
Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis


Abstract
:1. Introduction
2. Pathophysiology and Classification of Non-Infectious Choroiditis: A Glimpse of the Essential
3. Diagnostic and Monitoring Methods: A Summary of the Relevant Techniques
3.1. Invasive Methods
3.1.1. Indocyanine Green Angiography (ICGA)
3.1.2. Fluorescein Angiography (FA)
3.2. Non-Invasive Methods
3.2.1. Fundus Autofluorescence (FAF)
3.2.2. Spectral Domain-Optical Coherence Tomography (SD-OCT) and Enhanced Depth Imaging OCT (EDI-OCT)
3.2.3. OCT Angiography (OCT-A)
3.2.4. Visual Field Testing and Microperimetry
3.3. Imaging Biomarkers of Inflammation in Non-Infectious Choroiditis and Monitoring of Therapeutical Intervention
4. General Principles of Immunomodulatory Therapy for Non-Infectious Choroiditis: A Brief Overview of the Main Agents Used
4.1. Corticosteroids
4.2. Immunomodulatory/Immunosuppressive Agents
4.2.1. Antimetabolites
4.2.2. Calcineurin Inhibitors (CI)
4.3. Biological Agents
5. Treatments and Novel Therapeutic Approaches of Non-Infectious Choroiditis
5.1. Choriocapillaritis
5.1.1. MEWDS
5.1.2. Acute Posterior Multifocal Placoid Pigment Epitheliopathy/Acute Ischemic Multifocal Choriocapillaritis (APMPPE/AMIC)
5.1.3. Idiopathic Multifocal Choroiditis (MFC)
5.1.4. Serpiginous Choroiditis (SC)
5.1.5. Tuberculosis Related Serpiginous Choroiditis (TB-SC)
5.1.6. Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC)
5.2. Stromal Choroiditis
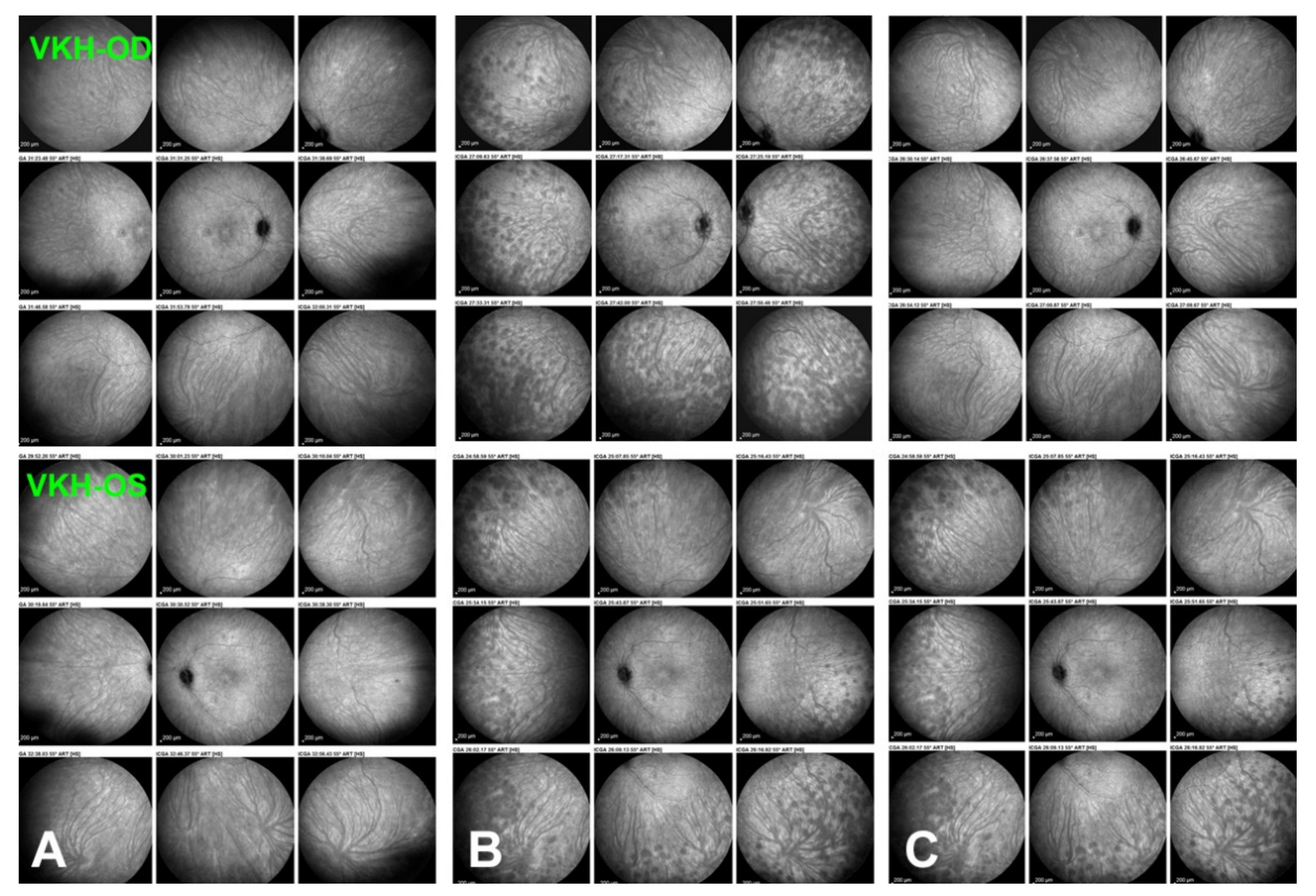
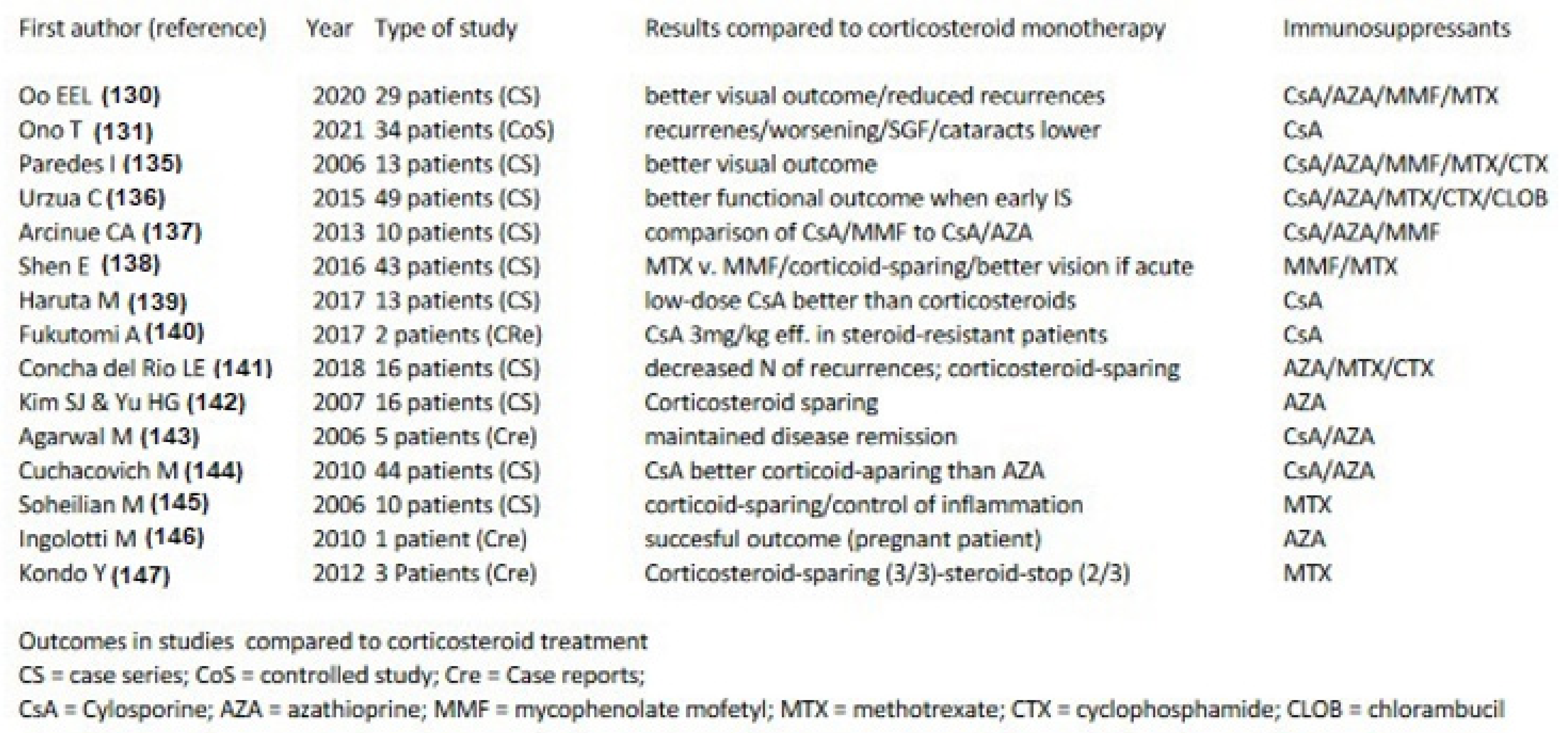
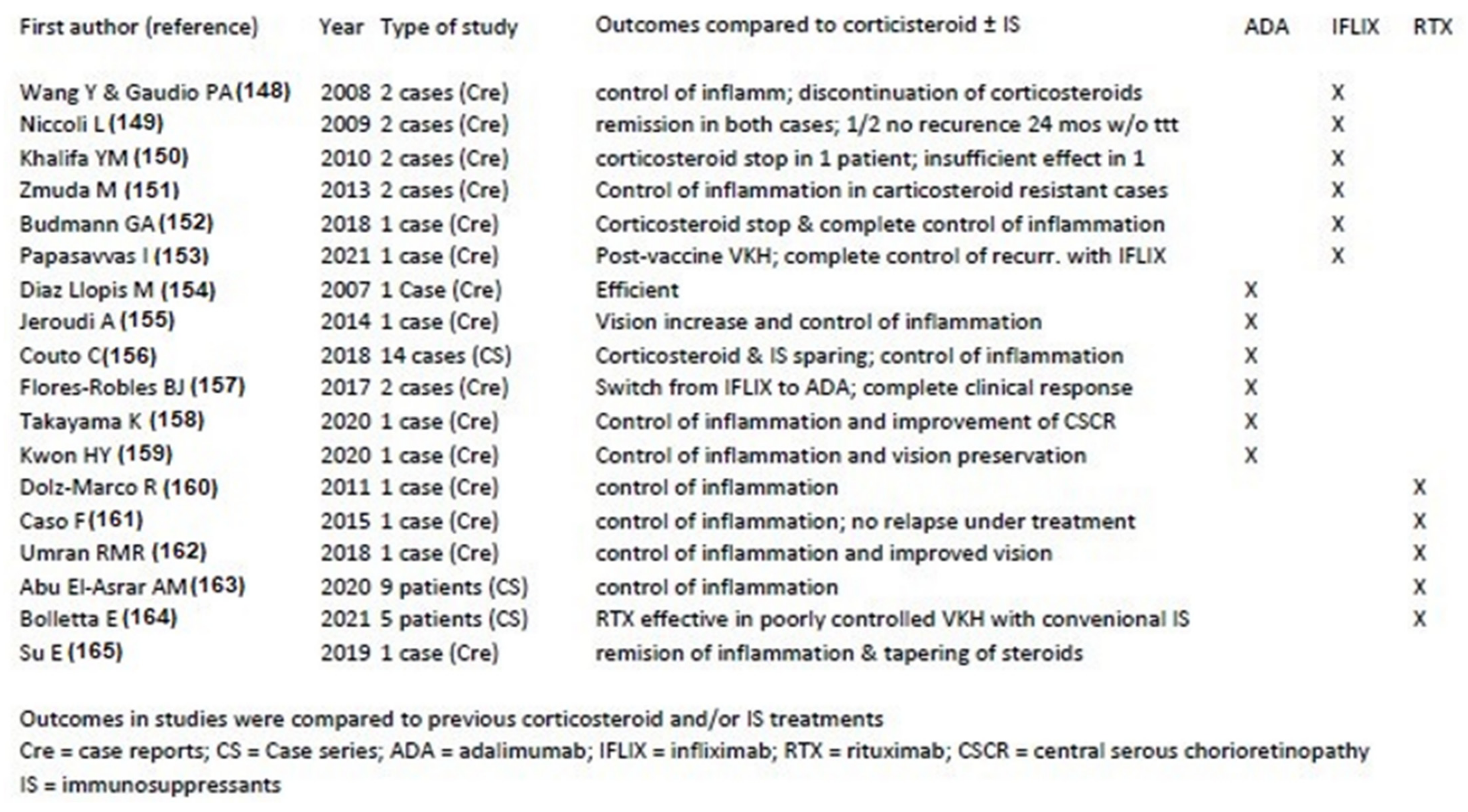
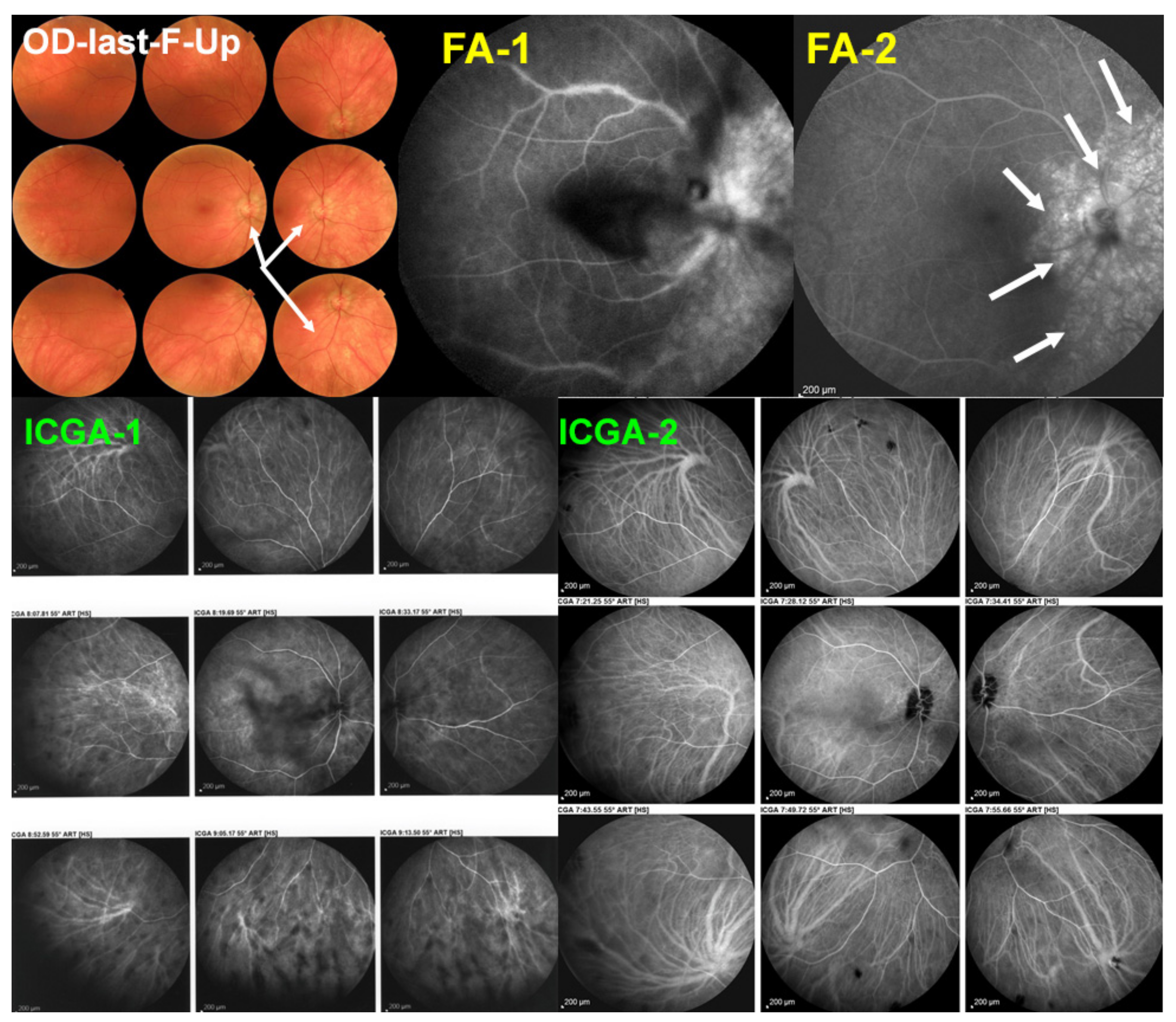
5.2.1. Vogt-Koyanagi-Harada Disease (VKH)
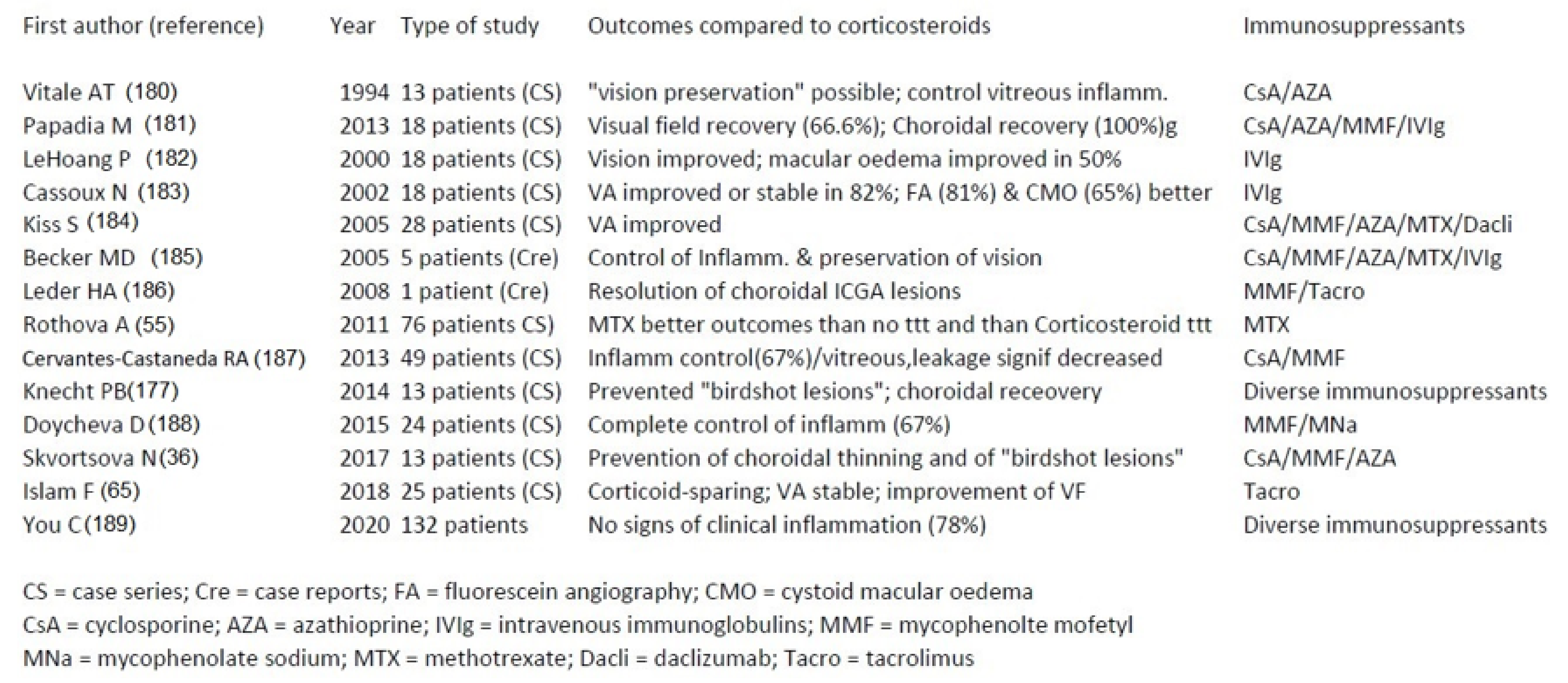
5.2.2. HLA-A29 Birdshot Retinochoroiditis (BRC)
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barry, R.; Denniston, A. Controversies in the Pharmacological Treatment of Uveitis. Curr. Pharm. Des. 2015, 21, 4682–4687. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, A.; Loza, E.; Rosario, M.P.; Espinosa, G.; de Morales, J.M.G.R.; Herrera, J.M.; Muñoz-Fernández, S.; Rodríguez-Rodríguez, L.; Cordero-Coma, M.; Spanish Society of Ocular Inflammation (SEIOC). Efficacy and safety of immunomodulatory drugs in patients with non-infectious intermediate and posterior uveitis, panuveitis and macular edema: A systematic literature review. Semin. Arthritis Rheum. 2020, 50, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Neri, P.; Pichi, F.; Pirani, V.; Arapi, I. Systemic Immunosuppression Is Highly Effective in the Long-term Control of Inflammatory non-infectious Uveitic Choroidal Neovascularization: A Comparative Study. Ocul. Immunol. Inflamm. 2021, 29, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, R.A.; Flores, I.; Pujol, M.; Llanos, C.; Carreño, E.; Rada, G.; Herbort, C.P., Jr.; Cuitino, L.; Urzua, C.A. Definition of Uveitis Refractory to Treatment: A Systematic Review in the Absence of a Consensus. Ocul. Immunol. Inflamm. 2020, 30, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.; Mantovani, A.; Tugal-Tutkun, I.; Papasavvas, I. Classification of Non-Infectious and/or Immune Mediated Choroiditis: A Brief Overview of the Essentials. Diagnostics 2021, 11, 939. [Google Scholar] [CrossRef]
- Papasavvas, I.; Herbort, C.P., Jr. Diagnosis and Treatment of Primary Inflammatory Choriocapillaropathies (PICCPs): A Comprehensive Overview. Medicina 2022, 58, 165. [Google Scholar] [CrossRef]
- Haw, Y.-L.; Yu, T.-C.; Yang, C.-S. A CARE-compliant article: A case report of possible association between recurrence of multiple evanescent white dot syndrome and the Herpesviridae family. Medicine 2020, 99, e19794. [Google Scholar] [CrossRef] [PubMed]
- Papasavvas, I.; Mantovani, A.; Tugal-Tutkun, I.; Herbort, C.P., Jr. Multiple evanescent white dot syndrome (MEWDS): Update on practical appraisal, diagnosis and clinicopathology; a review and an alternative comprehensive perspective. J. Ophthalmic Inflamm. Infect. 2021, 11, 45. [Google Scholar] [CrossRef]
- Testi, I.; Vermeirsch, S.; Pavesio, C. Acute posterior multifocal placoid pigment epitheliopathy (APMPPE). J. Ophthalmic Inflamm. Infect. 2021, 11, 31. [Google Scholar] [CrossRef]
- Papasavvas, I.; Neri, P.; Mantovani, A.; Herbort, C.P., Jr. Idiopathic multifocal choroiditis (MFC): Aggressive and prolonged therapy with multiple immunosuppressive agents is needed to halt the progression of active disease. An offbeat review and a case series. J. Ophthalmic Inflamm. Infect. 2022, 12, 2. [Google Scholar] [CrossRef]
- Dutta Majumder, P.; Biswas, J.; Gupta, A. Enigma of serpiginous choroiditis. Indian J. Ophthalmol. 2019, 67, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Oray, M.; Zakiev, Z.; Çağatay, T.; Tuğal-Tutkun, I. Treatment Results in Serpiginous Choroiditis and Multifocal Serpiginoid Choroiditis Associated with Latent Tuberculosis. Turk. J. Ophthalmol. 2017, 47, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Bansal, R.; Gupta, A. Continuous Progression of Tubercular Serpiginous-like Choroiditis After Initiating Antituberculosis Treatment. Am. J. Ophthalmol. 2011, 152, 857–863.e2. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Papasavvas, I.; Mantovani, A. Choriocapillaris involvement in acute syphilis posterior placoid chorioretinitis is responsible for functional impairment and points towards an immunologic mechanism: A comprehensive clinicopathological approach. J. Curr. Ophthalmol. 2020, 32, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Lavezzo, M.M.; Sakata, V.M.; Morita, C.; Rodriguez, E.E.C.; Abdallah, S.F.; Da Silva, F.T.G.; Hirata, C.E.; Yamamoto, J.H. Vogt-Koyanagi-Harada disease: Review of a rare autoimmune disease targeting antigens of melanocytes. Orphanet J. Rare Dis. 2016, 11, 29. [Google Scholar] [CrossRef] [Green Version]
- Papadia, M.; Pavésio, C.; Fardeau, C.; Neri, P.; Kestelyn, P.; Papasavvas, I.; Herbort, C. HLA-A29 Birdshot Retinochoroiditis in Its 5th Decade: Selected Glimpses into the Intellectual Meanderings and Progresses in the Knowledge of a Long-Time Misunderstood Disease. Diagnostics 2021, 11, 1291. [Google Scholar] [CrossRef]
- Ezra, D.B.; Forrester, J.V. Fundal white dots: The spectrum of a similar pathological process. Br. J. Ophthalmol. 1995, 79, 856–860. [Google Scholar] [PubMed] [Green Version]
- Neri, P.; Herbort, C.P., Jr.; Hedayatfar, A.; Tugal-Tutkun, I.; Cimino, L.; Urzua, C.A.; Papasavvas, I.; Takeuchi, M.; Lages, V. “White dot syndromes”, an inappropriate and outdated misnomer. Int. Ophthalmol. 2021, 42, 1–6. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; LeHoang, P.; Guex-Crosier, Y. Schematic interpretation of indocyanine green angiography in posterior uveitis using a standard angiographic protocol. Ophthalmology 1998, 105, 432–440. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Papadia, M.; Mantovani, A. Classification of Choroiditis Based on Inflammatory Lesion Process rather than Fundus Appearance: Enhanced Comprehension through the ICGA Concepts of the Iceberg and Jellyfish Effects. Klin. Monbl. Augenheilkd. 2012, 229, 306–313. [Google Scholar] [CrossRef]
- Elahi, S.; Herbort, C.P., Jr. Vogt-Koyanagi-Harada Disease and Birdshot Retinochoroidopathy, Similarities and Differences: A Glimpse into the Clinicopathology of Stromal Choroiditis, a Perspective and a Review. Klin. Monbl. Augenheilkd. 2019, 236, 492–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbort, C.P., Jr.; Mantovani, A.; Papadia, M. Use of Indocyanine Green Angiography in Uveitis. Int. Ophthalmol. Clin. 2012, 52, 13–31. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Neri, P.; Papasavvas, I. Clinicopathology of non-infectious choroiditis: Evolution of its appraisal during the last 2–3 decades from “white dot syndromes” to precise classification. J. Ophthalmic Inflamm. Infect. 2021, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.; Sun, H.J.; Ham, D.I. Ultra-wide-field angiography findings in acute Vogt-Koyanagi-Harad disease. Br. J. Ophthalmol. 2019, 103, 942–948. [Google Scholar] [PubMed]
- Abouammoh, M.A.; Gupta, V.; Hemachandran, S.; Herbort, C.P.; Abu El-Asrar, A.M. Indocyanine green angiographic findings in initial-onset acute Vogt-Koyanagi-Harada disese. Acta Ophthalmol. 2016, 94, 573–578. [Google Scholar]
- Miyanaga, M.; Kawaguchi, T.; Miyata, K.; Horie, S.; Mochizuki, M.; Herbort, C.P., Jr. Indocyanine green angiography findings in initial acute pretreatment Vogt-Koyanagi-Harada disease in Japanese patients. Jpn. J. Ophthalmol. 2010, 54, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Balci, O.; Gasc, A.; Jeannin, B.; Herbort, C.P., Jr. Enhanced depth imaging is less suited than indocyanine green angiography for close monitoring of primary stromal choroiditis: A pilot report. Int. Ophthalmol. 2017, 37, 737–748. [Google Scholar] [CrossRef]
- Bouchenaki, N.; Herbort, C.P., Jr. Indocyanine Green Angiography Guided Management of Vogt-Koyanagi-Harada Disease. J. Ophthalmic Vis. Res. 2011, 6, 241–248. [Google Scholar]
- Deutman, A.F. Acute multifocal ischaemic choroidopathy and the choriocapillaris. Int. Ophthalmol. 1983, 6, 155–160. [Google Scholar] [CrossRef]
- Birnbaum, A.D.; Blair, M.P.; Tessler, H.H.; Goldstein, D.A. Subretinal fluid in acute posterior multifocal placoid pigment epitheliopathy. Retina 2010, 30, 810–814. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Giani, A.; Herbort, C.P., Jr.; Staurenghi, G. Interpretation of fundus autofluorescence changes in choriocapillaritis: A multi-modality imaging study. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Priel, E. Fundus Autofluorescence Imaging in Multifocal Choroiditis: Beyond the Spots. Ocul. Immunol. Inflamm. 2014, 22, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Inaba, M.; Kohzaki, K.; Tsuneoka, H. Resolution of Acute Photoreceptor Damage as Revealed by Serial SD-OCT. Optom. Vis. Sci. 2013, 90, e142–e146. [Google Scholar] [CrossRef] [PubMed]
- Papadia, M.; Jeannin, B.; Herbort, C.P., Jr. OCT Findings in Birdshot Chorioretinitis: A Glimpse Into Retinal Disease Evolution. Ophthalmic Surg. Lasers Imaging Retin. 2012, 43, S25–S31. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F.; Koizumi, H.; Pozonni, M.C. Enhanced Depth Imaging Spectral-Domain Optical Coherence Tomography. Am. J. Ophthalmol. 2008, 146, 496–500. [Google Scholar] [CrossRef]
- Skvortsova, N.; Gasc, A.; Jeannin, B.; Herbort, C.P., Jr. Evolution of choroidal thickness over time and effect of early and sustained therapy in birdshot retinochoroiditis. Eye 2017, 31, 1205–1211. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.R.; Vupparaboina, K.K.; Goud, A.; Dansingani, K.K.; Chhablani, J. Choroidal imaging biomarkers. Surv. Ophthalmol. 2019, 64, 312–333. [Google Scholar] [CrossRef]
- Gao, S.; Jia, Y.; Zhang, M.; Su, J.P.; Liu, G.; Hwang, T.; Bailey, S.T.; Huang, D. Optical Coherence Tomography Angiography. Investig. Opthalmology Vis. Sci. 2016, 57, OCT27–OCT36. [Google Scholar] [CrossRef]
- El Ameen, A.; Herbort, C.P., Jr. Serpiginous choroiditis imaged by optical coherence tomography angiography. Retin. Cases Brief Rep. 2018, 12, 279–285. [Google Scholar] [CrossRef]
- Tugal-Tutkun, I.; Herbort, C.P., Jr.; Khairallah, M.; The Angiography Scoring for Uveitis Working Group (ASUWOG). Scoring of dual fluorescein and ICG inflammatory angiographic signs for the grading of posterior segment inflammation (dual fluorescein and ICG angiographic scoring system for uveitis). Int. Ophthalmol. 2010, 30, 539–552. [Google Scholar] [CrossRef]
- Elahi, S.; Gillmann, K.; Gasc, A.; Jeannin, B.; Herbort, C.P., Jr. Sensitivity of indocyanine green angiography compared to fluorescein angiography and enhanced depth imaging optical coherence tomography during tapering and fine-tuning of therapy in primary stromal choroiditis: A case series. J. Curr. Ophthalmol. 2019, 31, 180–187. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Horie, S.; Bouchenaki, N.; Ohno-Matsui, K.; Mochizuki, M.; Herbort, C.P., Jr. Suboptimal therapy controls clinically apparent disease but not subclinical progression of Vogt-Koyanagi-Harada disease. Int. Ophthalmol. 2010, 30, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.C. Endogenous Uveitis: Current Concepts of Treatment. Mayo Clin. Proc. 1990, 65, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Alfano, J.E. Changes in the Intraocular Pressure associated with systemic corticosteroid therapy. Am. J. Ophthalmol. 1963, 56, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Schalenbourg, A.; Leys, A.; De Courten, C.; Coutteel, C.; Herbort, C.P., Jr. Corticosteroid-induced central serous chorioretinopathy in patients with ocular inflammatory disorders. Klin. Monbl. Augenheilkd. 2002, 219, 264–267. [Google Scholar] [CrossRef]
- Tavadia, S.M.; Mydlarski, P.R.; Reis, M.D.; Mittmann, N.; Pinkerton, P.H.; Shear, N.; Sauder, D.N. Screening for azathio-prine toxicity: A pharmacoeconomic analysis based on a target case. J. Am. Acad. Dermatol. 2000, 42, 628–632. [Google Scholar]
- Newell, F.W.; Krill, A.E. Treatment of uveitis with azathioprine (Imuran). Trans. Ophthalmol. Soc. UK 1967, 87, 499–511. [Google Scholar]
- World Health Organization. World Health Organization Model List of Essential Medicines–22nd List; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Chanaud, N.P.; Vistica, B.P.; Eugui, E.; Nussenblatt, R.B.; Allison, A.C.; Gery, I. Inhibition of experimental autoimmune uveoretinitis by mycophenolate mofetil, an inhibitor of purine metabolism. Exp. Eye Res. 1995, 61, 429–434. [Google Scholar] [CrossRef]
- Baltatzis, S.; Tufail, F.; Yu, E.N.; Vredeveld, C.M.; Foster, C.S. Mycophenolate mofetil as an immunomodulatory agent in the treatment of chronic ocular inflammatory disorders. Ophthalmology 2003, 110, 1061–1065. [Google Scholar] [CrossRef]
- Ortega, F.; Fructuoso, A.I.S.; Cruzado, J.M.; Gómez-Alamillo, J.C.; Alarcón, A.; Pallardó, L.; Morales, J.M.; Oliver, J.; Guinea, G.; MYVIDA Study Group. Gastrointestinal Quality of Life Improvement of Renal Transplant Recipients Converted From Mycophenolate Mofetil to Enteric-Coated Mycophenolate Sodium Drugs or Agents: Mycophenolate Mofetil and Enteric-Coated Mycophenolate Sodium. Transplantation 2011, 92, 426–432. [Google Scholar] [CrossRef]
- Suhler, E.B.; Biggee, K. Methotrexate. In Intraocular Inflammation; Zierhut, M., Pavésio, C., Ohno, S., Oréfice, F., Rao, N.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 355–360. [Google Scholar]
- Depla, J.A.; Van Calster, J. Serpiginous choroiditis treated in a stepladder approach. Bull. Soc. Belge Ophtalmol. 2007, 306, 9–13. [Google Scholar]
- Steeples, L.R.; Ashworth, J.; Jones, N. Multifocal chorioretinitis with progressive subretinal fibrosis in a young child. BMJ Case Rep. 2015, 2015, bcr2015212526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothova, A.; Norel, A.O.-V.; I Los, L.; Berendschot, T.T.J.M. Efficacy of low-dose methotrexate treatment in birdshot chorioretinopathy. Retina 2011, 31, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Tsui, E.; Fern, C.M.; Goldberg, N.R. Treatment of refractory tubercular serpiginous–like choroiditis with intravitreal methotrexate. Retin. Cases Brief Rep. 2021, 15, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Azzi, J.R.; Sayegh, M.H.; Mallat, S.G. Calcineurin Inhibitors: 40 Years Later, Can’t Live Without. J. Immunol. 2013, 191, 5785–5791. [Google Scholar] [CrossRef] [Green Version]
- Nussenblatt, R.B.; Rodrigues, M.M.; Salinas-Carmona, M.C.; Gery, I.; Cevario, S.; Wacker, W. Modulation of Experimental Autoimmune Uveitis With Cyclosporin A. Arch. Ophthalmol. 1982, 100, 1146–1149. [Google Scholar] [CrossRef]
- Nussenblatt, R.B.; Palestine, A.G.; Chan, C.-C. Cyclosporine Therapy for Uveitis: Long-Term Followup. J. Ocul. Pharmacol. Ther. 1985, 1, 369–382. [Google Scholar] [CrossRef]
- Johnston, A.; Holt, D.W. Therapeutic drug monitoring of immunosuppressant drugs. Br. J. Clin. Pharmacol. 1999, 47, 339–350. [Google Scholar] [CrossRef] [Green Version]
- Rocha, G.; Deschênes, J.; Cantarovich, M. Cyclosporine Monitoring with Levels 6 Hours after the Morning Dose in Patients with Noninfectious Uveitis. Ophthalmology 1997, 104, 245–251. [Google Scholar] [CrossRef]
- Patocka, J.; Nepovimova, E.; Kuca, K.; Wu, W. Cyclosporine A: Chemistry and Toxicity—A Review. Curr. Med. Chem. 2021, 28, 3925–3934. [Google Scholar] [CrossRef]
- Kilmartin, D.J.; Forrester, J.V.; Dick, A.D. Tacrolimus (FK506) in failed cyclosporin A therapy in endogenous posterior uveitis. Ocul. Immunol. Inflamm. 1998, 6, 101–109. [Google Scholar] [CrossRef]
- Murphy, C.; Greiner, K.; Plskova, J.; Duncan, L.; Frost, N.A.; Forrester, J.V.; Dick, A.D. Cyclosporine vs Tacrolimus Therapy for Posterior and Intermediate Uveitis. Arch. Ophthalmol. 2005, 123, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, F.; Westcott, M.; Rees, A.; Robson, A.G.; Kapoor, B.; Holder, G.; Pavesio, C. Safety profile and efficacy of tacrolimus in the treatment of birdshot retinochoroiditis: A retrospective case series review. Br. J. Ophthalmol. 2017, 102, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, M.; Masuda, K.; Sakane, T.; Ito, K.; Kogure, M.; Sugino, N.; Usui, M.; Mizushima, Y.; Ohno, S.; Inaba, G.; et al. A Clinical Trial of FK506 in Refractory Uveitis. Am. J. Ophthalmol. 1993, 115, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Kempen, J.H.; Daniel, E.; Gangaputra, S.; Dreger, K.; Jabs, D.A.; Kaçmaz, R.O.; Pujari, S.S.; Anzaar, F.; Foster, C.S.; Helzlsouer, K.J.; et al. Methods for Identifying Long-Term Adverse Effects of Treatment in Patients with Eye Diseases: The Systemic Immunosuppressive Therapy for Eye Diseases (SITE) Cohort Study. Ophthalmic Epidemiol. 2008, 15, 47–55. [Google Scholar] [CrossRef]
- Suelves, A.M.; Arcinue, C.A.; González-Martín, J.M.; Kruh, J.N.; Foster, C.S. Analysis of a Novel Protocol of Pulsed Intravenous Cyclophosphamide for Recalcitrant or Severe Ocular Inflammatory Disease. Ophthalmology 2013, 120, 1201–1209. [Google Scholar] [CrossRef]
- Pleyer, U.; Neri, P.; Deuter, C. New pharmacotherapy options for noninfectious posterior uveitis. Int. Ophthalmol. 2021, 41, 2265–2281. [Google Scholar] [CrossRef]
- Bodaghi, B.; Quoc, E.B.; Wechsler, B.; Tran, T.H.C.; Cassoux, N.; Huong, D.L.T.; Chosidow, O.; Herson, S.; Piette, J.-C.; LeHoang, P. Therapeutic use of infliximab in sight threatening uveitis: Retrospective analysis of efficacy, safety, and limiting factors. Ann. Rheum. Dis. 2005, 64, 962–964. [Google Scholar] [CrossRef]
- Neri, P.; Ricci, F.; Giovannini, A.; Arapi, I.; De Felici, C.; Cusumano, A.; Mariotti, C. Successful treatment of an overlapping choriocapillaritis between multifocal choroiditis and acute zonal occult outer retinopathy (AZOOR) with adalimumab (Humira™). Int. Ophthalmol. 2014, 34, 359–364. [Google Scholar] [CrossRef]
- Seve, P.; Mennesson, E.; Grange, J.-D.; Broussolle, C.; Kodjikian, L. Infliximab in serpiginous choroiditis. Acta Ophthalmol. 2010, 88, e342–e343. [Google Scholar] [CrossRef]
- Vegas-Revenga, N.; Calvo-Río, V.; Mesquida, M.; Adán, A.; Hernández, M.V.; Beltrán, E.; Pascual, E.V.; Díaz-Valle, D.; Díaz-Cordovés, G.; Hernandez-Garfella, M.; et al. Anti-IL6-Receptor Tocilizumab in Refractory and Noninfectious Uveitic Cystoid Macular Edema: Multicenter Study of 25 Patients. Am. J. Ophthalmol. 2019, 200, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo-Río, V.; Blanco, R.; Santos-Gómez, M.; Valle, D.D.; Pato, E.; Loricera, J.; González-Vela, M.C.; Demetrio-Pablo, R.; Hernandez, J.L.; González-Gay, M.A. Efficacy of Anti-IL6-Receptor Tocilizumab in Refractory Cystoid Macular Edema of Birdshot Retinochoroidopathy Report of Two Cases and Literature Review. Ocul. Immunol. Inflamm. 2017, 25, 609–614. [Google Scholar] [CrossRef]
- Jaffe, G.J.; Dick, A.D.; Brézin, A.P.; Nguyen, Q.D.; Thorne, J.E.; Kestelyn, P.; Barisani-Asenbauer, T.; Franco, P.; Heiligenhaus, A.; Scales, D.; et al. Adalimumab in Patients with Active Noninfectious Uveitis. N. Engl. J. Med. 2016, 375, 932–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheinfeld, N. Adalimumab (HUMIRA): A review. J. Drugs Dermatol. 2003, 2, 375–377. [Google Scholar] [PubMed]
- Wolf, D.; D’Haens, G.; Sandborn, W.J.; Colombel, J.-F.; Van Assche, G.; Robinson, A.M.; Lazar, A.; Zhou, Q.; Petersson, J.; Thakkar, R.B. Escalation to weekly dosing recaptures response in adalimumab-treated patients with moderately to severely active ulcerative colitis. Aliment. Pharmacol. Ther. 2014, 40, 486–497. [Google Scholar] [CrossRef] [Green Version]
- Golay, J.; Zaffaroni, L.; Vaccari, T.; Lazzari, M.; Borleri, G.M.; Bernasconi, S.; Tedesco, F.; Rambaldi, A.; Introna, M. Biologic re-sponse of B lymphoma cells to anti-CD20 monoclonal antibody rituximab in vitro: CD55 and CD59 regulate comple-ment-mediated cell lysis. Blood 2000, 95, 3900–3908. [Google Scholar]
- Teoh, S.C.B.; Sharma, S.; Hogan, A.; Lee, R.; Ramanan, A.V.; Dick, A.D. Tailoring biological treatment: Anakinra treatment of posterior uveitis associated with the CINCA syndrome. Br. J. Ophthalmol. 2007, 91, 263–264. [Google Scholar] [CrossRef] [Green Version]
- Mesquida, M.; Molins, B.; Llorenç, V.; Hernández, M.V.; Espinosa, G.; De La Maza, M.S.; Adán, A. Twenty-four month follow-up of tocilizumab therapy for refractory uveitis-related macular edema. Retina 2018, 38, 1361–1370. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr. Multiple Evanescent White Dot Syndrome (MEWDS). In Intraocular Inflammation; Zierhut, M., Pavésio, C., Ohno, S., Oréfice, F., Rao, N.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 997–1005. [Google Scholar]
- Khurana, R.; Albini, T.; Dea, M.K.; Rao, N.A.; Lim, J.I. Atypical Presentation of Multiple Evanescent White Dot Syndrome Involving Granular Lesions of Varying Size. Am. J. Ophthalmol. 2005, 139, 935–937. [Google Scholar] [CrossRef]
- Kuznetcova, T.; Jeannin, B.; Herbort, C.P. A case of overlapping choriocapillaritis syndromes: Multimodal imaging ap-praisal. J. Ophthalmic. Vis. Res. 2012, 7, 67–75. [Google Scholar]
- Gass, J.D.M. Acute Posterior Multifocal Placoid Pigment Epitheliopathy. Arch. Ophthalmol. 1968, 80, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Fiore, T.; Iaccheri, B.; Androudi, S.; Papadaki, T.G.; Anzaar, F.; Brazitikos, P.; D’Amico, D.J.; Foster, C.S. Acute posterior multifocal placoid pigment epitheliopathy. Retina 2009, 29, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Uraki, T.; Namba, K.; Mizuuchi, K.; Iwata, D.; Ohno, S.; Kitaichi, N.; Ishida, S. Cyclosporine and prednisolone combination therapy as a potential therapeutic strategy for relentless placoid chorioretinitis. Am. J. Ophthalmol. Case Rep. 2019, 14, 87–91. [Google Scholar] [CrossRef]
- Berger, E.; Ghorayeb, G.; Hogg, J. An atypical case of acute posterior multifocal placoid pigment epitheliopathy with recurrent strokes. Am. J. Ophthalmol. Case Rep. 2019, 16, 100574. [Google Scholar] [CrossRef]
- El-Markaby, H.S.; Mohammed, T.H.; El-Raggal, T.M. Acute posterior multifocal placoid pigment epitheliopathy: Role of TNF blocker in severe cases. Retina 2012, 32, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Vianna, R.N.G.; Vanzan, V.; Turchetti, R.; Burnier, M.; Burnier, M.N., Jr. Intravitreal and posterior subtenon triamcinolone acetonide for severe acute posterior multifocal placoid pigment epitheliopathy. Arq. Bras. Oftalmol. 2019, 82, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Mora-Cantallops, A.; Pérez, M.D.; Revenga, M.; González-López, J.J. Ellipsoid layer restoration after Ozurdex® treatment in a patient with acute posterior multifocal placoid pigment epitheliopathy. Eur. J. Ophthalmol. 2021, 31, NP49–NP53. [Google Scholar] [CrossRef] [PubMed]
- Tavallali, A.; Yannuzzi, L.A. Idiopathic multifocal choroiditis. J. Ophthalmic Vis. Res. 2016, 11, 429–432. [Google Scholar] [CrossRef]
- De Groot, E.L.; ten Dam-van Loon, N.H.; de Boer, J.H.; Ossewaarde-van Norel, J. The efficacy of corticoid-aparing immuno-modulatory therapy in treating patients with central multifocal choroiditis. Acta Ophthalmol. 2020, 98, 816–821. [Google Scholar]
- Neri, P.; Manoni, M.; Fortuna, C.; Lettieri, M.; Mariotti, C.; Giovannini, A. Association of systemic steroids and mycophenolate mofetil as rescue therapy for uveitic choroidal neovascularization unresponsive to the traditional immunesuppressants: Interventional case series. Int. Ophthalmol. 2010, 30, 583–590. [Google Scholar] [CrossRef]
- Goldberg, N.R.; Lyu, T.; Moshier, E.; Godbold, J.; Jabs, D.A. Success with Single-Agent Immunosuppression for Multifocal Choroidopathies. Am. J. Ophthalmol. 2014, 158, 1310–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Hu, J.-H.; Chen, J.; Xie, X. An efficacy analysis of anti-vascular endothelial growth factor therapy for choroidal neovascularization secondary to multifocal choroiditis and comparison with wet age-related macular degeneration. J. Zhejiang Univ. Sci. B 2018, 19, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Hooper, P.L.; Kaplan, H.J. Triple Agent Immunosuppression in Serpiginous Choroiditis. Ophthalmology 1991, 98, 944–951; discussion 951–952. [Google Scholar] [CrossRef] [PubMed]
- Akpek, E.K.; Baltatzis, S.; Yang, J.; Foster, C.S. Long-term immunosuppressive treatment of serpiginous choroiditis. Ocul. Immunol. Inflamm. 2001, 9, 153–167. [Google Scholar] [CrossRef]
- Khanamiri, H.N.; Rao, N.A. Serpiginous Choroiditis and Infectious Multifocal Serpiginoid Choroiditis. Surv. Ophthalmol. 2013, 58, 203–232. [Google Scholar] [CrossRef] [Green Version]
- Markomichelakis, N.N.; Halkiadakis, I.; Papaeythymiou-Orchan, S.; Giannakopoulos, N.; Ekonomopoulos, N.; Kouris, T. Intravenous Pulse Methylprednisolone Therapy for Acute Treatment of Serpiginous Choroiditis. Ocul. Immunol. Inflamm. 2006, 14, 29–33. [Google Scholar] [CrossRef]
- Venkatesh, P.; Tayade, A.; Gogia, V.; Gupta, S.; Shah, B.M.; Vohra, R. Short-term Intensive Immunosuppression: A Randomized, Three-arm Study of Intravenous Pulse Methylprednisolone and Cyclophosphamide in Macular Serpiginous Choroiditis. Ocul. Immunol. Inflamm. 2018, 26, 469–476. [Google Scholar] [CrossRef]
- Ebrahimiadib, N.; Modjtahedi, B.S.; Davoudi, S.; Foster, C.S. Treatment of Serpiginous Choroiditis with Chlorambucil: A Report of 17 Patients. Ocul. Immunol. Inflamm. 2016, 26, 228–238. [Google Scholar] [CrossRef]
- Capote, A.C.; Jiménez, J.M.R.; Soto, M.L.; Gómez, C.R.; De Lucas, M.D.G. Effectiveness of Adalimumab for Refractory Serpiginous Choroiditis. Ocul. Immunol. Inflamm. 2014, 22, 405–408. [Google Scholar] [CrossRef] [Green Version]
- Noda, K.; Oishi, A.; Uji, A.; Tanaka, S.; Tsujikawa, A. Limited efficacy of adalimumab in the acute phase of serpiginous choroiditis refractory to corticosteroid and cyclosporine, a case report. BMC Ophthalmol. 2019, 19, 95. [Google Scholar] [CrossRef] [Green Version]
- Gupta, V.; Gupta, A.; Arora, S.; Bambery, P.; Dogra, M.R.; Agarwal, A. Presumed tubercular serpiginouslike choroiditis: Clinical presentations and management. Ophthalmology 2003, 110, 1744–1749. [Google Scholar] [CrossRef] [PubMed]
- Pathengay, A.; Mishra, S.B.; Saoji, K. Dual lesion margins on fundus autofluorescence associated with paradoxical worsening following treatment for tubercular serpiginous-like choroiditis. Indian J. Ophthalmol. 2020, 68, 536–538. [Google Scholar] [CrossRef]
- Agrawal, R.; Testi, I.; Mahajan, S.; Yuen, Y.S.; Agarwal, A.; Kon, O.M.; Barisani-Asenbauer, T.; Kempen, J.H.; Gupta, A.; Jabs, D.A.; et al. Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis—Report 1: Guidelines for Initiating An-titubercular Therapy in Tubercular Choroiditis. Ophthalmology 2021, 128, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Papasavvas, I.; Jeannin, B.; Herbort, C.P., Jr. Tuberculosis-related serpiginous choroiditis: Aggressive therapy with dual concomitant combination of multiple anti-tubercular and multiple immunosuppressive agents is needed to halt the progression of the disease. J. Ophthalmic Inflamm. Infect. 2022, 12, 7. [Google Scholar] [CrossRef]
- Cordero-Coma, M.; Benito, M.F.; Hernández, A.M.; Antolín, S.C.; Ruíz, J.M.G. Serpiginous Choroiditis. Ophthalmology 2008, 115, 1633–1633.e2. [Google Scholar] [CrossRef] [PubMed]
- Llorenç, V.; Molins, B.; Rey, A.; Mesquida, M.; Adán, A. Adalimumab in Serpiginous Choroiditis. Ocul. Immunol. Inflamm. 2013, 21, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Ormaechea, M.S.; Hassan, M.; Nguyen, Q.D.; Schlaen, A. Acute syphilis posterior placoid chorioretinopathy: An infectious or autoimmune disease? Am. J. Ophthalmol. Case Rep. 2019, 14, 70–73. [Google Scholar]
- Furtado, J.M.; Simões, M.; Vasconcelos-Santos, D.; Oliver, G.F.; Tyagi, M.; Nascimento, H.; Gordon, D.L.; Smith, J.R. Ocular syphilis. Surv. Ophthalmol. 2021, 67, 440–462. [Google Scholar] [CrossRef]
- Fathilah, J.; Choo, M.M. The Jarisch-Herxheimer reaction in ocular syphilis. Med. J. Malays. 2003, 58, 437–439. [Google Scholar]
- Attia, S.; Khochtali, S.; Kahloum, R.; Zouali, S.; Khairallah, M. Vogt-Koyanagi-Harada disease. Expert Rev. Ophthalmol. 2012, 7, 565–568. [Google Scholar]
- Damico, F.M.; Bezerra, F.T.; Da Silva, G.C.; Gasparin, F.; Yamamoto, J.H. New insights into Vogt-Koyanagi-Harada disease. Arq. Bras. Oftalmol. 2009, 72, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu El-Asrar, A.M.; Van Damme, J.; Struyf, S.; Opdenakker, G. New Perspectives on the Immunopathogenesis and Treatment of Uveitis Associated With Vogt-Koyanagi-Harada Disease. Front. Med. 2021, 8, 705796. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Abu El Asrar, A.M.; Yamamoto, J.H.; Pavésio, C.E.; Gupta, V.; Khairallah, M.; Tugal-Tutkun, I.; Soheilian, M.; Takeuchi, M.; Papadia, M.; et al. Reappraisal of the management of Vogt–Koyanagi–Harada disease: Sunset glow fundus is no more a fatality. Int. Ophthalmol. 2016, 37, 1383–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbort, C.P., Jr.; Abu El Asrar, A.M.; Takeuchi, M.; Pavésio, C.E.; Couto, C.; Hedayatfar, A.; Maruyama, K.; Rao, X.; Silpa-Archa, S.; Somkijrungroj, T. Catching the therapeutic window of opportunity in early initial-onset Vogt–Koyanagi–Harada uveitis can cure the disease. Int. Ophthalmol. 2018, 39, 1419–1425. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.; Ye, Z.; Du, L.; Zhou, Q.; Qi, J.; Liang, L.; Wu, L.; Wang, C.; Kijlstra, A. Novel treatment regimen of Vogt–Koyanagi–Harada disease with a reduced dose of corticosteroids combined with immunosuppressive agents. Curr. Eye Res. 2017, 43, 254–261. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Tugal-Tutkun, I.; Abu-El-Asrar, A.; Gupta, A.; Takeuchi, M.; Fardeau, C.; Hedayatfar, A.; Urzua, C.; Papasavvas, I. Precise, simplified diagnostic criteria and optimised management of initial-onset Vogt–Koyanagi–Harada disease: An updated review. Eye 2021, 36, 29–43. [Google Scholar] [CrossRef]
- Silpa-Archa, S.; Silpa-Archa, N.; Preble, J.M.; Foster, C.S. Vogt–Koyanagi–Harada syndrome: Perspectives for immunogenetics, multimodal imaging, and therapeutic options. Autoimmun. Rev. 2016, 15, 809–819. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Tugal-Tutkun, I.; Khairallah, M.; Abu El Asrar, A.M.; Pavésio, C.E.; Soheilian, M. Vogt–Koyanagi–Harada disease: Recurrence rates after initial-onset disease differ according to treatment modality and geographic area. Int. Ophthalmol. 2020, 40, 2423–2433. [Google Scholar] [CrossRef]
- Nakayama, M.; Keino, H.; Watanabe, T.; A Okada, A. Clinical features and visual outcomes of 111 patients with new-onset acute Vogt-Koyanagi-Harada disease treated with pulse intravenous corticosteroids. Br. J. Ophthalmol. 2018, 103, 274–278. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Dosari, M.; Hemachandran, S.; Gikandi, P.W.; Al-Muammar, A. Mycophenolate mofetil combined with systemic corticosteroids prevents progression to chronic recurrent inflammation and development of ‘sunset glow fundus’ in initial-onset acute uveitis associated with Vogt-Koyanagi-Harada disease. Acta Ophthalmol. 2016, 95, 85–90. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Hemachandran, S.; Al-Mezaine, H.S.; Kangave, D.; Al-Muammar, A.M. The outcomes of mycophenolate mofetil therapy combined with systemic corticosteroids in acute uveitis associated with Vogt-Koyanagi-Harada disease. Acta Ophthalmol. 2012, 90, e603–e608. [Google Scholar] [CrossRef] [PubMed]
- Lodhi, S.A.; Reddy, J.L.; Perum, V. Clinical spectrum and management options in Vogt–Koyanagi–Harada disease. Clin. Ophthalmol. 2017, 11, 1399–1406. [Google Scholar] [CrossRef] [Green Version]
- Herbort, C.P., Jr.; Papasavvas, I.; Tugal-Tutkun, I. Vogt–Koyanagi–Harada is a curable autoimmune disease: Early diagnosis and immediate dual steroidal and non-steroidal immunosuppression are crucial prerequisites. J. Curr. Ophthalmol. 2020, 32, 310–314. [Google Scholar] [CrossRef]
- Read, R.W.; Yu, F.; Accorinti, M.; Bodaghi, B.; Chee, S.-P.; Fardeau, C.; Goto, H.; Holland, G.N.; Kawashima, H.; Kojima, E.; et al. Evaluation of the Effect on Outcomes of the Route of Administration of Corticosteroids in Acute Vogt-Koyanagi-Harada Disease. Am. J. Ophthalmol. 2006, 142, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Sakata, V.M.; da Silva, F.T.; Hirata, C.E.; Marin, M.L.C.; Rodrigues, H.; Kalil, J.; Costa, R.A.; Yamamoto, J.H. High rate of clinical recurrence in patients with Vogt–Koyanagi–Harada disease treated with early high-dose corticosteroids. Graefes. Arch. Clin. Exp. Ophthalmol. 2015, 253, 785–790. [Google Scholar] [CrossRef]
- Oo, E.E.L.; Chee, S.-P.; Wong, K.K.Y.; Htoon, H.M. Vogt-Koyanagi-Harada Disease Managed With Immunomodulatory Therapy Within 3 Months of Disease Onset. Am. J. Ophthalmol. 2020, 220, 37–44. [Google Scholar] [CrossRef]
- Ono, T.; Goto, H.; Sakai, T.; Nitta, F.; Mizuki, N.; Takase, H.; Kaneko, Y.; Hori, J.; Nakano, S.; Nao-I, N.; et al. Comparison of combination therapy of prednisolone and cyclosporine with corticosteroid pulse therapy in Vogt–Koyanagi–Harada disease. Jpn. J. Ophthalmol. 2021, 66, 119–129. [Google Scholar] [CrossRef]
- Urzua, C.A.; Herbort, C.; Valenzuela, R.A.; Abu El-Asrar, A.M.; Arellanes-Garcia, L.; Schlaen, A.; Yamamoto, J.; Pavesio, C. Initial-onset acute and chronic recurrent stages are two distinctive courses of Vogt-Koyanagi-Harada disease. J. Ophthalmic Inflamm. Infect. 2020, 10, 23. [Google Scholar] [CrossRef]
- Tugal-Tutkun, I.; Herbort, C.P., Jr.; Mantovani, A.; Neri, P.; Khairallah, M. Advances and potential new developments in imaging techniques for posterior uveitis. Part 1: Noninvasive imaging methods. Eye 2021, 35, 33–51. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Tugal-Tutkun, I.; Mantovani, A.; Neri, P.; Khairallah, M.; Papasavvas, I. Advances and potential new developments in imaging techniques for posterior uveitis Part 2: Invasive imaging methods. Eye 2021, 35, 52–73. [Google Scholar] [CrossRef]
- Paredes, I.; Ahmed, M.; Foster, C.S. Immunomodulatory Therapy for Vogt-Koyanagi-Harada Patients as First-Line Therapy. Ocul. Immunol. Inflamm. 2006, 14, 87–90. [Google Scholar] [CrossRef]
- Urzua, C.A.; Velasquez, V.; Sabat, P.; Berger, O.; Ramirez, S.; Goecke, A.; Vasquez, D.H.; Gatica, H.; Guerrero, J. Earlier immunomodulatory treatment is associated with better visual outcomes in a subset of patients with Vogt-Koyanagi-Harada disease. Acta Ophthalmol. 2015, 93, e475–e480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcinue, C.A.; Radwan, A.; Lebanan, M.O.; Foster, C.S. Comparison of Two Different Combination Immunosuppressive Therapies in the Treatment of Vogt-Koyonagi-Harada Syndrome. Ocul. Immunol. Inflamm. 2013, 21, 47–52. [Google Scholar] [CrossRef]
- Shen, E.; Rathinam, S.R.; Babu, M.; Kanakath, A.; Thundikandy, R.; Lee, S.M.; Browne, E.; Porco, T.C.; Acharya, N.R. Outcomes of Vogt-Koyanagi-Harada Disease: A Subanalysis From a Randomized Clinical Trial of Antimetabolite Therapies. Am. J. Ophthalmol. 2016, 168, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haruta, M.; Yoshioka, M.; Fukutomi, A.; Minami, T.; Mashimo, H.; Shimojo, H.; Ohguro, N. The Effect of Low-dose Cyclo-sporine (100 mg Once Daily) for Chronic Vogt-Koyanagi-Harada Disease. Nippon Ganka Gakkai Zasshi 2017, 121, 474–479. [Google Scholar] [PubMed]
- Fukutomi, A.; Mashimo, H.; Yoshioka, M.; Haruta, M.; Minami, T.; Shimojo, H.; Ohguro, N. Steroid Resistant Vogt-Koyanagi-Harada Disease Treated Effectively with Cyclosporine. Nippon Ganka Gakkai Zasshi 2017, 121, 480–486. [Google Scholar] [PubMed]
- Concha-Del Río, L.E.; Gómez, L.; Arellanes-García, L. Corticotherapy vs. Corticotherapy Plus Immunosuppressive Therapy in Acute Vogt-Koyanagi-Harada Disease. Arch. Soc. Esp. Oftalmol. 2018, 93, 225–230. [Google Scholar]
- Kim, S.J.; Yu, H.G. The Use of Low-Dose Azathioprine in Patients with Vogt-Koyanagi-Harada Disease. Ocul. Immunol. Inflamm. 2007, 15, 381–387. [Google Scholar] [CrossRef]
- Agarwal, M.; Ganesh, S.K.; Biswas, J. Triple Agent Immunosuppressive Therapy in Vogt-Koyanagi-Harada Syndrome. Ocul. Immunol. Inflamm. 2006, 14, 333–339. [Google Scholar] [CrossRef]
- Cuchacovich, M.; Solanes, F.; Díaz, G.; Cermenati, T.; Avila, S.; Verdaguer, J.I.; Carpentier, C.; Stopel, J.; Rojas, B.; Traipe, L.; et al. Comparison of the Clinical Efficacy of Two Different Immunosuppressive Regimens in Patients with Chronic Vogt-Koyanagi-Harada Disease. Ocul. Immunol. Inflamm. 2010, 18, 200–207. [Google Scholar] [CrossRef]
- Soheilian, M.; Aletaha, M.; Yazdani, S.; Dehghan, M.H.; Peyman, G.A. Management of Pediatric Vogt-Koyanagi- Harada (VKH)-Associated Panuveitis. Ocul. Immunol. Inflamm. 2006, 14, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Ingolotti, M.; Schlaen, B.A.; Melo-Granados, E.A.R.; García, H.R.; Partida, J.A.A. Azathioprine During the First Trimester of Pregnancy in a Patient with Vogt-Koyanagi-Harada Disease: A Multimodal Imaging Follow-Up Study. Am. J. Case Rep. 2019, 20, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Fukuda, K.; Suzuki, K.; Nishida, T. Chronic noninfectious uveitis associated with Vogt–Koyanagi–Harada disease treated with low-dose weekly systemic methotrexate. Jpn. J. Ophthalmol. 2012, 56, 104–106. [Google Scholar] [CrossRef]
- Wang, Y.; Gaudio, P.A. Infliximab Therapy for 2 Patients with Vogt-Koyanagi-Harada Syndrome. Ocul. Immunol. Inflamm. 2008, 16, 167–171. [Google Scholar] [CrossRef]
- Niccoli, L.; Nannini, C.; Cassara, E.; Gini, G.; Lenzetti, I.; Cantini, F. Efficacy of infliximab therapy in two patients with refractory Vogt-Koyanagi-Harada disease. Br. J. Ophthalmol. 2009, 93, 1553–1554. [Google Scholar] [CrossRef]
- Khalifa, Y.M.; Bailony, M.R.; Acharya, N.R. Treatment of Pediatric Vogt-Koyanagi-Harada Syndrome with Infliximab. Ocul. Immunol. Inflamm. 2010, 18, 218–222. [Google Scholar] [CrossRef]
- Zmuda, M.; Tiev, K.P.; Knoeri, J.; Héron, E. Successful Use of Infliximab Therapy in Sight-threatening Corticosteroid-resistant Vogt-Koyanagi-Harada Disease. Ocul. Immunol. Inflamm. 2013, 21, 310–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budmann, G.A.; Franco, L.G.; Pringe, A. Long term treatment with infliximab in pediatric Vogt-Koyanagi-Harada disease. Am. J. Ophthalmol. Case Rep. 2018, 11, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Papasavvas, I.; Herbort, C.P., Jr. Reactivation of Vogt-Koyanagi-Harada disease under control for more than 6 years, following anti-SARS-CoV-2 vaccination. J. Ophthalmic Inflamm. Infect. 2021, 11, 21. [Google Scholar] [CrossRef]
- Llopis, M.D.; Amselem, L.; Romero, F.; García-Delpech, S.; Hernandez, M. Tratamiento con Adalimumab -nuevo antiTNF- del síndrome de Vogt-Koyanagi-Harada [Adalimumab therapy for Vogt-Koyanagi-Harada syndrome]. Arch. Soc. Esp. Oftalmol. 2007, 82, 131–132. [Google Scholar] [CrossRef]
- Jeroudi, A.; Angeles-Han, S.T.; Yeh, S. Efficacy of Adalimumab for Pediatric Vogt-Koyanagi-Harada Syndrome. Ophthalmic Surg. Lasers Imaging Retin. 2014, 45, 332–334. [Google Scholar] [CrossRef] [Green Version]
- Couto, C.; Schlaen, A.; Frick, M.; Khoury, M.; Lopez, M.; Hurtado, E.; Goldstein, D. Adalimumab Treatment in Patients with Vogt–Koyanagi–Harada Disease. Ocul. Immunol. Inflamm. 2018, 26, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Robles, B.J.F.; Madrigal, J.B.; Sanchinel, A.A.S.; Pascual, D.H.; Pablo, R.D.; Blanco, R. Anti-TNF? Therapy and switching in severe uveitis related to Vogt-Koyanagi-Harada syndrome. Eur. J. Rheumatol. 2017, 4, 226–228. [Google Scholar] [CrossRef]
- Takayama, K.; Obata, H.; Takeuchi, M. Efficacy of Adalimumab for Chronic Vogt-Koyanagi-Harada Disease Refractory to Conventional Corticosteroids and Immunosuppressive Therapy and Complicated by Central Serous Chorioretinopathy. Ocul. Immunol. Inflamm. 2020, 28, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.Y.; Woo, S.J. A Case of Recurrent Vogt-Koyanagi-Harada Disease Successfully Treated with Adalimumab in Young Female Adult Patient. Korean J. Ophthalmol. 2020, 34, 92–93. [Google Scholar] [CrossRef] [PubMed]
- Dolz-Marco, R.; Gallego-Pinazo, R.; Díaz-Llopis, M. Rituximab in refractory Vogt–Koyanagi–Harada disease. J. Ophthalmic Inflamm. Infect. 2011, 1, 177–180. [Google Scholar] [CrossRef] [Green Version]
- Caso, F.; Rigante, D.; Vitale, A.; Costa, L.; Bascherini, V.; Latronico, E.; Franceschini, R.; Cantarini, L. Long-lasting uveitis remission and hearing loss recovery after rituximab in Vogt-Koyanagi-Harada disease. Clin. Rheumatol. 2015, 34, 1817–1820. [Google Scholar] [CrossRef] [Green Version]
- Umran, R.M.R.; Shukur, Z.Y.H. Rituximab for sight-threatening refractory pediatric Vogt–Koyanagi–Harada disease. Mod. Rheumatol. 2015, 28, 197–199. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Dheyab, A.; Khatib, D.; Struyf, S.; Van Damme, J.; Opdenakker, G. Efficacy of B Cell Depletion Therapy with Rituximab in Refractory Chronic Recurrent Uveitis Associated with Vogt-Koyanagi-Harada Disease. Ocul. Immunol. Inflamm. 2020; 1–8, epub ahead of print. [Google Scholar] [CrossRef]
- Bolletta, E.; Gozzi, F.; Mastrofilippo, V.; Pipitone, N.; De Simone, L.; Croci, S.; Invernizzi, A.; Adani, C.; Iannetta, D.; Coassin, M.; et al. Efficacy of Rituximab Treatment in Vogt-Koyanagi-Harada Disease Poorly Controlled by Traditional Immunosuppressive Treatment. Ocul. Immunol. Inflamm. 2021, 1–6. [Google Scholar] [CrossRef]
- Su, E.; Oza, V.S.; Latkany, P. A case of recalcitrant pediatric Vogt-Koyanagi-Harada disease successfully controlled with adalimumab. J. Formos. Med Assoc. 2019, 118, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, V.; Paldino, G.; Paladini, F.; Mattorre, B.; Tuosto, L.; Sorrentino, R.; Fiorillo, M.T. The Impact of the ‘Mis-Peptidome’ on HLA Class I-Mediated Diseases: Contribution of ERAP1 and ERAP2 and Effects on the Immune Response. Int. J. Mol. Sci. 2020, 21, 9608. [Google Scholar] [CrossRef]
- A Gaudio, P.; Kaye, D.B.; Crawford, J.B. Histopathology of birdshot retinochoroidopathy. Br. J. Ophthalmol. 2002, 86, 1439–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbort, C.P., Jr.; Probst, K.; Cimino, L.; Tran, V.T. Differential Inflammatory Involvement in Retina and Choroïd in Birdshot Chorioretinopathy. Klin. Monbl. Augenheilkd. 2004, 221, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Fardeau, C.; Herbort, C.P., Jr.; Kullmann, N.; Quentel, G.; LeHoang, P. Indocyanine green angiography in birdshot chorioretinopathy. Ophthalmology 1999, 106, 1928–1934. [Google Scholar] [CrossRef]
- Cao, J.H.; Silpa-Archa, S.; Freitas-Neto, C.A.; Foster, C.S. Birdshot chorioretinitis lesions on indocyanine green angiography as an indicator of disease activity. Retina 2016, 36, 1751–1757. [Google Scholar] [CrossRef]
- Priem, H.A.; Oosterhuis, J.A. Birdshot chorioretinopathy: Clinical characteristics and evolution. Br. J. Ophthalmol. 1988, 72, 646–659. [Google Scholar] [CrossRef] [Green Version]
- Gasch, A.T.; Smith, J.A.; Whitcup, S.M. Birdshot retinochoroidopathy. Br. J. Ophthalmol. 1999, 83, 241–249. [Google Scholar]
- Fuerst, D.J.; Tessler, H.H.; Fishman, G.A.; Yokoyama, M.; Wyhinny, G.J.; Vygantas, C.M. Birdshot Retinochoroidopathy. Arch. Ophthalmol. 1984, 102, 214–219. [Google Scholar]
- Rothova, A.; Berendschot, T.T.; Probst, K.; van Kooij, B.; Baarsma, G.S. Birdshot chorioretinopathy: Long-term manifestations and visual prognosis. Ophthalmology 2004, 111, 954–959. [Google Scholar] [CrossRef]
- Lages, V.; Skvortsova, N.; Jeannin, B.; Gasc, A.; Herbort, C.P., Jr. Low-grade “benign” birdshot retinochoroiditis: Prevalence and characteristics. Int. Ophthalmol. 2019, 39, 2111–2120. [Google Scholar] [CrossRef] [PubMed]
- Papadia, M.; Herbort, C.P., Jr. Indocyanine Green Angiography (ICGA) is Essential for the Early Diagnosis of Birdshot Chorioretinopathy. Klin. Monbl. Augenheilkd. 2012, 229, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Knecht, P.B.; Papadia, M.; Herbort, C.P., Jr. Early and sustained treatment modifies the phenotype of birdshot retinochoroiditis. Int. Ophthalmol. 2013, 34, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Papadia, M.; Herbort, C.P., Jr. New concepts in the appraisal and management of birdshot retinochoroiditis, a global perspective. Int. Ophthalmol. 2015, 35, 287–301. [Google Scholar] [CrossRef]
- Maleki, A.; Look-Why, S.; Manhapra, A.; Asgari, S.; Philip, A.M.; Chang, P.Y.; Anesi, S.D.; Foster, C.S. Late recurrence in birdshot chorioretinopathy. Can. J. Ophthalmol. 2021; epub ahead of print. [Google Scholar] [CrossRef]
- Vitale, A.T.; Rodriguez, A.; Foster, C.S. Low-dose Cyclosporine Therapy in the Treatment of Birdshot Retinochoroidopathy. Ophthalmology 1994, 101, 822–831. [Google Scholar] [CrossRef]
- Papadia, M.; Herbort, C.P., Jr. Reappraisal of birdshot retinochoroiditis (BRC): A global approach. Graefes. Arch. Clin. Exp. Ophthalmol. 2012, 251, 861–869. [Google Scholar] [CrossRef] [Green Version]
- LeHoang, P.; Cassoux, N.; George, F.; Kullmann, N.; Kazatchkine, M.D. Intravenous immunoglobulin (IVIg) for the treat-ment of birdshot retinochoroidopathy. Ocul. Immunol. Inflamm. 2000, 8, 49–57. [Google Scholar]
- Cassoux, N.; Goichot-Bonnat, L.; Karmochkine, M.; Georges, F.; Kullmann, N.; Lehoang, P.; Kazatchkine, M. Efficacité et tolé-rance des immunoglobulines intraveineuses dans le traitement de la rétinochoroïdopathie de type Birdshot [Efficacy of intravenous immunoglobulin in the treatment of Birdshot retinochoroiditis]. J. Fr. Ophtalmol. 2002, 25, 23–30. [Google Scholar]
- Kiss, S.; Ahmed, M.; Letko, E.; Foster, C. Long-term Follow-up of Patients with Birdshot Retinochoroidopathy Treated with Corticosteroid-Sparing Systemic Immunomodulatory Therapy. Ophthalmology 2005, 112, 1066–1071.e2. [Google Scholar] [CrossRef]
- Becker, M.D.; Wertheim, M.S.; Smith, J.R.; Rosenbaum, J.T. Long-Term Follow-Up of Patients with Birdshot Retinochoroidopathy Treated with Systemic Immunosuppression. Ocul. Immunol. Inflamm. 2005, 13, 289–293. [Google Scholar] [CrossRef]
- Leder, H.A.; Galor, A.; E Thorne, J.; Jabs, D. Disappearance of classic birdshot spots after immunosuppression with tacrolimus and mycophenolate mofetil. Br. J. Ophthalmol. 2008, 92, 291. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Castañeda, R.A.; Gonzalez-Gonzalez, L.A.; Cordero-Coma, M.; Yilmaz, T.; Foster, C.S. Combined therapy of cyclosporine A and mycophenolate mofetil for the treatment of birdshot retinochoroidopathy: A 12-month follow-up. Br. J. Ophthalmol. 2013, 97, 637–643. [Google Scholar] [CrossRef]
- Doycheva, D.; Jägle, H.; Zierhut, M.; Deuter, C.; Blumenstock, G.; Schiefer, U.; Stingl, K.; Januschowski, K.; Voykov, B.; Stuebiger, N. Mycophenolic acid in the treatment of birdshot chorioretinopathy: Long-term follow-up. Br. J. Ophthalmol. 2014, 99, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, C.; Lasave, A.F.; Kubaisi, B.; Syeda, S.; Ma, L.; Wai, K.C.K.; Diaz, M.H.; Walsh, M.; Stephenson, A.; Montieth, A.; et al. Long-term outcomes of systemic corticosteroid-sparing immunomodulatory therapy for Birdshot Retinochoroidopathy. Ocul. Immunol. Inflamm. 2020, 28, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Sobrin, L. Daclizumab for Treatment of Birdshot Chorioretinopathy. Arch. Ophthalmol. 2008, 126, 186–191. [Google Scholar] [CrossRef]
- Veld, P.I.H.I.H.; van Asten, F.; Kuijpers, R.W.; Rothova, A.; de Jong, E.K.; Hoyng, C.B. Adalimumab therapy for refractory birdshot chorioretinopathy. Retina 2019, 39, 2189–2197. [Google Scholar] [CrossRef]
- Steeples, L.R.; Spry, P.; Lee, R.; Carreño, E. Adalimumab in refractory cystoid macular edema associated with birdshot chorioretinopathy. Int. Ophthalmol. 2017, 38, 1357–1362. [Google Scholar] [CrossRef]
- Mainguy, A.; Lebreton, O.; Masse, H.; Weber, M. Recurrence of inflammatory choroidal lesions on indocyanine green angiography despite adalimumab treatment as monotherapy in two patients with birdshot retinochoroidopathy: Report of two cases. J. Fr. Ophtalmol. 2021, 45, e103–e105. [Google Scholar] [CrossRef]
- Leclercq, M.; Le Besnerais, M.; Langlois, V.; Girszyn, N.; Benhamou, Y.; Ngo, C.; Levesque, H.; Muraine, M.; Gueudry, J. Tocilizumab for the treatment of birdshot uveitis that failed interferon alpha and anti-tumor necrosis factor-alpha therapy: Two cases report and literature review. Clin. Rheumatol. 2018, 37, 849–853. [Google Scholar] [CrossRef]
- Artornsombudh, P.; Gevorgyan, O.; Payal, A.; Siddique, S.S.; Foster, C.S. Infliximab Treatment of Patients with Birdshot Retinochoroidopathy. Ophthalmology 2012, 120, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Burkholder, B.M.; Wang, J.; Dunn, J.P.; Nguyen, Q.D.; Thorne, J.E. Postoperative outcomes after fluocinolone acetonide implant surgery in patients with birdshot chorioretinitis and other types of posterior and panuveitis. Retina 2013, 33, 1684–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajamil-Rodanes, S.; Testi, I.; Luis, J.; Robson, A.G.; Westcott, M.; Pavesio, C. Evaluation of fluocinolone acetonide 0.19 mg intravitreal implant in the management of birdshot retinochoroiditis. Br. J. Ophthalmol. 2020, 106, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Rush, R.B.; Goldstein, D.A.; Callanan, D.G.; Meghpara, B.; Feuer, W.J.; Davis, J.L. Outcomes of Birdshot Chorioretinopathy Treated With an Intravitreal Sustained-Release Fluocinolone Acetonide–Containing Device. Am. J. Ophthalmol. 2011, 151, 630–636. [Google Scholar] [CrossRef] [Green Version]
- Bajwa, A.; Aziz, K.; Foster, C.S. Safety and efficacy of fluocinolone acetonide intravitreal implant (0.59 mg) in birdshot retinochoroidopathy. Retina 2014, 34, 2259–2268. [Google Scholar] [CrossRef]
- Cheng, S.K.; Thompson, I.; Okeagu, C.; Sen, H.N. Choroidal lesions unresponsive to fluocinolone acetonide intravitreal implant in birdshot chorioretinopathy. Retin. Cases Brief Rep. 2022, 16, 56–58. [Google Scholar] [CrossRef]
- Bajwa, A.; Peck, T.; Reddy, A.K.; A Netland, P.; Shildkrot, Y. Dexamethasone implantation in birdshot chorioretinopathy—Long-term outcome. Int. Med Case Rep. J. 2018, 11, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, J.; Reddy, A.K. Intravitreal dexamethasone implantation for birdshot chorioretinopathy. Retin. Cases Brief Rep. 2017, 11, 51–55. [Google Scholar] [CrossRef]
- Rivera de Zea, P.; García-Ben, A.; Rachwani Parshotam, N.; García-Campos, J.M. Dexamethasone intravitreal implant for treatment of persistent macular oedema in Birdshot retinochoroidopathy. Arch. Soc. Esp. Oftalmol. 2016, 91, 138–141. [Google Scholar]
- Terrada, C.; Bruneau, S.; Perrenoud, F.; Massin, P.; Souied, E. Utilisation de l’implant intravitréen de dexaméthasone dans le traitement de la rétinochoroïdopathie de type birdshot [Role of intravitreal dexamethasone implant in the treatment of birdshot retinochoroidopathy]. J. Fr. Ophtalmol. 2012, 35, 745–748. [Google Scholar] [CrossRef]
- Shah, A.; Branley, M. Use of intravitreal triamcinolone in the management of birdshot retinochoroidopathy associated with cystoid macular oedema: A case study over a three-year period. Clin. Exp. Ophthalmol. 2005, 33, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Martidis, A.; Duker, J.S.; Puliafito, C.A. Intravitreal triamcinolone for refractory cystoid macular edema secondary to bird-shot retinochoroidopathy. Arch. Ophthalmol. 2001, 119, 1380–1383. [Google Scholar] [PubMed]
- Gobuty, M.; Adhi, M.; Read, S.P.; Duker, J.S. Visual response and anatomical changes on sequential spectral-domain optical coherence tomography in birdshot chorioretinopathy treated with local corticosteroid therapy. Int. J. Retin. Vitr. 2016, 2, 9. [Google Scholar] [CrossRef] [Green Version]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mechanism of Action | Dose | Side Effects | |
|---|---|---|---|
| Azathioprine | Purine analogue which interferes with DNA and RNA synthesis. Cytostatic drug for T-cells | 2.25–2.75 mg/kg/day (not if absence of TPMT) |
|
| Mycophenolate Mofetil (MMF)/Mycophenolic Acid (MA) | Inhibit the inosine-5′monophosphate dehydrogenase ⇒ stop the purine biosynthetic pathways/decrease antibody production of B-cells. Strong cytostatic effect on T and B lymphocytes | MMF: 1–3 g/day MA: 1440 mg/day |
|
| Methotrexate | Inhibits dihydrofolate reductase ⇒ reduction in DNA and RNA synthesis of rapidly dividing cells | 7.5 to 25 mg/week |
|
| Calcineurin Inhibitors (CsA/Tarcolimus) | Block T lymphocytes by suppressing the production of IL-2, a major enhancer for T-cell activation and recruitment | CsA: 3–5 mg/kg/day Tarcolimus:0.05–0.15 mg/kg/day |
|
| Mechanism of Action | Dose | Side Effects | |
|---|---|---|---|
| Infliximab [70] | Chimeric monoclonal antibody, bound to both transmembrane and soluble form of TNF-a. Kills cells that express TNF-a | iv 5–20 mg/kg/day Loading dose at 0, 2, 4 weeks then every 6–10 weeks |
|
| Adalimumab [76,77] | Human monoclonal antibody, same as infliximab | SC 40 mg every 2 weeks (in severe cases interval can decrease to 7–10 days [3]) |
|
| Rituximab [78] | Chimeric anti-CD20 monoclonal antibody, targets peripheral CD20 B-cells | iv 375 mg/m2 every week for 8 w then every 4 w for 4 months |
|
| Anakinra [79] | Humanized monoclonal IgG antibody, anti-IL-1 receptor | 100 mg/day |
|
| Tocilizumab [80] | Humanized monoclonal antibody, anti-IL 6 receptor | 8 mg/kg every 4 w |
|
| Author | Year | N of Patients | Treatment | Number of Patients with Chronicity (%) | Number of Patients with SGF (%) |
|---|---|---|---|---|---|
| Bouchenaki [28] | 2011 | 5 | CS + IST | 0 (0) | 0 (0) |
| Abu El Asrar [123] | 2017 | 38 | CS + MMF | 0 (0) | 0 (0) |
| Lodhi [125] | 2017 | 24 | CS + AZA | 4 (17) | 6 (25) |
| Yang [118] | 2018 | 105 | CS + IST | 0 (0) | 24 (23) |
| Total | 172 | CS + IST | 4/172 = 2.3% | 30/172 = 17.5% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papasavvas, I.; Tugal-Tutkun, I.; Herbort, C.P., Jr. Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis. Pharmaceuticals 2022, 15, 398. https://doi.org/10.3390/ph15040398
Papasavvas I, Tugal-Tutkun I, Herbort CP Jr. Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis. Pharmaceuticals. 2022; 15(4):398. https://doi.org/10.3390/ph15040398
Chicago/Turabian StylePapasavvas, Ioannis, Ilknur Tugal-Tutkun, and Carl P. Herbort, Jr. 2022. "Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis" Pharmaceuticals 15, no. 4: 398. https://doi.org/10.3390/ph15040398
APA StylePapasavvas, I., Tugal-Tutkun, I., & Herbort, C. P., Jr. (2022). Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis. Pharmaceuticals, 15(4), 398. https://doi.org/10.3390/ph15040398