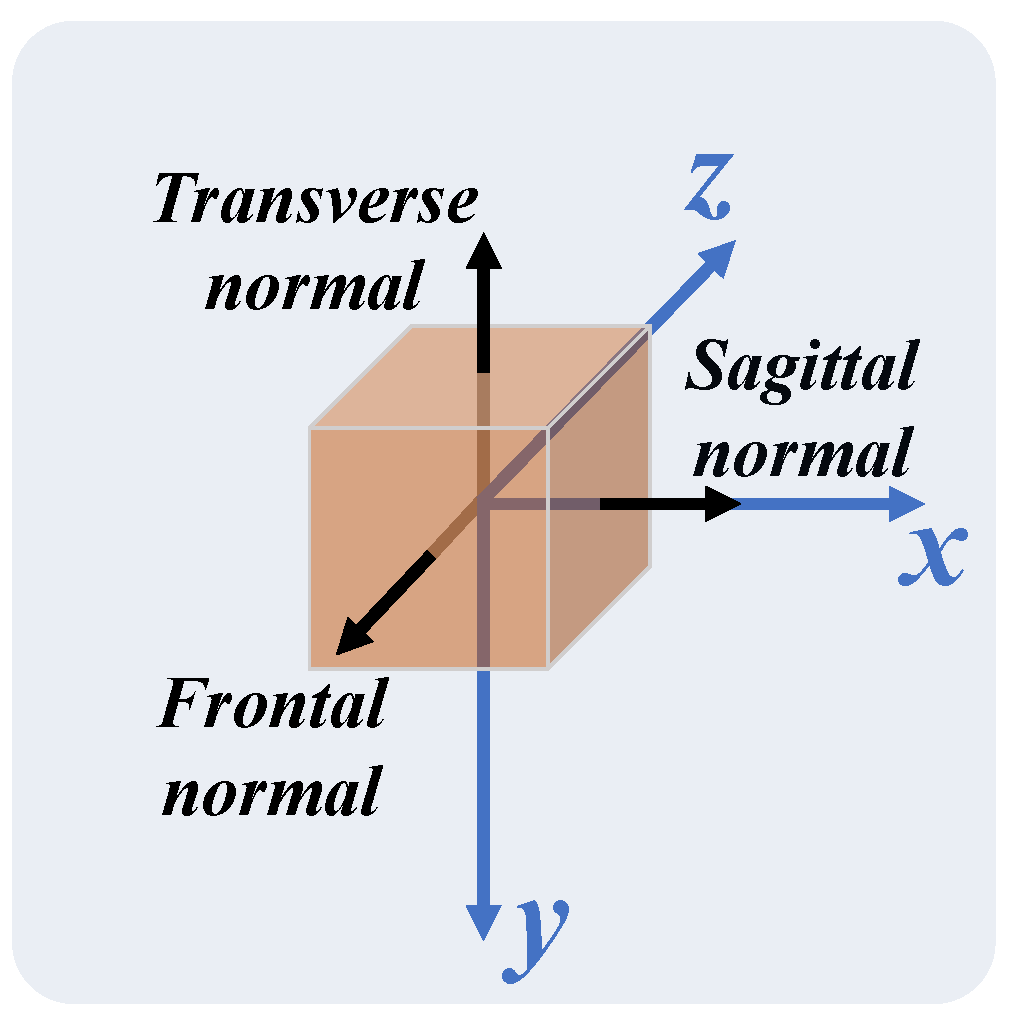
3.3.1. 3D Cartesian Coordinate System
3.3.2. Amplitude Calculation
3.3.3. Data Alignment
3.4. Evaluation Metrics
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HPE | Human Pose Estimation |
| MoCap | Motion Capture |
| ROM | Range of Motion |
| FPS | Frames per Second |
| SF | Shoulder Flexion/Extension |
| SA | Shoulder Abduction/Adduction |
| EF | Elbow Flexion/Extension |
| SP | Shoulder Press |
| HA | Hip Abduction/Adduction |
| SQ | Squat |
| MCH | March |
| SKF | Seated Knee Flexion/Extension |
| MAE | Mean Absolute Error |
| MAPE | Mean Absolute Percentage Error |
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Vieira, L.M.S.M.d.A.; de Andrade, M.A.; Sato, T.d.O. Telerehabilitation for musculoskeletal pain–An overview of systematic reviews. Digit. Health 2023, 9, 20552076231164242. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; Russell, T.G. Telehealth for musculoskeletal physiotherapy. Musculoskelet. Sci. Pract. 2020, 48, 102193. [Google Scholar] [CrossRef]
- Areias, A.C.; Costa, F.; Janela, D.; Molinos, M.; Moulder, R.G.; Lains, J.; Scheer, J.K.; Bento, V.; Yanamadala, V.; Correia, F.D. Long-term clinical outcomes of a remote digital musculoskeletal program: An ad hoc analysis from a longitudinal study with a non-participant comparison group. Healthcare 2022, 10, 2349. [Google Scholar] [CrossRef] [PubMed]
- Dias, G.; Adrião, M.L.; Clemente, P.; da Silva, H.P.; Chambel, G.; Pinto, J.F. Effectiveness of a Gamified and Home-Based Approach for Upper-limb Rehabilitation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Scotland, UK, 11–15 July 2022; pp. 2602–2605. [Google Scholar]
- Khan, M.H.; Zöller, M.; Farid, M.S.; Grzegorzek, M. Marker-based movement analysis of human body parts in therapeutic procedure. Sensors 2020, 20, 3312. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, H.M. Musculoskeletal Assessment-Joint Motion and Muscle Testing; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Alarcón-Aldana, A.C.; Callejas-Cuervo, M.; Bo, A.P.L. Upper limb physical rehabilitation using serious videogames and motion capture systems: A systematic review. Sensors 2020, 20, 5989. [Google Scholar] [CrossRef] [PubMed]
- Correia, F.D.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Molinos, M.; Teixeira, L.; Pires, J.; Seabra, R.; et al. Digital versus conventional rehabilitation after total hip arthroplasty: A single-center, parallel-group pilot study. JMIR Rehabil. Assist. Technol. 2019, 6, e14523. [Google Scholar] [CrossRef] [PubMed]
- Correia, F.D.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Molinos, M.; Teixeira, L.; Tulha, J.; Seabra, R.; et al. Medium-term outcomes of digital versus conventional home-based rehabilitation after total knee arthroplasty: Prospective, parallel-group feasibility study. Jmir Rehabil. Assist. Technol. 2019, 6, e13111. [Google Scholar] [CrossRef]
- Pinto, J.F.; Carvalho, H.R.; Chambel, G.R.; Ramiro, J.; Goncalves, A. Adaptive gameplay and difficulty adjustment in a gamified upper-limb rehabilitation. In Proceedings of the IEEE International Conference on Serious Games and Applications for Health (SeGAH), Vienna, Austria, 16–18 May 2018; pp. 1–8. [Google Scholar]
- Zheng, C.; Wu, W.; Chen, C.; Yang, T.; Zhu, S.; Shen, J.; Kehtarnavaz, N.; Shah, M. Deep learning-based human pose estimation: A survey. ACM Comput. Surv. 2023, 56, 1–37. [Google Scholar] [CrossRef]
- Milosevic, B.; Leardini, A.; Farella, E. Kinect and wearable inertial sensors for motor rehabilitation programs at home: State of the art and an experimental comparison. Biomed. Eng. Online 2020, 19, 1–26. [Google Scholar] [CrossRef]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I. A review of the evolution of vision-based motion analysis and the integration of advanced computer vision methods towards developing a markerless system. Sport Med.-Open 2018, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kadambi, A.; Bhandari, A.; Raskar, R. 3D Depth Cameras in Vision: Benefits and Limitations of the Hardware: With an Emphasis on the First-and Second-Generation Kinect Models. Comput. Vis. Mach. Learn. RGB-D Sens. 2014, 3–26. [Google Scholar] [CrossRef]
- Hellsten, T.; Karlsson, J.; Shamsuzzaman, M.; Pulkkis, G. The Potential of Computer Vision-Based Markerless Human Motion Analysis for Rehabilitation. Rehabil. Process. Outcome 2021, 10, 11795727211022330. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Yang, B.; Wang, B.; Yan, W.; Tan, R.T. Occlusion-aware networks for 3D human pose estimation in video. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Republic of Korea, 27 October–2 November 2019; pp. 723–732. [Google Scholar]
- Mehta, D.; Sotnychenko, O.; Mueller, F.; Xu, W.; Elgharib, M.; Fua, P.; Seidel, H.; Rhodin, H.; Pons-Moll, G.; Theobalt, C. XNect: Real-time multi-person 3D motion capture with a single RGB camera. ACM Trans. Graph. (TOG) 2020, 39, 82:1–82:17. [Google Scholar] [CrossRef]
- Kendall, A.; Grimes, M.; Cipolla, R. PoseNet: A convolutional network for real-time 6-DOF camera relocalization. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 2938–2946. [Google Scholar]
- Bajpai, R.; Joshi, D. MoveNet: A deep neural network for joint profile prediction across variable walking speeds and slopes. IEEE Trans. Instrum. Meas. 2021, 70, 1–11. [Google Scholar]
- Fang, H.S.; Li, J.; Tang, H.; Xu, C.; Zhu, H.; Xiu, Y.; Li, Y.L.; Lu, C. AlphaPose: Whole-body regional multi-person pose estimation and tracking in real-time. IEEE Trans. Pattern Anal. Mach. Intell. 2022, 45, 7157–7173. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Simon, T.; Wei, S.E.; Sheikh, Y. Realtime multi-person 2D pose estimation using part affinity fields. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 7291–7299. [Google Scholar]
- Bazarevsky, V.; Grishchenko, I.; Raveendran, K.; Zhu, T.; Zhang, F.; Grundmann, M. BlazePose: On-device real-time body pose tracking. arXiv 2020, arXiv:2006.10204. [Google Scholar]
- Bolaños, C.; Fernández-Bermejo, J.; Dorado, J.; Agustín, H.; Villanueva, F.J.; Santofimia, M.J. A comparative analysis of pose estimation models as enablers for a smart-mirror physical rehabilitation system. Procedia Comput. Sci. 2022, 207, 2536–2545. [Google Scholar] [CrossRef]
- Huang, Y.P.; Chou, Y.J.; Lee, S.H. An OpenPose-based System for Evaluating Rehabilitation Actions in Parkinson’s Disease. In Proceedings of the International Automatic Control Conference (CACS), Kaohsiung, Taiwan, 3–6 November 2022; pp. 1–6. [Google Scholar]
- Lv, X.; Ta, N.; Chen, T.; Zhao, J.; Wei, H. Analysis of Gait Characteristics of Patients with Knee Arthritis Based on Human Posture Estimation. Biomed Res. Int. 2022, 2022, 7020804. [Google Scholar] [CrossRef]
- Marusic, A.; Nguyen, S.M.; Tapus, A. Evaluating Kinect, OpenPose and BlazePose for Human Body Movement Analysis on a Low Back Pain Physical Rehabilitation Dataset. In Proceedings of the Companion of the 2023 ACM/IEEE International Conference on Human-Robot Interaction, Stockholm, Sweden, 13–16 March 2023; pp. 587–591. [Google Scholar]
- Mehta, D.; Sridhar, S.; Sotnychenko, O.; Rhodin, H.; Shafiei, M.; Seidel, H.P.; Xu, W.; Casas, D.; Theobalt, C. Vnect: Real-time 3D human pose estimation with a single RGB camera. ACM Trans. Graph. (TOG) 2017, 36, 1–14. [Google Scholar] [CrossRef]
- Xu, H.; Bazavan, E.G.; Zanfir, A.; Freeman, W.T.; Sukthankar, R.; Sminchisescu, C. Ghum & Ghuml: Generative 3D human shape and articulated pose models. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 6184–6193. [Google Scholar]
- Ionescu, C.; Papava, D.; Olaru, V.; Sminchisescu, C. Human3.6M: Large scale datasets and predictive methods for 3D human sensing in natural environments. IEEE Trans. Pattern Anal. Mach. Intell. 2013, 36, 1325–1339. [Google Scholar] [CrossRef] [PubMed]
- Fischler, M.A.; Bolles, R.C. Random sample consensus: A paradigm for model fitting with applications to image analysis and automated cartography. Commun. ACM 1981, 24, 381–395. [Google Scholar] [CrossRef]
- Asuero, A.G.; Sayago, A.; González, A. The correlation coefficient: An overview. Crit. Rev. Anal. Chem. 2006, 36, 41–59. [Google Scholar] [CrossRef]
- Xia, P.; Zhang, L.; Li, F. Learning similarity with cosine similarity ensemble. Inf. Sci. 2015, 307, 39–52. [Google Scholar] [CrossRef]
- Lewis, C.D. Industrial and Business Forecasting Methods: A Practical Guide to Exponential Smoothing and Curve Fitting; Butterworth Scientific: Boston, MA, USA, 1982. [Google Scholar] [CrossRef]
- Slowik, J.S.; McCutcheon, T.W.; Lerch, B.G.; Fleisig, G.S. Comparison of a Single-view Image-based System to a Multi-camera Marker-based System for Human Static Pose Estimation. J. Biomech. 2023, 159, 111746. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, C.; Dong, W.; Fan, B. A survey on depth ambiguity of 3D human pose estimation. Appl. Sci. 2022, 12, 10591. [Google Scholar] [CrossRef]
- Qiu, Z.; Qiu, K.; Fu, J.; Fu, D. Weakly-supervised pre-training for 3D human pose estimation via perspective knowledge. Pattern Recognit. 2023, 139, 109497. [Google Scholar] [CrossRef]
- Zhang, D.; Wu, Y.; Guo, M.; Chen, Y. Deep learning methods for 3D human pose estimation under different supervision paradigms: A survey. Electronics 2021, 10, 2267. [Google Scholar] [CrossRef]
- Liu, Z.; Zhu, J.; Bu, J.; Chen, C. A survey of human pose estimation: The body parts parsing based methods. J. Vis. Commun. Image Represent. 2015, 32, 10–19. [Google Scholar] [CrossRef]
- Hossain, M.R.I. Understanding the Sources of Error for 3D Human Pose Estimation from Monocular Images and Videos. Ph.D. Thesis, University of British Columbia, Kelowna, BC, Canada, 2017. [Google Scholar]
- Andriluka, M.; Pishchulin, L.; Gehler, P.; Schiele, B. 2D human pose estimation: New benchmark and state of the art analysis. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 3686–3693. [Google Scholar]
- Barré, A.; Thiran, J.P.; Jolles, B.M.; Theumann, N.; Aminian, K. Soft tissue artifact assessment during treadmill walking in subjects with total knee arthroplasty. IEEE Trans. Biomed. Eng. 2013, 60, 3131–3140. [Google Scholar] [CrossRef]
- Moro, M.; Marchesi, G.; Hesse, F.; Odone, F.; Casadio, M. Markerless vs. marker-based gait analysis: A proof of concept study. Sensors 2022, 22, 2011. [Google Scholar] [CrossRef] [PubMed]
- Seber, G.A.; Lee, A.J. Polynomial regression. In Linear Regression Analysis; Wiley Series in Probability and Statistics; John Wiley & Sons: Hoboken, NJ, USA, 2003; pp. 165–185. [Google Scholar] [CrossRef]
- Fieraru, M.; Zanfir, M.; Pirlea, S.C.; Olaru, V.; Sminchisescu, C. AIFit: Automatic 3D Human-Interpretable Feedback Models for Fitness Training. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Nashville, TN, USA, 20–25 June 2021; pp. 9919–9928. [Google Scholar]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
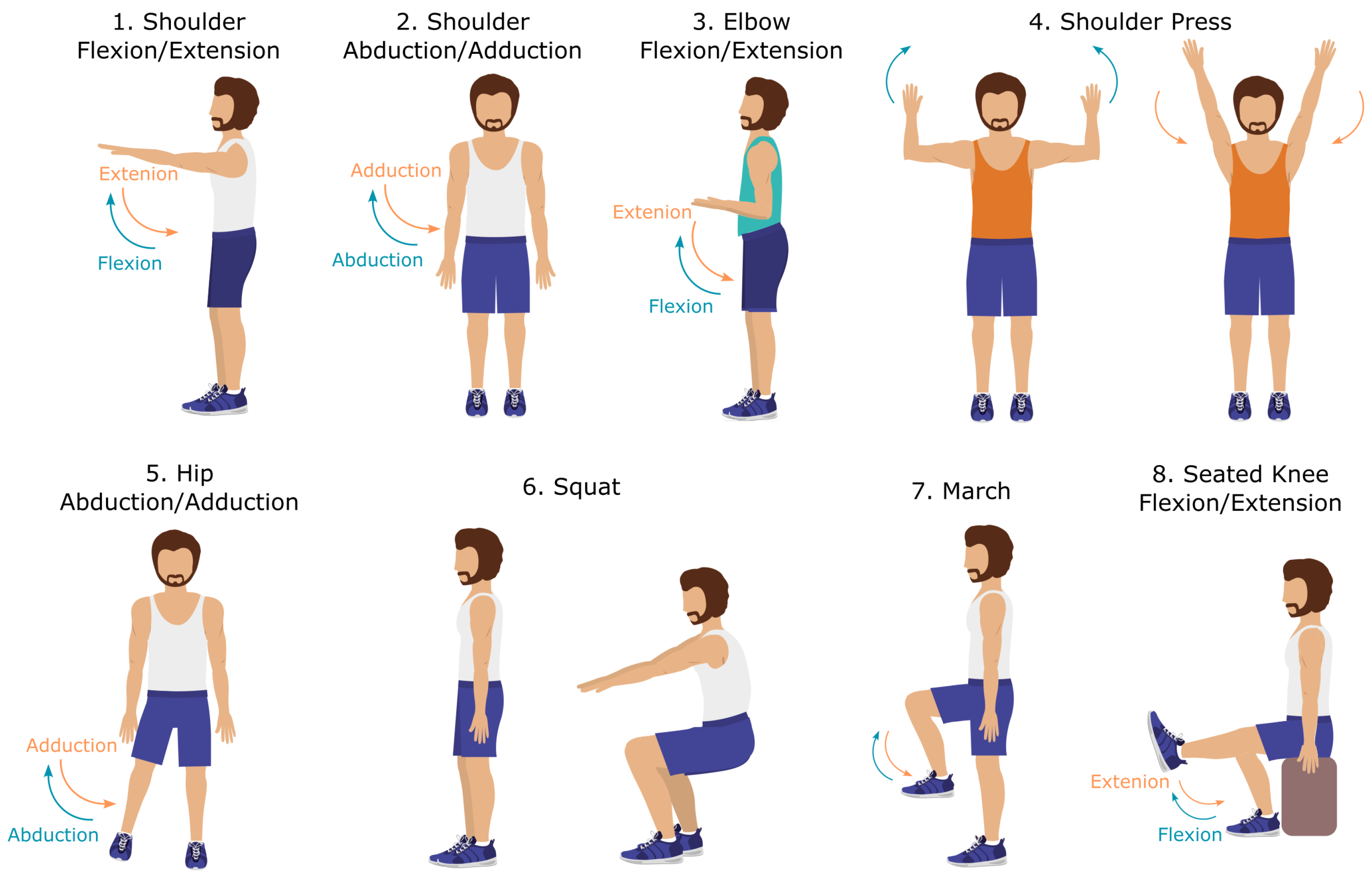
| Exercises | Limb in Motion | Plane of Movement | Evaluated Joint |
|---|---|---|---|
| 1. Shoulder Flexion/Extension (SF) | Right arm | Sagittal | Right shoulder |
| 2. Shoulder Abduction/Adduction (SA) | Right arm | Frontal | Right shoulder |
| 3. Elbow Flexion/Extension (EF) | Arms (bilateral) | Sagittal | Right elbow |
| 4. Shoulder Press (SP) | Arms (bilateral) | Frontal | Right shoulder |
| 5. Hip Abduction/Adduction (HA) | Right leg | Frontal | Right hip |
| 6. Squat (SQ) | Legs (bilateral) | Sagittal | Right knee |
| 7. March (MCH) | Legs (bilateral) | Sagittal | Right hip |
| 8. Seated Knee Flexion/Extension (SKF) | Right leg | Sagittal | Right knee |
| MoCap Anatomical Location | Joint |
|---|---|
| 1. Acromion | Shoulder |
| 2. Lateral epicondyle of humerus | Elbow |
| 3. Styloid apophysis of radius | Wrist |
| 4. Greater trochanter | Hip |
| 5. Lateral epicondyle of the femur | Knee |
| 6. Lateral malleolus of the ankle | Ankle |
| Exercises | Plane of Movement | Body Segment (Joint 1–Joint 2) | Reference Direction |
|---|---|---|---|
| 1. SF | Sagittal | Shoulder–elbow | ↓ |
| 2. SA | Frontal | Shoulder–elbow | ↓ |
| 3. EF | Sagittal | Elbow–wrist | ↓ |
| 4. SP | Frontal | Shoulder–elbow | ↓ |
| 5. HA | Frontal | Hip–knee | ↓ |
| 6. SQ | Sagittal | Knee–hip | Foot-knee |
| 7. MCH | Sagittal | Hip–knee | ↓ |
| 8. SKF | Sagittal | Knee–foot | ↓ |
| Exercise | Peak Amplitudes | Motion Amplitudes (Threshold = 1°) | ||
|---|---|---|---|---|
| MAE (°) | MAPE (%) | MAE (°) | MAPE (%) | |
| 1. SF (s) | 28.8 | 28.7 | 15.6 | 66.60 |
| 2. SA (f) | 13.0 | 10.2 | 7.7 | 14.90 |
| 3. EF (s) | 11.7 | 9.6 | 10.6 | 24.2 |
| 4. SP (f) | 13.8 | 9.5 | 18.7 | 23.0 |
| 5. HA (f) | 3.7 | 9.0 | 3.2 | 62.9 |
| 6. SQ (s) | 7.6 | 7.9 | 8.3 | 25.0 |
| 7. MCH (s) | 6.3 | 7.7 | 6.3 | 107.4 |
| 8. SKF (s) | 4.9 | 6.6 | 9.9 | 78.10 |
| Exercise | Peak Amplitudes | Motion Amplitudes | ||
|---|---|---|---|---|
| cos_sim | cos_sim | |||
| 1. SF (s) | 0.894 | 0.992 | 0.904 | 0.949 |
| 2. SA (f) | 0.939 | 0.999 | 0.996 | 0.999 |
| 3. EF (s) | 0.903 | 0.997 | 0.963 | 0.990 |
| 4. SP (f) | 0.744 | 0.999 | 0.985 | 0.997 |
| 5. HA (f) | 0.915 | 0.995 | 0.985 | 0.987 |
| 6. SQ (s) | 0.833 | 0.998 | 0.981 | 0.993 |
| 7. MCH (s) | 0.961 | 0.996 | 0.964 | 0.979 |
| 8. SKF (s) | 0.765 | 0.997 | 0.942 | 0.961 |
| Exercise | Motion Amplitudes | |||
|---|---|---|---|---|
| Slope | Intercept | Curve Shape | ||
| 1. SF (s) | 0.75 | 11.3 | 0.82 | Not linear |
| 2. SA (f) | 0.89 | 1.72 | 0.99 | Linear |
| 3. EF (s) | 1.23 | −11.86 | 0.93 | Not linear |
| 4. SP (f) | 0.96 | −14.2 | 0.97 | Linear |
| 5. HA (f) | 0.92 | 3.39 | 0.97 | Linear |
| 6. SQ (s) | 1.05 | 5.12 | 0.96 | Linear |
| 7. MCH (s) | 1.03 | −0.82 | 0.93 | Linear |
| 8. SKF (s) | 1.13 | −4.19 | 0.89 | Not linear |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemente, C.; Chambel, G.; Silva, D.C.F.; Montes, A.M.; Pinto, J.F.; Silva, H.P.d. Feasibility of 3D Body Tracking from Monocular 2D Video Feeds in Musculoskeletal Telerehabilitation. Sensors 2024, 24, 206. https://doi.org/10.3390/s24010206
Clemente C, Chambel G, Silva DCF, Montes AM, Pinto JF, Silva HPd. Feasibility of 3D Body Tracking from Monocular 2D Video Feeds in Musculoskeletal Telerehabilitation. Sensors. 2024; 24(1):206. https://doi.org/10.3390/s24010206
Chicago/Turabian StyleClemente, Carolina, Gonçalo Chambel, Diogo C. F. Silva, António Mesquita Montes, Joana F. Pinto, and Hugo Plácido da Silva. 2024. "Feasibility of 3D Body Tracking from Monocular 2D Video Feeds in Musculoskeletal Telerehabilitation" Sensors 24, no. 1: 206. https://doi.org/10.3390/s24010206
APA StyleClemente, C., Chambel, G., Silva, D. C. F., Montes, A. M., Pinto, J. F., & Silva, H. P. d. (2024). Feasibility of 3D Body Tracking from Monocular 2D Video Feeds in Musculoskeletal Telerehabilitation. Sensors, 24(1), 206. https://doi.org/10.3390/s24010206