1. Introduction
Neuro-musculo-skeletal disorders often result in degradation of the human balance control system. Balance control deterioration may occur suddenly, for example after spinal cord injury, or gradually, as is often the case with the elderly. The long term goal of this study is to develop a neuroprothesis using a functional electrical stimulation (FES) technology [
1] which can be used by people with balance impairment in their daily life. In recent years several efforts have been done towards addressing some of the design issues pertaining to this technology, such as dynamic redundancy problem of quiet standing [
2], physiological control system of quiet standing in able-bodied individuals [
3] and neurological time delays and their impact on control of quiet standing [
4]. The natural expansion of this work is the development of a sensor that can measure balance in real-time during quiet standing. This sensor can be used in close-loop with a neuroprosthesis for quiet standing to facilitate balance control. Therefore, the main focus of this article is the development of an algorithm for instability detection that can be later used as an integral part of a sensor for measuring balance and stability during quiet standing. The proposed algorithm will be implemented in a miniaturized footsole sensor system.
A conventional approach towards assessing balance during quiet standing states that the center of mass (COM) of the body has to be confined within the vertical space above the body's base of support (BOS) for the body to maintain stability [
5–
7]. Pai and his colleagues demonstrated that the relative displacement of the COM with respect to the BOS alone is not an accurate predictor of a stepping reaction, i.e., the confinement of the COM to the vertical space above the BOS cannot guarantee that the balance will be maintained during quiet standing [
8–
14]. Therefore they proposed that one has to measure the magnitude and the direction of the COM velocity in addition to the COM position to be able to predict stepping during standing.
One of the fundamental problems with obtaining COM position and velocity is that they cannot be measured using any direct method. Instead, one has to measure other body parameters and then by applying a model extract COM position and velocity values from these measurements. The fundamental problem with this technique is that it heavily depends on body anthropometry and body mass distribution, which cannot be accurately determined. As a result, the COM position estimation is as good as the model used to derive it and these models are inherently inaccurate. To circumvent this problem, Popovic et al. [
15] have been investigating the use of center of pressure (COP) measurements to assess balance. The benefit of using COP measurements is that one can obtain them accurately using a portable sensory system. Motivated by this idea, they have proposed a stability measure using COP measurements alone. They have identified four different stability zones: the high preference, low preference, undesirable, and unstable zones. Depending on the position of the COP with respect to these four zones, it is possible to determine whether a standing able-bodied individual is stable or unstable. They proposed that the border of the unstable zone represents a threshold that COP has to exceed for a person to make a step after being perturbed during quiet standing. Therefore, they have proposed a method that can predict stepping by measuring COP alone.
One shortcoming of their method is that it applies well for quasi-static conditions, i.e., when perturbations are slow, and the COP moves with relatively low velocity. In the event the COP moves fast this method is not as effective. To rectify the problem in this study we have focused our efforts at analyzing the dynamic properties of the COP, i.e., COP velocity (COPv), and using that information to predict stepping resulted from perturbations during quiet standing. In what follows, we are presenting experiments and statistical analysis that helped us develop a step predictor based on COP position and velocity measurements.
2. Methods
2.1. Subjects
Sixteen healthy able-bodied adults (8 male and 8 female) with no previous record of neuro-muscular disorders were recruited (
Table 1). Each participant signed written informed consent that was approved by the Health Sciences Ethics Review Boards of the University of Toronto and Toronto Rehabilitation Institute. After the experiments were concluded data obtained with one male subject (Subj 3 in
Table 1) had to be excluded due to his peculiar responses to the perturbations. This subject tried consciously to maintain balance such that he did not need to make a step by plantar flexing, i.e. standing on his toes after every perturbation.
2.2. COP/COPv Sensor
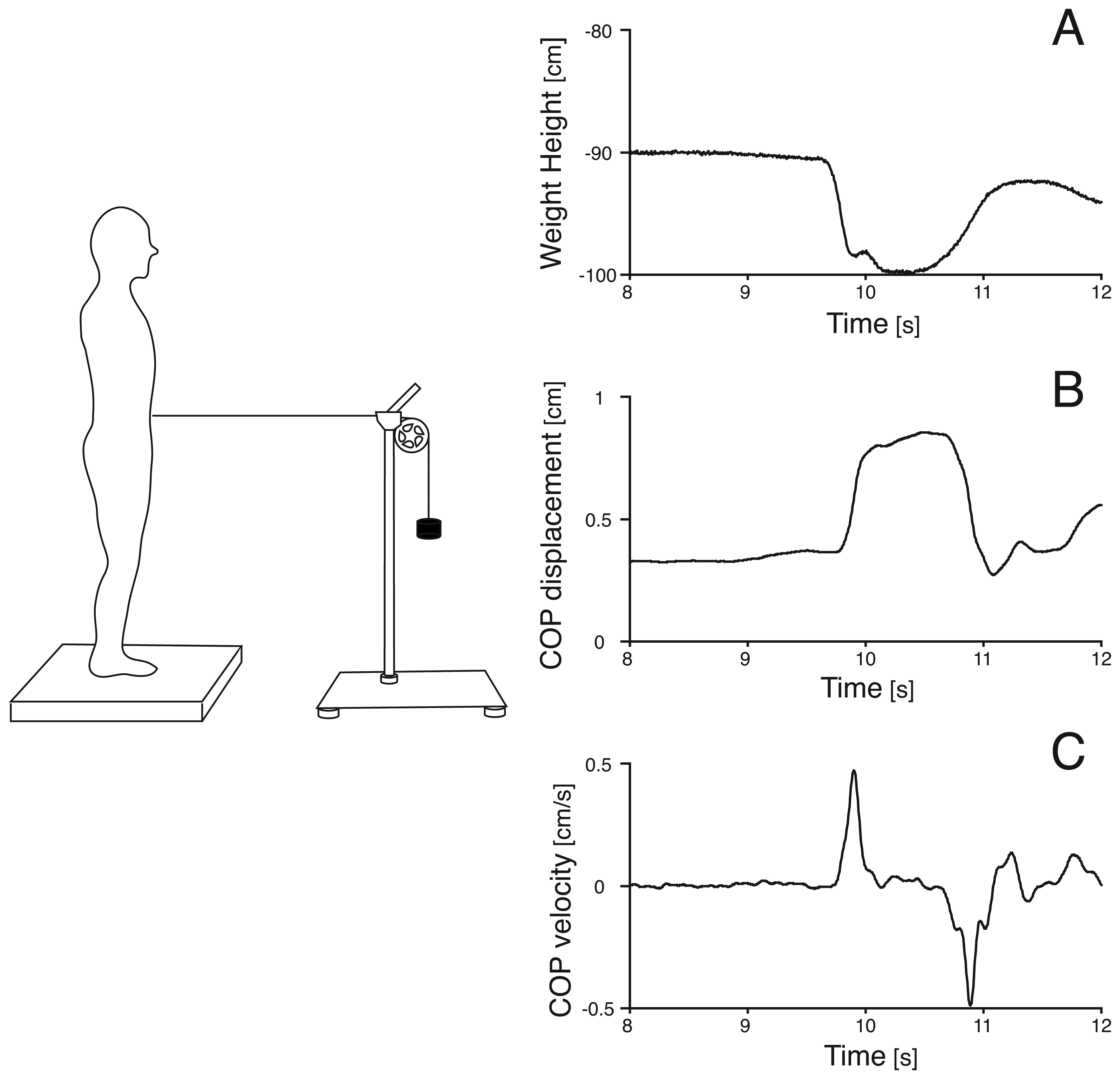
The experimental setup consisted of: 1) two force plates (Type 9366AB05, Kistler, Switzerland); 2) a data acquisition system consisting of a 133 MHz Pentium PC, A/D card (NI PCI-6701E, National Instruments, USA) and custom-made data acquisition software; 3) a 3D motion capture system (Op-totrak 3020, Northern Digital Inc., Canada); and 4) a dropped-weight pulley system (
Figure 1). The dropped-weight pulley system was designed such that when the release mechanism was pulled, the pulley generated instantaneous, horizontal, and adjustable pulling force.
The force plates were used to measure the subject's COP position. The optical markers of the 3D motion capture system were placed on the lateral malleolus and the head of the metatarsal II to examine the movements of the ankle and toe, respectively. Since in this study we considered only the anterior-posterior direction of sway and perturbation, only the kinematics of the anterior-posterior displacements were recorded.
The net COP position in the anterior-posterior direction was obtained according to [
16]. The COPv was obtained by differentiating the COP position. COP position was normalized by dividing the COP coordinates by the length of the subject's feet. This way the measured COP excursions were made proportional to the length of the subject's feet. Hence, the COP measurements were normalized for all subjects such that 0 was the posterior limit of the heel and 1 was the anterior limit of the 1st toe. In order to be consistent with previous studies [
9,
12], COPv was normalized using the subject's height. The force plates and the kinematic measurements were synchronized and the sampling frequency for both systems was 140 Hz. For noise removal the data were filtered using a 4th order, low pass, zero-lag Butterworth digital filter [
17] with a low pass cutoff frequency of 10 Hz.
2.3. Protocol
The participants in the study were asked to stand still on the force plates, with bare feet, in an upright position. The subjects were attached to the perturbation system using a velcro belt, aligned with the mid-line of the body at the level of the umbilicus. In order to minimize anticipatory reactions and muscle contractions the subjects were asked to stand with their eyes closed during all trials. Also, to distract the attention of the subjects from the perturbation, the subjects wore headphones and listened to whale sounds, which relaxed the participants and did not have a particular rhythm that could potentially influence the subjects' sway.
Anterior and posterior perturbations were applied at the waist. For each subject, and for each direction, weights were used from 0.454 kg up to the maximum weight required to produce a step (the maximum weight used among the subjects group was 6.8 kg). The weight applied was incremented by 0.454 kg until the subject made a step, and then one more weight of 0.454 kg was added, to ensure that at least two stepping trials were recorded per subject. The instance when a step occurs was defined by the moment when the vertical ground reaction force from one of the two force plates was reduced to zero. The order of the perturbations, i.e. weight used to cause the perturbation, was randomly selected. In previously published studies involving perturbation experiments, the subjects were instructed to try to maintain balance without stepping or were instructed to ‘react naturally’ in response to perturbations. As it was our intention to obtain a model that is representative of the actual able-bodied individuals' response to perturbation, the subjects were asked to react as naturally as possible to the perturbations.
2.4. Data Analysis
Estimation of COP Position Peak From COP Velocity Peak: Data from the non-stepping trials were used in the following analysis. The peaks of COPv and COP were determined for all the anterior and posterior perturbation trials. A linear regression analysis that applies a least square method was used to obtain an equation that describes the relationship between the COP peak and the COPv peak. These equations predict the subject's COP peak based on the COPv peak.
Step Predictor: The linear regression equation developed using the analysis described above will predict the COP peak that a subject will experience from a perturbation using the COPv measurements. Therefore, if the output of the equation is compared with a COP threshold for instability that will cause stepping, a step predictor is obtained. Five different anterior step thresholds were chosen:
- Th.1A
The anterior limit of the undesirable zone proposed by [
15].
- Th.2A
The mean value of the maximum COP among trials in which no ankle movement was detected, i.e. the subject did not try to compensate for the perturbation by moving his/her ankle joint.
- Th.3A
The minimum value of the maximum COP among trials in which ankle movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her ankle joint.
- Th.4A
The mean value of the maximum COP among trials in which ankle movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her ankle joint.
- Th.5A
The maximum value of the maximum COP among trials in which ankle movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her ankle joint.
These anterior stepping thresholds were determined using all the anterior-perturbation non-stepping trials. Five different posterior step thresholds were chosen:
- Th.1P
The posterior limit of the undesirable zone proposed by [
15].
- Th.2P
The mean value of the minimum COP among trials in which no toe movement was detected, i.e. the subject did not try to compensate for the perturbation by moving his/her toes.
- Th.3P
The maximum value of the minimum COP among trials in which toe movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her toes.
- Th.4P
The mean value of the minimum COP among trials in which toe movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her toes.
- Th.5P
The minimum value of the minimum COP among trials in which movement was detected, i.e. the subject tried to compensate for the perturbation by moving his/her toes.
These posterior stepping thresholds were determined using all the posterior-perturbation non-stepping trials.
We refer to the abovementioned step predictors as
dynamic predictors, since they use COPv in addition to COP to predict if a step will be taken by the able-bodied individual after he/she has been perturbed by an external force. We compared these dynamic predictors with the step predictor proposed by [
15], which used only COP position information and therefore is referred to as
static predictor. A binary test was performed for each step predictor with all the perturbation trials [
18,
19]. A binary classification test is the task of classifying the members of a given set of objects into two groups on the basis of whether they have some property or not. To measure the performance of a binary classifier, the concepts sensitivity and specificity are often used, and are defined as follows:
A binary test was performed for each step predictor with all the perturbation trials (stepping and non-stepping trials). According to the abovementioned equations, the sensitivity of a step predictor is the probability that steps were detected in a trial in which the subject had to step. The specificity of the predictor is the probability that steps were not detected in a trial in which the subject did not have to step.
Differences in time between the moment when the step was predicted and the moment when the subject actually made a step (marginal time) were calculated to investigate the advantage of the dynamic predictor. Only the trials in which the predictor performed satisfactorily, i.e. if the predictor detected stepping before the subject made a step, were used for calculating the prediction time.
3. Results and Discussion
3.1. Estimation of Peak COP Position From Peak COP Velocity
The total number of the participants whose data could be used for the purpose of this study was 15. In total 222 trials were carried out (137 anterior perturbations and 85 posterior perturbations) successfully (
Table 1). The number of trials differed for each subject, because each individual participant required a different amount of weight to be perturbed sufficiently to make a step to recover balance.
Figure 1 shows the time-history data from a single non-stepping trial induced by an anterior perturbation. It is clearly shown that the COPv peak occurred before the COP peak. All perturbation trials showed the same behavior.
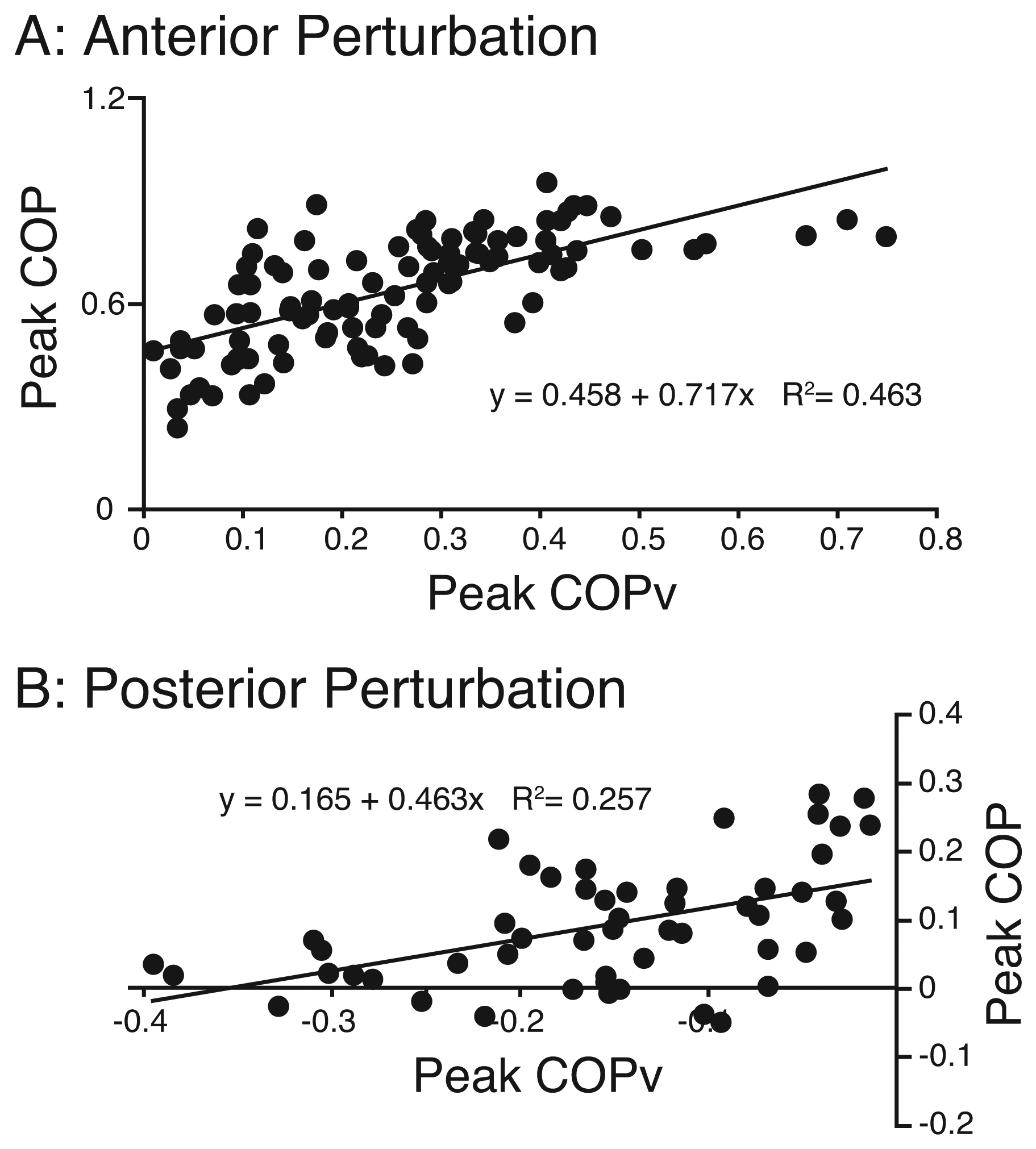
Anterior Perturbations: Figure 2A shows the group result of the relationship between the COP peak and the COPv peak from anterior perturbation trials. A least squares regression estimation resulted in the following equation:
The
R2 of the estimate was 0.463 (
n = 137,
p < 0.001). 95 % confidence bounds were 0.565 <
slope < 0.869 and 0.413 <
intercept < 0.503.
Posterior Perturbations: Figure 2B shows the group result of the relationship between the COP peak and the COPv peak from posterior perturbation trials. A least squares regression estimation resulted in the following equation:
The
R2 of the estimate was 0.257 (
n = 85,
p < 0.001). 95 % confidence bounds were 0.245 <
slope < 0.681 and 0.126 <
intercept < 0.204 for the slope and intercept, respectively.
3.2. Step Predictor
The values for the thresholds for each step predictor are shown in
Table 2. Binary tests were performed for each step predictor to assess their performance.
Table 3 shows 2
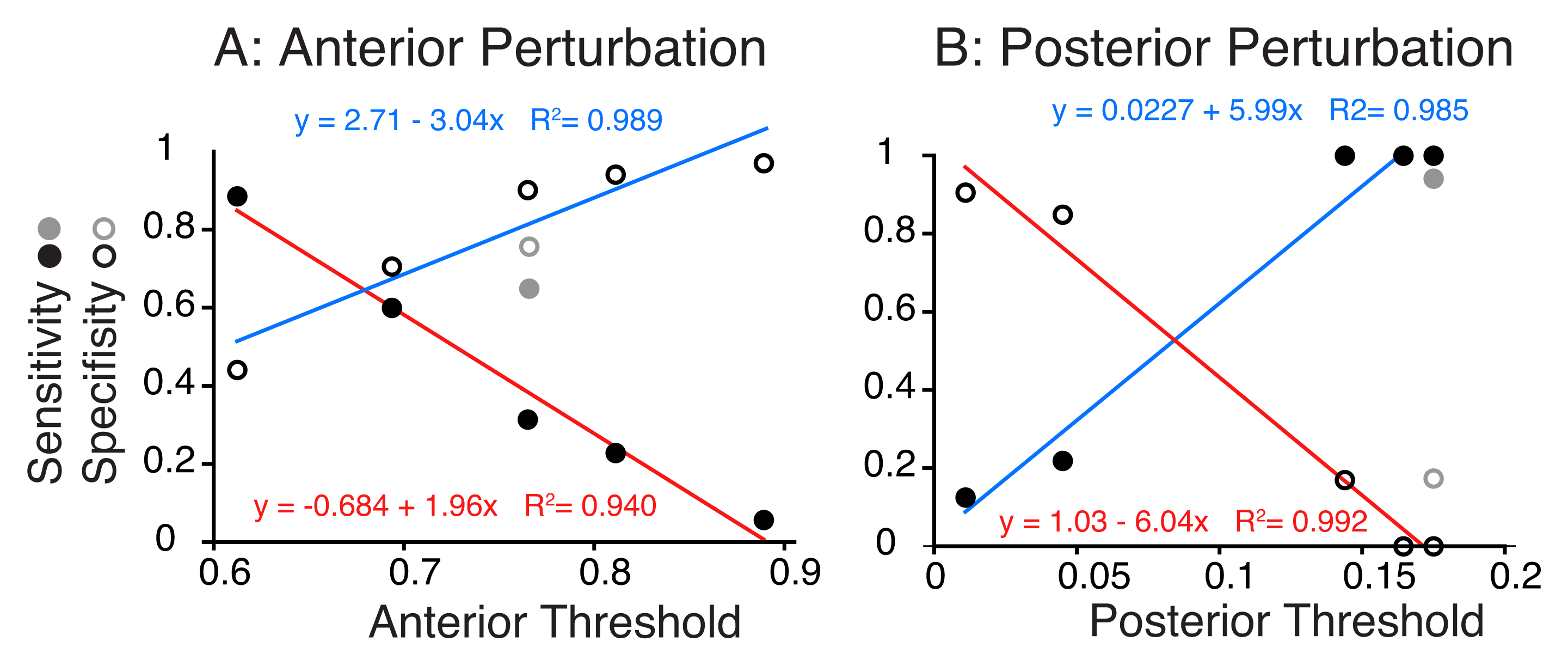
× 2 contingency tables for each step predictor for anterior perturbations. By applying binary tests, we assessed the performance of each predictor. The sensitivity and specificity for step predictors are plotted against the step threshold for anterior movements in
Figure 3A. The ‘sensitivity’ of a predictor is the probability that stepping was predicted in a trial in which the subject made a step. The ‘specificity’ is the probability that stepping was not detected in a trial in which the subject did not have to step. As the step threshold increases, the sensitivity decreases linearly whereas generally the specificity increases linearly. The static predictor had relatively high values for both of sensitivity (grey closed circle) and specificity (grey open circle). Only the dynamic predictor with the Th.3A conditions (threshold of 0.694) showed similarly high values for both sensitivity and specificity, similar to the static predictor.
Table 4 shows 2
× 2 contingency tables for posterior perturbations. Using COPv during natural standing, the estimated COP position always reached the threshold of Th.1P and Th.3P. As a result, the dynamic predictor with Th.1P and Th.3P predicted stepping in all trials. On the contrary, the dynamic predictor with Th.4P and Th.5P rarely predicted stepping. Binary tests were performed for each step predictor using the 2
× 2 contingency tables. The sensitivity and specificity are plotted against the step threshold for posterior movements in
Figure 3B. Similarly to the anterior perturbation case, higher sensitivity predictors have a lower specificity, and
vice versa. The dynamic predictor with Th.2P showed a sensitivity and specificity similar to those of the static predictor.
The dynamic predictors with sensitivity similar to that of the static predictors were the one with Th.3A for anterior perturbations, and the one with Th.2P for posterior perturbations. We examined how early these dynamic predictors were able to predict stepping compared with the static predictors.
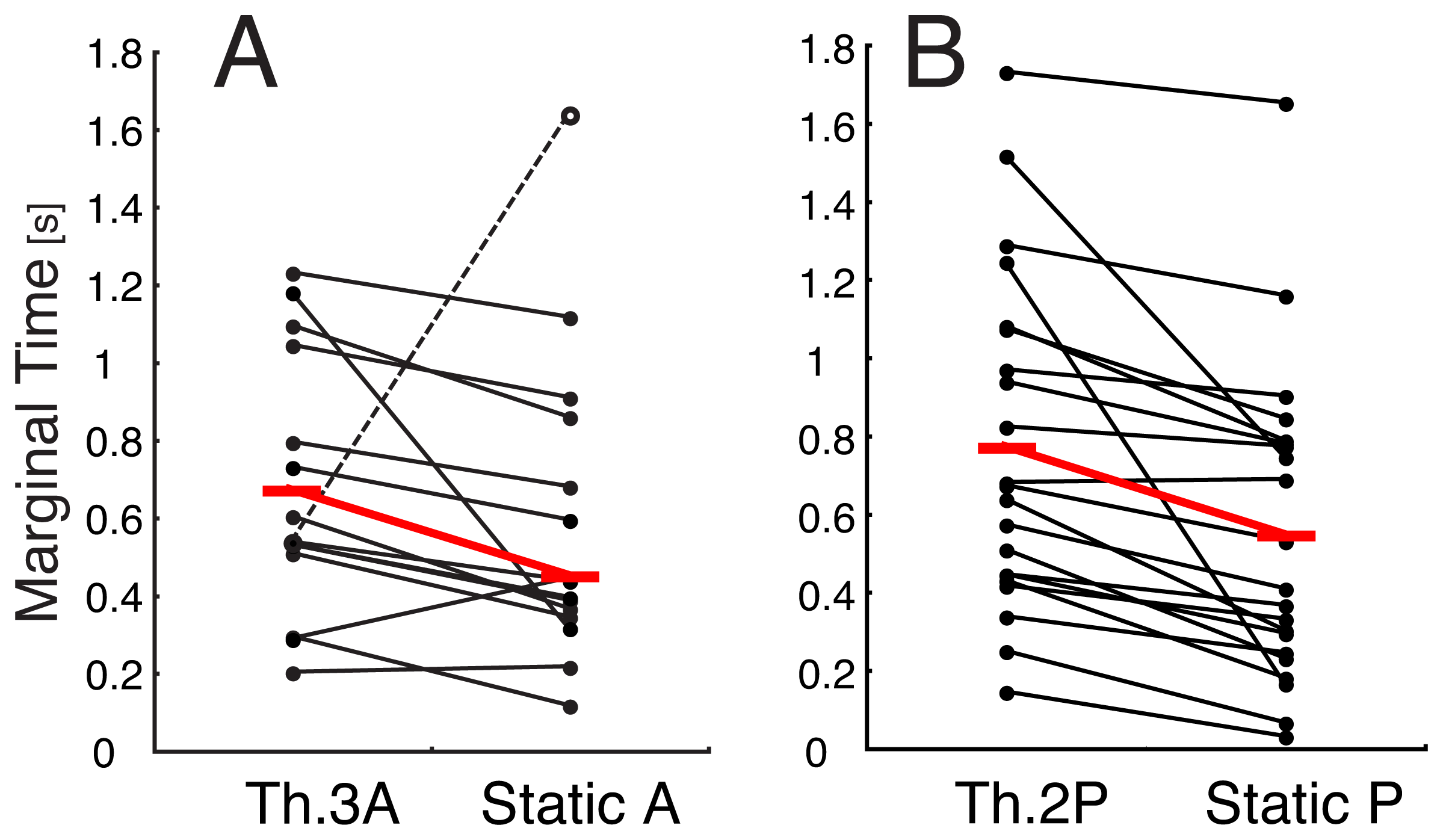
Figure 4 shows the marginal time for these dynamic predictors and the static predictors for the anterior (
Figure 4A) and posterior perturbations (
Figure 4B). In most cases, the dynamic predictors predicted stepping earlier than the static predictors. When the outlier (open circle in
Figure 4A) was eliminated, the difference of the marginal time between the dynamic predictor and the static predictor were 0.171 ± 0.223 s for Th.3A and 0.225 ± 0.253 s for Th.2P. The paired
t-test revealed that there was a significant difference in the marginal times between the dynamic predictor and the static predictor for the anterior perturbations (
p = 0.013,
n = 15) and for the posterior perturbations (
p < 0.001,
n = 21).
3.3. Discussion
We first demonstrated that there is a sufficient linear relationship between the COPv peak and the resulting COP peak involved in a perturbation during standing (
Figure 2). The results suggest that it is possible to estimate the COP peak using COPv measurements according to the
equations (1) and
(2). By introducing step thresholds, we were able to predict instability that results in stepping using the estimated COP peak. The choice of the COP threshold made significant differences with respect to the accuracy with which the system was able to predict stepping. The static predictor previously established by [
15] showed a good performance in predicting stepping (
Figure 3). The dynamic predictors that had closer sensitivity and specificity to those from the static predictor were the one with Th.3A for the anterior perturbation and the one with Th.2P for the posterior perturbation. Since the dynamic predictors used statistically estimated values of COP, their performance might have been poor. Despite of this disadvantage, the dynamic predictor with Th.3A showed equivalent performance to that of the static predictor. In addition to this good performance, the prediction times of these dynamic predictors were considerably longer than those of the static predictors (
Figure 4). These results suggest that the dynamic predictors with Th.3A and Th.2P perform better compared to the static predictor proposed by [
15] because they can predict stepping 171-225 ms earlier, while having sensitivity and specificity similar to those of the static predictor. The capability to predict instability is very important and particularly relevant for applications such as close-loop control of FES systems for standing where early detection of stepping plays a key role in making this system applicable in activities of daily living.
For posterior perturbations, the static predictor showed good sensitivity but poor specificity (
Figure 3B). Although the dynamic predictors with Th.1P and Th.3P showed high sensitivity, it was due to the fact that these thresholds were so large that the COPv during natural standing always reached them. Therefore, these dynamic predictors are not suitable for the step predictors. The dynamic predictors with Th.4P and Th.5P showed high specificity but low sensitivity. If we consider incorporating the step predictor into an FES standing system it would be better for the step predictor to have high sensitivity even if it has low specificity. Therefore, these dynamic predictors are not suitable for those purposes. The predictor that showed a performance equivalent to that of the static predictor was the one with Th.2P. Additionally, the dynamic predictor showed a longer prediction time compared to that of the static predictor (
Figure 4B). The results indicate that the dynamic predictor with Th.2P is capable of predicting stepping better than the static predictor. However, both the dynamic predictor and the static predictor for the posterior perturbation showed poor specificity. This point remains to be improved in future before incorporating the step predictor into an FES standing system.
As this study involved only young subjects, it would be valuable to examine the relationship between COP and COPv for the elderly, and whether the predictor coefficients are affected by age, neurological and musculo-skeletal disorders. Also, different thresholds may be found for different populations.
3.4. Conclusions
We found a linear relationship between the peak COPv and the peak COP caused by a perturbation applied to an able-bodied individual during quiet standing. As the peak COPv occurs considerably before the peak COP displacement, the peak COP estimated using a regression equation from the peak COPv may serve as a step predictor if it is compared with a COP step threshold. Thus, we proposed the dynamic predictor which can determine 171-225 ms earlier than the static predictor whether a perturbed individual will have to take a step due to a perturbation.
The results of this study showed an important parameter of human standing physiology and provided an algorithm for the sensor system that can be used to detect instability during quiet standing. In the near future, the sensor system with this algorithm will be implemented in a close-loop feedback system with a neuroprosthesis for standing. The sensor system will be developed using insole miniaturized pressure sensors which will be used to measure the COPv continuously and in real-time. By means of COPv measurements, this sensory system will be able to predict instability during quiet stance and will be able to predict how much COP will be displaced as a result of an external perturbation. Such information can be used by a neuroprosthesis to generate an appropriate sequence of muscle contractions to compensate for the perturbation and prevent the body from losing balance and falling. The same sensory system could be also used as a diagnostic tool to evaluate balance in stroke patients or aged individuals. These individuals could be instrumented with the sensor to measure their behavior during activities of daily living to help clinicians understand better when and why these individuals became unstable and fall.






{kind=link}
{kind=link}
{kind=link}
{kind=link}