
Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review


Abstract
:1. Introduction
1.1. Background
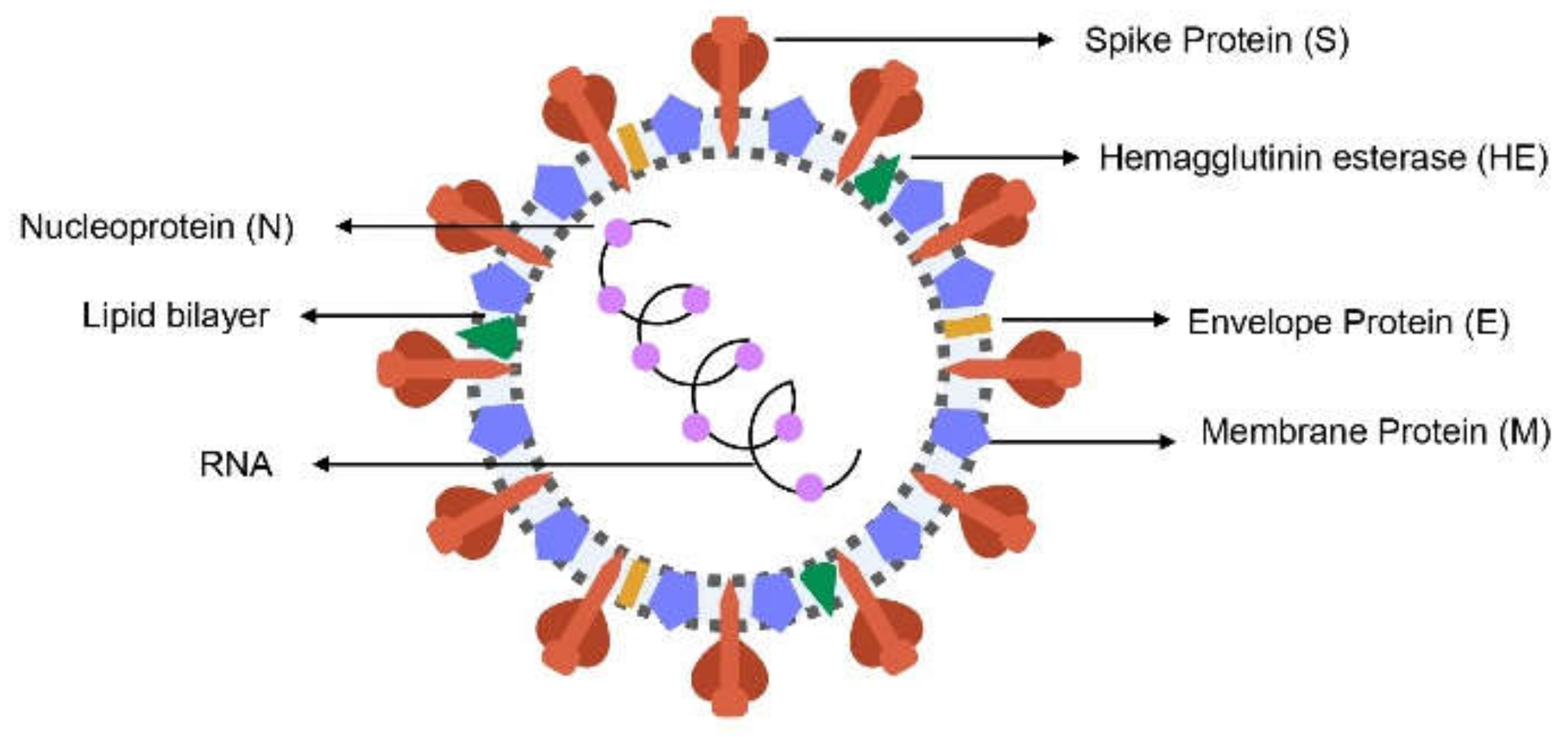
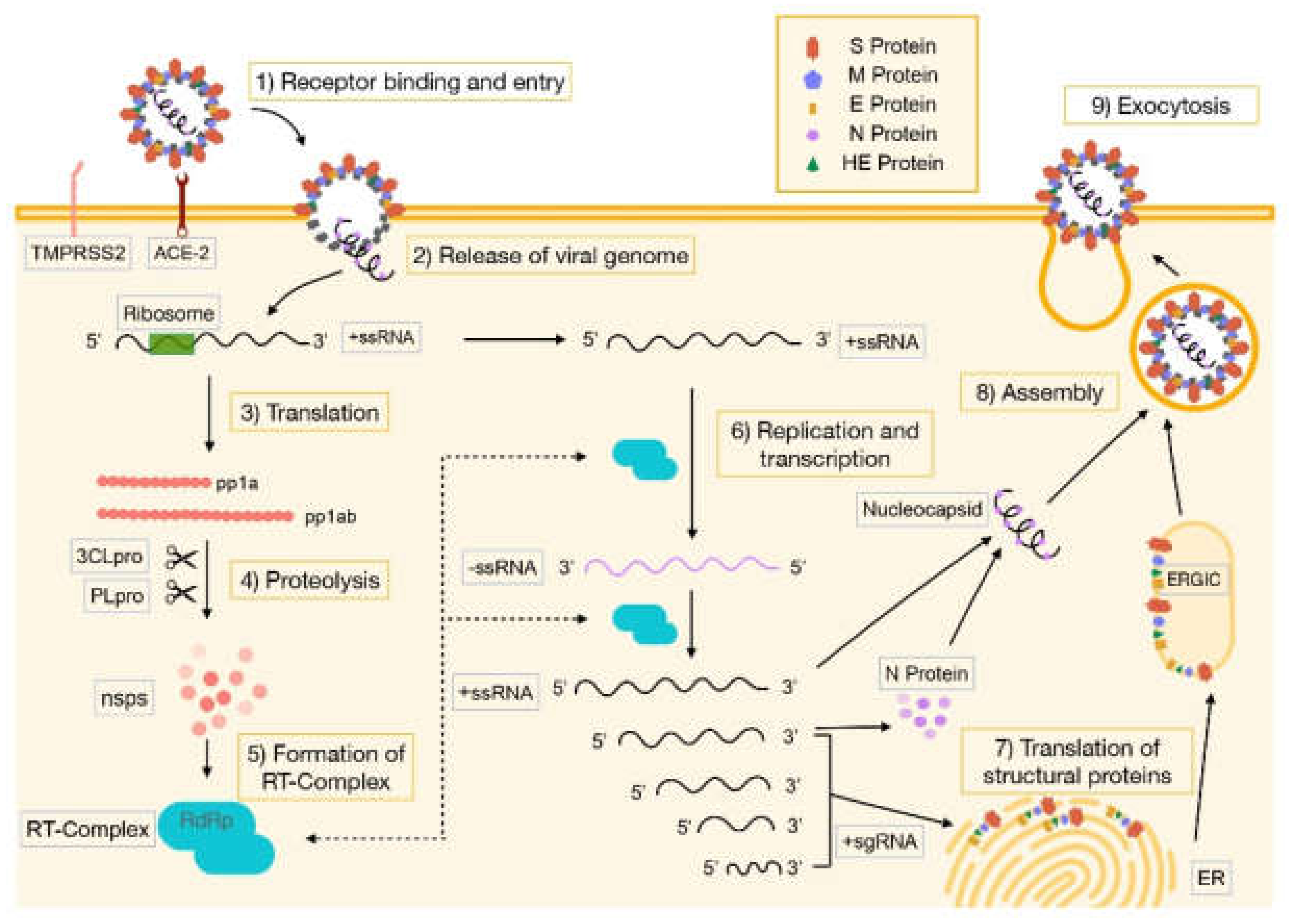
1.2. SARS-CoV-2 Molecular Structure and Pathogenesis
1.3. Immune Response and Clinical Features
1.4. Therapeutic Possibilities
Vaccination
1.5. Justification and Aim
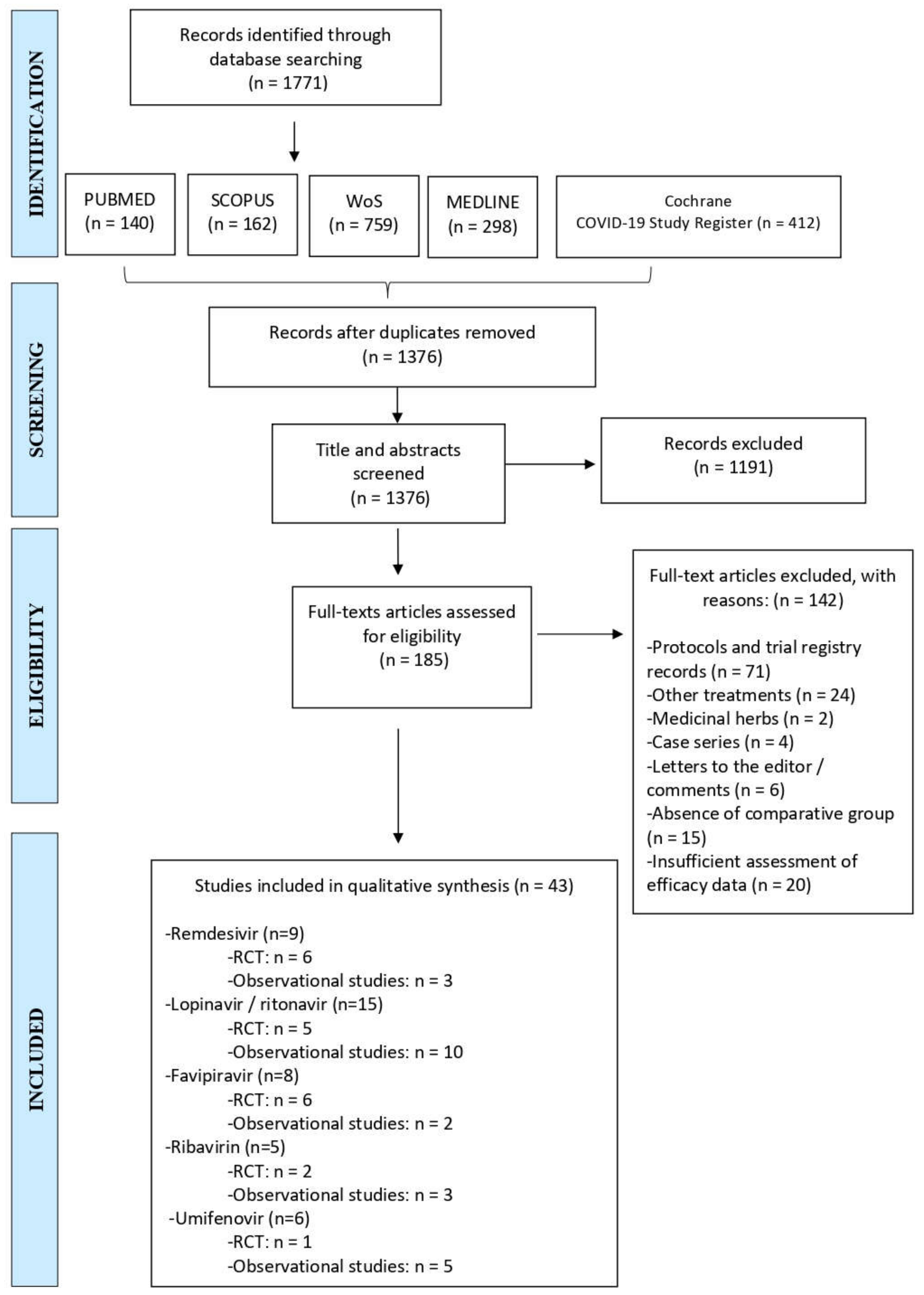
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection and Analysis
3. Results
3.1. Remdesivir
3.1.1. Efficacy
3.1.2. Safety
3.2. Lopinavir/Ritonavir
3.2.1. Efficacy
3.2.2. Safety
3.3. Favipiravir
3.3.1. Efficacy
3.3.2. Safety
3.4. Ribavirin
3.4.1. Efficacy
3.4.2. Safety
3.5. Umifenovir
3.5.1. Efficacy
3.5.2. Safety
4. Discussion
Limitations
5. Conclusions
- Remdesivir may help accelerate clinical improvement in hospitalized COVID-19 patients, but it is not effective in reducing mortality. Regarding the duration of the treatment, a 5-day course seems to be sufficient. In terms of safety, this drug has proven to be as tolerable as placebo or other drugs that it has been compared to.
- Lopinavir/ritonavir has not proven to be an effective treatment for patients with SARS-CoV-2 infection in improving clinical status, reducing mortality, or increasing viral clearance. In fact, it has been associated with a higher risk of gastrointestinal adverse events.
- Treatment with favipiravir is associated with significant clinical improvement, mainly in reducing time to fever resolution, and is also safe and well-tolerated. Likewise, the combination of favipiravir with tocilizumab seems to have promising results in terms of reducing lung parenchyma inflammation and symptom resolution. However, the use of favipiravir has failed to increase viral clearance.
- Ribavirin has not proven to be an effective treatment for COVID-19 patients, and its concomitant use with lopinavir/ritonavir is not recommended, due to an increase in the risk of adverse events.
- Arbidol has proven to be a safe and well-tolerated treatment for COVID-19 patients. However, it is not associated with a significant reduction in the length of hospital stay. Due to the small number of studies included in this systematic review regarding arbidol, we do not have sufficient evidence to support the use of this drug in patients with COVID-19.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, D.X.; Liang, J.Q.; Fung, T.S. Human Coronavirus-229E, -OC43, -NL63, and -HKU1. In Encyclopedia of Virology, 4th ed.; Dennis, H., Bamford, M.Z., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 428–440. [Google Scholar] [CrossRef]
- Payne, S. Family Coronaviridae. Viruses 2017, 149–158. [Google Scholar] [CrossRef]
- Rabaan, A.A.; Al-Ahmed, S.H.; Haque, S.; Sah, R.; Tiwari, R.; Malik, Y.S.; Dhama, K.; Yatoo, M.I.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J.; et al. SARS-CoV-2, SARS-CoV, and MERS-CoV: A comparative overview. Infez Med. 2020, 28, 174–184. Available online: https://pubmed.ncbi.nlm.nih.gov/32275259/ (accessed on 27 November 2020). [PubMed]
- van Boheemen, S.; de Graaf, M.; Lauber, C.; Bestebroer, T.M.; Raj, V.S.; Zaki, A.M.; Osterhaus, A.D.M.E.; Haagmans, B.L.; Gorbalenya, A.E.; Snijder, E.J.; et al. Genomic Characterization of a Newly Discovered Coronavirus Associated with Acute Respiratory Distress Syndrome in Humans. mBio 2012, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haagmans, B.L.; Al Dhahiry, S.H.S.; Reusken, C.B.E.M.; Raj, V.S.; Galiano, M.; Myers, R.; Godeke, G.-J.; Jonges, M.; Farag, E.; Diab, A.; et al. Middle East respiratory syndrome coronavirus in dromedary camels: An outbreak investigation. Lancet Infect. Dis. 2014, 14, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Report of Pneumonia of Unknown Cause—China. Available online: http://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 28 November 2020).
- World Health Organization (WHO). COVID-19: Cronología de la Actuación de la OMS. Available online: https://www.who.int/es/news/item/27-04-2020-who-timeline---covid-19 (accessed on 28 November 2020).
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A Review of Viral, Host, and Environmental Factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Pastrian-Soto, G. Bases Genéticas y Moleculares del COVID-19 (SARS-CoV-2). Mecanismos de Patogénesis y de Respuesta Inmune. Int. J. Odontostomatol. 2020, 14, 331–337. [Google Scholar] [CrossRef]
- Boopathi, S.; Poma, A.B.; Kolandaivel, P. Novel 2019 coronavirus structure, mechanism of action, antiviral drug promises and rule out against its treatment. J. Biomol. Struct. Dyn. 2021, 39, 3409–3418. [Google Scholar] [CrossRef] [Green Version]
- Tortorici, M.A.; Veesler, D. Structural Insights into Coronavirus Entry; Academic Press Inc.: Amsterdam, The Netherlands, 2019; Volume 105, pp. 93–116. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Ewan, P.P. The role of programmed-1 ribosomal frameshifting in coronavirus propagation. Front. Biosci. 2008, 13, 4873–4881. [Google Scholar] [CrossRef] [Green Version]
- Báez-Santos, Y.M.; John, S.E.S.; Mesecar, A.D. The SARS-coronavirus papain-like protease: Structure, function and inhibition by designed antiviral compounds. Antivir. Res. 2015, 115, 21–38. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, S.G.; Sawicki, D.L.; Siddell, S. A Contemporary View of Coronavirus Transcription. J. Virol. 2007, 81, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- V’Kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Genet. 2021, 19, 155–170. [Google Scholar] [CrossRef]
- De Haan, C.A.; Rottier, P.J. Molecular Interactions in the Assembly of Coronaviruses. Adv Virus Res. 2005, 64, 165–230. [Google Scholar] [CrossRef]
- Cantini, F.; Goletti, D.; Petrone, L.; Fard, S.N.; Niccoli, L.; Foti, R. Immune Therapy, or Antiviral Therapy, or Both for COVID-19: A Systematic Review. Drugs 2020, 80, 1929–1946. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Hanna, R.; Dalvi, S.; Sălăgean, T.; Pop, I.D.; Bordea, I.R.; Benedicenti, S. Understanding COVID-19 Pandemic: Molecular Mechanisms and Potential Therapeutic Strategies. An Evidence-Based Review. J. Inflamm. Res. 2021, 14, 13–56. [Google Scholar] [CrossRef] [PubMed]
- Abou-Ismail, M.Y.; Diamond, A.; Kapoor, S.; Arafah, Y.; Nayak, L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb. Res. 2020, 194, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Perazzolo, S.; Zhu, L.; Lin, W.; Nguyen, A.; Ho, R.J. Systems and Clinical Pharmacology of COVID-19 Therapeutic Candidates: A Clinical and Translational Medicine Perspective. J. Pharm. Sci. 2021, 110, 1002–1017. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Liu, X.; Liu, C.; Liu, G.; Luo, W.; Xia, N. COVID-19: Progress in diagnostics, therapy and vaccination. Theranostics 2020, 10, 7821–7835. [Google Scholar] [CrossRef] [PubMed]
- Borbone, N.; Piccialli, G.; Roviello, G.N.; Oliviero, G. Nucleoside Analogs and Nucleoside Precursors as Drugs in the Fight against SARS-CoV-2 and Other Coronaviruses. Molecules 2021, 26, 986. [Google Scholar] [CrossRef]
- Delang, L.; Abdelnabi, R.; Neyts, J. Favipiravir as a potential countermeasure against neglected and emerging RNA viruses. Antivir. Res. 2018, 153, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19). JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef]
- Esposito, S.; Noviello, S.; Pagliano, P. Update on treatment of COVID-19: Ongoing studies between promising and disappointing results. Infez Med. 2020, 28, 198–211. Available online: https://pubmed.ncbi.nlm.nih.gov/32335561/ (accessed on 17 January 2021).
- Vijayvargiya, P.; Garrigos, Z.E.; Almeida, N.E.C.; Gurram, P.R.; Stevens, R.W.; Razonable, R.R. Treatment Considerations for COVID-19: A Critical Review of the Evidence (or Lack Thereof). Mayo Clin. Proc. 2020, 95, 1454–1466. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 14 July 2021).
- Abdulla, Z.; Al-Bashir, S.; Al-Salih, N.; Aldamen, A.; Abdulazeez, M. A Summary of the SARS-CoV-2 Vaccines and Technologies Available or under Development. Pathogens 2021, 10, 788. [Google Scholar] [CrossRef]
- Forchette, L.; Sebastian, W.; Liu, T. A Comprehensive Review of COVID-19 Virology, Vaccines, Variants, and Therapeutics. Curr. Med. Sci. 2021, 1–15. [Google Scholar] [CrossRef]
- Huang, Q.; Zeng, J.; Yan, J. COVID-19 mRNA vaccines. J. Genet. Genom. 2021, 48, 107–114. [Google Scholar] [CrossRef]
- Livingston, E.H.; Malani, P.N.; Creech, C.B. The Johnson & Johnson Vaccine for COVID-19. JAMA 2021, 325, 1575. [Google Scholar] [CrossRef]
- Park, J.; Lee, H. Delivery Routes for COVID-19 Vaccines. Vaccines 2021, 9, 524. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Indari, O.; Jakhmola, S.; Manivannan, E.; Jha, H.C. An Update on Antiviral Therapy Against SARS-CoV-2: How Far Have We Come? Front. Pharmacol. 2021, 12, 632677. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration (FDA). FDA’s Approval of Veklury (Remdesivir) for the Treatment of COVID-19—The Science of Safety and Effectiveness. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fdas-approval-veklury-remdesivir-treatment-covid-19-science-safety-and-effectiveness (accessed on 16 July 2021).
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; Arribas López, J.R.; Cattelan, A.M.; Soriano Viladomiu, A.; Ogbuagu, O.; Malhotra, P.; Mullane, K.M.; Castagna, A.; et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients with Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1048–1057. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.; Galli, M.; Ahn, M.-Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. New Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Pan, H.; Peto, R.; Henao-Restrepo, A.-M.; Karim, Q.A.; Alejandria, M.; García, C.H.; Kieny, M.-P.; Malekzadeh, R.; Murthy, S.; Preziosi, M.-P.; et al. Repurposed Antiviral Drugs for Covid-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Pasquini, Z.; Montalti, R.; Temperoni, C.; Canovari, B.; Mancini, M.; Tempesta, M.; Pimpini, D.; Zallocco, N.; Barchiesi, F. Effectiveness of remdesivir in patients with COVID-19 under mechanical ventilation in an Italian ICU. J. Antimicrob. Chemother. 2020, 75, 3359–3365. [Google Scholar] [CrossRef] [PubMed]
- Olender, S.A.; Perez, K.K.; Go, A.S.; Balani, B.; Price-Haywood, E.G.; Shah, N.S.; Wang, S.; Walunas, T.L.; Swaminathan, S.; Slim, J.; et al. Remdesivir for Severe COVID-19 versus a Cohort Receiving Standard of Care. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Kalligeros, M.; Tashima, K.T.; Mylona, E.K.; Rybak, N.; Flanigan, T.P.; Farmakiotis, D.; Beckwith, C.G.; Sanchez, M.; Neill, M.; Johnson, J.E.; et al. Remdesivir Use Compared with Supportive Care in Hospitalized Patients With Severe COVID-19: A Single-Center Experience. Open Forum Infect. Dis. 2020, 7, ofaa319. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Ader, F.; Peiffer-Smadja, N.; Poissy, J.; Bouscambert-Duchamp, M.; Belhadi, D.; Diallo, A.; Delmas, C.; Saillard, J.; Dechanet, A.; Mercier, N.; et al. Antiviral drugs in hospitalized patients with COVID-19—The DisCoVeRy trial. MedRxiv 2021. [Google Scholar] [CrossRef]
- Gao, G.; Wang, A.; Wang, S.; Qian, F.; Chen, M.; Yu, F.; Zhang, J.; Wang, X.; Ma, X.; Zhao, T.; et al. Brief Report: Retrospective Evaluation on the Efficacy of Lopinavir/Ritonavir and Chloroquine to Treat Nonsevere COVID-19 Patients. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 85, 239–243. [Google Scholar] [CrossRef]
- Grimaldi, D.; for the COVADIS Study Group; Aissaoui, N.; Blonz, G.; Carbutti, G.; Courcelle, R.; Gaudry, S.; Gaultier, A.; D’Hondt, A.; Higny, J.; et al. Characteristics and outcomes of acute respiratory distress syndrome related to COVID-19 in Belgian and French intensive care units according to antiviral strategies: The COVADIS multicentre observational study. Ann. Intensiv. Care 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Choi, M.J.; Kang, M.; Shin, S.Y.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Jung, J.; Song, J.Y. Comparison of antiviral effect for mild-to-moderate COVID-19 cases between lopinavir/ritonavir versus hydroxychloroquine: A nationwide propensity score-matched cohort study. Int. J. Infect. Dis. 2021, 102, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.-T.; Luo, Y.-L.; Xia, S.-C.; Sun, Q.-F.; Ding, J.-G.; Zhou, Y.; Chen, W.; Wang, X.-F.; Zhang, W.-W.; Du, W.-J.; et al. Clinical efficacy of lopinavir/ritonavir in the treatment of Coronavirus disease 2019. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3390–3396. [Google Scholar] [CrossRef]
- Lecronier, M.; Beurton, A.; Burrel, S.; Haudebourg, L.; Deleris, R.; Le Marec, J.; Virolle, S.; Nemlaghi, S.; Bureau, C.; Mora, P.; et al. Comparison of hydroxychloroquine, lopinavir/ritonavir, and standard of care in critically ill patients with SARS-CoV-2 pneumonia: An opportunistic retrospective analysis. Crit. Care 2020, 24, 1–9. [Google Scholar] [CrossRef]
- Lu, J.M.; Zhou, A.F.; Zhang, X.B.; Xu, H.; Wang, X.-F.; Ye, Q.-F.; Shang, F.-N.; He, Y.-L.; Ma, S.-L.; Cui, Y.-X.; et al. Safety and efficacy of oral lopinavir/ritonavir in pediatric patients with coronavirus disease: A nationwide comparative analysis. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 549–555. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pagani, G.; Ridolfo, A.L.; Oreni, L.; Conti, F.; Pezzati, L.; Bradanini, L.; Casalini, G.; Bassoli, C.; Morena, V.; et al. Early administration of lopinavir/ritonavir plus hydroxychloroquine does not alter the clinical course of SARS-CoV-2 infection: A retrospective cohort study. J. Med. Virol. 2021, 93, 1421–1427. [Google Scholar] [CrossRef]
- Zhu, Z.; Lu, Z.; Xu, T.; Chen, C.; Yang, G.; Zha, T.; Lu, J.; Xue, Y. Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19. J. Infect. 2020, 81, e21–e23. [Google Scholar] [CrossRef] [PubMed]
- Vernaz, N.; Agoritsas, T.; Calmy, A.; Gayet-Ageron, A.; Gold, G.; Perrier, A.; Picard, F.; Prendki, V.; Reny, J.-L.; Samer, C.; et al. Early experimental COVID-19 therapies: Associations with length of hospital stay, mortality and related costs. Swiss Med. Wkly. 2020, 150, w20446. [Google Scholar] [CrossRef]
- Yan, D.; Liu, X.-Y.; Zhu, Y.-N.; Huang, L.; Dan, B.-T.; Zhang, G.-J.; Gao, Y.-H. Factors associated with prolonged viral shedding and impact of lopinavir/ritonavir treatment in hospitalised non-critically ill patients with SARS-CoV-2 infection. Eur. Respir. J. 2020, 56, 2000799. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Hibino, M.; Hase, R.; Yamamoto, M.; Kasamatsu, Y.; Hirose, M.; Mutoh, Y.; Homma, Y.; Terada, M.; Ogawa, T.; et al. A Prospective, Randomized, Open-Label Trial of Early versus Late Favipiravir Therapy in Hospitalized Patients with COVID-19. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef]
- Udwadia, Z.F.; Singh, P.; Barkate, H.; Patil, S.; Rangwala, S.; Pendse, A.; Kadam, J.; Wu, W.; Caracta, C.F.; Tandon, M. Efficacy and safety of favipiravir, an oral RNA-dependent RNA polymerase inhibitor, in mild-to-moderate COVID-19: A randomized, comparative, open-label, multicenter, phase 3 clinical trial. Int. J. Infect. Dis. 2021, 103, 62–71. [Google Scholar] [CrossRef]
- Balykova, L.A.; Pavelkina, V.F.; Shmyreva, N.V.; Pyataev, N.A.; Selezneva, N.M.; Shepeleva, O.I.; Almyasheva, R.Z. Efficacy and safety of some etiotropic therapeutic schemes for treating patients with novel coronavirus infection (COVID-19). Pharm. Pharmacol. 2020, 8, 150–159. [Google Scholar] [CrossRef]
- Dabbous, H.M.; Abd-Elsalam, S.; El-Sayed, M.H.; Sherief, A.F.; Ebeid, F.F.S.; El Ghafar, M.S.A.; Soliman, S.; Elbahnasawy, M.; Badawi, R.; Tageldin, M.A. Efficacy of favipiravir in COVID-19 treatment: A multi-center randomized study. Arch. Virol. 2021, 166, 949–954. [Google Scholar] [CrossRef]
- Ivashchenko, A.A.; Dmitriev, K.A.; Vostokova, N.V.; Azarova, V.N.; Blinow, A.A.; Egorova, A.N.; Gordeev, I.G.; Ilin, A.P.; Karapetian, R.N.; Kravchenko, D.V.; et al. AVIFAVIR for Treatment of Patients with Moderate Coronavirus Disease 2019 (COVID-19): Interim Results of a Phase II/III Multicenter Randomized Clinical Trial. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Zhao, H.; Zhu, Q.; Zhang, C.; Li, J.; Wei, M.; Qin, Y.; Chen, G.; Wang, K.; Yu, J.; Wu, Z.; et al. Tocilizumab combined with favipiravir in the treatment of COVID-19: A multicenter trial in a small sample size. Biomed. Pharmacother. 2021, 133, 1–8. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering 2020. [Google Scholar] [CrossRef]
- Kocayiğit, H.; Süner, K.Ö.; Tomak, Y.; Demir, G.; Yaylacı, S.; Dheir, H.; Güçlü, E.; Erdem, A.F. Observational study of the effects of Favipiravir vs Lopinavir/Ritonavir on clinical outcomes in critically Ill patients with COVID-19. J. Clin. Pharm. Ther. 2021, 46, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Kasgari, H.A.; Moradi, S.; Shabani, A.M.; Babamahmoodi, F.; Badabi, A.R.D.; Davoudi, L.; Alikhani, A.; Omran, A.H.; Saeedi, M.; Merat, S.; et al. Evaluation of the efficacy of sofosbuvir plus daclatasvir in combination with ribavirin for hospitalized COVID-19 patients with moderate disease compared with standard care: A single-centre, randomized controlled trial. J. Antimicrob. Chemother. 2020, 75, 3373–3378. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-Q.; Tang, S.-Q.; Xu, X.-L.; Zeng, Y.-M.; He, X.-Q.; Li, Y.; Harypursat, V.; Lu, Y.-Q.; Wan, Y.; Zhang, L.; et al. No Statistically Apparent Difference in Antiviral Effectiveness Observed Among Ribavirin Plus Interferon-Alpha, Lopinavir/Ritonavir Plus Interferon-Alpha, and Ribavirin Plus Lopinavir/Ritonavir Plus Interferon-Alpha in Patients with Mild to Moderate Coronavirus Disease 2019: Results of a Randomized, Open-Labeled Prospective Study. Front. Pharmacol. 2020, 11, 1071. [Google Scholar] [CrossRef]
- Eslami, G.; Mousaviasl, S.; Radmanesh, E.; Jelvay, S.; Bitaraf, S.; Simmons, B.; Wentzel, H.; Hill, A.; Sadeghi, A.; Freeman, J.; et al. The impact of sofosbuvir/daclatasvir or ribavirin in patients with severe COVID-19. J. Antimicrob. Chemother. 2020, 75, 3366–3372. [Google Scholar] [CrossRef] [PubMed]
- Elalfy, H.; Besheer, T.; El-Mesery, A.; El-Gilany, A.; Soliman, M.A.; Alhawarey, A.; Alegezy, M.; Elhadidy, T.; Hewidy, A.A.; Zaghloul, H.; et al. Effect of a combination of nitazoxanide, ribavirin, and ivermectin plus zinc supplement (MANS.NRIZ study) on the clearance of mild COVID-19. J. Med. Virol. 2021, 93, 3176–3183. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Su, Y.; Yu, Y.; Wu, C.; Chen, J.; Wang, S.; Jiang, J. Ribavirin therapy for severe COVID-19: A retrospective cohort study. Int. J. Antimicrob. Agents 2020, 56, 106114. [Google Scholar] [CrossRef] [PubMed]
- Nojomi, M.; Yassin, Z.; Keyvani, H.; Makiani, M.J.; Roham, M.; Laali, A.; Dehghan, N.; Navaei, M.; Ranjbar, M. Effect of Arbidol (Umifenovir) on COVID-19: A randomized controlled trial. BMC Infect. Dis. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lian, N.; Xie, H.; Lin, S.; Huang, J.; Zhao, J.; Lin, Q. Umifenovir treatment is not associated with improved outcomes in patients with coronavirus disease 2019: A retrospective study. Clin. Microbiol. Infect. 2020, 26, 917–921. [Google Scholar] [CrossRef]
- Chen, W.; Yao, M.; Fang, Z.; Lv, X.; Deng, M.; Wu, Z. A study on clinical effect of Arbidol combined with adjuvant therapy on COVID-19. J. Med Virol. 2020, 92, 2702–2708. [Google Scholar] [CrossRef]
- Deng, L.; Li, C.; Zeng, Q.; Liu, X.; Li, X.; Zhang, H.; Hong, Z.; Xia, J. Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study. J. Infect. 2020, 81, e1–e5. [Google Scholar] [CrossRef]
- Xu, P.; Huang, J.; Fan, Z.; Huang, W.; Qi, M.; Lin, X.; Song, W.; Yi, L. Arbidol/IFN-α2b therapy for patients with corona virus disease 2019: A retrospective multicenter cohort study. Microbes Infect. 2020, 22, 200–205. [Google Scholar] [CrossRef]
- Gao, W.; Chen, S.; Wang, K.; Chen, R.; Guo, Q.; Lu, J.; Wu, X.; He, Y.; Yan, Q.; Wang, S.; et al. Clinical features and efficacy of antiviral drug, Arbidol in 220 nonemergency COVID-19 patients from East-West-Lake Shelter Hospital in Wuhan: A retrospective case series. Virol. J. 2020, 17, 1–9. [Google Scholar] [CrossRef]
- Lai, C.-C.; Chen, C.-H.; Wang, C.-Y.; Chen, K.-H.; Wang, Y.-H.; Hsueh, P.-R. Clinical efficacy and safety of remdesivir in patients with COVID-19: A systematic review and network meta-analysis of randomized controlled trials. J. Antimicrob. Chemother. 2021. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.K.; Patel, P.B.; Barvaliya, M.; Saurabh, M.K.; Bhalla, H.L.; Khosla, P.P. Efficacy and safety of lopinavir-ritonavir in COVID-19: A systematic review of randomized controlled trials. J. Infect. Public Health 2021, 14, 740–748. [Google Scholar] [CrossRef]
- Shrestha, D.B.; Budhathoki, P.; Khadka, S.; Shah, P.B.; Pokharel, N.; Rashmi, P. Favipiravir versus other antiviral or standard of care for COVID-19 treatment: A rapid systematic review and meta-analysis. Virol. J. 2020, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; Nourian, A.; Ahmadinejad, Z.; Kouchak, H.E.; Jafari, S.; Manshadi, S.A.D.; Rasolinejad, M.; Kebriaeezadeh, A. Efficacy and safety of sofosbuvir/ ledipasvir in treatment of patients with COVID-19; A randomized clinical trial. Acta Biomed. 2020, 91, e2020102. [Google Scholar] [CrossRef]
- Simmons, B.; Wentzel, H.; Mobarak, S.; Eslami, G.; Sadeghi, A.; Asgari, A.A.; Kasgari, H.A.; Fakheri, H.T.; Merat, S.; Hill, A. Sofosbuvir/daclatasvir regimens for the treatment of COVID-19: An individual patient data meta-analysis. J. Antimicrob. Chemother. 2021, 76, 286–291. [Google Scholar] [CrossRef]
- Mobarak, S.; Salasi, M.; Hormati, A.; Khodadadi, J.; Ziaee, M. Evaluation of the Effect of Sofosbuvir and Daclatasvir in Hospitalised COVID-19 Patients: A Randomized Double-Blind Clinical Trial (DISCOVER). 2021. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3792895 (accessed on 20 July 2021).
- Roozbeh, F.; Saeedi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Merat, S.; Wentzel, H.; Levi, J.; Hill, A.; Shamshirian, A. Sofosbuvir and daclatasvir for the treatment of COVID-19 outpatients: A double-blind, randomized controlled trial. J. Antimicrob. Chemother. 2021, 76, 753–757. [Google Scholar] [CrossRef]
- Huang, D.; Yu, H.; Wang, T.; Yang, H.; Yao, R.; Liang, Z. Efficacy and safety of umifenovir for coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 481–490. [Google Scholar] [CrossRef]
- Singh, B.; Ryan, H.; Kredo, T.; Chaplin, M.; Fletcher, T. Chloroquine or hydroxychloroquine for prevention and treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 2021, CD013587. [Google Scholar] [CrossRef]
- Llover, M.N.; Jiménez, M.C. Estado actual de los tratamientos para la COVID-19. FMC Form. Médica Contin. en Atención Primaria 2021, 28, 40–56. [Google Scholar] [CrossRef]
- WHO Discontinues Hydroxychloroquine and Lopinavir/Ritonavir Treatment Arms for COVID-19. Published 2020. Available online: https://www.who.int/news/item/04-07-2020-who-discontinues-hydroxychloroquine-and-lopinavir-ritonavir-treatment-arms-for-covid-19 (accessed on 20 July 2021).
- The RECOVERY Collaborative Group. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef] [PubMed]
- No Clinical Benefit from Use of Hydroxychloroquine in Hospitalised Patients with COVID-19. Published 2020. Available online: https://www.recoverytrial.net/news/statement-from-the-chief-investigators-of-the-randomised-evaluation-of-covid-19-therapy-recovery-trial-on-hydroxychloroquine-5-june-2020-no-clinical-benefit-from-use-of-hydroxychloroquine-in-hospitalised-patients-with-co (accessed on 20 July 2021).
- Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Chloroquine and Hydroxychloroquine. FDA; Published 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and (accessed on 20 July 2021).
- Elavarasi, A.; Prasad, M.; Seth, T.; Sahoo, R.K.; Madan, K.; Nischal, N.; Soneja, M.; Sharma, A.; Maulik, S.K.; Shalimar; et al. Chloroquine and Hydroxychloroquine for the Treatment of COVID-19: A Systematic Review and Meta-analysis. J. Gen. Intern. Med. 2020, 35, 3308–3314. [Google Scholar] [CrossRef]
- Axfors, C.; Schmitt, A.M.; Janiaud, P.; Hooft, J.V.; Abd-Elsalam, S.; Abdo, E.F.; Abella, B.S.; Akram, J.; Amaravadi, R.K.; Angus, D.C.; et al. Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials. Nat. Commun. 2021, 12, 1–13. [Google Scholar] [CrossRef]
- Khateeb, J.; Li, Y.; Zhang, H. Emerging SARS-CoV-2 variants of concern and potential intervention approaches. Crit. Care 2021, 25, 244. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Category | Group | Drug | Supposed Mechanism of Action |
|---|---|---|---|
| Antivirals | Cell membrane fusion inhibitors | Umifenovir (Arbidol) [28] | Blocks the entry and intracellular vesicular traffic |
| RNA polymerase inhibitors / RNA synthesis inhibitors | Remdesivir (GS-5734) [29] | Nucleotide analog (Adenosine), prodrug, RNA-dependent RNA polymerase (RdRp) inhibitor | |
| Favipiravir [30,31,32] | Nucleotide precursor analog, oral drug, inhibits the viral RNA dependent RNA polymerase (RdRp) (its triphosphoribosylated form, is recognized as a substrate RdRp) acting as a chain terminator and inhibiting the viral polymerase activity | ||
| Ribavirin [33] | Nucleoside analogue, RNA-dependent RNA polymerase (RdRp) inhibitor | ||
| Viral protease inhibitors | Lopinavir/Ritonavir [23] | Lopinavir (HIV-1 aspartate protease inhibitor); Ritonavir (CYP450 inhibitor) | |
| Antimalarials | Aminoquinolines | Chloroquine/Hydroxychloroquine [34] | Increases endosomal pH and hinders the interaction of the virus with the ACE-2 receptor on the cell surface. |
| Serine protease inhibitors | Camostat Mesylate [30] | Blocks the entry of SARS-CoV-2 into the host cell by inhibiting TMPRSS2 | |
| Immunotherapy | IL-6 inhibitors [35] | Tocilizumab | Blocks soluble IL-6 receptors attached to the cell membrane. |
| Sarilumab | Blocks soluble IL-6 receptors attached to the cell membrane | ||
| Convalescent plasma or hyperimmune immunoglobulins [33] | Treatment by plasma or purified monoclonal antibodies produced in patients already recovered from COVID-19 | ||
| Corticosteroids | Dexamethasone Hydrocortisone [33] | Reduce the host’s inflammatory response in the lungs |
| Patient (P) | We included individuals with a confirmed diagnosis of COVID-19, with no restrictions on age, sex, ethnicity, or severity of the disease. |
| Intervention (I) | We included the following antiviral treatments: remdesivir, lopinavir/ritonavir, favipiravir, umifenovir, or ribavirin. Co-interventions with other antivirals were allowed but must be comparable between intervention groups. |
| Comparison (C) | We included the following comparisons for studies with a control arm: placebo, standard care, another dosage regimen, any other drug treatment (including but not limited to antivirals) |
| Outcome (O) | We included studies that evaluate efficacy of interventions being this estimated by mortality rate, improvement of clinical symptoms, need for mechanical ventilation, length of hospital stay, number of patients admitted to ICU, length of stay on the ICU, rate of viral clearance or time to viral clearance. We also included studies that assess safety outcomes as measured by proportion of mild, moderate, or severe adverse events. Secondary outcomes include need to discontinue treatment because of adverse events, dosage regimen, and duration of antiviral treatment. |
| Reference | Study Design/Population of Study | No. of Participants | Median Age, [IQR], Years | Sex ♂ |
|---|---|---|---|---|
| Remdesivir vs. Standard of care | ||||
| Spinner C., et al., 2020 [46] | RCT (open-label, phase III, multicentre)/Adults with moderate COVID-19 | IG1: n = 197 IG2: n = 199 CG: n = 200 | IG1: 56 [45–66] IG2: 58 [48–66] CG: 57 [45–66] | IG1: 61% IG2: 60% CG: 63% |
| Remdesivir for 5 days vs. 10 days | ||||
| Goldman J., et al., 2020 [47] | RCT (open-label, phase III, multicentre)/Patients with severe COVID-19 | IG: n = 200; CG: n = 197 | IG: 61 [50–69] CG: 62 [50–71] | IG: 60% CG: 68% |
| Remdesivir vs. Placebo | ||||
| Beigel J., et al., 2020 [48] | RCT (double blind, multicentre, placebo-controlled)/Adults with moderate or severe COVID-19 | IG: n = 541 CG: n = 521 | Mean age, ± SD: IG: 58.6 ± 14.6 CG: 59.2 ± 15.4 | IG: 65.1% CG: 63.7% |
| Remdesivir vs. Placebo | ||||
| Wang Y., et al., 2020 [49] | RCT (double blind, multicentre, placebo-controlled)/Adults with severe COVID-19 | IG: n = 158 CG: n = 78 | IG: 66 [57–73] CG: 64 [53–70] | IG: 56% CG: 65% |
| Remdesivir vs. Standard of care | ||||
| Pan et al., 2021 [50] | RCT (open-label, international, multicentre) WHO Solidarity trial consortium/Adults with COVID-19 | IG: n = 2743 CG: n = 2708 | Age 50–69 years: IG: 46.7% CG: 47.5% | IG: 62.2% CG: 63.7% |
| Remdesivir vs. Standard of care | ||||
| Pasquini Z., et al., 2020 [51] | Observational and retrospective study/Critically ill patients under MV with confirmed COVID-19 and admitted to the intensive care unit | IG: n = 25 CG: n = 26 | IG: 64 [57–75] CG: 70 [63.3–76] | IG: 92% CG: 92.3% |
| Remdesivir vs. Standard of care | ||||
| Olender S., et al., 2020 [52] | IG: data from a phase III prospective, randomized RDV trial; CG: data from a longitudinal retrospective cohort/Adults with severe COVID-19 | IG: n = 312 CG: n = 818 | Age 40–64 years IG: 50% CG: 50% | IG: 59% CG: 59% |
| Remdesivir vs. Supportive care | ||||
| Kalligeros M., et al., 2020 [53] | Observational, retrospective study/Adults with severe COVID-19 | GI: n = 99 GC: n = 125 | IG: 58 [50–68] CG: 60 [50–68] | IG: 69.7% CG: 64.8% |
| (Barticinib + Remdesivir) vs. Remdesivir | ||||
| Kalil P., et al., 2020 [54] | Double blind RCT (placebo-controlled)/Hospitalized adults with COVID-19 | IG: n = 515 CG: n = 518 | Mean age, ± SD: IG: 55 ± 15.4: CG: 55.8 ± 16 | IG: 61.9% CG: 64.3% |
| Reference | Study Design /Population of Study | No. of Participants | Median Age [IQR], Years | Sex ♂ |
|---|---|---|---|---|
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Cao B., et al., 2020 [55] | RCT (open-label)/Adults with severe COVID-19 | IG: n = 99 CG: n = 100 | IG: 58 [50–68] CG: 58 [48–68] | IG: 61.6% CG: 59.0% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Horby, P., et al., 2020 [56] | RCT (open-label) RECOVERY/Patients with COVID-19 | IG: n = 1616 CG: n = 3424 | Mean age, ± SD: IG: 66 ± 16 CG: 66.4 ± 15.8 | IG: 60% CG: 61% |
| (Lopinavir/Ritonavir + Ribavarin + IFNβ1b) vs. Lopinavir/Ritonavir | ||||
| Hung I., et al., 2020 [57] | RCT (phase II, open-label, multicentre)/Adults with mild to moderate COVID-19 | IG: n = 86 CG: n = 41 | IG: 51 [31.0–61.3] CG: 52 [33.5–62.5] | IG: 52% CG: 56% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Pan et al., 2021 [50] | RCT (open-label, international, multicentre) WHO Solidarity trial consortium/Adults with COVID-19 | IG: n = 1399 CG: n = 1372 | Age 50–69: IG: 42.67% CG: 43.44% | IG: 60.83% CG: 58.45% |
| Lopinavir/Ritonavir vs. Standard of care // (Lopinavir/Ritonavir + IFN-β1a) vs Standard of care | ||||
| Ader F., et al., 2021 [58] | RCT (open-label, multicentre, phase III) DisCoVery trial/Patients with moderate to severe COVID-19 | IG1: n = 145 IG2: n = 145 CG: n = 148 | IG1: 63 [55–71] IG2: 64 [53–71] CG: 62 [52–71] | IG1: 73.1% IG2: 71% GC: 70.9% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Gao, G., et al., 2020 [59] | Observational, retrospective study/Adults with non-severe COVID-19 | IG1: n = 51 CG: n = 59 | IG1: 33 [27–41] CG: 30 [23–45] | IG1: 58.8% CG: 50.8% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Grimaldi D., et al., 2020 [60] | Observational multicentre cohort study/Adults with moderate to severe COVID-19 | IG1: n = 57 CG: n = 85 | Mean age, ± SD: IG1: 63 ± 12 CG: 63 ± 11 | IG1: 80% CG: 75% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Choi M., et al., 2020 [61] | Observational retrospective cohort study/Adults with mild to moderate COVID-19 | IG1: n = 1407 CG: n = 1407 | Mean age, ± SD: IG1: 45.9 ± 15.6 CG: 45.9 ± 15.6 | IG1: 38.59% CG: 38.59% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Ye X, et al., 2020 [62] | Observational, retrospective study/Patients with COVID-19 | IG: n = 42 CG: n = 5 | N/A | IG: 50% CG: 20% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Lecronier M., et al., 2020 [63] | Observational, retrospective study/Patients with severe COVID-19 requiring ICU admission | IG1: n = 20 IG2: n = 38 CG: n = 22 | IG1: 55 [49–61] IG2: 59 [53–66] CG: 63 [54–70] | IG1: 75% IG2: 82% CG: 82% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Lu J., et al., 2020 [64] | Observational, retrospective, multicentre study/Paediatric patients with mild COVID-19 | IG: n=23 CG: n=92 | IG: 8.66 [2.44–11.9] CG: 8.85 [2.00–11.6] | IG: 56.52% CG: 56.52% |
| Lopinavir/Ritonavir + Hydroxychloroquine: Early treatment (<5 days from symptom onset) vs. Late treatment (>5 days from symptom onset) | ||||
| Giacomelli A., et al., 2020 [65] | Retrospective cohort study/Adults with COVID-19 | IG: n = 43 CG: n = 129 | IG: 64.9 [55–78] CG: 61.7 [50.2–72.3] | IG: 67.4% CG: 73.6% |
| Lopinavir/Ritonavir vs. Arbidol | ||||
| Zhu, Z., et al., 2020 [66] | Observational, retrospective study/Adults with COVID-19 | IG: n = 34 CG: n = 16 | IG: 40.5 [34.8–52.3] CG: 26.5 [23.3–52.5] | IG: 58.8% CG: 37.5% |
| Lopinavir/Ritonavir vs. Standard of care | ||||
| Vernaz N., et al., 2020 [67] | Observational, retrospective, single centre, cohort study/Patients with COVID-19 | IG1: n = 93 IG2: n = 83 IG3: n = 158 CG: n = 506 | Mean age, ± SD: IG1: 66.14 ± 15.77 IG2: 63.4 ± 17.4 IG3: 62.15 ± 14.77 CG: 70.75 ± 20.01 | IG1: 59.1% IG2: 55.4% IG3: 36.1% CG: 43.9% |
| Lopinavir/Ritonavir vs. Standard therapy | ||||
| Yan D., et al., 2020 [68] | Observational, retrospective study/Non critically ill COVID-19 patients | IG: n = 78 CG: n = 42 | IG: 50 [34–61] CG: 57 [36.5–66] | IG: 44.9% CG: 45.2% |
| Reference | Study Design/Population of Study | No. of Participants | Median Age, [IQR], Years | Sex ♂ |
|---|---|---|---|---|
| Favipiravir early vs. late administration | ||||
| Doi Y., et al., 2020 [69] | RCT (open-label, prospective, multicentre)/Patients with asymptomatic or mild COVID-19 | IG: n = 44 CG: n = 45 | IG: 48 [34.5–68] CG: 51 [39.5-62] | IG: 52.3% CG: 70.5% |
| Favipiravir vs. Supportive care | ||||
| Udwadia Z., et al., 2020 [70] | RCT (open-label, phase III, multicentre)/Adults with mild to moderate COVID-19 | IG: n = 72 CG: n = 75 | Mean age, ± SD: IG: 43.6 ± 12.2 CG: 43 ± 11.2 | IG: 70.8% CG: 76% |
| Favipiravir vs. Standard of care | ||||
| Balykova L., et al., 2020 [71] | RCT (open-label, multicentre)/Adults with moderate COVID-19 and presence of bilateral pneumonia | IG: n = 17 CG: n = 22 | Mean age, ± SD: IG: 47.12 ± 2.26 CG: 47.5 ± 1.99 | N/A |
| Favipiravir vs. Chloroquine | ||||
| Dabbous H., et al., 2020 [72] | RCT (open-label, phase II/III, multicentre)/Adults with mild to moderate COVID-19 | IG: n = 44 CG: n =48 | Mean age, ± SD: IG: 34.86 ± 15.9 CG: 36.15 ± 17.7 | IG: 45.5% CG: 52.1% |
| Favipiravir vs. Standard of care | ||||
| Ivashchenko, A., et al., 2020 [73] | RCT (open-label, phase II/III, multicentre)/Adults with moderate COVID-19 | IG1: n = 20 IG2: n = 20 CG: n = 20 | N/A | N/A |
| (Favipiravir + Tocilizumab) vs. Favipiravir | ||||
| Zhao H., et al., 2020 [74] | RCT (multicentre)/Adults with COVID-19 | IG: n = 14 CG: n = 7 | IG: 75 [34–81] CG: 70 [45–89] | IG: 42.9% CG: 71.4% |
| (Favipiravir + IFN-α1b) vs. (Lopinavir/Ritonavir + IFN-α1b) | ||||
| Cai Q., et al., 2020 [75] | Comparative controlled study (non-randomized, open-label)/Patients with confirmed COVID-19 | IG: n = 35 CG: n = 45 | IG: 43 [35.5–59] CG: 49 [36–61] | IG: 40% CG: 46.7% |
| (Favipiravir + Hydroxychloroquine) vs. (Lopinavir/Ritonavir + Hydroxychloroquine) | ||||
| Kocayiğit H., et al., 2020 [76] | Observational retrospective study/Critically ill patients with COVID-19 (admitted to ICU) | IG: n = 65 CG: n = 42 | Mean age, ± SD: IG: 69.8 ± 12.6 CG: 70.6 ± 12.7 | IG: 58.5% CG: 64.3% |
| Reference | Study Design/Population of Study | No. of Participants | Median Age, [IQR], Years: | Sex ♂ |
|---|---|---|---|---|
| (Ribavirin + Sofosbuvir + Daclatasvir) vs. Standard therapy | ||||
| Abbaspour Kasgari H., et al., 2020 [77] | RCT (single centre)/Adults with moderate COVID-19 | IG: n = 24 CG: n = 24 | IG: 45 [38–69] CG: 60 [47.5–68.5] | IG: 46% CG: 29% |
| (Ribavirin + IFN-α) vs. (Lopinavir/Ritonavir + IFN-α) vs (Ribavirin + Lopinavir/Ritonavir + IFN-α) | ||||
| Huang Y., et al., 2020 [78] | RCT (open-label, single centre, prospective)/Adults with mild to moderate COVID-19 | IG1: n = 33 IG2: n = 36 IG3: n = 32 | Mean age, ± SD: IG1: 40.3 ± 12.5 IG2: 43.3 ± 10.4 IG3: 43.8 ± 11.7 | IG1: 55% IG2: 53% IG3: 28% |
| Sofosbuvir/Daclastavir vs. Ribavirin | ||||
| Eslami G., et al., 2020 [79] | Open-label, parallel trial, prospective, pseudorandom allocation/Adults with severe COVID-19 | IG: n = 35 CG: n = 27 | IG: 62 [47–69] CG: 60 [43–73] | IG: 49% CG: 52% |
| (Ribavirin + Nitazoxanide + Ivermectin + Zinc supplement) vs. Standard of care | ||||
| Elalfy H., et al., 2020 [80] | Controlled clinical trial (non-randomized, Phase I)/Adults with mild to moderate COVID-19 | IG: n = 62 CG: n = 51 | Mean age, ± SD: IG: 37.9 ± 11.9 CG: 37.5 ± 10.9 | IG: 48.4%; CG: 43.1% |
| Ribavirin vs. Supportive care | ||||
| Tong S., et al., 2020 [81] | Observational, retrospective, single centre cohort study/Patients with severe COVID-19 | IG: n = 44 CG: n = 71 | Mean age, ± SD: IG: 54.6 ± 13.3 CG: 55.1 ± 16.2 | IG: 43.2%; CG: 60.6% |
| Reference | Study Design/Population of Study | No. of Participants | Median Age, [IQR], Years | Sex ♂ |
|---|---|---|---|---|
| Arbidol vs. Lopinavir/Ritonavir | ||||
| Nojomi M., et al., 2020 [82] | RCT (open-label)/Adults with COVID-19 | IG: n = 50 CG: n = 50 | Mean age, ± SD: IG: 56.6 ± 17.8 CG: 56.2 ± 14.8 | IG: 66% CG: 54% |
| Umifenovir vs. Standard of care | ||||
| Lian N., et al., 2020 [83] | Observational, retrospective study (single centre)/Adults with COVID-19 in a non-ICU | IG: n = 45 CG: n = 36 | IG: 58 [50–66] CG: 63 [49–66] | IG: 62% CG: 47% |
| Arbidol vs. Standard of care | ||||
| Chen W., et al., 2020 [84] | Observational, retrospective study/Adults with COVID-19 | IG: n = 42 CG: n = 20 | IG: N/A CG: N/A | IG: 57.1% CG: 50% |
| (Arbidol + Lopinavir/Ritonavir) vs. Lopinavir/Ritonavir | ||||
| Deng L., et al., 2020 [85] | Observational retrospective cohort study (single centre)/Adults with COVID-19 without IMV | IG: n = 16 CG: n = 17 | Mean age, ± SD: IG: 41.8 ± 14.08 CG: 47.25 ± 17.25 | IG: 43.8% CG: 58.8% |
| (Arbidol + IFN-α2b) vs. IFN-α2b | ||||
| Xu P., et al., 2020 [86] | Retrospective, multicentre cohort study/Adults with COVID-19 without IMV | IG: n = 71 CG: n = 70 | Median age, [range] IG: 50.9 [24–75] CG: 53.2 [26–83] | IG: 57.7% CG: 47.1% |
| Arbidol vs. Standard therapy | ||||
| Gao W., et al., 2020 [87] | Observational, retrospective cohort study/Patients with COVID-19 | IG: n = 90 CG: n = 45 | IG: 48 [36–56] CG: 51 [40–61] | IG: 57.8% CG: 48.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil Martínez, V.; Avedillo Salas, A.; Santander Ballestín, S. Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review. Pharmaceuticals 2021, 14, 736. https://doi.org/10.3390/ph14080736
Gil Martínez V, Avedillo Salas A, Santander Ballestín S. Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review. Pharmaceuticals. 2021; 14(8):736. https://doi.org/10.3390/ph14080736
Chicago/Turabian StyleGil Martínez, Victoria, Ana Avedillo Salas, and Sonia Santander Ballestín. 2021. "Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review" Pharmaceuticals 14, no. 8: 736. https://doi.org/10.3390/ph14080736
APA StyleGil Martínez, V., Avedillo Salas, A., & Santander Ballestín, S. (2021). Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review. Pharmaceuticals, 14(8), 736. https://doi.org/10.3390/ph14080736