
A Comparison of Different Approaches to Clinical Phenotyping of Lithium Response: A Proof of Principle Study Employing Genetic Variants of Three Candidate Circadian Genes

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Sample Characteristics and Li Response Phenotypes
2.2. Comparison of Accuracy and Discordance for Li Response Phenotypes
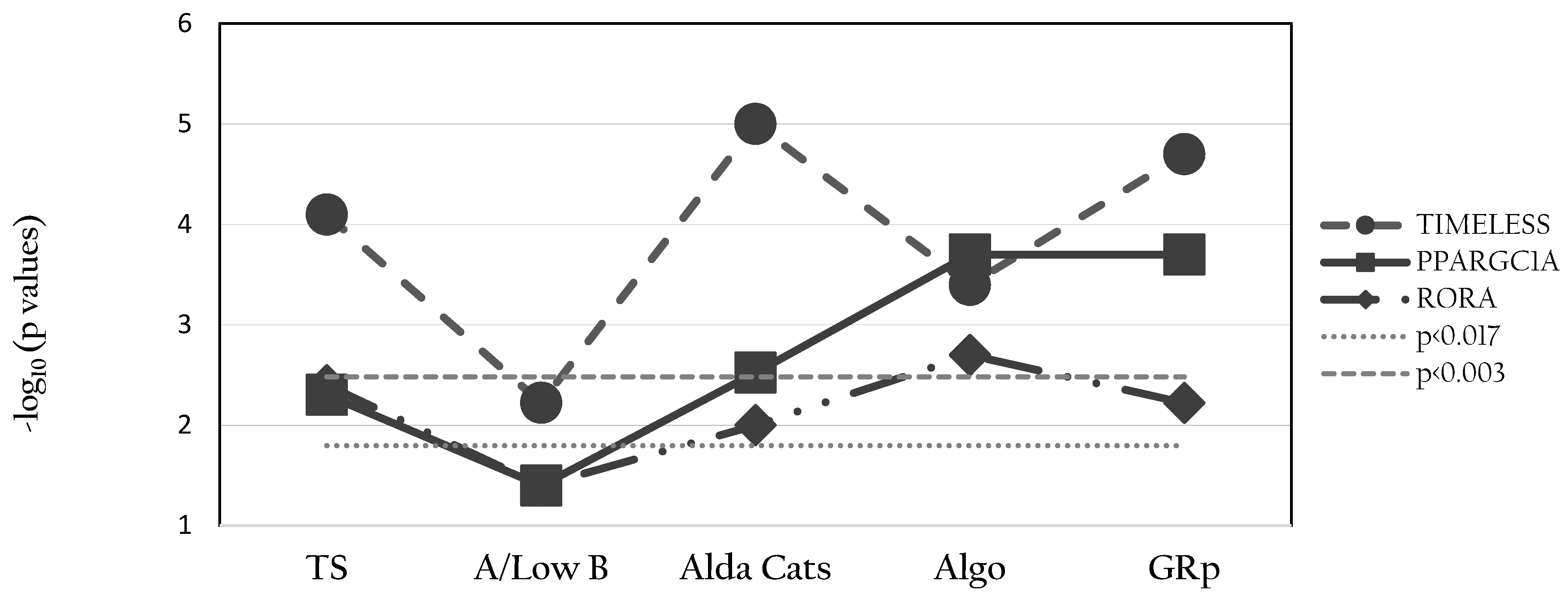
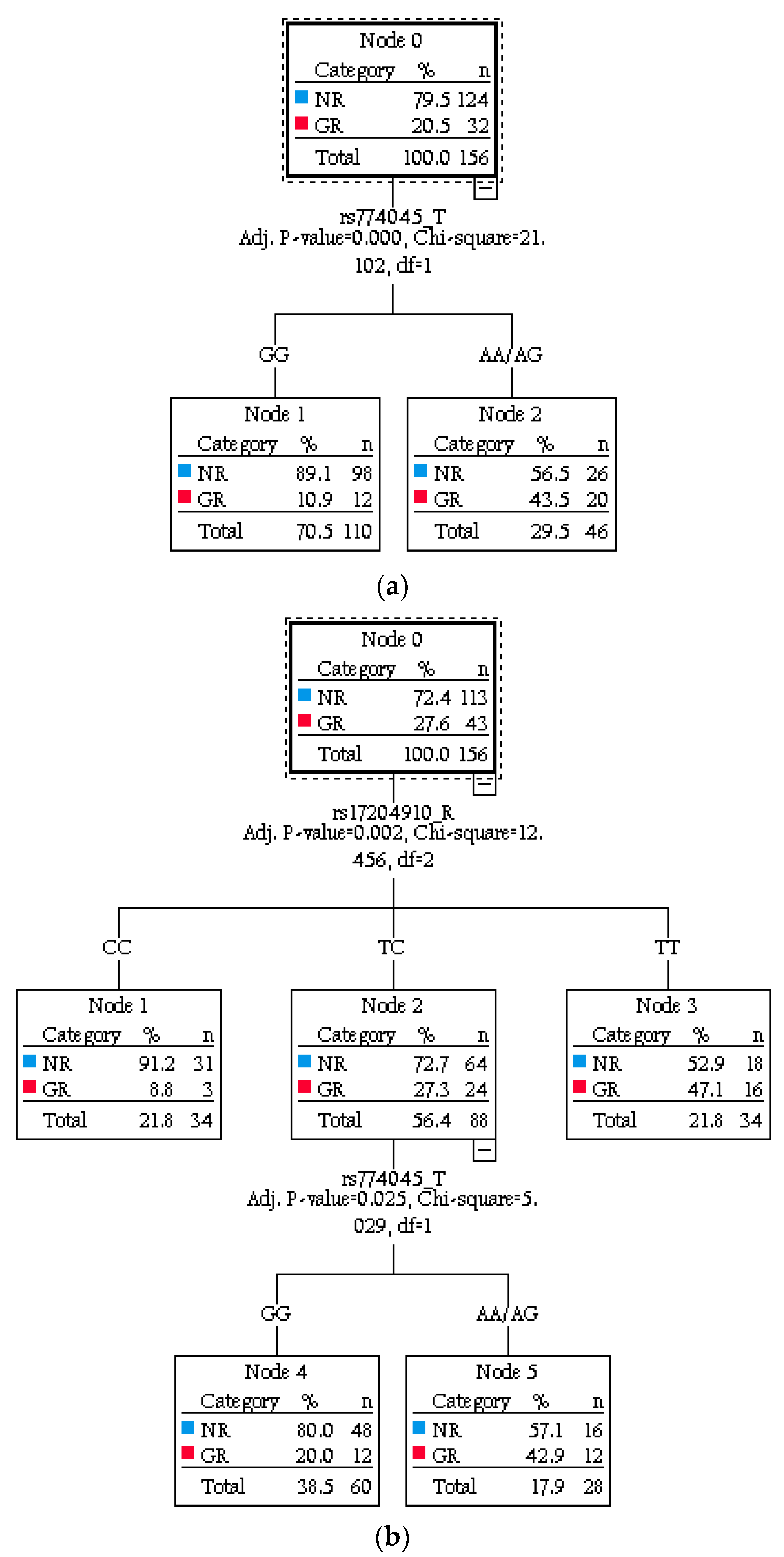
2.3. Associations between Genotypes and Li Response Phenotypes
3. Discussion
4. Materials and Methods
4.1. Sample
4.2. Phenotyping
- (a)
- Original approaches to rating the Alda scaleThe three most widely used approaches are:
- -
- Total Score (TS): a continuous measure represented by the TS (A scale minus B scale score); if B > A, then the TS is reported as zero.
- -
- Original classification (Alda Cats): Li response categorized as GR (TS >= 7) or NR (TS < 7).
- -
- A score in cases with a low B scale score (A/Low B): Li response is represented by the A scale score (continuous variable), but assessment is restricted to individuals with B < 4; those with high B scores are excluded from the analysis.
- (b)
- Machine learning approach to rating the Alda scaleIn the best estimate classification approach, a machine learning algorithm determines a set of “if–then” rules for determining the probability of GR and NR. The analysis enters the B scale item scores in a sequence; this usually starts with treatment complexity (adherence and polypharmacy), then duration of Li treatment and/or illness activity (the exact sequence and combination of item scores is generated by the machine learning model). The algorithm stops running once the optimal classification is reached, irrespective of whether all B items have been included (for details, see [16]). Here, we report the findings on Li response phenotypes as a categorical measure (New Algorithm; Algo). To create a continuous measure to compare with TS and A/Low B, we also estimated GRp (a measure of probability of GR in this sample).
4.3. Genotyping, Quality Control and Selection of Polymorphisms in RORA, PPARGC1A and TIMELESS
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verdolini, N.; Hidalgo-Mazzei, D.; Del Matto, L.; Muscas, M.; Pacchiarotti, I.; Murru, A.; Samalin, L.; Aedo, A.; Tohen, M.; Grunze, H.; et al. Long-term treatment of bipolar disorder type I: A systematic and critical review of clinical guidelines with derived practice algorithms. Bipolar Disord. 2021, 23, 324–340. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Bell, E.; Boyce, P.; Bassett, D.; Berk, M.; Bryant, R.; Gitlin, M.; Hamilton, A.; Hazell, P.; Hopwood, M.; et al. The 2020 Royal Australian and New Zealand College of psychiatrists clinical practice guidelines for mood disorders: Bipolar disorder summary. Bipolar Disord. 2020, 22, 805–821. [Google Scholar] [CrossRef]
- Laroche, D.G.; Etain, B.; Severus, E.; Scott, J.; Bellivier, F. Socio-demographic and clinical predictors of outcome to long-term treatment with lithium in bipolar disorders: A systematic review of the contemporary literature and recommendations from the ISBD/IGSLI Task Force on treatment with lithium. Int. J. Bipolar Disord. 2020, 8, 40. [Google Scholar] [CrossRef]
- Scott, J.; Etain, B.; Bellivier, F. Can an Integrated Science Approach to Precision Medicine Research Improve Lithium Treatment in Bipolar Disorders? Front. Psychiatry 2018, 9, 360. [Google Scholar] [CrossRef] [Green Version]
- Hui, T.P.; Kandola, A.; Shen, L.; Lewis, G.; Osborn, D.P.J.; Geddes, J.R.; Hayes, J.F. A systematic review and meta-analysis of clinical predictors of lithium response in bipolar disorder. Acta Psychiatr. Scand. 2019, 140, 94–115. [Google Scholar] [CrossRef] [Green Version]
- Schulze, T.G.; Alda, M.; Adli, M.; Akula, N.; Ardau, R.; Bui, E.T.; Chillotti, C.; Cichon, S.; Czerski, P.; Del Zompo, M.; et al. The International Consortium on Lithium Genetics (ConLiGen): An Initiative by the NIMH and IGSLI to Study the Genetic Basis of Response to Lithium Treatment. Neuropsychobiology 2010, 62, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Senner, F.; Kohshour, M.O.; Abdalla, S.; Papiol, S.; Schulze, T.G. The Genetics of Response to and Side Effects of Lithium Treatment in Bipolar Disorder: Future Research Perspectives. Front. Pharmacol. 2021, 12, 638882. [Google Scholar] [CrossRef]
- Turecki, G.; Grof, P.; Grof, E.; D’Souza, V.; Lebuis, L.; Marineau, C.; Cavazzoni, P.; Duffy, A.; Bétard, C.; Zvolský, P.; et al. Mapping susceptibility genes for bipolar disorder: A pharmacogenetic approach based on excellent response to lithium. Mol. Psychiatry 2001, 6, 570–578. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.; Hidalgo-Mazzei, D.; Strawbridge, R.; Young, A.; Resche-Rigon, M.; Etain, B.; Andreassen, O.A.; Bauer, M.; Bennabi, D.; Blamire, A.M.; et al. Prospective cohort study of early biosignatures of response to lithium in bipolar-I-disorders: Overview of the H2020-funded R-LiNK initiative. Int. J. Bipolar Disord. 2019, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Vecera, C.; Fries, G.; Shahani, L.; Soares, J.; Machado-Vieira, R. Pharmacogenomics of Lithium Response in Bipolar Disorder. Pharmaceuticals 2021, 14, 287. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, C.S.; Lee, M.T.; Ouyang, W.C.; Chen, C.C.; Chong, M.Y.; Wu, J.Y.; Tan, H.K.; Lee, Y.C.; Chuo, L.J.; et al. Variant GADL1 and response to lithium therapy in bipolar I disorder. N. Engl. J. Med. 2014, 370, 119–128. [Google Scholar] [CrossRef]
- Chen, C.-K.; Lee, C.-S.; Chen, H.-Y.; Wu, L.S.-H.; Chang, J.-C.; Liu, C.-Y.; Cheng, A.T.-A. GADL1 variant and medication adherence in predicting response to lithium maintenance treatment in bipolar I disorder. BJPsych Open 2016, 2, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Grof, P.; Duffy, A.; Cavazzoni, P.; Grof, E.; Garnham, J.; MacDougall, M.; O’Donovan, C.; Alda, M. Is response to prophylactic lithium a familial trait? J. Clin. Psychiatry 2002, 63, 942–947. [Google Scholar] [CrossRef]
- Nunes, A.; Trappenberg, T.; Alda, M. The international Consortium on Lithium Genetics (ConLiGen) Asymmetrical reliability of the Alda score favours a dichotomous representation of lithium responsiveness. PLoS ONE 2020, 15, e0225353. [Google Scholar] [CrossRef] [Green Version]
- Manchia, M.; Adli, M.; Akula, N.; Ardau, R.; Aubry, J.-M.; Backlund, L.; Banzato, C.; Baune, B.T.; Bellivier, F.; Bengesser, S.; et al. Assessment of Response to Lithium Maintenance Treatment in Bipolar Disorder: A Consortium on Lithium Genetics (ConLiGen) Report. PLoS ONE 2013, 8, e65636. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.; Etain, B.; Manchia, M.; Brichant-Petitjean, C.; Geoffroy, P.A.; Schulze, T.; Alda, M.; Bellivier, F.; Amare, A.; Ardau, R.; et al. An examination of the quality and performance of the Alda scale for classifying lithium response phenotypes. Bipolar Disord. 2020, 22, 255–265. [Google Scholar] [CrossRef]
- Scott, J.; Bellivier, F.; Manchia, M.; Schulze, T.; Alda, M.; Etain, B.; Investigators Involved in the ConLiGen Collaboration; Cervantes, P.; Garnham, J.; Nunes, A.; et al. Can network analysis shed light on predictors of lithium response in bipolar I disorder? Acta Psychiatr. Scand. 2020, 141, 522–533. [Google Scholar] [CrossRef]
- Scott, J.; Hennion, V.; Meyrel, M.; Bellivier, F.; Etain, B. An ecological study of objective rest–activity markers of lithium response in bipolar-I-disorder. Psychol. Med. 2020, 13, 1–9. [Google Scholar] [CrossRef]
- McCarthy, M.J. Missing a beat: Assessment of circadian rhythm abnormalities in bipolar disorder in the genomic era. Psychiatr. Genet. 2019, 29, 29–36. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Wei, H.; Nievergelt, C.M.; Stautland, A.; Maihofer, A.X.; Welsh, D.K.; Shilling, P.; Alda, M.; Alliey-Rodriguez, N.; Anand, A.; et al. Chronotype and cellular circadian rhythms predict the clinical response to lithium maintenance treatment in patients with bipolar disorder. Neuropsychopharmacology 2019, 44, 620–628. [Google Scholar] [CrossRef]
- Oliveira, T.; Marinho, V.; Carvalho, V.; Magalhães, F.; Rocha, K.; Ayres, C.; Teixeira, S.; Nunes, M.; Bastos, V.H.; Pinto, G. Genetic polymorphisms associated with circadian rhythm dysregulation provide new perspectives on bipolar disorder. Bipolar Disord. 2018, 20, 515–522. [Google Scholar] [CrossRef]
- Xu, N.; Shinohara, K.; Saunders, K.E.A.; Geddes, J.R.; Cipriani, A. Effect of lithium on circadian rhythm in bipolar disorder: A systematic review and meta-analysis. Bipolar Disord. 2021, 23, 445–453. [Google Scholar] [CrossRef]
- Moreira, J.; Geoffroy, P.A. Lithium and bipolar disorder: Impacts from molecular to behavioural circadian rhythms. Chronobiol. Int. 2016, 33, 351–373. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Nievergelt, C.M.; Kelsoe, J.R.; Welsh, D.K. A Survey of Genomic Studies Supports Association of Circadian Clock Genes with Bipolar Disorder Spectrum Illnesses and Lithium Response. PLoS ONE 2012, 7, e32091. [Google Scholar] [CrossRef] [Green Version]
- Pisanu, C.; Congiu, D.; Melis, C.; Severino, G.; Angius, A.; Ardau, R.; Chillotti, C.; Del Zompo, M.; Squassina, A. Involvement of core clock genes in lithium response. World J. Biol. Psychiatry 2018, 19, 645–646. [Google Scholar] [CrossRef]
- Etain, B.; Jamain, S.; Milhiet, V.; Lajnef, M.; Boudebesse, C.; Dumaine, A.; Mathieu, F.; Gombert, A.; Ledudal, K.; Gard, S.; et al. Association between circadian genes, bipolar disorders and chronotypes. Chronobiol. Int. 2014, 31, 807–814. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Etain, B.; Lajnef, M.; Zerdazi, E.-H.; Brichant-Petitjean, C.; Heilbronner, U.; Hou, L.; Degenhardt, F.; Rietschel, M.; McMahon, F.; et al. Circadian genes and lithium response in bipolar disorders: Associations with PPARGC1A (PGC-1α) and RORA. Genes Brain Behav. 2016, 15, 660–668. [Google Scholar] [CrossRef] [Green Version]
- Geoffroy, P.A.; Curis, E.; Courtin, C.; Moreira, J.; Morvillers, T.; Etain, B.; Laplanche, J.-L.; Bellivier, F.; Marie-Claire, C. Lithium response in bipolar disorders and core clock genes expression. World J. Biol. Psychiatry 2018, 19, 619–632. [Google Scholar] [CrossRef]
- Rybakowski, J.K.; Dmitrzak-Weglarz, M.; Kliwicki, S.; Hauser, J. Polymorphism of circadian clock genes and prophylactic lithium response. Bipolar Disord. 2013, 16, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Heilbronner, U.; Degenhardt, F.; Adli, M.; Akiyama, K.; Akula, N.; Ardau, R.; Arias, B.; Backlund, L.; Banzato, C.; et al. Genetic variants associated with response to lithium treatment in bipolar disorder: A genome-wide association study. Lancet 2016, 387, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Hou, L.; Bergen, S.E.; Akula, N.; Song, J.; Hultman, C.M.; Landén, M.; Adli, M.; Alda, M.; Ardau, R.; Arias, B.; et al. Genome-wide association study of 40,000 individuals identifies two novel loci associated with bipolar disorder. Hum. Mol. Genet. 2016, 25, 3383–3394. [Google Scholar] [CrossRef]
- Stone, W.; Nunes, A.; Akiyama, K.; Akula, N.; Ardau, R.; Aubry, J.-M.; Backlund, L.; Bauer, M.; Bellivier, F.; Cervantes, P.; et al. Prediction of lithium response using genomic data. Sci. Rep. 2021, 11, 1155. [Google Scholar] [CrossRef]
- Ching, C.R.K.; Hibar, D.P.; Gurholt, T.P.; Nunes, A.; Thomopoulos, S.I.; Abé, C.; Agartz, I.; Brouwer, R.M.; Cannon, D.M.; de Zwarte, S.M.; et al. What we learn about bipolar disorder from large-scale neuroimaging: Findings and future directions from the ENIGMA Bipolar Disorder Working Group. Hum. Brain Mapp. 2020, 29, 1–27. [Google Scholar] [CrossRef]
- Frey, B.N.; Andreazza, A.C.; Houenou, J.; Jamain, S.; Goldstein, B.I.; Frye, M.A.; Leboyer, M.; Berk, M.; Malhi, G.S.; Lopez, C.; et al. Biomarkers in bipolar disorder: A positional paper from the International Society for Bipolar Disorders Biomarkers Task Force. Aust. N. Z. J. Psychiatry 2013, 47, 321–332. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Preisig, M.; Fenton, B.T.; Matthey, M.-L.; Berney, A.; Ferrero, F. Diagnostic interview for genetic studies (DIGS): Inter-rater and test-retest reliability of the French version. Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 174–179. [Google Scholar] [CrossRef]
- Nurnberger, J.I.; Blehar, M.C.; Kaufmann, C.A.; York-Cooler, C.; Simpson, S.G.; Harkavyfriedman, J.M.; Severe, J.B.; Malaspina, D.; Reich, T. Diagnostic interview for genetic studies: Rationale, unique features, and training. NIMH Genetics Initiative. Arch. Gen. Psychiatry 1994, 51, 849–859. [Google Scholar] [CrossRef]
- Tohen, M.; Frank, E.; Bowden, C.L.; Colom, F.; Ghaemi, S.N.; Yatham, L.N.; Malhi, G.S.; Calabrese, J.R.; Nolen, W.A.; Vieta, E.; et al. The International Society for Bipolar Disorders (ISBD) Task Force report on the nomenclature of course and outcome in bipolar disorders. Bipolar Disord. 2009, 11, 453–473. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry J. Ment. Sci. 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry J. Ment. Sci. 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A Tool Set for Whole-Genome Association and Population-Based Linkage Analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Mean (s.d.) or Number (% *) |
|---|---|
| Demography and diagnosis | |
| Female | 99 (60%) |
| Mean age at interview in years | 44.70 (12.29) |
| Bipolar Disorder type I | 128 (78%) |
| Mean duration of illness in years | 19.43 (11.27) |
| Alda Scale scores | |
| A scale score | 6.33 (2.99) |
| B scale items: prevalence of raw scores ** | |
| B1—Number of episodes pre-Li | 112 (68%): 45 (27%): 8 (5%) |
| B2—Frequency of episodes pre-Li | 100 (61%): 57 (34%): 8 (5%) |
| B3—Duration Li treatment | 122 (74%): 15 (9%): 28 (17%) |
| B4—Adherence to Li | 18 (11%): 140 (85%): 7 (4%) |
| B5—Co-prescriptions/Polypharmacy | 57 (34%): 63 (39%): 45 (27%) |
| Genotypes *** | |
| RORA (rs17204910) | CC: 34 - TC: 88 - TT: 34 |
| PPARGC1A (rs2932965) | AA: 23 - AG: 79 - GG: 53 |
| TIMELESS (rs774045) | AA: 1 - AG: 45 - GG: 110 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, J.; Lajnef, M.; Icick, R.; Bellivier, F.; Marie-Claire, C.; Etain, B. A Comparison of Different Approaches to Clinical Phenotyping of Lithium Response: A Proof of Principle Study Employing Genetic Variants of Three Candidate Circadian Genes. Pharmaceuticals 2021, 14, 1072. https://doi.org/10.3390/ph14111072
Scott J, Lajnef M, Icick R, Bellivier F, Marie-Claire C, Etain B. A Comparison of Different Approaches to Clinical Phenotyping of Lithium Response: A Proof of Principle Study Employing Genetic Variants of Three Candidate Circadian Genes. Pharmaceuticals. 2021; 14(11):1072. https://doi.org/10.3390/ph14111072
Chicago/Turabian StyleScott, Jan, Mohamed Lajnef, Romain Icick, Frank Bellivier, Cynthia Marie-Claire, and Bruno Etain. 2021. "A Comparison of Different Approaches to Clinical Phenotyping of Lithium Response: A Proof of Principle Study Employing Genetic Variants of Three Candidate Circadian Genes" Pharmaceuticals 14, no. 11: 1072. https://doi.org/10.3390/ph14111072
APA StyleScott, J., Lajnef, M., Icick, R., Bellivier, F., Marie-Claire, C., & Etain, B. (2021). A Comparison of Different Approaches to Clinical Phenotyping of Lithium Response: A Proof of Principle Study Employing Genetic Variants of Three Candidate Circadian Genes. Pharmaceuticals, 14(11), 1072. https://doi.org/10.3390/ph14111072