
Antidepressants in Alzheimer’s Disease: A Focus on the Role of Mirtazapine



Abstract
:1. Introduction
2. Alzheimer’s Disease and Depression
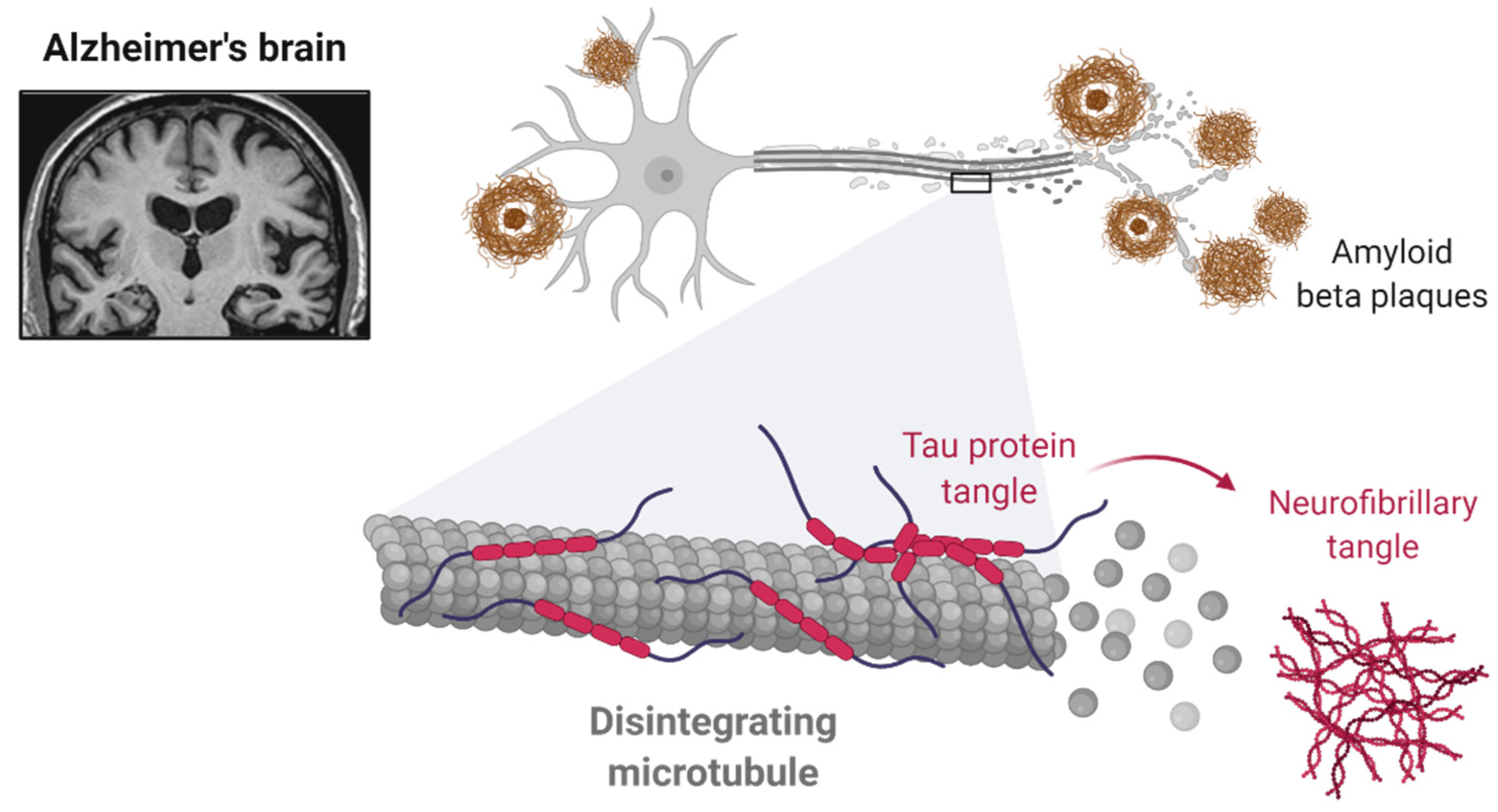
2.1. Alzheimer’s Disease: A Brief Characterization
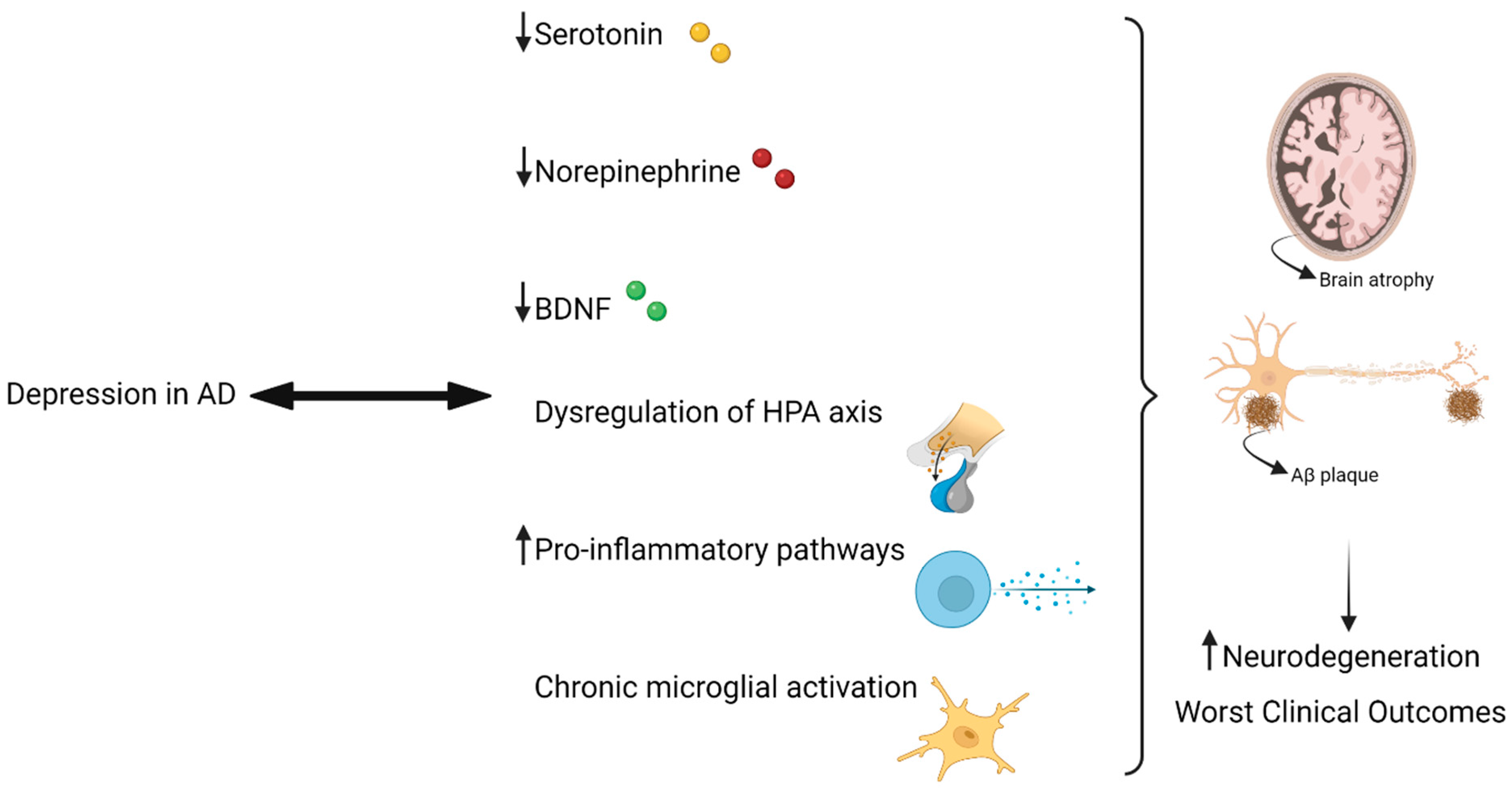
2.2. Depression in Alzheimer’s Disease
2.3. Antidepressants in Alzheimer’s Disease
3. Mirtazapine
3.1. Characterization and Clinical Indications
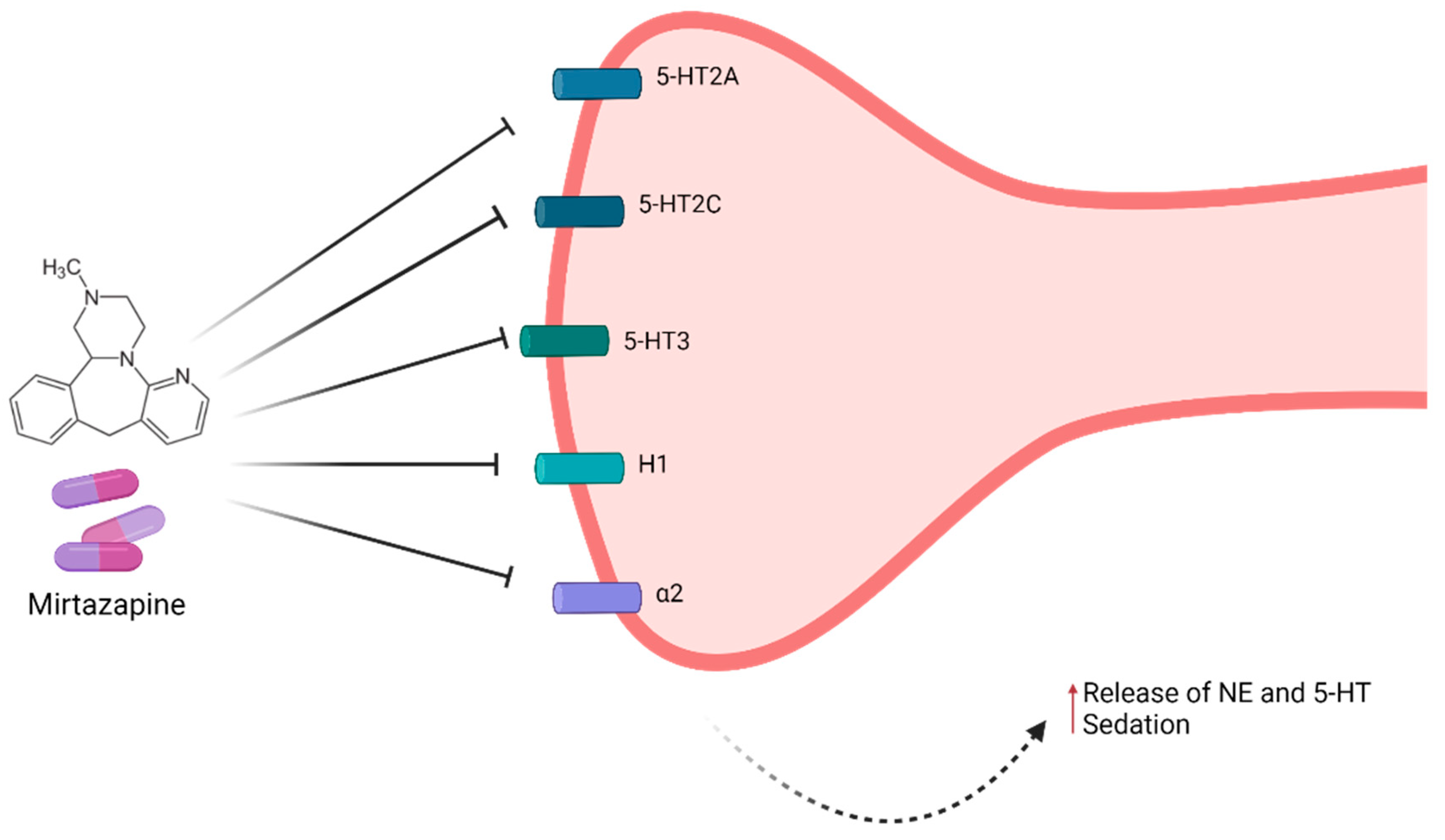
3.2. Mechanism of Action and Pharmacokinetics of Mirtazapine
3.3. Mirtazapine in Alzheimer’s Disease
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef]
- Duthey, B. Background paper 6.11: Alzheimer disease and other dementias. Public Health Approach Innov. 2013, 6, 1–74. [Google Scholar]
- Depression Alzheimer’s Association. Available online: https://www.alz.org/help-support/caregiving/stages-behaviors/depression (accessed on 13 August 2021).
- Dafsari, F.S.; Jessen, F. Depression—An underrecognized target for prevention of dementia in Alzheimer’s disease. Transl. Psychiatry 2020, 10, 160. [Google Scholar] [CrossRef] [PubMed]
- Agüera-Ortiz, L.; García-Ramos, R.; Grandas Pérez, F.J.; López-Álvarez, J.; Montes Rodríguez, J.M.; Olazarán Rodríguez, F.J.; Olivera Pueyo, J.; Pelegrin Valero, C.; Porta-Etessam, J. Depression in Alzheimer’s Disease: A Delphi Consensus on Etiology, Risk Factors, and Clinical Management. Front. Psychiatry 2021, 12, 141. [Google Scholar] [CrossRef] [PubMed]
- Long, J.M.; Holtzman, D.M. Alzheimer Disease: An Update on Pathobiology and Treatment Strategies. Cell 2019, 179, 312–339. [Google Scholar] [CrossRef]
- Scheltens, P.; De Strooper, B.; Kivipelto, M.; Holstege, H.; Chételat, G.; Teunissen, C.E.; Cummings, J.; van der Flier, W.M. Alzheimer’s disease. Lancet 2021, 397, 1577–1590. [Google Scholar] [CrossRef]
- Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 27 July 2021).
- Kumar, A.; Sidhu, J.; Goyal, A.; Tsao, J.W. Alzheimer Disease; StatPearls Publishing: Treasure Island, FL, USA, 2021; pp. 1–27. [Google Scholar]
- De-Paula, V.J.; Radanovic, M.; Diniz, B.S.; Forlenza, O.V. Alzheimer’s Disease. Subcell. Biochem. 2012, 65, 329–352. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Khachaturian, A.S.; Trzepacz, P.; Amatniek, J.; Cedarbaum, J.; Brashear, R.; Miller, D.S. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 532–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Prim. 2021, 7, 1–21. [Google Scholar] [CrossRef]
- Metaxas, A.; Kempf, S.J. Neurofibrillary tangles in Alzheimer’s disease: Elucidation of the molecular mechanism by immunohistochemistry and tau protein phospho-proteomics. Neural Regen. Res. 2016, 11, 1579. [Google Scholar] [CrossRef]
- Chen, G.; Xu, T.; Yan, Y.; Zhou, Y.; Jiang, Y.; Melcher, K.; Xu, H.E. Amyloid beta: Structure, biology and structure-based therapeutic development. Acta Pharmacol. Sin. 2017, 38, 1205–1235. [Google Scholar] [CrossRef]
- Ferreira-Vieira, T.H.; Guimaraes, I.M.; Silva, F.R.; Ribeiro, F.M. Alzheimer’s Disease: Targeting the Cholinergic System. Curr. Neuropharmacol. 2016, 14, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinney, J.W.; Bemiller, S.M.; Murtishaw, A.S.; Leisgang, A.M.; Salazar, A.M.; Lamb, B.T. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 575. [Google Scholar] [CrossRef]
- Gella, A.; Durany, N. Oxidative stress in Alzheimer disease. Cell Adh. Migr. 2009, 3, 88. [Google Scholar] [CrossRef] [Green Version]
- BioRender Templates. Available online: https://app.biorender.com/biorender-templates (accessed on 16 August 2021).
- Kraus, C.; Kadriu, B.; Lanzenberger, R.; Zarate, C.A., Jr.; Kasper, S. Prognosis and improved outcomes in major depression: A review. Transl. Psychiatry 2019, 9, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Kaltenboeck, A.; Harmer, C. The neuroscience of depressive disorders: A brief review of the past and some considerations about the future. Brain Neurosci. Adv. 2018, 2, 239821281879926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, S.H. Core symptoms of major depressive disorder: Relevance to diagnosis and treatment. Dialogues Clin. Neurosci. 2008, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.W.; Bharwani, A.; Lee, K.R.; Fox, M.; Thomson, J.A. Is serotonin an upper or a downer? The evolution of the serotonergic system and its role in depression and the antidepressant response. Neurosci. Biobehav. Rev. 2015, 51, 164–188. [Google Scholar] [CrossRef]
- Otte, C.; Gold, S.M.; Penninx, B.W.; Pariante, C.M.; Etkin, A.; Fava, M.; Mohr, D.C.; Schatzberg, A.F. Major depressive disorder. Nat. Rev. Dis. Prim. 2016, 2, 16065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yohn, C.N.; Gergues, M.M.; Samuels, B.A. The role of 5-HT receptors in depression. Mol. Brain 2017, 10, 1–12. [Google Scholar] [CrossRef]
- Willeit, M.; Sitte, H.H.; Thierry, N.; Michalek, K.; Praschak-Rieder, N.; Zill, P.; Winkler, D.; Brannath, W.; Fischer, M.B.; Bondy, B.; et al. Enhanced Serotonin Transporter Function during Depression in Seasonal Affective Disorder. Neuropsychopharmacology 2008, 33, 1503–1513. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, J.S.; Bell, C.E.; Pollard, D.A. Revisiting the Monoamine Hypothesis of Depression: A New Perspective. Perspect. Medicin. Chem. 2014, 6, PMC-S11375. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer Disease Treatment & Management: Approach Considerations, Treatment of Mild to Moderate Disease, Treatment of Moderate to Severe Disease. Available online: https://emedicine.medscape.com/article/1134817-treatment#d12 (accessed on 13 August 2021).
- Ownby, R.L.; Crocco, E.; Acevedo, A.; John, V.; Loewenstein, D. Depression and Risk for Alzheimer Disease: Systematic Review, Meta-analysis, and Metaregression Analysis. Arch. Gen. Psychiatry 2006, 63, 530. [Google Scholar] [CrossRef] [Green Version]
- Lozupone, M.; La Montagna, M.; D’Urso, F.; Piccininni, C.; Sardone, R.; Dibello, V.; Giannelli, G.; Solfrizzi, V.; Greco, A.; Daniele, A.; et al. Pharmacotherapy for the treatment of depression in patients with alzheimer’s disease: A treatment-resistant depressive disorder. Expert Opin. Pharmacother. 2018, 19, 823–842. [Google Scholar] [CrossRef] [PubMed]
- Ismail, Z.; Elbayoumi, H.; Fischer, C.E.; Hogan, D.B.; Millikin, C.P.; Schweizer, T.; Mortby, M.E.; Smith, E.E.; Patten, S.B.; Fiest, K.M. Prevalence of Depression in Patients with Mild Cognitive Impairment. JAMA Psychiatry 2017, 74, 58. [Google Scholar] [CrossRef] [PubMed]
- Defrancesco, M.; Marksteiner, J.; Kemmler, G.; Fleischhacker, W.W.; Blasko, I.; Deisenhammer, E.A. Severity of Depression Impacts Imminent Conversion from Mild Cognitive Impairment to Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 59, 1439–1448. [Google Scholar] [CrossRef]
- Rapp, M.A.; Schnaider-Beeri, M.; Grossman, H.T.; Sano, M.; Perl, D.P.; Purohit, D.P.; Gorman, J.M.; Haroutunian, V. Increased Hippocampal Plaques and Tangles in Patients With Alzheimer Disease with a Lifetime History of Major Depression. Arch. Gen. Psychiatry 2006, 63, 161. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Steele, C.; Baker, L.; Galik, E.; Kopunek, S.; Steinberg, M.; Warren, A. Major and minor depression in Alzheimer’s disease: Prevalence and impact. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Qiu, W.Q.; Zhu, H.; Dean, M.; Liu, Z.; Vu, L.; Fan, G.; Li, H.; Mwamburi, M.; Steffens, D.C.; Au, R. Amyloid-associated depression and ApoE4 allele: Longitudinal follow-up for the development of Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2016, 31, 316–322. [Google Scholar] [CrossRef]
- Burke, A.D.; Goldfarb, D.; Bollam, P.; Khokher, S. Diagnosing and Treating Depression in Patients with Alzheimer’s Disease. Neurol. Ther. 2019, 8, 325. [Google Scholar] [CrossRef] [Green Version]
- Holmes, C.; Arranz, M.; Collier, D.; Powell, J.; Lovestone, S. Depression in Alzheimer’s disease: The effect of serotonin receptor gene variation. Am. J. Med. Genet. 2003, 119B, 40–43. [Google Scholar] [CrossRef]
- Heneka, M.T.; Carson, M.J.; El Khoury, J.; Landreth, G.E.; Brosseron, F.; Feinstein, D.L.; Jacobs, A.H.; Wyss-Coray, T.; Vitorica, J.; Ransohoff, R.M.; et al. Neuroinflammation in Alzheimer’s disease. Lancet Neurol. 2015, 14, 388–405. [Google Scholar] [CrossRef] [Green Version]
- Sierksma, A.S.R.; van den Hove, D.L.A.; Steinbusch, H.W.M.; Prickaerts, J. Major depression, cognitive dysfunction and Alzheimer’s disease: Is there a link? Eur. J. Pharmacol. 2010, 626, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Sheline, Y.I.; Gado, M.H.; Kraemer, H.C. Untreated Depression and Hippocampal Volume Loss. Am. J. Psychiatry 2003, 160, 1516–1518. [Google Scholar] [CrossRef] [Green Version]
- Green, K.N. Glucocorticoids Increase Amyloid-beta and Tau Pathology in a Mouse Model of Alzheimer’s Disease. J. Neurosci. 2006, 26, 9047–9056. [Google Scholar] [CrossRef] [Green Version]
- Neto, F.L.; Borges, G.; Torres-Sanchez, S.; Mico, J.A.; Berrocoso, E. Neurotrophins Role in Depression Neurobiology: A Review of Basic and Clinical Evidence. Curr. Neuropharmacol. 2011, 9, 530–552. [Google Scholar] [CrossRef] [Green Version]
- Mattson, M.P.; Maudsley, S.; Martin, B. BDNF and 5-HT: A dynamic duo in age-related neuronal plasticity and neurodegenerative disorders. Trends Neurosci. 2004, 27, 589–594. [Google Scholar] [CrossRef]
- Mdawar, B.; Ghossoub, E.; Khoury, R. Selective serotonin reuptake inhibitors and Alzheimer’s disease. Neural Regen. Res. 2020, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Herbert, J.; Lucassen, P.J. Depression as a risk factor for Alzheimer’s disease: Genes, steroids, cytokines and neurogenesis—What do we need to know? Front. Neuroendocrinol. 2016, 41, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Sims, R.; van der Lee, S.J.; Naj, A.C.; Bellenguez, C.; Badarinarayan, N.; Jakobsdottir, J.; Kunkle, B.W.; Boland, A.; Raybould, R.; Bis, J.C.; et al. Rare coding variants in PLCG2, ABI3, and TREM2 implicate microglial-mediated innate immunity in Alzheimer’s disease. Nat. Genet. 2017, 49, 1373–1384. [Google Scholar] [CrossRef]
- Harrington, K.D.; Gould, E.; Lim, Y.Y.; Ames, D.; Pietrzak, R.H.; Rembach, A.; Rainey-Smith, S.; Martins, R.N.; Salvado, O.; Villemagne, V.L.; et al. Amyloid burden and incident depressive symptoms in cognitively normal older adults. Int. J. Geriatr. Psychiatry 2017, 32, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, J.R.; Rabin, J.S.; Buckley, R.F.; Locascio, J.J.; Quiroz, Y.T.; Yang, H.-S.; Vannini, P.; Amariglio, R.E.; Rentz, D.M.; Properzi, M.; et al. Longitudinal Association of Depression Symptoms With Cognition and Cortical Amyloid Among Community-Dwelling Older Adults. JAMA Netw. Open 2019, 2, e198964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassano, T.; Calcagnini, S.; Carbone, A.; Bukke, V.N.; Orkisz, S.; Villani, R.; Romano, A.; Avolio, C.; Gaetani, S. Pharmacological Treatment of Depression in Alzheimer’s Disease: A Challenging Task. Front. Pharmacol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- BioRender. Available online: https://biorender.com/ (accessed on 16 August 2021).
- Schmitt, J.; Wingen, M.; Ramaekers, J.; Evers, E.; Riedel, W. Serotonin and Human Cognitive Performance. Curr. Pharm. Des. 2006, 12, 2473–2486. [Google Scholar] [CrossRef] [PubMed]
- Caraci, F.; Copani, A.; Nicoletti, F.; Drago, F. Depression and Alzheimer’s disease: Neurobiological links and common pharmacological targets. Eur. J. Pharmacol. 2010, 626, 64–71. [Google Scholar] [CrossRef]
- Khoury, R.; Grossberg, G.T. Impact of Antidepressant Use on the Trajectory of Alzheimer’s Disease: Evidence, Mechanisms, and Therapeutic Implications. CNS Drugs 2018, 33, 17–29. [Google Scholar] [CrossRef]
- Kessing, L.V.; Søndergård, L.; Forman, J.L.; Andersen, P.K. Antidepressants and dementia. J. Affect. Disord. 2009, 117, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Lyketsos, C.G.; DelCampo, L.; Steinberg, M.; Miles, Q.; Steele, C.D.; Munro, C.; Baker, A.S.; Sheppard, J.-M.E.; Frangakis, C.; Brandt, J.; et al. Treating Depression in Alzheimer Disease. Arch. Gen. Psychiatry 2003, 60, 737. [Google Scholar] [CrossRef]
- Mowla, A.; Mosavinasab, M.; Pani, A. Does Fluoxetine Have Any Effect on the Cognition of Patients with Mild Cognitive Impairment? J. Clin. Psychopharmacol. 2007, 27, 67–70. [Google Scholar] [CrossRef]
- Bartels, C.; Wagner, M.; Wolfsgruber, S.; Ehrenreich, H.; Schneider, A. Impact of SSRI Therapy on Risk of Conversion From Mild Cognitive Impairment to Alzheimer’s Dementia in Individuals With Previous Depression. Am. J. Psychiatry 2018, 175, 232–241. [Google Scholar] [CrossRef]
- Cirrito, J.R.; Disabato, B.M.; Restivo, J.L.; Verges, D.K.; Goebel, W.D.; Sathyan, A.; Hayreh, D.; D’Angelo, G.; Benzinger, T.; Yoon, H.; et al. Serotonin signaling is associated with lower amyloid-β levels and plaques in transgenic mice and humans. Proc. Natl. Acad. Sci. USA 2011, 108, 14968–14973. [Google Scholar] [CrossRef] [Green Version]
- Wyss-Coray, T.; Rogers, J. Inflammation in Alzheimer Disease—A Brief Review of the Basic Science and Clinical Literature. Cold Spring Harb. Perspect. Med. 2012, 2, a006346. [Google Scholar] [CrossRef]
- Sheline, Y.I.; West, T.; Yarasheski, K.; Swarm, R.; Jasielec, M.S.; Fisher, J.R.; Ficker, W.D.; Yan, P.; Xiong, C.; Frederiksen, C.; et al. An Antidepressant Decreases CSF A Production in Healthy Individuals and in Transgenic AD Mice. Sci. Transl. Med. 2014, 6, 236re4. [Google Scholar] [CrossRef] [Green Version]
- Sun, D.-S.; Gao, L.-F.; Jin, L.; Wu, H.; Wang, Q.; Zhou, Y.; Fan, S.; Jiang, X.; Ke, D.; Lei, H.; et al. Fluoxetine administration during adolescence attenuates cognitive and synaptic deficits in adult 3×TgAD mice. Neuropharmacology 2017, 126, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, Y.; Xu, H.; Zhu, S.; Wang, H.; He, J.; Zhang, H.; Guo, H.; Kong, J.; Huang, Q.; et al. Fluoxetine Improves Behavioral Performance by Suppressing the Production of Soluble β-Amyloid in APP/PS1 Mice. Curr. Alzheimer Res. 2014, 11, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Wang, J.; Wang, H.; Zhang, Y.; Zhu, S.; Adilijiang, A.; Guo, H.; Zhang, R.; Guo, W.; Luo, G.; et al. Regulation of astrocyte pathology by fluoxetine prevents the deterioration of Alzheimer phenotypes in an APP/PS1 mouse model. Glia 2016, 64, 240–254. [Google Scholar] [CrossRef]
- Caraci, F.; Tascedda, F.; Merlo, S.; Benatti, C.; Spampinato, S.F.; Munafò, A.; Leggio, G.M.; Nicoletti, F.; Brunello, N.; Drago, F.; et al. Fluoxetine Prevents Aβ1-42-Induced Toxicity via a Paracrine Signaling Mediated by Transforming-Growth-Factor-β1. Front. Pharmacol. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.-J.; Ren, Q.-G.; Gong, W.-G.; Wu, D.; Tang, X.; Li, X.-L.; Wu, F.-F.; Bai, F.; Xu, L.; Zhang, Z.-J. Escitalopram attenuates β-amyloid-induced tau hyperphosphorylation in primary hippocampal neurons through the 5-HT1A receptor mediated Akt/GSK-3β pathway. Oncotarget 2016, 7, 13328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, R.L.; Guo, Z.; Halagappa, V.M.; Pearson, M.; Gray, A.J.; Matsuoka, Y.; Brown, M.; Clark, R.F.; Mattson, M.P. Prophylactic Treatment with Paroxetine Ameliorates Behavioral Deficits and Retards the Development of Amyloid and Tau Pathologies in 3xTgAD Mice. Exp. Neurol. 2007, 205, 166. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.S.; Fu, Y.; Dobson-Stone, C.; Hsiao, J.-H.T.; Shang, K.; Hallupp, M.; Schofield, P.R.; Garner, B.; Karl, T.; Kwok, J.B.J. Effect of Fluvoxamine on Amyloid-β Peptide Generation and Memory. J. Alzheimer’s Dis. 2018, 62, 1777–1787. [Google Scholar] [CrossRef] [PubMed]
- Tin, G.; Mohamed, T.; Shakeri, A.; Pham, A.T.; Rao, P.P.N. Interactions of Selective Serotonin Reuptake Inhibitors with β-Amyloid. ACS Chem. Neurosci. 2019, 10, 226–234. [Google Scholar] [CrossRef]
- La, A.L.; Walsh, C.M.; Neylan, T.C.; Vossel, K.A.; Yaffe, K.; Krystal, A.D.; Miller, B.L.; Karageorgiou, E. Long-Term Trazodone Use and Cognition: A Potential Therapeutic Role for Slow-Wave Sleep Enhancers. J. Alzheimer’s Dis. 2019, 67, 911–921. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, Q.; Hu, T.; Wang, Y.; Zhao, J.; Lu, J.; Pei, G. A tricyclic antidepressant, amoxapine, reduces amyloid-β generation through multiple serotonin receptor 6-mediated targets. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tran, N.Q.V.; Nguyen, A.N.; Takabe, K.; Yamagata, Z.; Miyake, K. Pre-treatment with amitriptyline causes epigenetic up-regulation of neuroprotection-associated genes and has anti-apoptotic effects in mouse neuronal cells. Neurotoxicol. Teratol. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Wang, D.-D.; Li, J.; Yu, L.-P.; Wu, M.-N.; Sun, L.-N.; Qi, J.-S. Desipramine improves depression-like behavior and working memory by up-regulating p-CREB in Alzheimer’s disease associated mice. J. Integr. Neurosci. 2016, 15, 247–260. [Google Scholar] [CrossRef]
- Chavant, F.; Deguil, J.; Pain, S.; Ingrand, I.; Milin, S.; Fauconneau, B.; Pérault-Pochat, M.-C.; Lafay-Chebassier, C. Imipramine, in Part through Tumor Necrosis Factor α Inhibition, Prevents Cognitive Decline and β-Amyloid Accumulation in a Mouse Model of Alzheimer’s Disease. J. Pharmacol. Exp. Ther. 2010, 332, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, Y.; Wang, Y.; Yuan, L.; Luo, Z. Moclobemide up-regulates proliferation of hippocampal progenitor cells in chronically stressed mice. Acta Pharmacol. Sin. 2016, 25, 1408412. [Google Scholar]
- Caraci, F.; Pappalardo, G.; Basile, L.; Giuffrida, A.; Copani, A.; Tosto, R.; Sinopoli, A.; Giuffrida, M.L.; Pirrone, E.; Drago, F.; et al. Neuroprotective effects of the monoamine oxidase inhibitor tranylcypromine and its amide derivatives against Aβ(1–42)-induced toxicity. Eur. J. Pharmacol. 2015, 764, 256–263. [Google Scholar] [CrossRef]
- Li, N.; Lee, B.; Liu, R.-J.; Banasr, M.; Dwyer, J.M.; Iwata, M.; Li, X.-Y.; Aghajanian, G.; Duman, R.S. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science 2010, 329, 959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeffer, C.A.; Klann, E. mTOR signaling: At the crossroads of plasticity, memory and disease. Trends Neurosci. 2010, 33, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, A.; Wadhwa, R. Selective Serotonin Reuptake Inhibitors; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Moraczewski, J.; Aedma, K.K. Tricyclic Antidepressants; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Laban, T.S.; Saadabadi, A. Monoamine Oxidase Inhibitors (MAOI); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Shin, J.J.; Saadabadi, A. Trazodone; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rosenbaum, S.B.; Gupta, V.; Palacios, J.L. Ketamine; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Alam, A.; Voronovich, Z.; Carley, J.A. A Review of Therapeutic Uses of Mirtazapine in Psychiatric and Medical Conditions. Prim. Care Companion CNS Disord. 2013, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jilani, T.N.; Gibbons, J.R.; Faizy, R.M.; Saadabadi, A. Mirtazapine; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Watanabe, N.; Omori, I.M.; Nakagawa, A.; Cipriani, A.; Barbui, C.; Churchill, R.; Furukawa, T.A. Mirtazapine versus other antidepressive agents for depression. Cochrane Database Syst. Rev. 2011, 12. [Google Scholar] [CrossRef] [Green Version]
- Matthews, M.; Basil, B.; Evcimen, H.; Adetunji, B.; Joseph, S. Mirtazapine-Induced Nightmares. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 311. [Google Scholar] [CrossRef]
- Barkin, R.L.; Schwer, W.A.; Barkin, S.J. Recognition and Management of Depression in Primary Care. Am. J. Ther. 2000, 7, 205–228. [Google Scholar] [CrossRef]
- Kessler, D.; Burns, A.; Tallon, D.; Lewis, G.; MacNeill, S.; Round, J.; Hollingworth, W.; Chew-Graham, C.; Anderson, I.; Campbell, J.; et al. Introduction; NIHR Journals Library: Southampton, UK, 2018. [Google Scholar]
- Blier, P.; Gobbi, G.; Turcotte, J.E.; de Montigny, C.; Boucher, N.; Hébert, C.; Debonnel, G. Mirtazapine and paroxetine in major depression: A comparison of monotherapy versus their combination from treatment initiation. Eur. Neuropsychopharmacol. 2009, 19, 457–465. [Google Scholar] [CrossRef]
- Blier, P.; Ward, H.E.; Tremblay, P.; Laberge, L.; Hébert, C.; Bergeron, R. Combination of Antidepressant Medications From Treatment Initiation for Major Depressive Disorder: A Double-Blind Randomized Study. Am. J. Psychiatry 2010, 167, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Behnke, K.; Søgaard, J.; Martin, S.; Bäuml, J.; Ravindran, A.V.; Ågren, H.; Vester-Blokland, E.D. Mirtazapine orally disintegrating tablet versus sertraline: A prospective onset of action study. J. Clin. Psychopharmacol. 2003, 23, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Remeron, Remeron SolTab (Mirtazapine) Dosing, Indications, Interactions, Adverse Effects, and More. Available online: https://reference.medscape.com/drug/remeron-soltab-mirtazapine-342966#4 (accessed on 6 August 2021).
- Thase, M.E.; Nierenberg, A.A.; Vrijland, P.; Van Oers, H.J.J.; Schutte, A.J.; Simmons, J.H. Remission with mirtazapine and selective serotonin reuptake inhibitors: A meta-analysis of individual patient data from 15 controlled trials of acute phase treatment of major depression. Int. Clin. Psychopharmacol. 2010, 25, 189–198. [Google Scholar] [CrossRef]
- Wang, S.-M.; Han, C.; Bahk, W.-M.; Lee, S.-J.; Patkar, A.A.; Masand, P.S.; Pae, C.-U. Addressing the Side Effects of Contemporary Antidepressant Drugs: A Comprehensive Review. Chonnam Med. J. 2018, 54, 101. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, T.A.; Cipriani, A.; Cowen, P.J.; Leucht, S.; Egger, M.; Salanti, G. Optimal dose of selective serotonin reuptake inhibitors, venlafaxine, and mirtazapine in major depression: A systematic review and dose-response meta-analysis. Lancet Psychiatry 2019, 6, 601–609. [Google Scholar] [CrossRef] [Green Version]
- Winokur, A.; Sateia, M.J.; Hayes, J.B.; Bayles-Dazet, W.; MacDonald, M.M.; Gary, K.A. Acute effects of mirtazapine on sleep continuity and sleep architecture in depressed patients: A pilot study. Biol. Psychiatry 2000, 48, 75–78. [Google Scholar] [CrossRef]
- Boshuisen, M.L.; Slaap, B.R.; Vester-Blokland, E.D.; den Boer, J.A. The effect of mirtazapine in panic disorder: An open label pilot study with a single-blind placebo run-in period. Int. Clin. Psychopharmacol. 2001, 16, 363–368. [Google Scholar] [CrossRef]
- Anxiety Disorders Treatment & Management: Approach Considerations, Pharmacotherapy for Anxiety and Panic Disorders, Psychotherapy for Anxiety and Panic Disorders. Available online: https://emedicine.medscape.com/article/286227-treatment#d8 (accessed on 21 July 2021).
- Bahk, W.-M.; Pae, C.-U.; Tsoh, J.; Chae, J.-H.; Jun, T.-Y.; Kim, K.-S. Effects of mirtazapine in patients with post-traumatic stress disorder in Korea: A pilot study. Hum. Psychopharmacol. Clin. Exp. 2002, 17, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Alderman, C.P.; Condon, J.T.; Gilbert, A.L. An Open-Label Study of Mirtazapine as Treatment for Combat-Related PTSD. Ann. Pharmacother. 2009, 43, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Koran, L.M.; Gamel, N.N.; Choung, H.W.; Smith, E.H.; Aboujaoude, E.N. Mirtazapine for Obsessive-Compulsive Disorder: An Open Trial Followed by Double-Blind Discontinuation. J. Clin. Psychiatry 2005, 66, 515–520. [Google Scholar] [CrossRef]
- Pallanti, S.; Quercioli, L.; Bruscoli, M. Response Acceleration With Mirtazapine Augmentation of Citalopram in Obsessive-Compulsive Disorder Patients Without Comorbid Depression. J. Clin. Psychiatry 2004, 65, 1394–1399. [Google Scholar] [CrossRef]
- Kim, J.E.; Yoon, S.J.; Kim, J.; Jung, J.Y.; Jeong, H.S.; Cho, H.B.; Shin, E.; Lyoo, I.K.; Kim, T.S. Efficacy and tolerability of mirtazapine in treating major depressive disorder with anxiety symptoms: An 8-week open-label randomised paroxetine-controlled trial. Int. J. Clin. Pract. 2011, 65, 323–329. [Google Scholar] [CrossRef]
- Rifkin-Zybutz, R.; MacNeill, S.; Davies, S.J.; Dickens, C.; Campbell, J.; Anderson, I.M.; Chew-Graham, C.A.; Peters, T.J.; Lewis, G.; Wiles, N.; et al. Does anxiety moderate the effectiveness of mirtazapine in patients with treatment-resistant depression? A secondary analysis of the MIR trial. J. Psychopharmacol. 2020, 34, 1342–1349. [Google Scholar] [CrossRef]
- Schutters, S.I.J.; Van Megen, H.J.G.M.; Van Veen, J.F.; Denys, D.A.J.P.; Westenberg, H.G.M. Mirtazapine in generalized social anxiety disorder: A randomized, double-blind, placebo-controlled study. Int. Clin. Psychopharmacol. 2010, 25, 302–304. [Google Scholar] [CrossRef]
- Lévy, E.; Margolese, H.C. Migraine headache prophylaxis and treatment with low-dose mirtazapine. Int. Clin. Psychopharmacol. 2003, 18, 301–303. [Google Scholar] [CrossRef]
- Mirtazapine: A Medicine to Treat Depression, Obsessive Compulsive Disorder and Anxiety Disorders—NHS. Available online: https://www.nhs.uk/medicines/mirtazapine/ (accessed on 21 July 2021).
- Al-Majed, A.; Bakheit, A.H.; Alharbi, R.M.; Abdel Aziz, H.A. Mirtazapine. Profiles Drug Subst. Excip. Relat. Methodol. 2018, 43, 209–254. [Google Scholar] [CrossRef]
- Bengtsson, H.J.; Kele, J.; Johansson, J.; Hjorth, S. Interaction of the antidepressant mirtazapine with α2-adrenoceptors modulating the release of 5-HT in different rat brain regions in vivo. Naunyn. Schmiedebergs. Arch. Pharmacol. 2000, 362, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Ito, C.; Tashiro, M.; Hiraoka, K.; Shibuya, K.; Funaki, Y.; Iwata, R.; Matsuoka, H.; Yanai, K. Histamine H1 receptor occupancy by the new-generation antidepressants fluvoxamine and mirtazapine: A positron emission tomography study in healthy volunteers. Psychopharmacology 2013, 230, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.A.; Wichniak, A.; Uhr, M.; Ising, M.; Brunner, H.; Held, K.; Weikel, J.C.; Sonntag, A.; Steiger, A. Changes of Sleep Architecture, Spectral Composition of Sleep EEG, the Nocturnal Secretion of Cortisol, ACTH, GH, Prolactin, Melatonin, Ghrelin, and Leptin, and the DEX-CRH Test in Depressed Patients during Treatment with Mirtazapine. Neuropsychopharmacology 2006, 31, 832–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmer, C.J.; Ad Sitsen, J.M.; Delbressine, L.P. Clinical Pharmacokinetics of Mirtazapine. Clin. Pharmacokinet. 2000, 38, 461–474. [Google Scholar] [CrossRef]
- Wang, F.; Feng, T.-Y.; Yang, S.; Preter, M.; Zhou, J.-N.; Wang, X.-P. Drug Therapy for Behavioral and Psychological Symptoms of Dementia. Curr. Neuropharmacol. 2016, 14, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Raji, M.A.; Brady, S.R. Mirtazapine for Treatment of Depression and Comorbidities in Alzheimer Disease. Ann. Pharmacother. 2001, 35, 1024–1027. [Google Scholar] [CrossRef]
- Cakir, S. The efficacy of mirtazapine in agitated patients with Alzheimer’s disease: A 12-week open-label pilot study. Neuropsychiatr. Dis. Treat. 2008, 4, 963. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, S.; Hellier, J.; Dewey, M.; Romeo, R.; Ballard, C.; Baldwin, R.; Bentham, P.; Fox, C.; Holmes, C.; Katona, C.; et al. Sertraline or mirtazapine for depression in dementia (HTA-SADD): A randomised, multicentre, double-blind, placebo-controlled trial. Lancet 2011, 378, 403–411. [Google Scholar] [CrossRef]
- Zuidersma, M.; Chua, K.C.; Hellier, J.; Voshaar, R.O.; Banerjee, S. Sertraline and Mirtazapine Versus Placebo in Subgroups of Depression in Dementia: Findings From the HTA-SADD Randomized Controlled Trial. Am. J. Geriatr. Psychiatry 2019, 27, 920–931. [Google Scholar] [CrossRef]
- Scoralick, F.M.; Louzada, L.L.; Quintas, J.L.; Naves, J.O.S.; Camargos, E.F.; Nóbrega, O.T. Mirtazapine does not improve sleep disorders in Alzheimer’s disease: Results from a double-blind, placebo-controlled pilot study. Psychogeriatrics 2017, 17, 89–96. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, H.; Huang, J.; Huang, S.; Bai, Y.; Li, Y.; Huang, W. Efficacy of antidepressant drugs in the treatment of depression in Alzheimer disease patients: A systematic review and network meta-analysis. J. Psychopharmacol. 2021. [Google Scholar] [CrossRef]
- Fabbretti, E.; Antognolli, G.; Tongiorgi, E. Amyloid-β Impairs Dendritic Trafficking of Golgi-Like Organelles in the Early Phase Preceding Neurite Atrophy: Rescue by Mirtazapine. Front. Mol. Neurosci. 2021, 14, 100. [Google Scholar] [CrossRef]
- Yiannopoulou, K.G.; Papageorgiou, S.G. Current and Future Treatments in Alzheimer Disease: An Update. J. Cent. Nerv. Syst. Dis. 2020, 12, 117957352090739. [Google Scholar] [CrossRef] [Green Version]
- Drug Interactions Checker—Medscape Drug Reference Database. Available online: https://reference.medscape.com/drug-interactionchecker (accessed on 1 September 2021).
- Miziak, B.; Błaszczyk, B.; Czuczwar, S.J. Some Candidate Drugs for Pharmacotherapy of Alzheimer’s Disease. Pharmaceuticals 2021, 14, 458. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Tong, G.; Ballard, C. Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J. Alzheimer’s Dis. 2019, 67, 779–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Drug | Drug Class | General Mechanism of Action | Examples of Evidence in AD |
|---|---|---|---|
| Fluoxetine Citalopram Escitalopram Paroxetine Fluvoxamine Sertraline | Selective serotonin reuptake inhibitors | This class of drugs inhibits the serotonin transporter (SERT) at the neurons, thereby enhancing the concentration of 5-HT in the synaptic cleft [77] | Increase in the hippocampus size, reduction of the amount of soluble Aβ peptide, improvements in memory, cognition, behavior, life quality, reduction of tau hyperphosphorylation, modulation of neuroinflammation |
| Desipramine Imipramine Amoxapine Amitriptyline | Tricyclic antidepressants | This class of drugs inhibits the serotonin transporter (SERT) and norepinephrine transporter (NET), enhancing the concentration of serotonin and norepinephrine in the synaptic cleft. Additionally, they are antagonists of α1 and α2, muscarinic, and H1 receptors [78] | Reduction in the production and accumulation of Aβ peptide, reduction in neuronal death and neuroinflammation, improvement in cognitive function, neuroprotection, cognition, and memory |
| Moclobemide Tranylcypromine | Monoamine oxidase inhibitors | This class of drugs inhibits monoamine oxidase enzyme, an enzyme responsible for the breakdown of several neurotransmitters such as 5-HT, NE and dopamine [79] | Increase in the proliferation of hippocampal progenitor cells, BDNF levels and reduction of neuronal death |
| Trazodone | Atypical antidepressant: serotonin-antagonist-and-reuptake-inhibitor [80] | This drug inhibits SERT and 5-HT2 receptors [80] | Delay of cognitive decline, improvement of insomnia |
| Ketamine | NMDA receptor antagonist | This drug acts mainly by antagonizing NMDA and glutamate receptors [81] | Behavioral improvement |
| Indication | Description |
|---|---|
| Insomnia | Decreases REM sleep, improves the quality of sleep and sleep continuity [95] |
| Panic disorder | Decreases agitation and panic attacks; Can be a fast and effective alternative to SSRIs [96,97] |
| Post-traumatic stress disorder (PTSD) | Effective and well-tolerated [98]; Effective in PTSD related to combat [99] |
| Obsessive-compulsive disorder (OCD) | Effective with continuous treatment [100]; Fast action, more effective and fewer side effects when added to citalopram [101] |
| Anxiety disorders | Effective and earlier-onset action (vs. paroxetine) [102]; Effective in reducing generalized anxiety [103]; Lack of efficiency in social anxiety disorder (vs. placebo) [104] |
| Migraine | Prevents migraine initiation and treats this condition [105]; However, side effects of mirtazapine’s use include headaches [106]. Thus, there is a lack of consistent evidence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia, A.S.; Vale, N. Antidepressants in Alzheimer’s Disease: A Focus on the Role of Mirtazapine. Pharmaceuticals 2021, 14, 930. https://doi.org/10.3390/ph14090930
Correia AS, Vale N. Antidepressants in Alzheimer’s Disease: A Focus on the Role of Mirtazapine. Pharmaceuticals. 2021; 14(9):930. https://doi.org/10.3390/ph14090930
Chicago/Turabian StyleCorreia, Ana Salomé, and Nuno Vale. 2021. "Antidepressants in Alzheimer’s Disease: A Focus on the Role of Mirtazapine" Pharmaceuticals 14, no. 9: 930. https://doi.org/10.3390/ph14090930
APA StyleCorreia, A. S., & Vale, N. (2021). Antidepressants in Alzheimer’s Disease: A Focus on the Role of Mirtazapine. Pharmaceuticals, 14(9), 930. https://doi.org/10.3390/ph14090930