
Association between Proton Pump Inhibitor Use and Parkinson’s Disease in a Korean Population



Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ethics
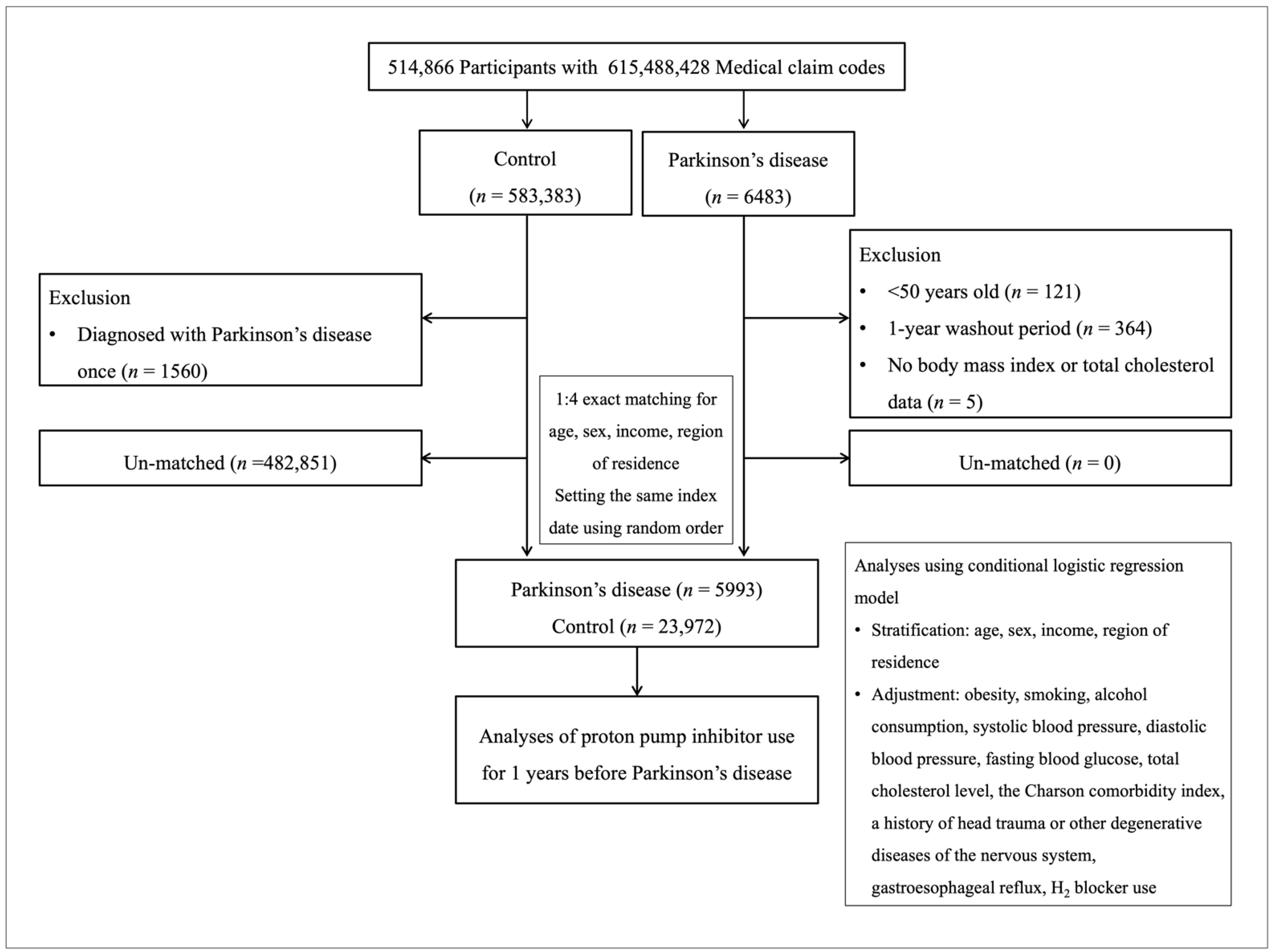
4.2. Study Population
4.3. Proton Pump Inhibitors (Exposure)
4.4. Parkinson’s Disease (Outcome)
4.5. Participant Selection
4.6. Covariates
4.7. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wirdefeldt, K.; Adami, H.-O.; Cole, P.; Trichopoulos, D.; Mandel, J. Epidemiology and etiology of parkinson’s disease: A review of the evidence. Eur. J. Epidemiol. 2011, 26, S1–S58. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Nehra, A.K.; Alexander, J.A.; Loftus, C.G.; Nehra, V. Proton pump inhibitors: Review of emerging concerns. Mayo Clinic Proc. 2018, 93, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, A.J.; Grady, D. Adverse effects associated with proton pump inhibitors. JAMA Intern. Med. 2016, 176, 172–174. [Google Scholar] [CrossRef]
- Lai, S.-W.; Liao, K.-F.; Lin, C.-L.; Lin, C.-H. Association between parkinson’s disease and proton pump inhibitors therapy in older people. Biomedicine 2020, 10, 1–4. [Google Scholar]
- Nielsen, H.H.; Qiu, J.; Friis, S.; Wermuth, L.; Ritz, B. Treatment for helicobacter pylori infection and risk of parkinson’s disease in denmark. Eur. J. Neurol. 2012, 19, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Guerrero, G.; Amador-Muñoz, D.; Calderón-Ospina, C.A.; López-Fuentes, D.; Nava Mesa, M.O. Proton pump inhibitors and dementia: Physiopathological mechanisms and clinical consequences. Neural Plast. 2018, 2018, 5257285. [Google Scholar] [CrossRef] [Green Version]
- Colacurcio, D.J.; Nixon, R.A. Disorders of lysosomal acidification—The emerging role of v-ATPase in aging and neurodegenerative disease. Ageing Res. Rev. 2016, 32, 75–88. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.L.; Bohnen, N.I. Cholinergic dysfunction in parkinson’s disease. Curr. Neurol. Neurosci. Rep. 2013, 13, 377. [Google Scholar] [CrossRef] [Green Version]
- Tata, A.M.; Velluto, L.; D’Angelo, C.; Reale, M. Cholinergic system dysfunction and neurodegenerative diseases: Cause or effect? CNS Neurol. Disord. Drug Targets 2014, 13, 1294–1303. [Google Scholar] [CrossRef]
- Kumar, R.; Kumar, A.; Nordberg, A.; Långström, B.; Darreh-Shori, T. Proton pump inhibitors act with unprecedented potencies as inhibitors of the acetylcholine biosynthesizing enzyme—A plausible missing link for their association with incidence of dementia. Alzheimer’s Dement. 2020, 16, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Ishimura, N.; Ishihara, S. Advantages and disadvantages of long-term proton pump inhibitor use. J. Neurogastroenterol. Motil. 2018, 24, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Main, B.S.; Minter, M.R. Microbial immuno-communication in neurodegenerative diseases. Front. Neurosci. 2017, 11, 151. [Google Scholar] [CrossRef] [PubMed]
- Tremlett, H.; Bauer, K.C.; Appel-Cresswell, S.; Finlay, B.B.; Waubant, E. The gut microbiome in human neurological disease: A review. Ann. Neurol. 2017, 81, 369–382. [Google Scholar] [CrossRef]
- Blacher, E.; Bashiardes, S.; Shapiro, H.; Rothschild, D.; Mor, U.; Dori-Bachash, M.; Kleimeyer, C.; Moresi, C.; Harnik, Y.; Zur, M. Potential roles of gut microbiome and metabolites in modulating als in mice. Nature 2019, 572, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, X.; Yang, S.; Meng, F.; Wang, X.; Wei, H.; Chen, T. Evaluation of the microbial diversity in amyotrophic lateral sclerosis using high-throughput sequencing. Front. Microbiol. 2016, 7, 1479. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.; Hiergeist, A.; Adis, C.; Mayer, B.; Gessner, A.; Ludolph, A.C.; Weishaupt, J.H. The fecal microbiome of als patients. Neurobiol. Aging 2018, 61, 132–137. [Google Scholar] [CrossRef]
- Hill-Burns, E.M.; Debelius, J.W.; Morton, J.T.; Wissemann, W.T.; Lewis, M.R.; Wallen, Z.D.; Peddada, S.D.; Factor, S.A.; Molho, E.; Zabetian, C.P. Parkinson’s disease and parkinson’s disease medications have distinct signatures of the gut microbiome. Mov. Disord. 2017, 32, 739–749. [Google Scholar] [CrossRef]
- Unger, M.M.; Spiegel, J.; Dillmann, K.-U.; Grundmann, D.; Philippeit, H.; Bürmann, J.; Faßbender, K.; Schwiertz, A.; Schäfer, K.-H. Short chain fatty acids and gut microbiota differ between patients with parkinson’s disease and age-matched controls. Parkinsonism. Relat. Disord. 2016, 32, 66–72. [Google Scholar] [CrossRef]
- Vink, R.; Nechifor, M. Magnesium in the Central Nervous System; University of Adelaide Press: Adelaide, Australia, 2011. [Google Scholar]
- Makunts, T.; Abagyan, R. How can proton pump inhibitors damage central and peripheral nervous systems? Neural Regen. Res. 2020, 15, 2041–2042. [Google Scholar]
- Shindo, Y.; Yamanaka, R.; Suzuki, K.; Hotta, K.; Oka, K. Intracellular magnesium level determines cell viability in the mpp+ model of parkinson’s disease. Biochim. Biophys. Acta 2015, 1853, 3182–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Huang, X.; Zhang, L.; Han, F.; Pang, K.L.; Li, X.; Shen, J.Y. Magnesium boosts the memory restorative effect of environmental enrichment in alzheimer’s disease mice. CNS Neurosci. 2018, 24, 70–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, K.M.; Fitzpatrick, P.F. Mechanisms of tryptophan and tyrosine hydroxylase. IUBMB Life 2013, 65, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, C.; Erikson, K.; Piñero, D.J.; Beard, J.L. In vivo dopamine metabolism is altered in iron-deficient anemic rats. J. Ntur. 1997, 127, 2282–2288. [Google Scholar] [CrossRef] [Green Version]
- Sanjida, A.; Rajib, H.; Mohammad, S.; Nahia, A.; Glam, A.; Mohiuddin, A.B. Cognitive impact after short-term exposure to different proton pump inhibitors: Assessment using CANTAB software. Alzheimer’s Res. 2015, 7, 79. [Google Scholar]
- Giovanni, P.; Paola, C.; Adele, G.; Salvatore, G.; Edoardo, S.; Achille, P.C. Rabepraole and psychiatric symptoms. Ann. Pharm. 2007, 41, 1315–1317. [Google Scholar]
- Abela, M.; Aquilina, N.; Attard, A. Omeprazole-induced delirium. Synapse 2014, 13, 18–19. [Google Scholar]
- Heckmann, J.G.; Birklein, F.; Neundorfer, B. Omeprazole-induced delirium. J. Neurol. 2000, 247, 56–57. [Google Scholar] [CrossRef]
- Kanazawa, H.; Okada, A.; Matsushima, Y.; Yokota, H.; Okubo, S.; Mashige, F.; Nakahara, K. Determination of omeprazole and its metabolites in human plasma by liquid chromatography–mass spectrometry. J. Chromatogr. 2002, 949, 1–9. [Google Scholar] [CrossRef]
- Nakagawa, S.; Arai, Y.; Kishida, T.; Hiraoka, N.; Tsuchida, S.; Inoue, H.; Sakai, R.; Mazda, O.; Kubo, T. Lansoprazole inhibits nitric oxide and prostaglandin e 2 production in murine macrophage raw 264.7 cells. Inflammation 2012, 35, 1062–1068. [Google Scholar] [CrossRef]
- Handa, O.; Yoshida, N.; Fujita, N.; Tanaka, Y.; Ueda, M.; Takagi, T.; Kokura, S.; Naito, Y.; Okanoue, T.; Yoshikawa, T. Molecular mechanisms involved in anti-inflammatory effects of proton pump inhibitors. Inflamm. Res. 2006, 55, 476–480. [Google Scholar] [CrossRef]
- Suzuki, M.; Mori, M.; Miura, S.; Suematsu, M.; Fukumura, D.; Kimura, H.; Ishii, H. Omeprazole attenuates oxygen-derived free radical production from human neutrophils. Free Radic. Biol. Med. 1996, 21, 727–731. [Google Scholar] [CrossRef]
- Hashioka, S.; Klegeris, A.; Mcgeer, P.L. Proton pump inhibitors reduce interferon-γ-induced neurotoxicity and stat3 phosphorylation of human astrocytes. Glia 2011, 59, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Oskar, O.H.; Anton, P.; Einar, S.B.; Sigrun, H.L.; Margret, H.O.; Eirikur, S.; Helga, M.O.; Helga, Z. Proton-pump inhibitors among adults: A nationwide drug-utilization study. Ther. Adv. Gastroenterol. 2018, 11, 1756284818777943. [Google Scholar]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco smoking and alcohol consumption are related to benign parotid tumor: A nested case-control study using a national health screening cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional association between gerd and asthma: Two longitudinal follow-up studies using a national sample cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e9. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total Participants | |||
|---|---|---|---|---|
| Parkinson’s Disease | Control | Standardized Difference | ||
| Total number (n, %) | 5993 (100.0) | 23,972 (100.0) | ||
| Age (years old) (n, %) | 0.00 | |||
| 50–54 | 234 (3.9) | 936 (3.9) | ||
| 55–59 | 361 (6.0) | 1444 (6.0) | ||
| 60–64 | 654 (10.9) | 2616 (10.9) | ||
| 65–69 | 1014 (16.9) | 4056 (16.9) | ||
| 70–74 | 1431 (23.9) | 5724 (23.9) | ||
| 75–79 | 1396 (23.3) | 5584 (23.3) | ||
| 80–84 | 721 (12.0) | 2884 (12.0) | ||
| 85+ | 182 (3.0) | 728 (3.0) | ||
| Sex (n, %) | 0.00 | |||
| Male | 2800 (46.7) | 11,200 (46.7) | ||
| Female | 3193 (53.3) | 12,772 (53.3) | ||
| Income (n, %) | 0.00 | |||
| 1 (lowest) | 1138 (19.0) | 4552 (19.0) | ||
| 2 | 665 (11.1) | 2660 (11.1) | ||
| 3 | 814 (13.6) | 3256 (13.6) | ||
| 4 | 1135 (18.9) | 4540 (18.9) | ||
| 5 (highest) | 2241 (37.4) | 8964 (37.4) | ||
| Region of residence (n, %) | 0.00 | |||
| Urban | 2224 (37.1) | 8896 (37.1) | ||
| Rural | 3769 (62.9) | 15,076 (62.9) | ||
| Obesity (n, %) a | 0.02 | |||
| Underweight | 251 (4.2) | 932 (3.9) | ||
| Normal | 2141 (35.7) | 8664 (36.1) | ||
| Overweight | 1564 (26.1) | 6255 (26.1) | ||
| Obese I | 1847 (30.8) | 7420 (31.0) | ||
| Obese II | 190 (3.2) | 701 (2.9) | ||
| Smoking status (n, %) | 0.09 | |||
| Nonsmokers | 4733 (79.0) | 18,103 (75.5) | ||
| Past smokers | 659 (11.0) | 2810 (11.7) | ||
| Current smokers | 601 (10.0) | 3059 (12.8) | ||
| Alcohol consumption (n, %) | 0.12 | |||
| <1 time a week | 4680 (78.1) | 17,436 (72.7) | ||
| ≥1 time a week | 1313 (21.9) | 6536 (27.3) | ||
| Systolic blood pressure (n, %) | 0.02 | |||
| <120 mmHg | 1351 (22.5) | 5487 (22.9) | ||
| 120–139 mmHg | 2839 (47.4) | 11,528 (48.1) | ||
| ≥140 mmHg | 1803 (30.1) | 6957 (29.0) | ||
| Diastolic blood pressure (n, %) | 0.02 | |||
| <80 mmHg | 2616 (43.7) | 10,668 (44.5) | ||
| 80–89 mmHg | 2163 (36.1) | 8609 (35.9) | ||
| ≥90 mmHg | 1214 (20.3) | 4695 (19.6) | ||
| Fasting blood glucose (n, %) | 0.12 | |||
| <100 mg/dL | 3235 (54.0) | 14,165 (59.1) | ||
| 100–125 mg/dL | 1897 (31.7) | 7166 (29.9) | ||
| ≥126 mg/dL | 861 (14.4) | 2641 (11.0) | ||
| Total cholesterol level (n, %) | 0.04 | |||
| <200 mg/dL | 3369 (56.2) | 13,078 (54.6) | ||
| 200–239 mg/dL | 1777 (29.7) | 7573 (31.6) | ||
| ≥240 mg/dL | 847 (14.1) | 3321 (13.9) | ||
| Charlson comorbidity index (n, %) | 0.35 | |||
| 0 | 2376 (39.6) | 13,554 (56.5) | ||
| 1 | 1369 (22.8) | 4391 (18.3) | ||
| ≥2 | 2248 (37.5) | 6027 (25.1) | ||
| A history of head trauma (n, %) | 0.2 | |||
| Yes | 477 (8.0) | 817 (3.4) | ||
| No | 5516 (92.0) | 23,155 (96.6) | ||
| A history of other degenerative diseases of the nervous system (n, %) | 0.26 | |||
| Yes | 476 (7.9) | 556 (2.3) | ||
| No | 5517 (92.1) | 23,416 (97.7) | ||
| Gastroesophageal reflux disease (n, %) | 0.13 | |||
| Yes | 1247 (20.8) | 3823 (15.9) | ||
| No | 4746 (79.2) | 20,149 (84.1) | ||
| Duration of H2 blocker use (mean, standard deviation) | 68.67 (103.84) | 39.92 (78.38) | 0.31 | |
| PPI exposure (n, %) | 0.17 | |||
| Current users | 467 (7.8) | 1010 (4.2) | ||
| Past users | 562 (9.4) | 1817 (7.6) | ||
| Duration of PPI use (n, %) | 0.18 | |||
| <30 days | 578 (9.6) | 2080 (8.7) | ||
| 30 to 90 days | 428 (7.1) | 1228 (5.1) | ||
| ≥90 days | 409 (6.8) | 867 (3.6) | ||
| Duration of PPI use (first-generation PPIs) (n, %) | 0.17 | |||
| <30 days | 447 (7.5) | 1323 (5.5) | ||
| 30 to 90 days | 312 (5.2) | 777 (3.2) | ||
| ≥90 days | 233 (3.9) | 499 (2.1) | ||
| Duration of PPI use (second-generation PPIs) (n, %) | 0.1 | |||
| <30 days | 281 (4.7) | 982 (4.1) | ||
| 30 to 90 days | 179 (3.0) | 518 (2.2) | ||
| ≥90 days | 147 (2.5) | 336 (1.4) | ||
| Characteristics | n of PD | n of Controls | Odds Ratio for PD (95% Confidence Interval) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (Exposure/ Total, %) | (Exposure/ Total, %) | Crude b | p -Value | Model 2 b,c | p -Value | Model 3 b,c,d | p -Value | ||
| PPI exposure | |||||||||
| Current users | 467/5993 (7.8%) | 1010/23,972 (4.2%) | 1.98 (1.76–2.22) | <0.001 a | 1.96 (1.74–2.20) | <0.001 a | 1.63 (1.44–1.84) | <0.001 a | |
| Past users | 562/5993 (9.4%) | 1817/23,972 (7.6%) | 1.32 (1.20–1.46) | <0.001 a | 1.31 (1.18–1.45) | <0.001 a | 1.12 (1.01–1.25) | 0.035 a | |
| Duration of PPI use | |||||||||
| <30 days | 578/5993 (9.6%) | 2080/23,972 (8.7%) | 1.20 (1.09–1.33) | 0.002 a | 1.22 (1.11–1.35) | <0.001 a | 1.10 (0.99–1.22) | 0.0724 | |
| 30–90 days | 428/5993 (7.1%) | 1228/23,972 (5.1%) | 1.51 (1.35–1.69) | <0.001 a | 1.47 (1.31–1.66) | <0.001 a | 1.26 (1.12–1.43) | <0.001 a | |
| ≥90 days | 409/5993 (6.8%) | 867/23,972 (3.6%) | 2.05 (1.81–2.32) | <0.001 a | 2.01 (1.78–2.28) | <0.001 a | 1.64 (1.43–1.89) | <0.001 a | |
| Duration of PPI use (first-generation PPIs) | |||||||||
| <30 days | 447/5993 (7.5%) | 1323/23,972 (5.5%) | 1.45 (1.29–1.62) | <0.001 a | 1.43 (1.28–1.61) | <0.001 a | 1.27 (1.13–1.43) | <0.001 a | |
| 30–90 days | 312/5993 (5.2%) | 777/23,972 (3.2%) | 1.72 (1.50–1.97) | <0.001 a | 1.64 (1.43–1.88) | <0.001 a | 1.41 (1.22–1.63) | <0.001 a | |
| ≥90 days | 233/5993 (3.9%) | 499/23,972 (2.1%) | 2.00 (1.71–2.34) | <0.001 a | 1.89 (1.61–2.23) | <0.001 a | 1.52 (1.27–1.80) | <0.001 a | |
| Duration of PPI use (second-generation PPIs) | |||||||||
| <30 days | 281/5993 (4.7%) | 982/23,972 (4.1%) | 1.18 (1.03–1.35) | 0.018 a | 1.22 (1.06–1.40) | 0.005 a | 1.07 (0.93–1.24) | 0.342 | |
| 30–90 days | 179/5993 (3.0%) | 518/23,972 (2.2%) | 1.42 (1.20–1.69) | <0.001 a | 1.45 (1.21–1.73) | <0.001 a | 1.14 (0.95–1.37) | 0.166 | |
| ≥90 days | 147/5993 (2.5%) | 336/23,972 (1.4%) | 1.80 (1.48–2.20) | <0.001 a | 1.83 (1.49–2.23) | <0.001 a | 1.45 (1.17–1.79) | <0.001 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Oh, J.-K.; Kim, Y.-H.; Kwon, M.-J.; Kim, J.-H.; Choi, H.-G. Association between Proton Pump Inhibitor Use and Parkinson’s Disease in a Korean Population. Pharmaceuticals 2022, 15, 327. https://doi.org/10.3390/ph15030327
Kim J-H, Oh J-K, Kim Y-H, Kwon M-J, Kim J-H, Choi H-G. Association between Proton Pump Inhibitor Use and Parkinson’s Disease in a Korean Population. Pharmaceuticals. 2022; 15(3):327. https://doi.org/10.3390/ph15030327
Chicago/Turabian StyleKim, Ji-Hee, Jae-Keun Oh, Yoo-Hwan Kim, Mi-Jung Kwon, Joo-Hee Kim, and Hyo-Geun Choi. 2022. "Association between Proton Pump Inhibitor Use and Parkinson’s Disease in a Korean Population" Pharmaceuticals 15, no. 3: 327. https://doi.org/10.3390/ph15030327
APA StyleKim, J. -H., Oh, J. -K., Kim, Y. -H., Kwon, M. -J., Kim, J. -H., & Choi, H. -G. (2022). Association between Proton Pump Inhibitor Use and Parkinson’s Disease in a Korean Population. Pharmaceuticals, 15(3), 327. https://doi.org/10.3390/ph15030327