
Effect of ITPA Polymorphism on Adverse Drug Reactions of 6-Mercaptopurine in Pediatric Patients with Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Methods
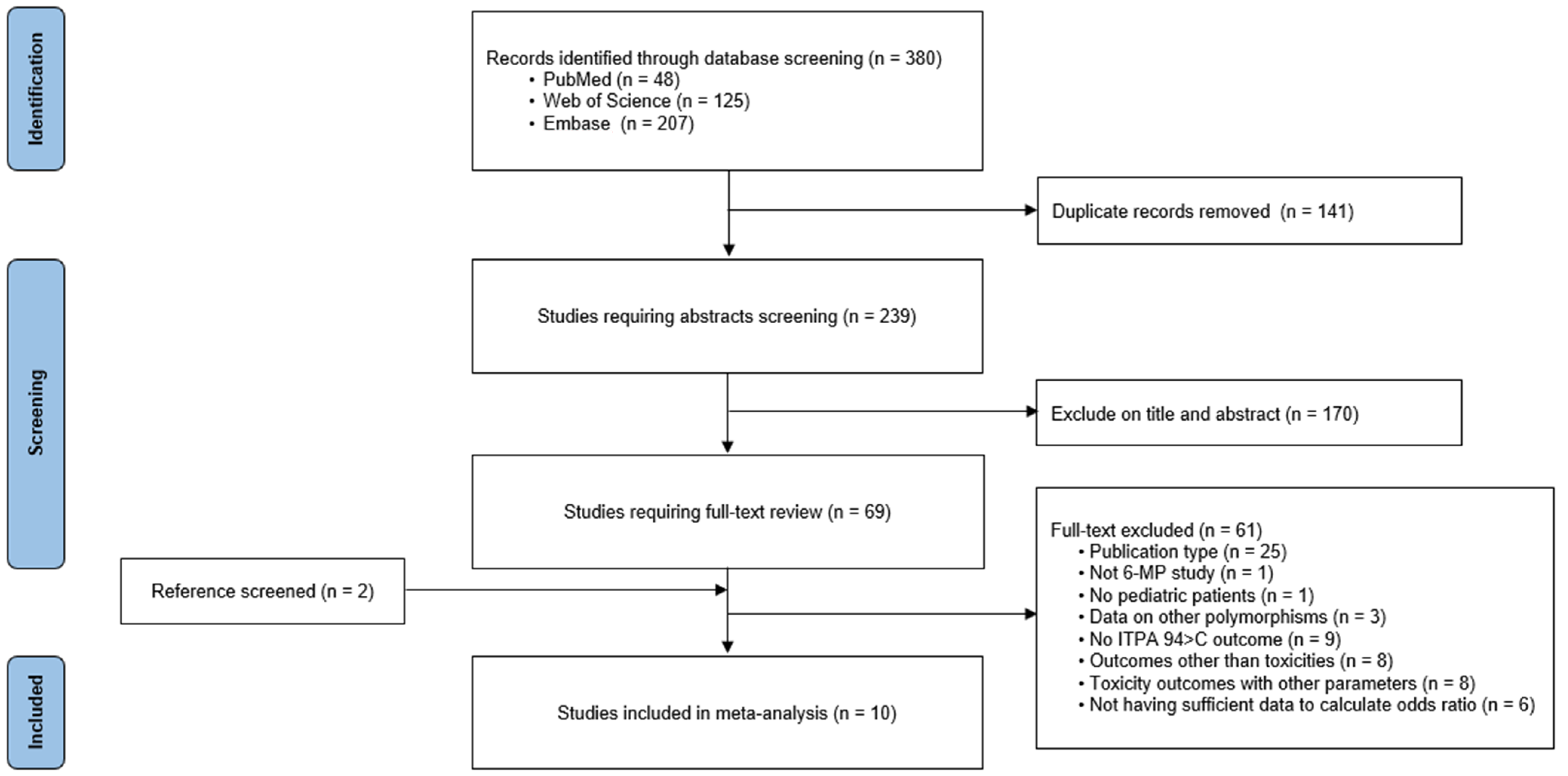
2.1. Literature Search and Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hunger, S.P.; Mullighan, C.G. Acute Lymphoblastic Leukemia in Children. N. Engl. J. Med. 2015, 373, 1541–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mody, R.; Li, S.; Dover, D.C.; Sallan, S.; Leisenring, W.; Oeffinger, K.C.; Yasui, Y.; Robison, L.L.; Neglia, J.P. Twenty-Five-Year Follow-up among Survivors of Childhood Acute Lymphoblastic Leukemia: A Report from the Childhood Cancer Survivor Study. Blood 2008, 111, 5515–5523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, H.; Sun, H.; Sun, X. Survival Improvement by Decade of Patients Aged 0-14 Years with Acute Lymphoblastic Leukemia: A Seer Analysis. Sci. Rep. 2014, 4, 4227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pui, C.H.; Mullighan, C.G.; Evans, W.E.; Relling, M.V. Pediatric Acute Lymphoblastic Leukemia: Where Are We Going and How Do We Get There? Blood 2012, 120, 1165–1174. [Google Scholar] [CrossRef] [Green Version]
- Inaba, H.; Greaves, M.; Mullighan, C.G. Acute Lymphoblastic Leukaemia. Lancet 2013, 381, 1943–1955. [Google Scholar] [CrossRef] [Green Version]
- Seibel, N.L. Treatment of Acute Lymphoblastic Leukemia in Children and Adolescents: Peaks and Pitfalls. Hematol. Am Soc Hematol Educ Program 2008, 2008, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Fotoohi, A.K.; Coulthard, S.A.; Albertioni, F. Thiopurines: Factors Influencing Toxicity nd Response. Biochem. Pharm. 2010, 79, 1211–1220. [Google Scholar] [CrossRef]
- Yang, J.J.; Landier, W.; Yang, W.; Liu, C.; Hageman, L.; Cheng, C.; Pei, D.; Chen, Y.; Crews, K.R.; Kornegay, N.; et al. Inherited Nudt15 Variant Is a Genetic Determinant of Mercaptopurine Intolerance in Children with Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2015, 33, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Moriyama, T.; Nishii, R.; Lin, T.-N.; Kihira, K.; Toyoda, H.; Jacob, N.; Kato, M.; Koh, K.; Inaba, H.; Manabe, A.; et al. The effects of inherited NUDT15 polymorphisms on thiopurine active metabolites in Japanese children with acute lymphoblastic leukemia. Pharmacogenetics Genom. 2017, 27, 236–239. [Google Scholar] [CrossRef]
- Schmiegelow, K.; Nielsen, S.N.; Frandsen, T.L.; Nersting, J. Mercaptopurine/Methotrexate Maintenance Therapy of Childhood Acute Lymphoblastic Leukemia: Clinical Facts and Fiction. J. Pediatr. Hematol. Oncol. 2014, 36, 503–517. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.H.; Chang, Y.; Wang, D.; Jou, S.; Lin, C.; Lin, K.; Lu, M.; Raghav, L.; Chang, H.; Wu, K.; et al. Determination of Nudt15 Variants by Targeted Sequencing Can Identify Compound Heterozygosity in Pediatric Acute Lymphoblastic Leukemia Patients. Sci. Rep. 2020, 10, 14400. [Google Scholar] [CrossRef] [PubMed]
- Mei, L.; Ontiveros, E.P.; Griffiths, E.A.; Thompson, J.E.; Wang, E.S.; Wetzler, M. Pharmacogenetics Predictive of Response and Toxicity in Acute Lymphoblastic Leukemia Therapy. Blood Rev. 2015, 29, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Relling, M.V.; Schwab, M.; Whirl-Carrillo, M.; Suarez-Kurtz, G.; Pui, C.-H.; Stein, C.M.; Moyer, A.M.; Evans, W.E.; Klein, T.E.; Antillon-Klussmann, F.G.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clin. Pharmacol. Ther. 2018, 105, 1095–1105. [Google Scholar] [CrossRef] [Green Version]
- Stocco, G.; Crews, K.R.; Evans, W.E. Genetic Polymorphism of Inosine-Triphosphate-Pyrophosphatase Influences Mercaptopurine Metabolism and Toxicity During Treatment of Acute Lymphoblastic Leukemia Individualized for Thiopurine-S-Methyl-Transferase Status. Expert Opin. Drug. Saf. 2010, 9, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Bierau, J.; Lindhout, M.; Bakker, J.A. Pharmacogenetic Significance of Inosine Triphosphatase. Pharmacogenomics 2007, 8, 1221–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumi, S.; Marinaki, A.M.; Arenas, M.; Fairbanks, L.; Shobowale-Bakre, M.; Rees, D.; Thein, S.; Ansari, A.; Sanderson, J.; De Abreu, R.; et al. Genetic basis of inosine triphosphate pyrophosphohydrolase deficiency. Qual. Life Res. 2002, 111, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Mantel, N.; Haenszel, W. Statistical Aspects of the Analysis of Data from Retrospective Studies of Disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Moradveisi, B.; Muwakkit, S.; Zamani, F.; Ghaderi, E.; Mohammadi, E.; Zgheib, N.K. Itpa, Tpmt, and Nudt15 Genetic Polymorphisms Predict 6-Mercaptopurine Toxicity in Middle Eastern Children with Acute Lymphoblastic Leukemia. Front. Pharmacol. 2019, 10, 916. [Google Scholar] [CrossRef] [Green Version]
- Azimi, F.; Mortazavi, Y.; Alavi, S.; Khalili, M.; Ramazani, A. Frequency of Itpa Gene Polymorphisms in Iranian Patients with Acute Lymphoblastic Leukemia and Prediction of Its Myelosuppressive Effects. Leuk. Res. 2015, 39, 1048–1054. [Google Scholar] [CrossRef]
- Chiengthong, K.; Ittiwut, C.; Muensri, S.; Sophonphan, J.; Sosothikul, D.; Seksan, P.; Suppipat, K.; Suphapeetiporn, K.; Shotelersuk, V. Nudt15 C.415c>T Increases Risk of 6-Mercaptopurine Induced Myelosuppression During Maintenance Therapy in Children with Acute Lymphoblastic Leukemia. Haematologica 2016, 101, e24–e26. [Google Scholar] [CrossRef] [PubMed]
- Jantararoungtong, T.; Wiwattanakul, S.; Tiyasirichokchai, R.; Prommas, S.; Sukprasong, R.; Koomdee, N.; Jinda, P.; Rachanakul, J.; Nuntharadthanaphong, N.; Pakakasama, S.; et al. TPMT*3C as a Predictor of 6-Mercaptopurine-Induced Myelotoxicity in Thai Children with Acute Lymphoblastic Leukemia. J. Pers. Med. 2021, 11, 783. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Yin, R.; Sun, G.; Zhou, Y.; Yang, C.; Fang, C.; Tian, X. Effects of Tpmt, Nudt15, and Itpa Genetic Variants on 6-Mercaptopurine Toxicity for Pediatric Patients with Acute Lymphoblastic Leukemia in Yunnan of China. Front. Pediatr. 2021, 9, 719803. [Google Scholar] [CrossRef]
- Milosevic, G.; Kotur, N.; Krstovski, N.; Lazic, J.; Zukic, B.; Stankovic, B.; Dokmanovic, L. Variants in Tpmt, Itpa, Abcc4 and Abcb1 Genes as Predictors of 6-Mercaptopurine Induced Toxicity in Children with Acute Lymphoblastic Leukemia. J. Med. Biochem. 2018, 37, 320–327. [Google Scholar] [CrossRef]
- Wan Rosalina, W.R.; Teh, L.K.; Mohamad, N.; Nasir, A.; Yusoff, R.; Baba, A.A.; Salleh, M.Z. Polymorphism of Itpa 94c>a and Risk of Adverse Effects among Patients with Acute Lymphoblastic Leukaemia Treated with 6-Mercaptopurine. J. Clin. Pharm. Ther. 2012, 37, 237–241. [Google Scholar] [CrossRef]
- Stocco, G.; Cheok, M.H.; Crews, K.R.; Dervieux, T.; French, D.; Pei, D.; Yang, W.; Cheng, C.; Pui, C.-H.; Relling, M.V.; et al. Genetic Polymorphism of Inosine Triphosphate Pyrophosphatase Is a Determinant of Mercaptopurine Metabolism and Toxicity During Treatment for Acute Lymphoblastic Leukemia. Clin. Pharmacol. Ther. 2009, 85, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Nakadate, H.; Kondoh, K.; Nakamura, K.; Koh, K.; Manabe, A. Interaction between Nudt15 and Abcc4 Variants Enhances Intolerability of 6-Mercaptopurine in Japanese Patients with Childhood Acute Lymphoblastic Leukemia. Pharm. J 2018, 18, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Zaman, S.; Fukushima, H.; Suzuki, R.; Yoshimatsu, S.; Hawlader, M.D.H.; Fukushima, T. Tpmt and Itpa Gene Polymorphism and Their Adverse Events During Chemotherapy of Acute Lymphoblastic Leukemia among Bangladeshi Children. Iran. J. Blood Cancer 2019, 11, 96–100. [Google Scholar]
- Pui, C.H.; Robison, L.L.; Look, A.T. Acute Lymphoblastic Leukaemia. Lancet 2008, 371, 1030–1043. [Google Scholar] [CrossRef]
- Karran, P.; Attard, N. Thiopurines in Current Medical Practice: Molecular Mechanisms and Contributions to Therapy-Related Cancer. Nat. Rev. Cancer 2008, 8, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Hon, Y.Y.; Chu, Y.; Van de Poll, M.E.; Relling, M.V. Assay of 6-Mercaptopurine and Its Metabolites in Patient Plasma by High-Performance Liquid Chromatography with Diode-Array Detection. J. Chromatogr. B Biomed. Sci. Appl. 1999, 732, 459–468. [Google Scholar] [CrossRef]
- Citterio-Quentin, A.; Moulsma, M.; Gustin, M.P.; Boulieu, R. Itpa Activity in Adults and Children Treated with or without Azathioprine: Relationship between Tpmt Activity, Thiopurine Metabolites, and Co-Medications. Ther. Drug Monit. 2017, 39, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Citterio-Quentin, A.; Moulsma, M.; Gustin, M.P.; Lachaux, A.; Boulieu, R. Itpa Activity in Children Treated by Azathioprine: Relationship to the Occurrence of Adverse Drug Reactions and Inflammatory Response. Basic. Clin. Pharm. Toxicol. 2018, 122, 588–595. [Google Scholar] [CrossRef] [Green Version]
- Herting, G.; Barber, K.; Zappala, M.R.; Cunningham, R.P.; Burgis, N.E. Quantitative in Vitro and in Vivo Characterization of the Human P32t Mutant Itpase. Biochim. Biophys. Acta 2010, 1802, 269–274. [Google Scholar] [CrossRef]
- Adam de Beaumais, T.; Jacqz-Aigrain, E. Pharmacogenetic Determinants of Mercaptopurine Disposition in Children with Acute Lymphoblastic Leukemia. Eur. J. Clin. Pharmacol. 2012, 68, 1233–1242. [Google Scholar] [CrossRef]
- Dorababu, P.; Nagesh, N.; Linga, V.G.; Gundeti, S.; Kutala, V.K.; Reddanna, P.; Digumarti, R. Epistatic Interactions between Thiopurine Methyltransferase (Tpmt) and Inosine Triphosphate Pyrophosphatase (Itpa) Variations Determine 6-Mercaptopurine Toxicity in Indian Children with Acute Lymphoblastic Leukemia. Eur. J. Clin. Pharmacol. 2012, 68, 379–387. [Google Scholar] [CrossRef]
- Hareedy, M.S.; El Desoky, E.S.; Woillard, J.B.; Thabet, R.H.; Ali, A.M.; Marquet, P.; Picard, N. Genetic Variants in 6-Mercaptopurine Pathway as Potential Factors of Hematological Toxicity in Acute Lymphoblastic Leukemia Patients. Pharmacogenomics 2015, 16, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Zelinkova, Z.; Derijks, L.J.; Stokkers, P.C.; Vogels, E.W.; van Kampen, A.H.; Curvers, W.L.; Cohn, D.; van Deventer, S.J.; Hommes, D.W. Inosine Triphosphate Pyrophosphatase and Thiopurine S-Methyltransferase Genotypes Relationship to Azathioprine-Induced Myelosuppression. Clin. Gastroenterol. Hepatol. 2006, 4, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, K.; Nakamura, M.; Kubota, T.; Yamane, T.; Fujise, K.; Tajiri, H. Thiopurine S-Methyltransferase and Inosine Triphosphate Pyrophosphohydrolase Genes in Japanese Patients with Inflammatory Bowel Disease in Whom Adverse Drug Reactions Were Induced by Azathioprine/6-Mercaptopurine Treatment. J. Gastroenterol. 2009, 44, 197–203. [Google Scholar] [CrossRef]
- Adam de Beaumais, T.; Fakhoury, M.; Medard, Y.; Azougagh, S.; Zhang, D.; Yakouben, K.; Jacqz-Aigrain, E. Determinants of Mercaptopurine Toxicity in Paediatric Acute Lymphoblastic Leukemia Maintenance Therapy. Br. J. Clin. Pharmacol. 2011, 71, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Manabe, A.; Nakadate, H.; Kondoh, K.; Nakamura, K.; Koh, K.; Utano, T.; Kikuchi, A.; Komiyama, T. The Activity of the Inosine Triphosphate Pyrophosphatase Affects Toxicity of 6-Mercaptopurine During Maintenance Therapy for Acute Lymphoblastic Leukemia in Japanese Children. Leuk. Res. 2012, 36, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Marinaki, A.M.; Ansari, A.; Duley, J.A.; Arenas, M.; Sumi, S.; Lewis, C.M.; Shobowale-Bakre el, M.; Escuredo, E.; Fairbanks, L.D.; Sanderson, J.D. Adverse Drug Reactions to Azathioprine Therapy Are Associated with Polymorphism in the Gene Encoding Inosine Triphosphate Pyrophosphatase (Itpase). Pharmacogenetics 2004, 14, 181–187. [Google Scholar] [CrossRef]
- Gerbek, T.; Ebbesen, M.; Nersting, J.; Frandsen, T.L.; Appell, M.L.; Schmiegelow, K. Role of Tpmt and Itpa Variants in Mercaptopurine Disposition. Cancer Chemother. Pharmacol. 2018, 81, 579–586. [Google Scholar] [CrossRef]
- Wu, J.Z.; Larson, G.; Walker, H.; Shim, J.H.; Hong, Z. Phosphorylation of Ribavirin and Viramidine by Adenosine Kinase and Cytosolic 5′-Nucleotidase Ii: Implications for Ribavirin Metabolism in Erythrocytes. Antimicrob. Agents Chemother. 2005, 49, 2164–2171. [Google Scholar] [CrossRef] [Green Version]
- De Franceschi, L.; Fattovich, G.; Turrini, F.; Ayi, K.; Brugnara, C.; Manzato, F.; Noventa, F.; Stanzial, A.M.; Solero, P.; Corrocher, R. Hemolytic Anemia Induced by Ribavirin Therapy in Patients with Chronic Hepatitis C Virus Infection: Role of Membrane Oxidative Damage. Hepatology 2000, 31, 997–1004. [Google Scholar] [CrossRef]
- Jimmerson, L.C.; Clayton, C.W.; MaWhinney, S.; Meissner, E.G.; Sims, Z.; Kottilil, S.; Kiser, J.J. Effects of Ribavirin/Sofosbuvir Treatment and Itpa Phenotype on Endogenous Purines. Antiviral. Res. 2017, 138, 79–85. [Google Scholar] [CrossRef]
- Hitomi, Y.; Cirulli, E.T.; Fellay, J.; McHutchison, J.G.; Thompson, A.J.; Gumbs, C.E.; Shianna, K.V.; Urban, T.J.; Goldstein, D.B. Inosine Triphosphate Protects against Ribavirin-Induced Adenosine Triphosphate Loss by Adenylosuccinate Synthase Function. Gastroenterology 2011, 140, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Marsh, S.; Van Booven, D.J. The Increasing Complexity of Mercaptopurine Pharmacogenomics. Clin. Pharmacol. Ther. 2009, 85, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Marsh, S.; King, C.R.; Ahluwalia, R.; McLeod, H.L. Distribution of Itpa P32t Alleles in Multiple World Populations. J. Hum. Genet. 2004, 49, 579–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dieren, J.M.; Hansen, B.E.; Kuipers, E.J.; Nieuwenhuis, E.E.; Van der Woude, C.J. Meta-Analysis: Inosine Triphosphate Pyrophosphatase Polymorphisms and Thiopurine Toxicity in the Treatment of Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2007, 26, 643–652. [Google Scholar] [CrossRef]
- Barba, E.; Kontou, P.I.; Michalopoulos, I.; Bagos, P.G.; Braliou, G.G. Association of Itpa Gene Polymorphisms with Adverse Effects of Aza/6-Mp Administration: A Systematic Review and Meta-Analysis. Pharmacogenomics. J. 2022, 22, 39–54. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Sample Size (Male %) | Age (Years) (Mean ± SD) | 6-MP Dose | Dose Adjustment | Concomitant Drugs | Outcome | Genotyping Method | NOS Score |
|---|---|---|---|---|---|---|---|---|---|
| Azimi et al. (2015) [24] | Iran | 70 (48.6) | 1–9 c | 50 mg/m2 | To maintain a WBC count of 2000–3000/μL | MTX | Leukopenia Neutropenia Hepatotoxicity | Sanger method | 7 |
| Chiengthong et al. (2016) [25] | Thailand | 82 (40.2) | 5.4 (1–15) a | 50 mg/m2 | To maintain ANC 500 -1500/μL | VCR, PD, MTX, IT MTX | ANC < 500/μL | Pyrosequencing | 6 |
| Jantararoungtong et al. (2021) [26] | Thailand | 115 (54.8) | 6.11 ± 3.86 | 75 mg/m2 | To maintain WBC ≥ 1500/μL, ANC ≥ 500/μL ± infection records | Low risk: MTX 40 mg/m2 PO weekly VCR 2 mg/m2 IV monthly PD 40 mg/m2 PO 5 days/month Standard/high risk: MTX 40 mg/m2 PO weekly VCR 2 mg/m2 IV monthly PD 60 mg/m2 PO 5 days/month CP 300 mg/m2 IV monthly Ara-C 300 mg/m2 IV monthly | Leukopenia: WBC < 2000/μL Neutropenia: ANC < 1000/μL Hepatotoxicity: ALT > X 3 ULN | TaqMan assays | 6 |
| Mao et al. (2021) [27] | China | 149 (57.0) | 5.92 (0.63–13.75) a | 50 mg/m2 | To maintain a WBC count of 2000–3000/μL | MTX 20 mg/m2 PO weekly VCR 1.5 mg/m2 IV monthly DEX 6 mg/m2 PO 5 days/month | Leukopenia: WBC < 2000/μL Hepatotoxicity: ALT > X 5 ULN | Fluorescence in situ hybridization | 6 |
| Milosevic et al. (2018) [28] | Serbia | 60 (55.9) | 5.2 (0.9-17.6) a | 50 mg/m2 | To maintain a WBC count of 2000–3000/μL | MTX 20 mg/m2 PO weekly | Hepatotoxicity: Elevated levels of transaminases | PCR-RELP method | 6 |
| Moradveisi et al. (Kurdistan) (2019) [23] | Kurdistan | 74 (58.1) | 6.25 ± 3.07 | 75 mg/m2 | To maintain a WBC count of 2000–3000/μL, ANC > 500/μL | MTX 20 mg/m2 PO weekly | Febrile neutropenia: ANC < 1000/mm3 with a single temperature of >38.3 °C (101 °F) or a sustained temperature of ≥38 °C (100.4 °F) for more than one hour Hepatotoxicity: ALT ≥ X 3 ULN | PCR-RELP method | 6 |
| Moradveisi et al. (Lebanon) (2019) [23] | Lebanon | 136 (56.6) | 6.63 ± 4.93 | 75 mg/m2 | To maintain a WBC count of 1500–3000/μL, ANC > 300/μL, PLT > 50,000 | MTX 40 mg/m2 PO weekly | Febrile neutropenia: ANC < 1000/mm3 with a single temperature of >38.3 °C (101 °F) or a sustained temperature of ≥38 °C (100.4 °F) for more than one hour Direct bilirubin ≥ 1.5 | TaqMan allele | 6 |
| Rosalina et al. (2012) [29] | Malaysia | 63 (52.3) | 10.13 (1–20) b | N/A | N/A | N/A | Liver toxicity | Allele-specific PCR | 6 |
| Stocco et al. (2009) [30] | USA | 244 (58.6) | 5.9 (0.08–18.8) a | 75 mg/m2 | When patients developed toxicity attributable to 6-MP | Low risk: MTX 40 mg/m2 IV weekly DEX 8 mg/m2 PO 7 days/month VCR 1.5 mg/m2 IV monthly Higher risk: received drugs pairs rotating weekly d | Grade 3/4 febrile neutropenia Grade 3: ANC < 1000/μL with a single temperature of >38.3 °C (101 °F) or a sustained temperature of ≥ 38 °C (100.4 °F) for more than one hour Grade 4: Life-threatening consequences; urgent intervention indicated | TaqMan assay | 8 |
| Tanaka et al. (2018) [31] | Japan | 95 (49.5) | 4.9 (1–17) a | 40 mg/m2 | To maintain a WBC count of 2000–3500/μL | MTX 25 mg/m2 PO weekly | Leukopenia: WBC < 2000/μL or neutrophil count < 1000/μL Hepatotoxicity: ALT > 700 IU/L | TaqMan assays | 6 |
| Zaman et al. (2019) [32] | Bangladesh | 75 (NA) | 5 ± 2.5 | 75 mg/m2 | When patients developed toxicity attributable to 6-MP | NA | Leukopenia: WBC < 3000/μL Neutropenia: ANC < 1000/μL Raised serum ALT: ALT > 36 U/L | TaqMan assays | 8 |
| Study Excluded | Heterogeneity I2 (%) | Statistical Model | Odds Ratio (95% CI) |
|---|---|---|---|
| Neutropenia | |||
| None | 55 | Random | 2.60 (1.30–5.19) |
| Azimi et al. (2015) | 55 | Random | 2.27 (1.14–4.54) |
| Chiengthong et al. (2016) | 63 | Random | 2.87 (1.20–6.88) |
| Jantararoungtong et al. (2021) | 46 | Fixed | 3.07 (1.90–4.96) |
| Moradveisi et al. (2019) (Kurdistan) | 57 | Random | 2.36 (1.19–4.69) |
| Moradveisi et al. (2019) (Lebanon) | 53 | Random | 3.11 (1.51–6.38) |
| Stocco et al. (2009) | 61 | Random | 2.57 (1.09–6.06) |
| Zaman et al. (2019) | 50 | Random | 2.16 (1.05–4.43) |
| Leukopenia | |||
| None | 70 | Random | 1.75 (0.74–4.12) |
| Azimi et al. (2015) | 69 | Random | 1.39 (0.61–3.16) |
| Jantararoungtong et al. (2021) | 77 | Random | 2.11 (0.67–6.71) |
| Mao et al. (2021) | 77 | Random | 1.97 (0.56–6.89) |
| Tanaka et al. (2018) | 58 | Random | 2.38 (1.02–5.52) |
| Zaman et al. (2019) | 64 | Random | 1.30 (0.56–3.03) |
| Hepatotoxicity | |||
| None | 41 | Fixed | 1.98 (1.32–2.95) |
| Azimi et al. (2015) | 0 | Fixed | 1.68 (1.10–2.58) |
| Jantararoungtong et al. (2021) | 34 | Fixed | 2.41 (1.53–3.80) |
| Mao et al. (2021) | 46 | Fixed | 1.37 (1.37–3.44) |
| Milosevic et al. (2018) | 46 | Fixed | 1.90 (1.26–2.85) |
| Moradveisi et al. (2019) (Kurdistan) | 49 | Fixed | 1.99 (1.33–2.98) |
| Moradveisi et al. (2019) (Lebanon) | 48 | Fixed | 2.00 (1.33–3.01) |
| Rosalina et al. (2012) | 48 | Fixed | 2.05 (1.34–3.13) |
| Tanaka et al. (2018) | 48 | Fixed | 2.04 (1.34–3.12) |
| Zaman et al. (2019) | 36 | Fixed | 1.72 (1.11–2.66) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Jang, E.J.; Yoon, H.-Y.; Yee, J.; Gwak, H.-S. Effect of ITPA Polymorphism on Adverse Drug Reactions of 6-Mercaptopurine in Pediatric Patients with Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 416. https://doi.org/10.3390/ph15040416
Lee Y, Jang EJ, Yoon H-Y, Yee J, Gwak H-S. Effect of ITPA Polymorphism on Adverse Drug Reactions of 6-Mercaptopurine in Pediatric Patients with Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(4):416. https://doi.org/10.3390/ph15040416
Chicago/Turabian StyleLee, Yeonhong, Eun Jeong Jang, Ha-Young Yoon, Jeong Yee, and Hye-Sun Gwak. 2022. "Effect of ITPA Polymorphism on Adverse Drug Reactions of 6-Mercaptopurine in Pediatric Patients with Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 4: 416. https://doi.org/10.3390/ph15040416
APA StyleLee, Y., Jang, E. J., Yoon, H. -Y., Yee, J., & Gwak, H. -S. (2022). Effect of ITPA Polymorphism on Adverse Drug Reactions of 6-Mercaptopurine in Pediatric Patients with Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis. Pharmaceuticals, 15(4), 416. https://doi.org/10.3390/ph15040416