

Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability


Abstract
:1. Introduction
2. The Proposed Method
2.1. Conceptual Model
2.2. Participants and Equipment
2.3. Task


2.4. Experimental Protocol
2.5. Metric Extraction and Statistical Analysis
2.5.1. Pupil-Diameter Extraction
2.5.2. Heart-Rate-Variability Extraction
3. Results
3.1. Physiological Metrics
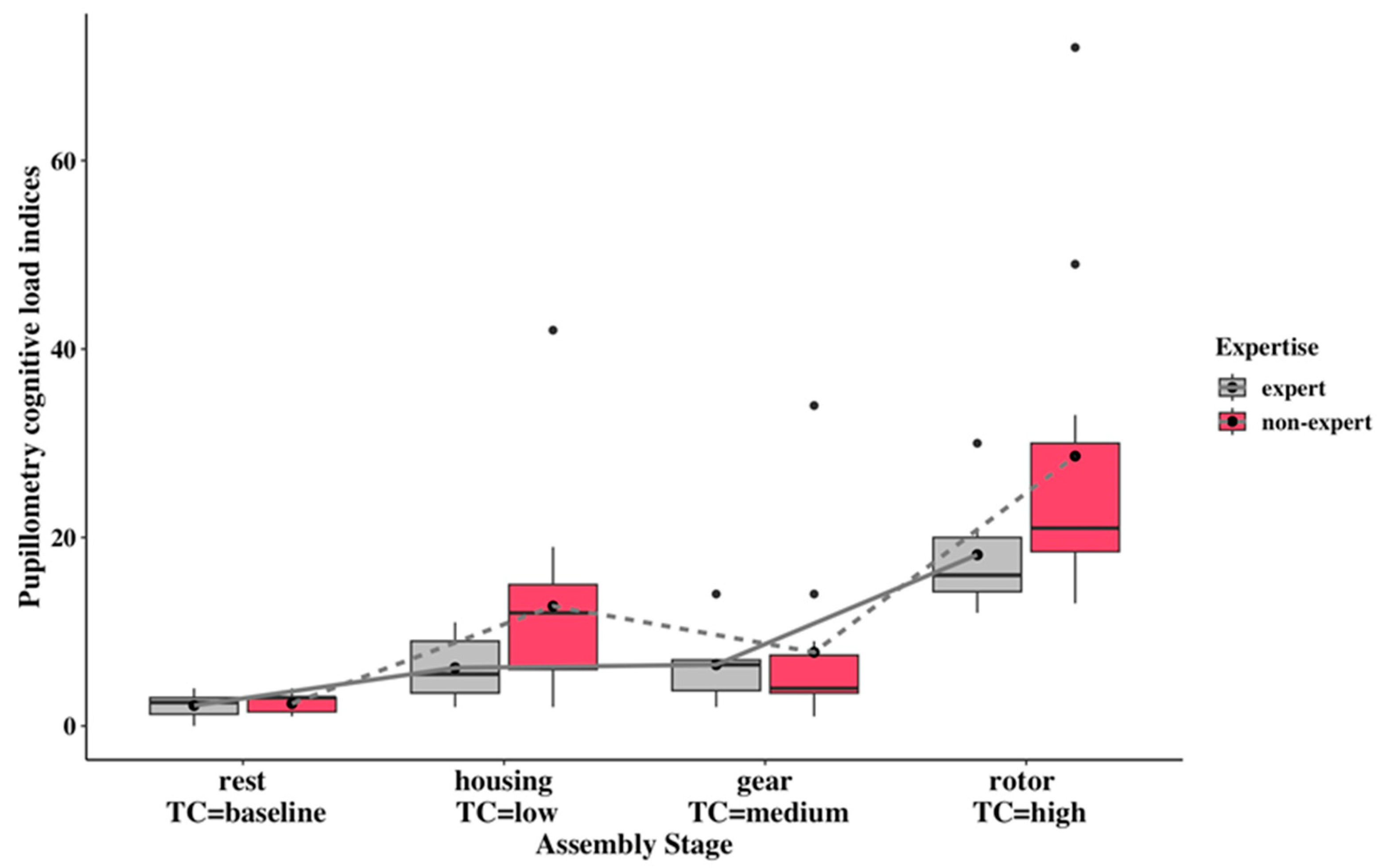
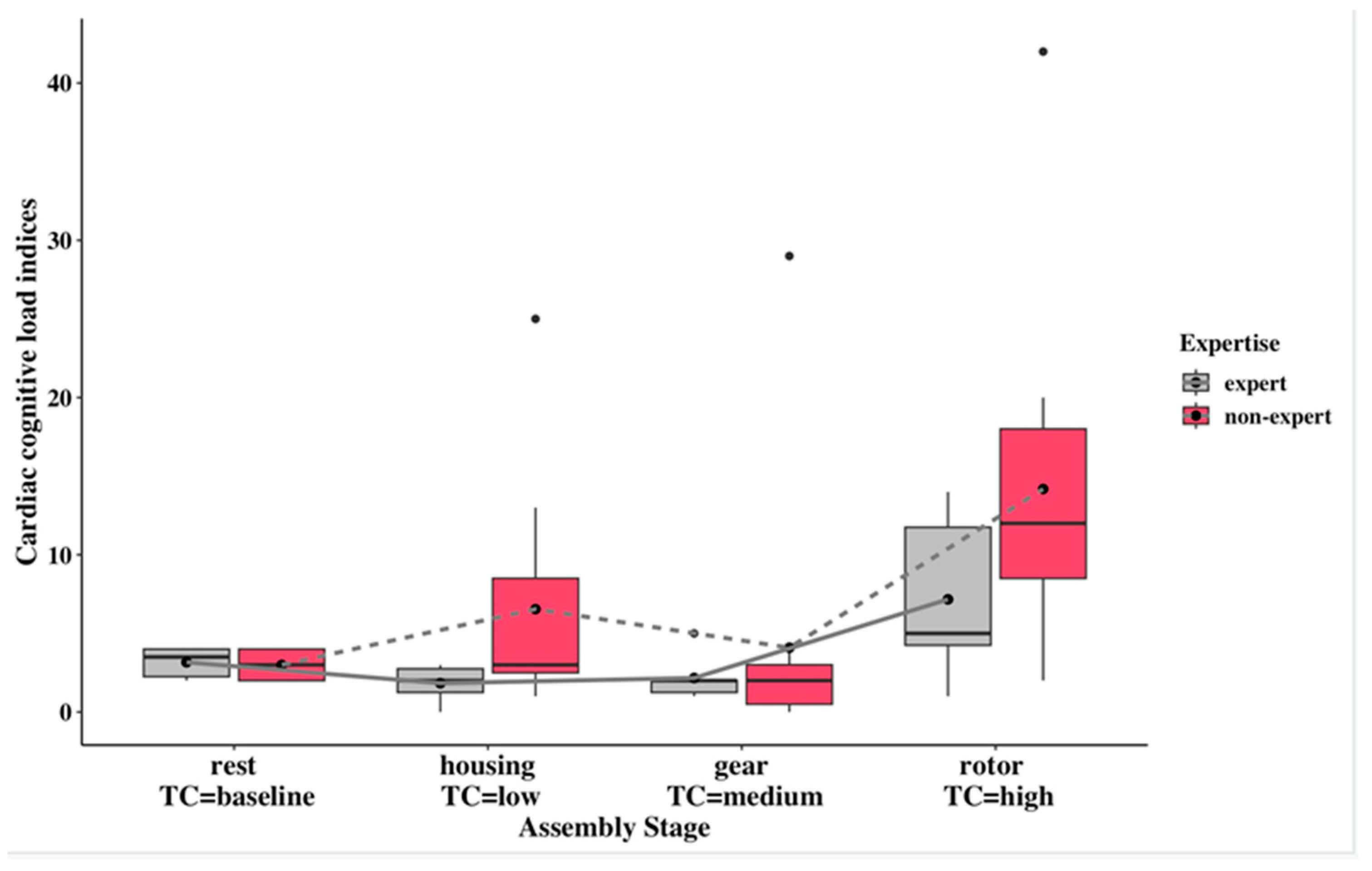
3.2. Cognitive-Workload Indices
3.3. Statistical Analysis for Cognitive-Workload Indices
3.4. Task Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romero, D.; Stahre, J.; Wuest, T.; Noran, O.; Bernus, P.; Fast-Berglund, Å.; Gorecky, D. Towards an Operator 4.0 Typology: A Human-Centric Perspective on the Fourth Industrial Revolution Technologies. In Proceedings of the International Conference on Computers & Industrial Engineering (CIE46), Tianjin, China, 29–31 October 2016; pp. 1–11. [Google Scholar]
- Yan, S.; Wei, Y.; Li, F.; Tran, C.C. Develop a Comprehensive Method to Evaluate the Mental Workload of Ship Operators. J. Mar. Sci. Eng. 2022, 10, 1133. [Google Scholar] [CrossRef]
- Singh, G.; Chanel, C.P.C.; Roy, R.N. Mental Workload Estimation Based on Physiological Features for Pilot-UAV Teaming Applications. Front. Hum. Neurosci. 2021, 15, 692878. [Google Scholar] [CrossRef]
- Paxion, J.; Galy, E.; Berthelon, C. Mental Workload and Driving. Front. Psychol. 2014, 5, 1344. [Google Scholar] [CrossRef]
- Umair Iqbal, M.; Srinivasan, B.; Srinivasan, R. Dynamic Assessment of Control Room Operator’s Cognitive Workload Using Electroencephalography (EEG). Comput. Chem. Eng. 2020, 141, 106726. [Google Scholar] [CrossRef]
- Brookhuis, K.A.; de Waard, D. Assessment of Drivers’ Workload: Performance and Subjective and Physiological Indexes. In Stress, Workload, and Fatigue; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar] [CrossRef]
- Wimisberg, J. Situation Awareness in Dynamic Decision Making: Effects of Practice and Working Memory. J. Cogn. Eng. Decis. Mak. 2007, 1, 56–74. [Google Scholar] [CrossRef]
- Kompier, M.A.; Aust, B.; van den Berg, A.M.; Siegrist, J. Stress Prevention in Bus Drivers: Evaluation of 13 Natural Experiments. J. Occup. Health Psychol. 2000, 5, 11–31. [Google Scholar] [CrossRef]
- Research and Innovation European Commission. Industry 5.0. Available online: https://research-and-innovation.ec.europa.eu/research-area/industrial-research-and-innovation/industry-50_en (accessed on 18 August 2023).
- Kong, X.T.R.; Luo, H.; Huang, G.Q.; Yang, X. Industrial Wearable System: The Human-Centric Empowering Technology in Industry 4.0. J. Intell. Manuf. 2019, 30, 2853–2869. [Google Scholar] [CrossRef]
- Morrar, R.; Arman, H.; Mousa, S. The Fourth Industrial Revolution (Industry 4.0): A Social Innovation Perspective. Technol. Innov. Manag. Rev. 2017, 7, 12–20. [Google Scholar] [CrossRef]
- Mindas, M.; Bednar, S. Mass Customization in the Context of Industry 4.0: Implications of Variety-Induced Complexity. In Advanced Industrial Engineering; Wydawnictwo Fundacji Centrum Nowych Technologii: Bielsko-Biała, Poland, 2016; pp. 21–38. [Google Scholar]
- Leesakul, N.; Oostveen, A.-M.; Eimontaite, I.; Wilson, M.L.; Hyde, R. Workplace 4.0: Exploring the Implications of Technology Adoption in Digital Manufacturing on a Sustainable Workforce. Sustainability 2022, 14, 3311. [Google Scholar] [CrossRef]
- Zhao, X.; Hsu, C.; Chang, P.; Li, L. A Genetic Algorithm for the Multi-Objective Optimization of Mixed-Model Assembly Line Based on the Mental Workload. Eng. Appl. Artif. Intell. 2016, 47, 140–146. [Google Scholar] [CrossRef]
- Falck, A.C.; Rosenqvist, M. What Are the Obstacles and Needs of Proactive Ergonomics Measures at Early Product Development Stages?—An Interview Study in Five Swedish Companies. Int. J. Ind. Ergon. 2012, 42, 406–415. [Google Scholar] [CrossRef]
- Zare, M.; Croq, M.; Hossein-Arabi, F.; Brunet, R.; Roquelaure, Y. Does Ergonomics Improve Product Quality and Reduce Costs? A Review Article. Hum. Factors Ergon. Manuf. 2016, 26, 205–223. [Google Scholar] [CrossRef]
- Morton, J.; Zheleva, A.; Van Acker, B.B.; Durnez, W.; Vanneste, P.; Larmuseau, C.; De Bruyne, J.; Raes, A.; Cornillie, F.; Saldien, J.; et al. Danger, High Voltage! Using EEG and EOG Measurements for Cognitive Overload Detection in a Simulated Industrial Context. Appl. Ergon. 2022, 102, 103763. [Google Scholar] [CrossRef] [PubMed]
- Biondi, F.N.; Cacanindin, A.; Douglas, C.; Cort, J. Overloaded and at Work: Investigating the Effect of Cognitive Workload on Assembly Task Performance. Hum. Factors 2021, 63, 813–820. [Google Scholar] [CrossRef]
- Buchholz, V.; Kopp, S. Towards an Adaptive Assistance System for Monitoring Tasks: Assessing Mental Workload Using Eye-Tracking and Performance Measures. In Proceedings of the IEEE International Conference on Human-Machine Systems (ICHMS), Rome, Italy, 7–9 September 2020; IEEE: Rome, Italy, 2020; pp. 1–6. [Google Scholar]
- Lagomarsino, M.; Lorenzini, M.; De Momi, E.; Ajoudani, A. An Online Framework for Cognitive Load Assessment in Industrial Tasks. Robot. Comput. Integr. Manuf. 2022, 78, 102380. [Google Scholar] [CrossRef]
- Brandler, S.; Rammsayer, T.H. Differences in Mental Abilities between Musicians and Non-Musicians. Psychol. Music 2003, 31, 123–138. [Google Scholar] [CrossRef]
- Murgia, M.; Di Fronso, S.; degli Studi, U.G.; Chieti Pescara, A.; Tommi Sipari, I.; Di Corrado, D.; Corrado, D.D.; Guarnera, M.; Savia Guerrera, C.; Mauro Maldonato, N.; et al. Mental Imagery Skills in Competitive Young Athletes and Non-Athletes. Front. Psychol. 2020, 11, 633. [Google Scholar] [CrossRef]
- Villa, A.E.P.; Pardo-Vazquez, J.L.; Cheron, G.; Andreu-Sánchez, C.; Ángel Martín-Pascual, M.; Gruart, A.; María Delgado-García, J. The Effect of Media Professionalization on Cognitive Neurodynamics during Audiovisual Cuts. Front. Syst. Neurosci. 2021, 15, 598383. [Google Scholar] [CrossRef]
- ISO 10075-1:2017; Ergonomic Principles Related to Mental Workload—Part 1: General Issues and Concepts, Terms and Definitions. ISO: Berlin, Germany, 2017. Available online: https://www.iso.org/standard/66900.html (accessed on 19 October 2023).
- Young, M.S.; Brookhuis, K.A.; Wickens, C.D.; Hancock, P.A. State of Science: Mental Workload in Ergonomics. Ergonomics 2015, 58, 1–17. [Google Scholar] [CrossRef]
- Stanton, N.A.; Hedge, A.; Brookhuis, K.; Salas, E.; Hendrick, H.W. Mental Workload. In Handbook of Human Factors and Ergonomics Methods; Neville, S., Ed.; Taylor & Francis: Abingdon, UK, 2019; Volume 39. [Google Scholar]
- Matthews, G.; Davies, D.R. Individual Differences in Energetic Arousal and Sustained Attention: A Dual-Task Study. Pers. Individ. Differ. 2001, 31, 575–589. [Google Scholar] [CrossRef]
- Wilson, G.F.; Russell, C.A. Real-Time Assessment of Mental Workload Using Psychophysiological Measures and Artificial Neural Networks. Hum. Factors 2003, 45, 635–643. [Google Scholar] [CrossRef] [PubMed]
- da Silva, M.H.d.O.C.; Macêdo, T.F.; de Carvalho Lourenço, C.; de Souza Rehder, I.; da Costa Marchiori, A.A.; Cesare, M.P.; Cortes, R.G.; Cardoso Junior, M.M.; Villani, E. Mental Workload Assessment in Military Pilots Using Flight Simulators and Physiological Sensors. In Proceedings of the International Symposium on Human Mental Workload: Models and Applications, Virtual, 24–26 November 2021; Springer: Berlin/Heidelberg, Germany, 2021; Volume 1493, pp. 99–115. [Google Scholar] [CrossRef]
- Guzmán-García, C.; Sánchez-González, P.; Sánchez Margallo, J.A.; Snoriguzzi, N.; Rabazo, J.C.; Sánchez Margallo, F.M.; Gómez, E.J.; Oropesa, I. Correlating Personal Resourcefulness and Psychomotor Skills: An Analysis of Stress, Visual Attention and Technical Metrics. Sensors 2022, 22, 837. [Google Scholar] [CrossRef]
- Tobii. Tobii Pro Glasses 3: Real Insights from the Real World. Available online: https://www.tobii.com/products/eye-trackers/wearables/tobii-pro-glasses-3 (accessed on 10 May 2023).
- Tobii Pro, A.B. Tobii Pro Lab User Manual. Available online: https://go.tobii.com/tobii_pro_lab_user_manual (accessed on 20 August 2023).
- Zephyr Technology. Zephyr BioHarness 3. Available online: https://www.zephyranywhere.com/system/components (accessed on 20 August 2023).
- Zephyr Technology. BioHarness 3 Log Data Descriptions. Available online: https://www.zephyranywhere.com/media/download/bioharness-log-data-descriptions-07-apr-2016.pdf (accessed on 20 August 2023).
- Wood, R.E. Task Complexity: Definition of the Construct. Organ. Behav. Hum. Decis. Process 1986, 37, 60–82. [Google Scholar] [CrossRef]
- The MathWorks Inc. MATLAB Version: 9.11.0 (R2021b). Available online: https://uk.mathworks.com/ (accessed on 13 February 2022).
- Kret, M.E.; Sjak-Shie, E.E. Preprocessing Pupil Size Data: Guidelines and Code. Behav. Res. Methods 2019, 51, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Mathôt, S.; Vilotijević, A. Methods in Cognitive Pupillometry: Design, Preprocessing, and Statistical Analysis. Behav. Res. Methods 2022, 55, 3055–3077. [Google Scholar] [CrossRef] [PubMed]
- Reimer, J.; McGinley, M.J.; Liu, Y.; Rodenkirch, C.; Wang, Q.; McCormick, D.; Tolias, A. Pupil Fluctuations Track Rapid Changes in Adrenergic and Cholinergic Activity in Cortex. Nat. Commun. 2016, 7, 13289. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. JSS J. Stat. Softw. 2012, 50, 1. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R. Available online: http://www.rstudio.com/ (accessed on 10 May 2023).
- Chandola, T.; Britton, A.; Brunner, E.; Hemingway, H.; Malik, M.; Kumari, M.; Badrick, E.; Kivimaki, M.; Marmot, M. Work Stress and Coronary Heart Disease: What Are the Mechanisms? Eur. Heart J. 2008, 29, 640–648. [Google Scholar] [CrossRef]
- Kang, M.; Koh, S.; Cha, B.; Park, J.K.; Woo, J.M.; Chang, S.J. Association between Job Stress on Heart Rate Variability and Metabolic Syndrome in Shipyard Male Workers. Yonsei Med. J. 2004, 45, 838–846. [Google Scholar] [CrossRef]
- Fink, L.; Simola, J.; Tavano, A.; Lange, E.; Wallot, S.; Laeng, B. From Pre-Processing to Advanced Dynamic Modeling of Pupil Data. Behav. Res. Methods 2023, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Held, J.; Vîslă, A.; Wolfer, C.; Messerli-Bürgy, N.; Flückiger, C. Heart Rate Variability Change during a Stressful Cognitive Task in Individuals with Anxiety and Control Participants. BMC Psychol. 2021, 9, 44. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assembly Stage | Required Acts | Information Cues |
|---|---|---|
| Gear assembly: first (or second) assembly stage | 1. Pushing (behaviour act 1) and rotating (behaviour act 2) the output shaft into the hole of the engine body. | 1. The correct side of the hole for output assembly; |
| 2. Quality of assembly completion of the gear of the output shaft. | ||
| Housing assembly: second (or first) assembly stage | 2. Align (behaviour act 1) the 4 holes on the housing with the four rods on the engine body. | 1. Visualization of 4 rods of the engine; |
| 2. Visualization of 4 correlated holes of engine rods on the housing. | ||
| Rotor and cover assembly: third assembly stage | 3. Assemble (behaviour act 1) the rotor inside the housing, align the correct holes on the cover with four rods on the engine body, and screw (behaviour 2) 5 nuts. | 1.Visualization of the output shaft, housing chamber, and rotor; |
| 2. Quality of assembly completion for the rotor; | ||
| 3. Visualization of 4 rods on the engine body; | ||
| 4. Visualization of 4 correlated holes on the cover; | ||
| 5. Finding 5 nuts. |
| Assembly Stage | Assembly Task Name | Task Complexity | Task Complexity Score |
|---|---|---|---|
| 2 or 1 | Housing assembly | Low complexity | 4 |
| 1 or 2 | Gear assembly | Medium complexity | 5 |
| 3 | Rotor and cover assembly | High complexity | 7 |
| Cognitive Workload Metrics | Definition |
|---|---|
| Baselined pupil diameter | The average pupil dilation from baseline time was subtracted from the pupil diameter. |
| Baselined pupil-diameter derivative | The average pupil-diameter derivative from baseline time was subtracted from the pupil-diameter derivative, and this metric can quantify the extent of pupil dilation or constriction from baseline time. |
| Baselined standard deviation of the RR intervals (baselined SDNN) | The average SDNN from baseline time was subtracted from the standard deviation of the RR intervals (SDNN). |
| Baselined Root Mean Square of successive differences between normal heartbeats (baselined RMSSD) | The average RMSSD from baseline time was subtracted from the Root Mean Square of successive differences between normal heartbeats (RMSSD). |
| Baselined proportion of the number of pairs of successive NN intervals that differ by more than 50 ms divided by the total number of NN intervals (baselined PNN50) | The average PNN50 from baseline time was subtracted from the proportion of the number of pairs of successive NN intervals that differ by more than 50 ms divided by the total number of NN intervals (PNN50). |
| The low-frequency band (LF) | The low-frequency band is from 0.04 to 0.15 Hz. |
| The high-frequency band (HF) | The high-frequency band is from 0.15 to 0.4 Hz. |
| The normalized low-frequency band power (LFnu) | The normalized low-frequency band power is from 0.04 to 0.15 Hz. |
| The normalized high-frequency band power (HFnu) | The normalized high-frequency band power is from 0.15 to 0.4 Hz. |
| The ratio of low-frequency to high-frequency (LF/HF ratio) | The ratio of low-frequency to high-frequency is LH/HF. |
| Physiological Metrics | Expertise Group 1 | Rest (B) 2 | Housing (LC) 2 | Gear (MC) 2 | Rotor and Cover (HC) 2 |
|---|---|---|---|---|---|
| Baselined peak pupil dilation (mm) 3 | E | 0.000 ± 0.000 | 0.457 ± 0.270 | 0.626 ± 0.253 | 0.484 ± 0.282 |
| N-E | 0.000 ± 0.000 | 0.631 ± 0.469 | 0.706 ± 0.419 | 0.736 ± 0.682 | |
| Baselined pupil- diameter derivative (mm/s) 3 | E | 0.000 ± 0.000 | 6.993 ± 0.114 | −0.041 ± 0.152 | 0.015 ± 0.026 |
| N-E | 0.000 ± 0.000 | −0.011 ± 0.010 | −0.002 ± 0.032 | −0.001 ± 0.006 | |
| Baselined SDNN (ms) 3 | E | 0.000 ± 0.000 | 4.363 ± 22.123 | −4.257 ± 13.977 | 5.780 ± 18.861 |
| N-E | 0.000 ± 0.000 | 30.434 ± 61.439 | −13.292 ± 33.977 | −2.375 ± 58.385 | |
| Baselined RMSSD (ms) 3 | E | 0.000 ± 0.000 | 18.934 ± 30.241 | 9.051 ± 18.609 | 16.374 ± 27.140 |
| N-E | 0.000 ± 0.000 | −34.743 ± 86.464 | −8.940 ± 47.154 | 1.340 ± 75.709 | |
| Baselined PNN50 (%) | E | 0.000 ± 0.000 | 0.382 ± 0.454 | 0.623 ± 0.686 | 0.401 ± 0.449 |
| N-E | 0.000 ± 0.000 | −0.044 ± 0.501 | 0.173 ± 0.787 | −0.108 ± 0.510 | |
| LF (ms2/Hz) 3 | E | 1.196 ± 2.825 | 14.776 ± 22.135 | 12.411 ± 26.253 | 0.909 ± 1.432 |
| N-E | 8.577 ± 28.084 | 0.797 ± 1.150 | 4.760 ± 13.400 | 1070.000 ± 34,400.000 | |
| HF (ms2/Hz) 3 | E | 0.021 ± 0.049 | 0.176 ± 0.274 | 0.147 ± 0.300 | 0.008 ± 0.012 |
| N-E | 0.104 ± 0.344 | 0.011 ± 0.021 | 0.012 ± 0.024 | 1770.000 ± 5860.000 | |
| LFnu (%) | E | 0.425 ± 0.364 | 99.505 ± 0.554 | 98.923 ± 0.606 | 99.263 ± 0.568 |
| N-E | 0.382 ± 0.506 | 82.252 ± 37.974 | 90.390 ± 29.900 | 81.900 ± 35.703 | |
| HFnu (%) | E | 0.005 ± 0.008 | 0.495 ± 0.554 | 1.077 ± 0.606 | 0.737 ± 0.568 |
| N-E | 0.003 ± 0.007 | 0.562 ± 0.675 | 0.539 ± 0.857 | 2.345 ± 4.320 | |
| LF/HF ratio (Unitless) | E | 425.491 ± 283.706 | 616.648 ± 541.243 | 179.885 ± 215.633 | 281.295 ± 258.100 |
| N-E | 566.180 ± 177.973 | 408.872 ± 363.832 | 527.458 ± 423.384 | 400.036 ± 729.143 |
| Pupillometry Cognitive-Load Indexes | Cardiac Cognitive-Load Indexes | |||||||
|---|---|---|---|---|---|---|---|---|
| Subject ID | Rest (B) | Housing (L) | Gear (M) | Rotor and Cover (H) | Rest (B) | Housing (L) | Gear (M) | Rotor and Cover (H) |
| 201 | 3 | 2 | 3 | 15 | 2 | 0 | 2 | 14 |
| 202 | 1 | 3 | 7 | 12 | 2 | 2 | 1 | 5 |
| 203 | 0 | 11 | 2 | 21 | 4 | 3 | 1 | 1 |
| 204 | 2 | 10 | 14 | 14 | 4 | 2 | 2 | 4 |
| 205 | 3 | 6 | 6 | 30 | 3 | 3 | 2 | 14 |
| 206 | 4 | 5 | 7 | 17 | 4 | 1 | 5 | 5 |
| 102 | 2 | 2 | 4 | 27 | 4 | 1 | 2 | 19 |
| 105 | 1 | 42 | 9 | 20 | 3 | 25 | 29 | 4 |
| 107 | 3 | 8 | 4 | 27 | 2 | 3 | 0 | 12 |
| 108 | 3 | 19 | 34 | 72 | 2 | 2 | 2 | 9 |
| 110 | 1 | 8 | 1 | 49 | 2 | 13 | 1 | 42 |
| 111 | 3 | 16 | 4 | 20 | 3 | 10 | 3 | 17 |
| 112 | 3 | 12 | 4 | 13 | 4 | 4 | 0 | 8 |
| 115 | 3 | 14 | 3 | 17 | 3 | 3 | 0 | 2 |
| 116 | 2 | 2 | 14 | 21 | 4 | 1 | 1 | 12 |
| 117 | 1 | 4 | 6 | 16 | 2 | 3 | 3 | 11 |
| 121 | 4 | 13 | 3 | 33 | 4 | 7 | 4 | 20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, X.; Monfared, R.; Grant, R.; Goh, Y.M. Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability. Sensors 2024, 24, 2010. https://doi.org/10.3390/s24062010
Ma X, Monfared R, Grant R, Goh YM. Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability. Sensors. 2024; 24(6):2010. https://doi.org/10.3390/s24062010
Chicago/Turabian StyleMa, Xinyue, Radmehr Monfared, Rebecca Grant, and Yee Mey Goh. 2024. "Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability" Sensors 24, no. 6: 2010. https://doi.org/10.3390/s24062010
APA StyleMa, X., Monfared, R., Grant, R., & Goh, Y. M. (2024). Determining Cognitive Workload Using Physiological Measurements: Pupillometry and Heart-Rate Variability. Sensors, 24(6), 2010. https://doi.org/10.3390/s24062010