
COVID-19: Failure of the DisCoVeRy Clinical Trial, and Now–New Hopes?


Abstract
:
1. Introduction
- Hydroxychloroquine, eventually associated with the antibiotic azithromycin;
- The combination lopinavir/ritonavir;
- The combination lopinavir/ritonavir with the addition of interferon β-1a;
- Remdesivir.
2. The DisCoVeRy Clinical Trial
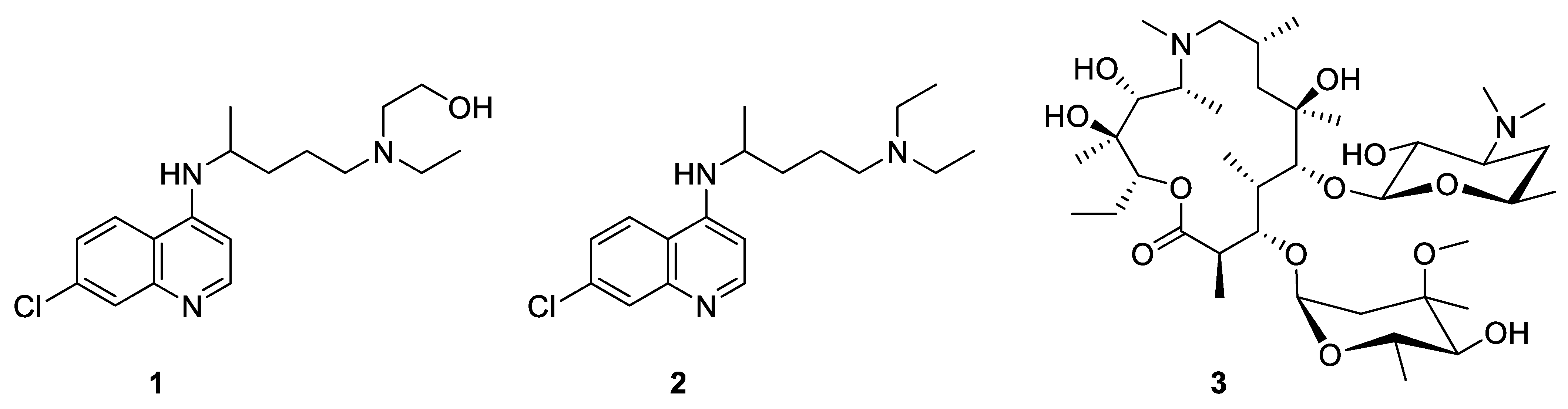
2.1. Hydroxychloroquine, Eventually Associated with Azithromycin
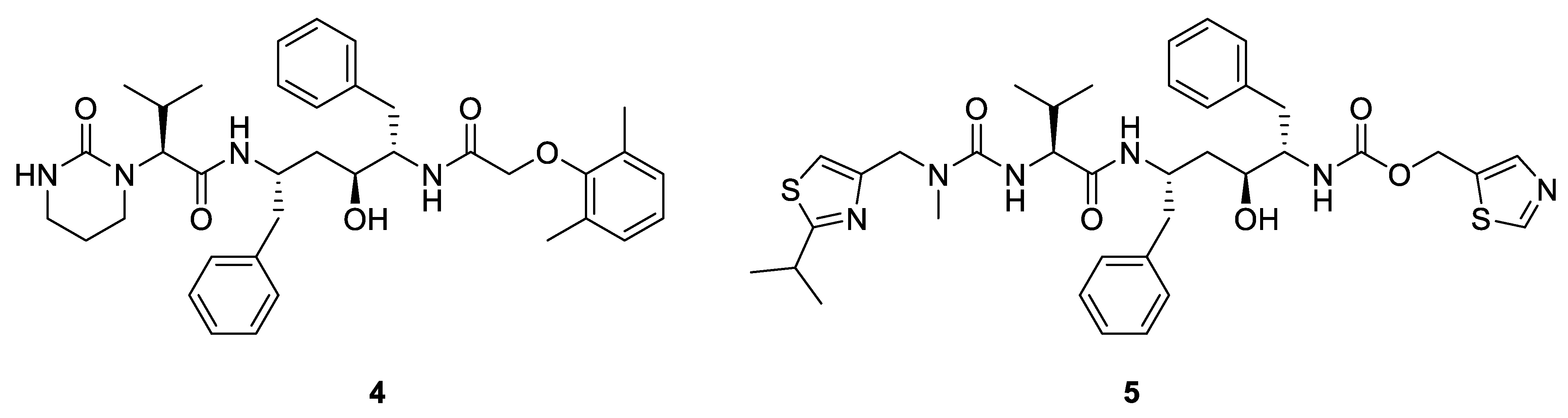
2.2. The Combination Lopinavir/Ritonavir and the Combination with the Addition of Interferon β-1a
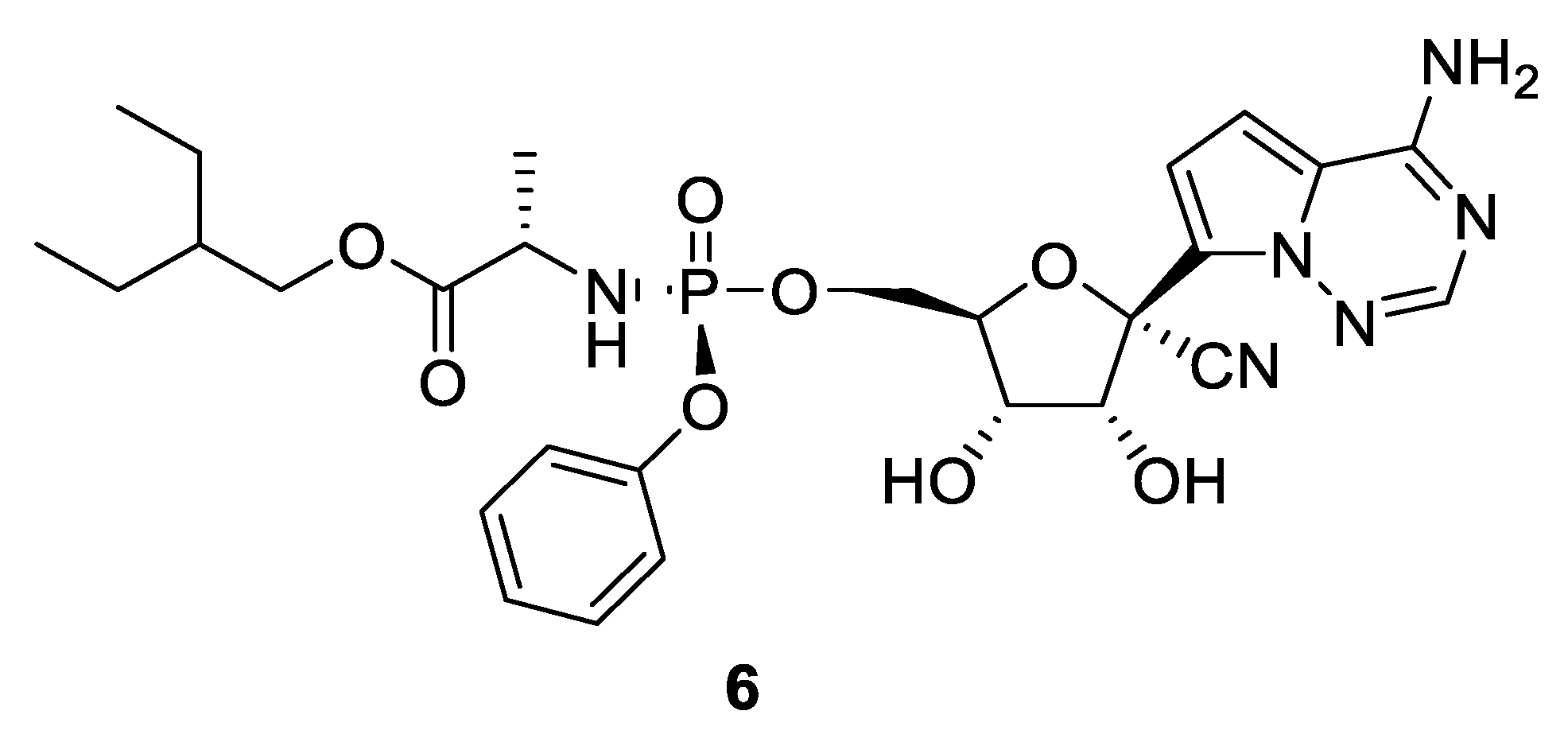
2.3. Remdesivir
2.4. The Conclusions of the DisCoVeRy Trial
3. New Hopes?
3.1. Vaccines
- Use of mRNA encoding a fragment of the spike protein;
- Use of a harmless virus that will produce spike proteins and consequently induce the immune response;
- Use of spike proteins themselves.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccine (Manufacturer) | Type of Vaccine | Number of Shots | Number of Doses Secured by the EU | Price per Dose in Euros (Tax Excluded) |
|---|---|---|---|---|
| Vaxzevria (AstraZeneca/Oxford) | Viral vector | 2 | 400 million | 1.78 |
| Comirnati (BioNTech/Pfizer) | mRNA | 2 | 2.4 billion | 12.00 |
| CVnCoV (CureVac) | mRNA | 2 | 405 million | 10.00 |
| Johnson & Johnson (Janssen) | Viral vector | 1 | 400 million | 7.08 |
| Spikevax (Moderna) | mRNA | 2 | 460 million | 15.00 |
| VAT00008 (Sanofi/GSK) | Protein-vector | 2 | 300 million | 7.56 |
3.2. Small Molecules
- Early inhibition of the interaction virus-host cells;
- Action on the virus replication;
- Late control of the cytokine storm.
3.2.1. Inhibition of the Interaction Virus-Host Cells
3.2.2. Action on the Virus Replication
3.2.3. Control of the Cytokine Storm
3.3. Antibodies
3.3.1. Convalescent Plasma
3.3.2. Monoclonal Antibodies
Inhibition of the Interaction Virus-Host Cells
Control of the Cytokine Storm
3.4. Mesenchymal Stem Cells
4. Official Status of the Potential Treatments
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krueger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 1–10. [Google Scholar] [CrossRef]
- Rathnayake, A.D.; Zheng, J.; Kim, Y.; Perera, K.D.; Mackin, S.; Meyerholz, D.K.; Kashipathy, M.M.; Battaile, K.P.; Lovell, S.; Perlman, S.; et al. 3C-like protease inhibitors block coronavirus replication in vitro and improve survival in MERS-CoV–infected mice. Sci. Transl. Med. 2020, 12, eabc5332. [Google Scholar] [CrossRef] [PubMed]
- Boras, B.; Jones, R.M.; Anson, B.J.; Arenson, D.; Aschenbrenner, L.; Bakowski, M.A.; Beutler, N.; Binder, J.; Chen, E.; Eng, H.; et al. Discovery of a novel inhibitor of coronavirus 3CL protease for the potential treatment of COVID-19. BioRxiv 2021. [Google Scholar] [CrossRef]
- WHO. UN Foundation and Partners Launch First-of-Its-Kind COVID-19 Solidarity Response Fund. Available online: https://www.who.int/news-room/detail/13-03-2020-who-un-foundation-and-partners-launch-first-of-its-kind-covid-19-solidarity-response-fund (accessed on 15 June 2021).
- An International Randomized Trial of Additional Treatments for COVID-19 in Hospitalized Patients Who Are All Receiving the Local Standard of Care. Available online: https://www.who.int/publications/m/item/an-international-randomised-trial-of-additional-treatments-for-covid-19-in-hospitalised-patients-who-are-all-receiving-the-local-standard-of-care (accessed on 15 June 2021).
- Treatments for COVID-19: Canadian Arm of the SOLIDARITY Trial (CATCO). Available online: https://clinicaltrials.gov/ct2/show/NCT04330690 (accessed on 15 June 2021).
- An International Randomized Trial of Additional Treatments for COVID-19 in Hospitalized Patients Who Are All Receiving the Local Standard of Care—WHO-SOLIDARITY-GERMANY. Available online: https://clinicaltrials.gov/ct2/show/NCT04575064 (accessed on 15 June 2021).
- World Health Organization (WHO) COVID-19 Solidarity Trial for COVID-19 Treatments (SOLIDARITY). Available online: https://clinicaltrials.gov/ct2/show/NCT04647669 (accessed on 15 June 2021).
- The (Norwegian) NOR Solidarity Multicenter Trial on the Efficacy of Different Anti-Viral Drugs in SARS-CoV-2 Infected Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04321616 (accessed on 15 June 2021).
- Launch of a European Clinical Trial against COVID-19. Available online: https://presse.inserm.fr/en/launch-of-a-european-clinical-trial-against-covid-19/38737/ (accessed on 15 June 2021).
- Trial of Treatments for COVID-19 in Hospitalized Adults (DisCoVeRy). Available online: https://clinicaltrials.gov/ct2/show/NCT04315948 (accessed on 15 June 2021).
- Vanden Eynde, J.J. COVID-19: A brief overview of the Discovery clinical trial. Pharmaceuticals 2020, 13, 65. [Google Scholar] [CrossRef] [PubMed]
- Vanden Eynde, J.J. COVID-19: An update about the Discovery clinical trial. Pharmaceuticals 2020, 13, 98. [Google Scholar] [CrossRef]
- Ader, F.; Discovery French Trial Management Team. Protocol for the DisCoVeRy trial: Multicentre, adaptive, randomised trial of the safety and efficacy of treatments for COVID-19 in hospitalised adults. BMJ Open 2020, 10, e041437. [Google Scholar] [CrossRef]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends 2020, 14, 72–73. [Google Scholar] [CrossRef] [Green Version]
- Gautret, P.; Lagiera, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Esteves Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Molina, J.M.; Delaugerre, C.; Le Goff, J.; Mela-Lima, B.; Ponscarme, D.; Goldwirt, L.; de Castro, N. No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med. Mal. Infect. 2020, 50, 384. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, S.; Dassarma, B.; Roy, S.; Chabalala, H.; Matsabis, M.G. A review on possible modes of action of chloroquine/hydroxychloroquine: Repurposing against SAR-CoV-2 (COVID-19) pandemic. Int. J. Antimicrob. Agents. 2020, 56, 106028. [Google Scholar] [CrossRef] [PubMed]
- Satarker, S.; Ahuja, T.; Banerjee, M.; Dogra, S.; Agarwal, T.; Nampoothiri, M. Hydroxychloroquine in COVID-19: Potential mechanism of action against SARS-CoV-2. Curr. Pharmacol. Rep. 2020, 6, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Devaux, C.A.; Camoin-Jau, L.; Mege, J.-L.; Raoult, D. Can hydroxychloroquine be protective against COVID-19-associated thrombotic events? J. Microbiol. Immunol. Infect. 2021, 54, 37–45. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine-Clinical Trials. Available online: https://clinicaltrials.gov/ct2/home (accessed on 15 June 2021).
- Catteau, L.; Dauby, N.; Montourcy, M.; Bottieau, E.; Hautekiet, J.; Goetghebeur, E.; van Ierssel, S.; Duysburgh, E.; Van Oyen, H.; Whyndham-Thomas, C.; et al. Low-dose hydroxychloroquine therapy and mortality in hospitalized patients with COVID-19: A nationwide observational study of 8075 participants. Int. J. Antimicrob. Agents 2020, 56, 106144. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Application Numbers 21–226 and 21–251. Approval Letter. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2000/21-226_Kaletra_Approv.pdf (accessed on 15 June 2021).
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A trial of Lopinavir–Ritonavir in adults hospitalized with severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Nutho, B.; Mahalapbutr, P.; Hengphasatporn, K.; Pattaranggoon, N.C.; Simanon, N.; Shigeta, Y.; Hannongbua, S.; Rungrotmongkol, T. Why are lopinavir and ritonavir effective against the newly emerged coronavirus 2019? Atomistic insights into the inhibitory mechanisms. Biochemistry 2020, 59, 1769–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, M.; Pichlmair, A.; Mühlberger, E.; Haller, O.; Weber, F. The antiviral effect of interferon-beta against SARS-Coronavirus is not mediated by MxA protein. J. Clin. Virol. 2004, 30, 211–213. [Google Scholar] [CrossRef]
- Hensley, L.E.; Fritz, E.A.; Jahrling, P.B.; Karp, C.L.; Huggins, J.W.; Geisbert, T.W. Interferon-β 1a and SARS coronavirus replication. Emerg. Infect. Dis. 2004, 10, 317–319. [Google Scholar] [CrossRef]
- Hart, B.; Dyall, J.; Postnikova, E.; Zhou, H.; Kindrachuk, J.; Johnson, R.F.; Olinger, G.; Frieman, M.B.; Holbrook, M.R.; Jahrling, P.B.; et al. Interferon-β and mycophenolic acid are potent inhibitors of Middle East respiratory syndrome coronavirus in cell-based assays. J. Gen. Virol. 2014, 95, 571–577. [Google Scholar] [CrossRef]
- González-Navajas, J.M.; Lee, J.; David, M.; Raz, E. Immunomodulatory functions of type I interferons. Nat. Rev. Immunol. 2012, 12, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, G. The role of type I interferons in the pathogenesis and treatment of COVID-19. Front. Immunol. 2020, 11, 595739. [Google Scholar] [CrossRef]
- Abdolvahab, M.H.; Moradi-kalbolandi, S.; Zarei, M.; Bose, D.; Majidzadeh-A, K.; Farahmand, L. Potential role of interferons in treating COVID-19 patients. Int. Immunopharmacol. 2021, 90, 107171. [Google Scholar] [CrossRef]
- Monk, P.D.; Marsden, R.J.; Tear, V.J.; Brookes, J.; Batten, T.N.; Mankowski, M.; Gabbay, F.J.; Davies, D.E.; Holgate, S.T.; Ho, L.-P.; et al. Safety and efficacy of inhaled nebulised interferon beta-1a (SNG001) for treatment of SARS-CoV-2 infection: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Respir. Med. 2021, 9, 196–206. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yao, Y.; Yeung, M.-L.; Deng, W.; Bao, L.; Jia, L.; Li, F.; Xiao, C.; Gao, H.; Yu, P.; et al. Treatment with Lopinavir/Ritonavir or Interferon-β1b improves outcome of MERS-CoV infection in a nonhuman primate model of common marmoset. J. Infect. Dis. 2015, 212, 1904–1913. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Asiri, A.Y.; Assiri, A.M.; Balkhy, H.H.; Bshabshe, A.A.; Jeraisy, M.A.; Mandourah, Y.; Azzam, M.H.A.; Eshaq, A.M.B.; Johani, S.A.; et al. Interferon beta-1b and lopinavir–ritonavir for Middle East respiratory syndrome. N. Engl. J. Med. 2020, 383, 1645–1656. [Google Scholar] [CrossRef]
- Baghaei, P.; Dastan, F.; Marjani, M.; Moniri, A.; Abtahian, Z.; Ghadimi, S.; Valizadeh, M.; Heshmatnia, J.; Mirenayat, M.S.; Abedini, A.; et al. Combination therapy of IFNβ1 with lopinavir–ritonavir, increases oxygenation, survival and discharging of severe COVID-19 infected inpatients. Int. Immunol. 2021, 92, 107329. [Google Scholar] [CrossRef]
- Investigational Therapeutics for the Treatment of People with Ebola Virus Disease. Available online: https://clinicaltrials.gov/ct2/show/results/NCT03719586 (accessed on 15 June 2021).
- Mulangu, S.; Dodd, L.E.; Davey, R.T., Jr.; Tshiani Mbaya, O.; Proschan, M.; Mukadi, D.; Lusakibanza Manzo, M.; Nzolo, D.; Tshomba Oloma, A.; Ibanda, A.; et al. A randomized, controlled trial of Ebola virus disease therapeutics. N. Engl. J. Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef] [PubMed]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Adaptive COVID-19 Treatment Trial (ACTT). Available online: https://clinicaltrials.gov/ct2/show/NCT04280705 (accessed on 15 June 2021).
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the treatment of Covid-19—Final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research. Approval Package. Application Number 214787Orig1s000. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/214787Orig1s000Approv.pdf (accessed on 15 June 2021).
- Press Release—INSERM Press Room: Discovery Stops Testing Remdesivir against Covid-19 for Lack of Evidence of Its Efficacy. Available online: https://presse.inserm.fr/en/discovery-stops-testing-remdesivir-against-covid-19-for-lack-of-evidence-of-its-efficacy/42034/ (accessed on 15 June 2021).
- European Commission Authorises First Treatment against COVID-19. Available online: https://ec.europa.eu/commission/presscorner/detail/en/mex_20_1266 (accessed on 15 June 2021).
- Kokic, G.; Hillen, H.S.; Tegunov, D.; Dienemann, C.; Seitz, F.; Schmitzova, J.; Farnung, L.; Siewert, A.; Höbartner, C.; Cramer, P. Mechanism of SARS-CoV-2 polymerase stalling by remdesivir. Nat. Commun. 2021, 12, 279. [Google Scholar] [CrossRef]
- Cao, Y.C.; Deng, Q.X.; Dai, S.X. Remdesivir for severe acute respiratory syndrome coronavirus 2 causing COVID-19: An evaluation of the evidence. Travel Med. Infect. Dis. 2020, 35, 101647. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.L.; Thai, N.Q.; Truong, D.T.; Li, M.S. Remdesivir strongly binds to both RNA-dependent RNA polymerase and Main protease of SARS-CoV-2: Evidence from molecular simulations. J. Phys. Chem. B 2020, 124, 11337–11348. [Google Scholar] [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium. Repurposed antiviral drugs for Covid-19—Interim WHO Solidarity trial results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics and COVID-19. Living Guideline. 31 March 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2021.1 (accessed on 15 June 2021).
- Kumar, A.; Kumar, A. Mucosal and transdermal vaccine delivery strategies against SARS-CoV-2. Drug Deliv. Transl. Res. 2021. [Google Scholar] [CrossRef]
- Olliaro, P.; Torreele, E.; Vaillant, M. COVID-19 vaccine efficacy and effectiveness—The elephant (not) in the room. Lancet Microbe 2021. [Google Scholar] [CrossRef]
- Francica, J.R.; Flynn, B.J.; Foulds, K.E.; Noe, A.T.; Werner, A.P.; Moore, I.N.; Gagne, M.; Johnston, T.S.; Tucker, C.; Davis, R.L. Vaccination with SARS-CoV-2 spike protein and AS03 adjuvant induces rapid anamnestic antibodies in the lung and protects against virus challenge in nonhuman primates. BioRxiv 2021. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Picot, M.-C.; Bousquet, J. Spike antibody levels of nursing home residents with or without prior COVID-19 3 weeks after a single BNT162b2 vaccine dose. JAMA 2021, 325, 1898–1899. [Google Scholar] [CrossRef]
- Edara, V.V.; Hudson, W.H.; Xie, X.; Ahmed, R.; Suthar, M.S. Neutralizing antibodies against SARS-CoV-2 variants after infection and vaccination. JAMA 2021, 325, 1896–1898. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 infection after vaccination in health care workers in California. N. Engl. J. Med. 2021, 348, 18. [Google Scholar] [CrossRef]
- Zimet, G.D.; Silverman, R.D.; Fortenberry, J.D. Coronavirus disease 2019 and vaccination of children and adolescents: Prospects and challenges. J. Pediatr. 2021, 231, 254–258. [Google Scholar] [CrossRef] [PubMed]
- COVID-19. Vaccination Tracker. Available online: https://graphics.reuters.com/world-coronavirus-tracker-and-maps/vaccination-rollout-and-access/ (accessed on 15 June 2021).
- Safe COVID-19 Vaccines for Europeans. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/safe-covid-19-vaccines-europeans_en (accessed on 15 June 2021).
- Dyer, O. Covid-19: Countries are learning what others paid for vaccines. BMJ 2021, 372, n281. [Google Scholar] [CrossRef]
- FOIPAN® Tablets 100 mg. Available online: http://www.shijiebiaopin.net/upload/product/201272318373223.PDF (accessed on 15 June 2021).
- Motoo, Y. Antiproteases in the treatment of chronic pancreatitis. JOP J. Pancreas 2007, 8, 533–537. [Google Scholar]
- Kawase, M.; Shirato, K.; van der Hoek, L.; Taguchi, F.; Matsuyama, S. Simultaneous treatment of human bronchial epithelial cells with serine and cysteine protease inhibitors prevents severe acute respiratory syndrome coronavirus entry. J. Virol. 2012, 86, 6537–6545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Vedantham, P.; Lu, K.; Agudelo, J.; Carrion, R., Jr.; Nunneley, J.W.; Barnard, D.; Phoelmann, L.; McKerrow, J.H.; Renslo, A.R.; et al. Protease inhibitors targeting coronavirus and filovirus entry. Antivir. Res. 2015, 116, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmidt, K. These drugs don’t target the coronavirus—They target us. ScienceMag 2020. Available online: https://www.sciencemag.org/news/2020/04/these-drugs-don-t-target-coronavirus-they-target-us (accessed on 15 June 2021). [CrossRef]
- Hoffmann, M.; Hofmann-Winkler, H.; Smith, J.C.; Krueger, N.; Arora, P.; Sørensen, L.K.; Søgaard, O.S.; Hasselstrøm, J.B.; Winkler, M.; Hempel, T.; et al. Camostat mesylate inhibits SARS-CoV-2 activation by TMPRSS2-related proteases and its metabolite GBPA exerts antiviral activity. EBioMedicine 2021, 65, 103255. [Google Scholar] [CrossRef]
- Hoffmann, M.; Schroeder, S.; Kleine-Weber, H.; Müller, M.A.; Drosten, C.; Pöhlmann, S. Nafamostat mesylate blocks activation of SARS-CoV-2: New treatment option for COVID-19. Antimicrob. Agents Chemother. 2020, 64, e00754-20. [Google Scholar] [CrossRef] [Green Version]
- Ko, M.; Jeon, S.; Ryu, W.-S.; Kim, S. Comparative analysis of antiviral efficacy of FDA-approved drugs against SARS-CoV-2 in human lung cells. J. Med. Virol. 2020, 93, 1403–1408. [Google Scholar] [CrossRef]
- Blaysing, J.; Polyak, S.J.; Pécheur, E.-I. Arbidol as a braod spectrum antiviral: An update. Antivir. Res. 2014, 107, 84–94. [Google Scholar] [CrossRef]
- Wang, X.; Cao, R.; Zhang, H.; Liu, J.; Xu, M.; Hu, H.; Li, Y.; Zhao, L.; Li, W.; Sun, X.; et al. The anti-influenza virus drug, arbidol is an efficient inhibitor of SARS-CoV-2 in vitro. Cell Discov. 2020, 6, 28. [Google Scholar] [CrossRef]
- Vankadari, N. Arbidol: An antiviral drug for the treatment of SARS-CoV-2 by blocking trimerization of the spike glycoprotein. Int. J. Antimicrob. Agents 2020, 56, 105998. [Google Scholar] [CrossRef]
- Padhi, A.K.; Seal, A.; Khan, J.M.; Ahamed, M.; Tripathi, T. Unraveling the mechanism of arbidol binding and inhibition of SARS-CoV-2: Insights from atomistic simulations. Eur. J. Pharmacol. 2021, 894, 173836. [Google Scholar] [CrossRef] [PubMed]
- Nojomi, M.; Yassin, Z.; Keyvani, H.; Makiani, M.J.; Roham, M.; Laali, A.; Dehghan, N.; Navaei, M.; Ranjbar, M. Effect of arbidol (umifenovir) on COVID-19: A randomized controlled trial. BMC Infect. Dis. 2020, 20, 954. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Yu, H.; Wang, T.; Yang, H.; Yao, R.; Liang, Z. Efficacy and safety of umifenovir for coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Khodashahi, R.; Naderi, H.; Bojdy, A.; Heydari, A.A.; Sani, A.T.; Ghabouli, M.J.; Sarvghad, M.R.; Nateghi, M.H.; Arian, M.; Jahanian, S. Comparison the effect of arbidol plus hydroxychloroquine vs. hydroxychloroquine alone in treatment of COVID-19 disease: A randomized clinical trial. Curr. Respir. Med. Rev. 2021, 16, 252–262. [Google Scholar] [CrossRef]
- Sangawa, H.; Komeno, T.; Nishikawa, H.; Yoshida, A.; Takahashi, K.; Nomura, N.; Furuta, Y. Mechanism of action of T-705 ribosyl triphosphate against influenza virus RNA polymerase. Antimicrob. Agents Chemother. 2013, 57, 5202–5208. [Google Scholar] [CrossRef] [Green Version]
- Shannon, A.; Selisko, B.; Le, N.-T.-T.; Huchting, J.; Touret, F.; Piorkowski, G.; Fattorini, V.; Ferron, F.; Decroly, E.; Meier, C.; et al. Rapid incorporation of Favipiravir by the fast and permissive viral RNA polymerase complex results in SARS-CoV-2 lethal mutagenesis. Nat. Commun. 2020, 11, 4682. [Google Scholar] [CrossRef]
- Kaptein, S.J.F.; Jacobs, S.; Langendriesa, L.; Seldeslachts, L.; ter Horst, S.; Liesenborghs, L.; Hens, B.; Vergote, V.; Heylen, E.; Barthelemy, K.; et al. Favipiravir at high doses has potent antiviral activity in SARS-CoV-2−infected hamsters, whereas hydroxychloroquine lacks activity. Proc. Natl. Acad. Sci. USA 2020, 117, 26955–26965. [Google Scholar] [CrossRef]
- Driouich, J.-S.; Cochin, M.; Lingas, G.; Moureau, G.; Touret, F.; Petit, P.-R.; Piorkowski, G.; Barthélémy, K.; Laprie, C.; Coutard, B.; et al. Favipiravir antiviral efficacy against SARS-CoV-2 in a hamster model. Nat. Commun. 2021, 12, 1735. [Google Scholar] [CrossRef]
- EU Clinical Trials Register: EudraCT Number: 2020-001435-27. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001435-27/FR (accessed on 15 June 2021).
- Control of COVID-19 Outbreaks in Long Term Care. Available online: https://clinicaltrials.gov/ct2/show/NCT04448119 (accessed on 15 June 2021).
- Principle. Platform Randomized Trial of Treatments in the Community for Epidemic and Pandemic Illnesses. Available online: https://www.principletrial.org/ (accessed on 15 June 2021).
- National Institute for Health Research. Favipiravir. Available online: https://www.nihr.ac.uk/news/favipiravir-to-be-investigated-as-a-possible-covid-19-treatment-for-at-home-recovery-in-the-principle-trial/27426 (accessed on 15 June 2021).
- Center for Drug Evaluation and Research. Approval Package for Application Number 050742. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/96/050742ap.pdf (accessed on 15 June 2021).
- Wagstaff, K.M.; Sivakumaran, H.; Heaton, S.M.; Harrich, D.; Jans, D.A. Ivermectin is a specific inhibitor of importin α/β-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus. Biochem. J. 2012, 443, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, L.; Pinkham, C.; Baer, A.; Amaya, M.; Narayanan, A.; Wagstaff, K.M.; Jans, D.A.; Kehn-Hall, K. Nuclear import and export inhibitors alter capsid protein distribution in mammalian cells and reduce Venezuelan Equine Encephalitis Virus replication. Antivir. Res. 2013, 100, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Y.; Fraser, J.E.; Chan, W.K.; Moreland, N.J.; Rathore, A.P.; Wang, C.; Vasudevan, S.G.; Jans, D.A. Nuclear localization of dengue virus (DENV) 1-4 non-structural protein 5; protection against all 4 DENV serotypes by the inhibitor Ivermectin. Antivir. Res. 2013, 99, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Götz, V.; Magar, L.; Dornfeld, D.; Giese, S.; Pohlmann, A.; Höper, D.; Kong, B.-W.; Jans, D.A.; Beer, M.; Haller, O.; et al. Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import. Sci. Rep. 2016, 6, 23138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caly, L.; Druce, J.D.; Catton, M.G.; Jans, D.A.; Wagstaff, K.M. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antivir. Res. 2020, 178, 104787. [Google Scholar] [CrossRef]
- Chaccour, C.; Casellas, A.; Blanco-Di Matteo, A.; Pineda, I.; Fernandez-Montero, A.; Ruiz-Castillo, P.; Richardson, M.-A.; Rodríguez-Mateos, M.; Jordan-Iborra, C.; Brew, J.; et al. The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine 2021, 32, 100720. [Google Scholar] [CrossRef] [PubMed]
- Ivermectin, Aspirin, Dexamethasone and Enoxaparin as Treatment of COVID-19 (IDEA). Available online: https://clinicaltrials.gov/ct2/show/NCT04425863 (accessed on 15 June 2021).
- Prophylactic Ivermectin in Covid-19 Contacts. Available online: https://clinicaltrials.gov/ct2/show/NCT04422561 (accessed on 15 June 2021).
- Center for Drug Evaluation and Research. Approval Package for Application Number 207924Orig1s000. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/207924Orig1s000Approv.pdf (accessed on 15 June 2021).
- Smolen, J.S.; Genovese, M.C.; Takeuchi, T.; Hyslop, D.L.; Macias, W.L.; Rooney, T.; Chen, L.; Dickson, C.L.; Riddle Camp, J.; Cardillo, T.E.; et al. Safety Profile of Baricitinib in Patients with Active Rheumatoid Arthritis with over 2 Years Median Time in Treatment. J. Rheumatol. 2019, 46, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Mayence, A.; Vanden Eynde, J.J. Baricitinib: A 2018 novel FDA-approved small molecule inhibiting JAK kinases. Pharmaceuticals 2019, 12, 37. [Google Scholar] [CrossRef] [Green Version]
- A Study of Baricitinib (LY3009104) in Participants with COVID-19 (COV-BARRIER). Available online: https://clinicaltrials.gov/ct2/show/NCT04421027 (accessed on 15 June 2021).
- Lilly and Incyte Announce Results from the Phase 3 COV-BARRIER Study of Baricitinib in Hospitalized COVID-19 Patients. Available online: https://investor.lilly.com/news-releases/news-release-details/lilly-and-incyte-announce-results-phase-3-cov-barrier-study (accessed on 15 June 2021).
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R. Baricitinib plus standard of care for hospitalized adults with COVID-19. MedRxiv 2021. [Google Scholar] [CrossRef]
- The COVID-19 Treatment Guidelines Panel’s Statement on Baricitinib for the Treatment of Adults with COVID-19. Available online: https://www.covid19treatmentguidelines.nih.gov/statement-on-baricitinib/ (accessed on 15 June 2021).
- Adaptive COVID-19 Treatment Trial 2 (ACTT-2). Available online: https://clinicaltrials.gov/ct2/show/NCT04401579 (accessed on 15 June 2021).
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.-M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus remdesivir for hospitalized adults with Covid-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- EMA Starts Evaluating Use of Olumiant in Hospitalised COVID-19 Patients Requiring Supplemental Oxygen. Available online: https://www.ema.europa.eu/en/news/ema-starts-evaluating-use-olumiant-hospitalised-covid-19-patients-requiring-supplemental-oxygen (accessed on 15 June 2021).
- Deftereos, S.; Giannopoulos, G.; Vrachatis, D.A.; Siasos, G.; Giotaki, S.G.; Cleman, M.; Dangas, G.; Stefanadis, C. Colchicine as a potent anti-inflammatory treatment in COVID-19: Can we teach an old dog new tricks? Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 255. [Google Scholar] [CrossRef]
- Lopes, M.I.; Bonjorno, L.P.; Giannini, M.C.; Amaral, N.B.; Menezes, P.I.; Dib, S.M.; Gigante, S.L.; Benatti, M.N.; Rezek, U.C.; Emrich-Filho, L.L.; et al. Beneficial effects of colchicine for moderate to severe COVID-19: A randomised, double-blinded, placebo-controlled clinical trial. RMD Open 2021, 7, e001455. [Google Scholar] [CrossRef]
- Colchicine Coronavirus SARS-CoV2 Trial (COLCORONA) (COVID-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04322682 (accessed on 15 June 2021).
- Tardif, J.-C.; Bouabdallaoui, N.; L’Allier, P.L.; Gaudet, D.; Shah, B.; Pillinger, M.H.; Lopez-Sendon, J.; da Luz, P.; Verret, L.; Audet, S.; et al. Efficacy of colchicine in non-hospitalized patients with COVID-19. MedRxiv 2021, 21250494. [Google Scholar] [CrossRef]
- PRINCIPLE COVID-19 Treatments Trial Widens to Under 50s and Adds Colchicine. Available online: https://www.principletrial.org/news/principle-covid-19-treatments-trial-widens-to-under-50s-adds-colchicine (accessed on 15 June 2021).
- RECOVERY Trial Closes Recruitment to Colchicine Treatment for Patients Hospitalised with COVID-19. Available online: https://www.recoverytrial.net/news/recovery-trial-closes-recruitment-to-colchicine-treatment-for-patients-hospitalised-with-covid-19 (accessed on 15 June 2021).
- Barnes, P.J. Inhaled corticosteroids. Pharmaceuticals 2010, 3, 514–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19. A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef] [PubMed]
- Randomised Evaluation of COVID-19 Therapy (RECOVERY). Available online: https://clinicaltrials.gov/ct2/show/NCT04381936 (accessed on 15 June 2021).
- RECOVERY. Randomised Evaluation of COVID-19 Therapy. Available online: https://www.recoverytrial.net/ (accessed on 15 June 2021).
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Katz, L.M. (A little) Clarity on convalescent plasma for Covid-19. N. Engl. J. Med. 2021, 384, 666–668. [Google Scholar] [CrossRef] [PubMed]
- Rojas, M.; Rodriguez, Y.; Monsalve, D.M.; Acosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Rojas-Villarraga, A.; Ramirez-Santana, C.; Diaz-Coronado, J.C.; Manrique, R.; et al. Convalescent plasma in COVID-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early high-titer plasma therapy to prevent severe Covid-19 in older adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef]
- Franchini, M.; Liumbruno, G.M. Convalescent plasma for the treatment of severe COVID-19. Biol. Targets Ther. 2021, 15, 31–38. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- The RECOVERY Collaborative Group. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): A randomised controlled, open-label, platform trial. Lancet 2021, 397, 2024–2025. [Google Scholar] [CrossRef]
- Scourfield, D.O.; Reed, S.G.; Quastel, M.; Alderson, J.; Bart, V.M.T.; Crespo, A.T.; Jones, R.; Pring, E.; Richter, F.C. The Oxford-Cardiff COVID-19Literature Consortium and Burnell, S.E.A. The role and uses of antibodies in COVID-19infections: A living review. Oxf. Open Immunol. 2021, 2, iqab003. [Google Scholar] [CrossRef]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef]
- Deb, P.; Molla, M.A.; Saif-Ur-Rahman, K.M. An update to monoclonal antibody as therapeutic option against COVID-19. Biosaf. Health 2021, 3, 87–91. [Google Scholar] [CrossRef] [PubMed]
- A Study of LY3819253 (LY-CoV555) and LY3832479 (LY-CoV016) in Participants with Mild to Moderate COVID-19 Illness (BLAZE-1). Available online: https://www.clinicaltrials.gov/ct2/show/NCT04427501 (accessed on 15 June 2021).
- Gottlieb, R.L.; Nirula, A.; Chen, P.; Boscia, J.; Heller, B.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. Effect of bamlanivimab as monotherapy or in combination with etesevimab on viral load in patients with mild to moderate COVID-19. A randomized clinical trial. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Health Care Providers. Emergency Use Authorization (EUA) for Bamlanivimab and Etesevimab. Available online: https://www.fda.gov/media/145802/download (accessed on 29 May 2021).
- U.S. Stops Distribution of Lilly’s COVID-19 Therapy due to Impact of Variants. Available online: https://www.reuters.com/article/health-coronavirus-lilly-idUSL4N2LN3TS (accessed on 15 June 2021).
- Kim, C.; Ryu, D.-K.; Lee, J.; Kim, Y.-I.; Seo, J.-M.; Kim, Y.-G.; Jeong, J.-H.; Kim, M.; Kim, J.-I.; Kim, P.; et al. A therapeutic neutralizing antibody targeting receptor binding domain of SARS-CoV-2 spike protein. Nat. Commun. 2021, 12, 288. [Google Scholar] [CrossRef] [PubMed]
- Ryu, D.-K.; Song, R.; Kim, M.; Kim, Y.-I.; Kim, C.; Kim, J.-I.; Kwon, K.-S.; Tijsma, A.S.L.; Nuijten, P.M.; van Baalen, C.A.; et al. Therapeutic effect of CT-P59 against SARS-CoV-2 South African variant. BioRxiv 2021. [Google Scholar] [CrossRef]
- Celltrion Confirms Neutralising Potency Against Emerging SARS-CoV-2 Variants with Anti-COVID-19 Monoclonal Antibody Treatment Regdanvimab (CT-P59). Available online: https://www.celltrionhealthcare.com/en-us/board/newsdetail?modify_key=482&pagenumber=1&keyword=&keyword_type= (accessed on 15 June 2021).
- EMA Issues Advice on Use of Regdanvimab for Treating COVID-19. Available online: https://www.ema.europa.eu/en/news/ema-issues-advice-use-regdanvimab-treating-covid-19 (accessed on 15 June 2021).
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a neutralizing antibody cocktail, in outpatients with Covid-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef]
- Fact Sheet for Health Care Providers. Emergency Use Authorization (EUA) for REGEN-COV™ (Casirivimab with Imdevimab). Available online: https://www.fda.gov/media/145611/download (accessed on 15 June 2021).
- Cathcart, A.L.; Havenar-Daughton, C.; Lempp, F.A.; Ma, D.; Schmid, M.; Agostini, M.L.; Guarino, B.; Di iulio, J.; Rosen, L.; Tucker, H.; et al. The dual function monoclonal antibodies VIR-7831 and VIR-7832 demonstrate potent in vitro and in vivo activity against SARS-CoV-2. BioRxiv Immunol. 2021. [Google Scholar] [CrossRef]
- Fact Sheet for Health Care Providers. Emergency Use Authorization (EUA) for Sotrovimab. Available online: https://www.fda.gov/media/149534/download (accessed on 15 June 2021).
- VIR-7831 for the Early Treatment of COVID-19 in Outpatients (COMET-ICE). Available online: https://clinicaltrials.gov/ct2/show/NCT04545060 (accessed on 15 June 2021).
- A Study of Immune System Proteins in Participants with Mild to Moderate COVID-19 Illness (BLAZE-4). Available online: https://clinicaltrials.gov/ct2/show/NCT04634409 (accessed on 15 June 2021).
- Della-Torre, E.; Campochiaro, C.; Cavalli, G.; De Luca, G.; Napolitano, A.; La Marca, S.; Boffini, N.; Da Prat, V.; Di Terlizzi, G.; Lanzillotta, M.; et al. Interleukin-6 blockade with sarilumab in severe COVID-19 pneumonia with systemic hyperinflammation: An open-label cohort study. Ann. Rheum. Dis. 2020, 79, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Sivapalasingam, S.; Lederer, D.J.; Bhore, R.; Hajizadeh, N.; Criner, G.; Hossain, R.; Mahmood, A.; Giannelou, A.; Somersan-Karakaya, S.; O’Brien, M.; et al. A randomized placebo-controlled trial of sarilumab in hospitalized patients with Covid-19. MedRxiv 2021. [Google Scholar] [CrossRef]
- Lescure, F.-X.; Honda, H.; Fowler, R.A.; Lazar, J.S.; Shi, G.; Wung, P.; Patel, N.; Hagino, O. Sarilumab in patients admitted to hospital with severe or critical COVID-19: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 522–532. [Google Scholar] [CrossRef]
- FDA Approves Phase III Clinical Trial of Tocilizumab for COVID-19 Pneumonia. Available online: https://www.cancernetwork.com/view/fda-approves-phase-iii-clinical-trial-tocilizumab-covid-19-pneumonia (accessed on 15 June 2021).
- A Study to Evaluate the Safety and Efficacy of Tocilizumab in Patients with Severe COVID-19 Pneumonia (COVACTA). Available online: https://clinicaltrials.gov/ct2/show/NCT04320615 (accessed on 15 June 2021).
- Genentech Provides an Update on the Phase III COVACTA Trial of Actemra in Hospitalized Patients with Severe COVID-19 Associated Pneumonia. Available online: https://www.gene.com/media/press-releases/14867/2020-07-28/genentech-provides-an-update-on-the-phas (accessed on 15 June 2021).
- A Study to Evaluate the Efficacy and Safety of Remdesivir Plus Tocilizumab Compared with Remdesivir Plus Placebo in Hospitalized Participants with Severe COVID-19 Pneumonia (REMDACTA). Available online: https://clinicaltrials.gov/ct2/show/NCT04409262 (accessed on 15 June 2021).
- Roche Provides Update on the Phase III REMDACTA Trial of Actemra/RoActemra Plus Veklury in Patients with Severe COVID-19 Pneumonia. Available online: https://www.roche.com/media/releases/med-cor-2021-03-11.htm (accessed on 15 June 2021).
- The RECOVERY Collaborative Group. Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): Preliminary Results of a Randomised, Controlled, Open-Label, Platform Trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Update: FDA Authorizes Drug for Treatment of COVID-19. 24 June 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-drug-treatment-covid-19 (accessed on 3 July 2021).
- Gritti, G.; Raimondi, F.; Bottazzi, B.; Ripamonti, D.; Riva, I.; Landi, F.; Alborghetti, L.; Frigeni, M.; Damiani, M.; Micò, C.; et al. Siltuximab downregulates interleukin-8 and pentraxin 3 to improve ventilatory status and survival in severe COVID-19. Leukemia 2021. [Google Scholar] [CrossRef]
- An Observational Study of the Use of Siltuximab (SYLVANT) in Patients Diagnosed with COVID-19 Infection Who Have Developed Serious Respiratory Complications (SISCO). Available online: https://www.clinicaltrials.gov/ct2/show/NCT04322188 (accessed on 15 June 2021).
- Anti-IL6 and Corticosteroid Monotherapy vs Combination in COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04486521 (accessed on 15 June 2021).
- Mehta, P.; Cron, R.Q.; Hartwell, J.; Manson, J.J.; Tattersall, R.S. Silencing the cytokine storm: The use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatol. 2020, 2, e358–e367. [Google Scholar] [CrossRef]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Din, C.T.; Boffini, N.; et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e325–e331. [Google Scholar] [CrossRef]
- Franzetti, M.; Forastieri, A.; Borsa, N.; Pandolfo, A.; Molteni, C.; Borghesi, L.; Pontiggia, S.; Evasi, G.; Guiotto, L.; Erba, M.; et al. IL-1 Receptor antagonist anakinra in the treatment of COVID-19 acute respiratory distress syndrome: A retrospective, observational study. J. Immunol. 2021, 206, 1569–1575. [Google Scholar] [CrossRef]
- Kooistra, E.J.; Waalders, N.J.B.; Grondman, I.; Janssen, N.A.F.; de Nooijer, A.H.; Netea, M.G.; van de Veerdonk, F.L.; Ewalds, E.; van der Hoeven, J.G.; Kox, M.; et al. Anakinra treatment in critically ill COVID-19 patients: A prospective cohort study. Crit. Care 2020, 24, 688. [Google Scholar] [CrossRef]
- Pasin, L.; Cavalli, G.; Navalesi, P.; Sella, N.; Landoni, G.; Yavorovskiy, A.G.; Likhvantsev, V.V.; Zangrillo, A.; Dagna, L.; Monti, G. Anakinra for patients with COVID-19: A meta-analysis of non-randomized cohort studies. Eur. J. Intern. Med. 2021, 86, 34–40. [Google Scholar] [CrossRef] [PubMed]
- The CORIMUNO-19 Collaborative Group. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomised controlled trial. Lancet Respir. Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- Harrell, C.R.; Sadikot, R.; Pascual, J.; Fellabaum, C.; Jankovic, M.G.; Jovicic, N.; Djonov, V.; Arsenijevic, N.; Volarevic, V. Mesenchymal stem cell-based therapy of inflammatory lung diseases: Current understanding and future perspectives. Stem Cells Int. 2019, 4236973. [Google Scholar] [CrossRef] [PubMed]
- Basiri, A.; Mansouri, F.; Azari, A.; Ranjbarvan, P.; Zarein, F.; Heidari, A.; Golchin, A. Stem cell therapy potency in personalizing severe COVID-19 treatment. Stem Cell Rev. Rep. 2021, 17, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Mahandiratta, S.; Bansal, S.; Sarma, P.; Kumar, H.; Choudhary, G.; Kumar, S.; Prakash, A.; Sehgal, R.; Medhi, G. Stem cell therapy in COVID-19: Pooled evidencefor SARS-CoV-2, SARS-CoV, MERS-CoV and ARDS: A systematic review. Biomed. Pharmacother. 2021, 137, 111300. [Google Scholar] [CrossRef] [PubMed]
- FDA Cautions against Use of Hydroxychloroquine or Chloroquine for COVID-19 Outside of the Hospital Setting or a Clinical Trial due to Risk of Heart Rhythm Problems. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-cautions-against-use-hydroxychloroquine-or-chloroquine-covid-19-outside-hospital-setting-or#:~:text=Hydroxychloroquine%20and%20chloroquine%20are%20FDA,in%20adults%2C%20and%20rheumatoid%20arthritis (accessed on 4 July 2021).
- COVID-19: Chloroquine and Hydroxychloroquine Only to be Used in Clinical Trials or Emergency Use Programmes. Available online: https://www.ema.europa.eu/en/documents/press-release/covid-19-chloroquine-hydroxychloroquine-only-be-used-clinical-trials-emergency-use-programmes_en.pdf (accessed on 15 June 2021).
- FAQ: COVID-19 and Ivermectin Intended for Animals. Available online: https://www.fda.gov/animal-veterinary/product-safety-information/faq-covid-19-and-ivermectin-intended-animals (accessed on 4 July 2020).
- EMA Advises against Use of Ivermectin for the Prevention or Treatment of COVID-19 Outside Randomised Clinical Trials. Available online: https://www.ema.europa.eu/en/news/ema-advises-against-use-ivermectin-prevention-treatment-covid-19-outside-randomised-clinical-trials (accessed on 15 June 2021).
- What’s New in the Guidelines. Last Updated: 11 June 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/about-the-guidelines/whats-new/ (accessed on 15 June 2021).
- Coronavirus (COVID-19) Update: FDA Authorizes Drug Combination for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-drug-combination-treatment-covid-19 (accessed on 4 July 2021).
- Corticosteroid for COVID-19. Living Guidance 2 September 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Corticosteroids-2020.1 (accessed on 15 June 2021).
- Temporary Policy for Compounding of Certain Drugs for Hospitalized Patients by Pharmacy Compounders not Registered as Outsourcing Facilities during the COVID-19 Public Health Emergency. Available online: https://www.fda.gov/media/138279/download (accessed on 4 July 2021).
- EMA Endorses Use of Dexamethasone in COVID-19 Patients on Oxygen or Mechanical Ventilation. Available online: https://www.ema.europa.eu/en/news/ema-endorses-use-dexamethasone-covid-19-patients-oxygen-mechanical-ventilation (accessed on 15 June 2021).
- Anti-SARS-CoV-2 Monoclonal Antibodies. Last Updated: 24 May 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/anti-sars-cov-2-antibody-products/anti-sars-cov-2-monoclonal-antibodies/ (accessed on 15 June 2021).
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf (accessed on 15 June 2021).
- Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab (accessed on 4 July 2021).
- EMA Issues Advice on Use of Antibody Combination (Bamlanivimab/Etesevimab). Available online: https://www.ema.europa.eu/en/news/ema-issues-advice-use-antibody-combination-bamlanivimab-etesevimab (accessed on 15 June 2021).
- Coronavirus Company News Summary. Available online: https://www.pharmaceutical-technology.com/uncategorised/coronavirus-company-news-summary-gsk-and-vir-submit-eua-application-to-fda-for-covid-19-monoclonal-antibody-treatment-ema-recommends-celltrions-regdanvimab-for-severe-covid-19/ (accessed on 4 July 2021).
- Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal Antibodies for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-monoclonal-antibodies-treatment-covid-19 (accessed on 4 July 2021).
- EMA Issues Advice on Use of REGN-COV2 Antibody Combination (Casirivimab/Imdevimab). Available online: https://www.ema.europa.eu/en/news/ema-issues-advice-use-regn-cov2-antibody-combination-casirivimab-imdevimab (accessed on 15 June 2021).
- Coronavirus (COVID-19) Update: FDA Authorizes Additional Monoclonal Antibody for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-monoclonal-antibody-treatment-covid-19 (accessed on 4 July 2021).
- EMA Issues Advice on Use of Sotrovimab (VIR-7831) for Treating COVID-19. Available online: https://www.ema.europa.eu/en/news/ema-issues-advice-use-sotrovimab-vir-7831-treating-covid-19 (accessed on 15 June 2021).
- Raoult, D. Carnets de Guerre COVID-19; Michel-Lafon: Neuilly-sur-Seine, France, 2021. [Google Scholar]
- Ip, A.; Ahn, J.; Zhou, Y.; Goy, A.H.; Hansen, E.; Pecora, A.L.; Sinclaire, B.A.; Bednarz, U.; Marafelias, M.; Sawczuk, I.S. Hydroxychloroquine in the treatment of outpatients with mildly symptomatic COVID-19: A multi-center observational study. BMC Infect. Dis. 2021, 21, 72. [Google Scholar] [CrossRef]






| Search Term | As of | ||||
|---|---|---|---|---|---|
| 28 March 2020 | 28 April 2020 | 28 September 2020 | 28 March 2021 | 28 May 2021 | |
| COVID-19 | 202 | 997 | 3479 | 5170 | 5619 |
| Hydroxychloroquine | 19 | 148 | 252 | 275 | 276 |
| Azithromycin | 16 | 62 | 118 | 126 | 127 |
| Lopinavir (+ritonavir) | 14 | 44 | 80 | 91 | 93 |
| Interferon | 21 | 42 | 99 | 140 | 153 |
| Remdesivir | 9 | 18 | 57 | 93 | 103 |
| Vaccine | 22 | 71 | 240 | 538 | 673 |
| Camostat | - | 2 | 9 | 22 | 24 |
| Nafamostat | - | 1 | 6 | 7 | 7 |
| Umifenovir | 9 | 11 | 14 | 14 | 14 |
| Favipiravir | 2 | 12 | 37 | 50 | 51 |
| Ivermectin | 2 | 5 | 44 | 65 | 68 |
| Baricitinib | 2 | 9 | 14 | 18 | 20 |
| Colchicine | 2 | 8 | 22 | 31 | 33 |
| Corticosteroid | 12 | 35 | 73 | 100 | 111 |
| Dexamethasone | 4 | 10 | 30 | 62 | 72 |
| Hydrocortisone | 4 | 6 | 15 | 18 | 20 |
| Methylprednisolone | 5 | 14 | 40 | 51 | 54 |
| Prednisone | 2 | 4 | 10 | 13 | 16 |
| Plasma | 42 | 123 | 398 | 559 | 593 |
| Bamlanivimab | - | - | 4 | 12 | 13 |
| Etesevimab | - | - | 2 | 4 | 5 |
| Regdanvimab/CT-P59 | - | - | 3 | 3 | 3 |
| Regn-Cov2 | 1 | 1 | 4 | 5 | 6 |
| Casirivimab | - | - | 3 | 7 | 9 |
| Imdevimab | - | - | 3 | 7 | 9 |
| Sotrovimab/VIR-7831 | - | - | 3 | 5 | 5 |
| Sarilumab | 4 | 12 | 16 | 17 | 17 |
| Tocilizumab | 6 | 32 | 69 | 82 | 84 |
| Siltuximab | 1 | 3 | 4 | 4 | 4 |
| Anakinra | 4 | 12 | 24 | 34 | 35 |
| Mesenchymal (cells) | 11 | 30 | 62 | 77 | 81 |
| Treatment | WHO | FDA | EMA |
|---|---|---|---|
| Hydroxychloroquine | a strong recommendation against use in patients with COVID-19 of any severity [50] (31 March 2020) | FDA cautions against use outside of the hospital setting or a clinical trial [160] (1 July 2020) | only to be used in clinical trials or emergency use programs [161] (1 April 2020) |
| Lopinavir ritonavir | a strong recommendation against use in patients with COVID-19 of any severity [50] (31 March 2020) | No data found | No data found |
| Remdesivir | a conditional recommendation against use in hospitalized patients [50] (31 March 2020) | approved for adults and pediatric patients requiring hospitalization [43] (22 October 2020) | conditional marketing authorization [45] (3 July 2020) |
| Ivermectin | not recommended in patients with COVID-19 except in the context of a clinical trial [50] (31 March 2020) | not approved for the prevention or treatment of COVID-19 [162] (26 April 2021) | against use for the prevention or treatment outside randomized clinical trials [163] (22 March 2021) |
| Baricitinib | in combination; for hospitalized patients on high-flow oxygen or noninvasive ventilation who have evidence of clinical progression or increased markers of inflammation [164] (27 May 2021) | emergency use authorization in combination with remdesivir [165] (19 November 2020) | EMA starts evaluating the use of Olumiant in hospitalized patients requiring supplemental oxygen [103] (29 April 2021) |
| Dexamethasone | use of systemic corticosteroids rather than no corticosteroids recommended for patients with severe or critical COVID-19 infection, use not recommended for patients with non-severe infection [166] (2 September 2020) | in the list of drugs used for hospitalized patients [167] (13 October 2020) | can be used in patients on oxygen or mechanical ventilation [168] (18 September 2020) |
| Bamlanivimab etesevimab | use recommended to treat outpatients with mild to moderate COVID-19 who are at high risk of clinical progression [169,170] (24 May 2021) | FDA revokes emergency use authorization [171] (19 April 2021) | can be used in patients not requiring oxygen and at high risk of progressing to severe disease [172] (5 March 2021) |
| Regdanvimab CT-P59 | No data found | application for emergency use authorization submitted [173] (29 March 2021) | can be used in patients not requiring oxygen and at high risk of progressing to severe disease [131] (26 March 2021) |
| Regn-Cov2 | Use recommended to treat outpatients with mild to moderate COVID-19 who are at high risk of clinical progression [169,170] (24 May 2021) | emergency use authorization [174] (21 November 2020) | can be used in patients not requiring oxygen and at high risk of progressing to severe disease [175] (26 February 2021) |
| Sotrovimab VIR-7831 | No data found | emergency use authorization [135,176] (26 May 2021) | can be used in patients not requiring oxygen and at high risk of progressing to severe disease [177] (21 May 2021) |
| Tocilizumab | in combination; for hospitalized patients on high-flow oxygen or noninvasive ventilation who have evidence of clinical progression or increased markers of inflammation [164] (27 May 2021) | emergency use authorization [147] (24 June 2021) | No data found |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanden Eynde, J.J. COVID-19: Failure of the DisCoVeRy Clinical Trial, and Now–New Hopes? Pharmaceuticals 2021, 14, 664. https://doi.org/10.3390/ph14070664
Vanden Eynde JJ. COVID-19: Failure of the DisCoVeRy Clinical Trial, and Now–New Hopes? Pharmaceuticals. 2021; 14(7):664. https://doi.org/10.3390/ph14070664
Chicago/Turabian StyleVanden Eynde, Jean Jacques. 2021. "COVID-19: Failure of the DisCoVeRy Clinical Trial, and Now–New Hopes?" Pharmaceuticals 14, no. 7: 664. https://doi.org/10.3390/ph14070664
APA StyleVanden Eynde, J. J. (2021). COVID-19: Failure of the DisCoVeRy Clinical Trial, and Now–New Hopes? Pharmaceuticals, 14(7), 664. https://doi.org/10.3390/ph14070664