
Antihyperglycemic Effects of Annona cherimola Miller and the Flavonoid Rutin in Combination with Oral Antidiabetic Drugs on Streptozocin-Induced Diabetic Mice

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Acute Antihyperglycemic Effects of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
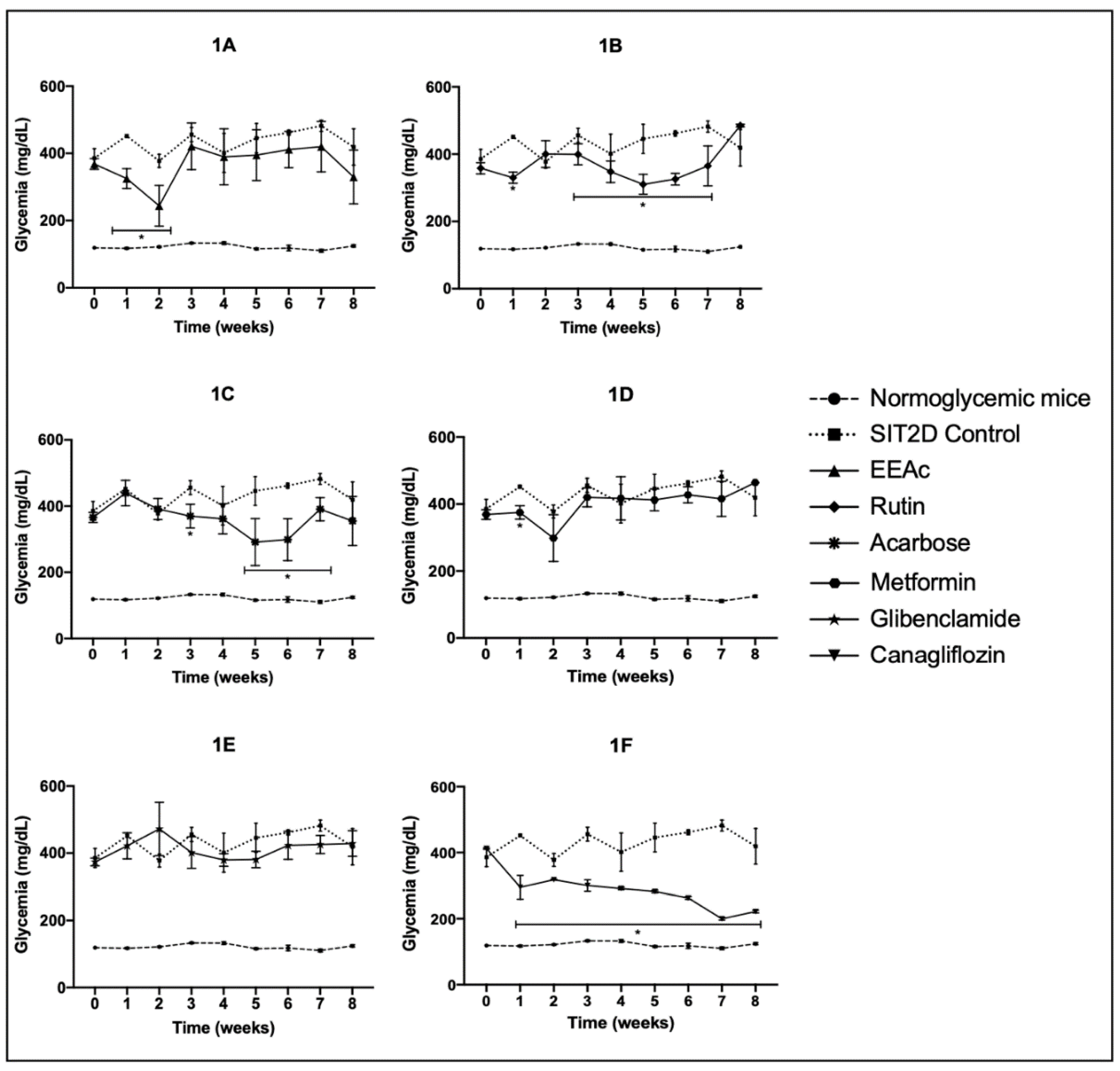
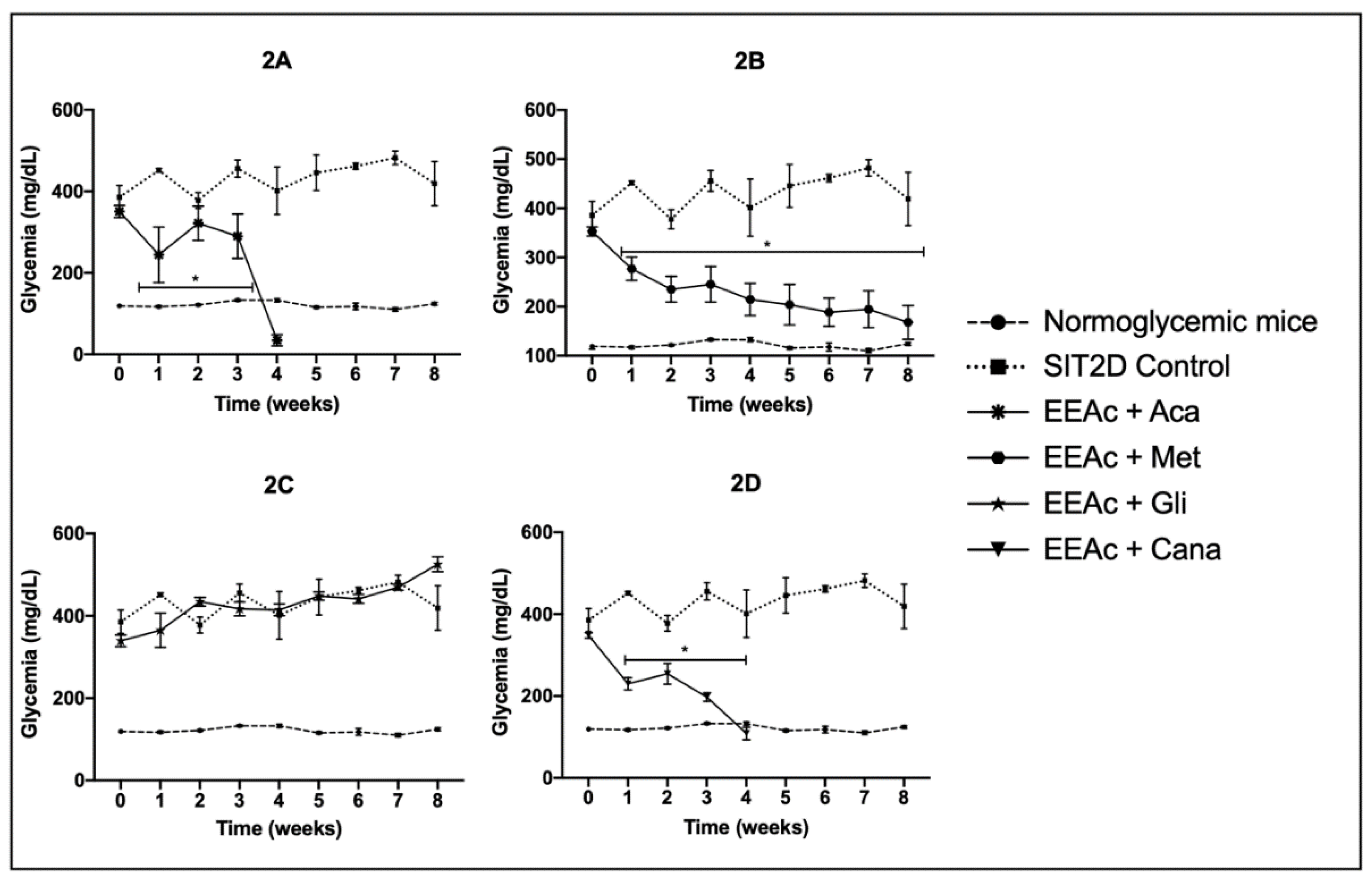
2.2. Subchronic Effects of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
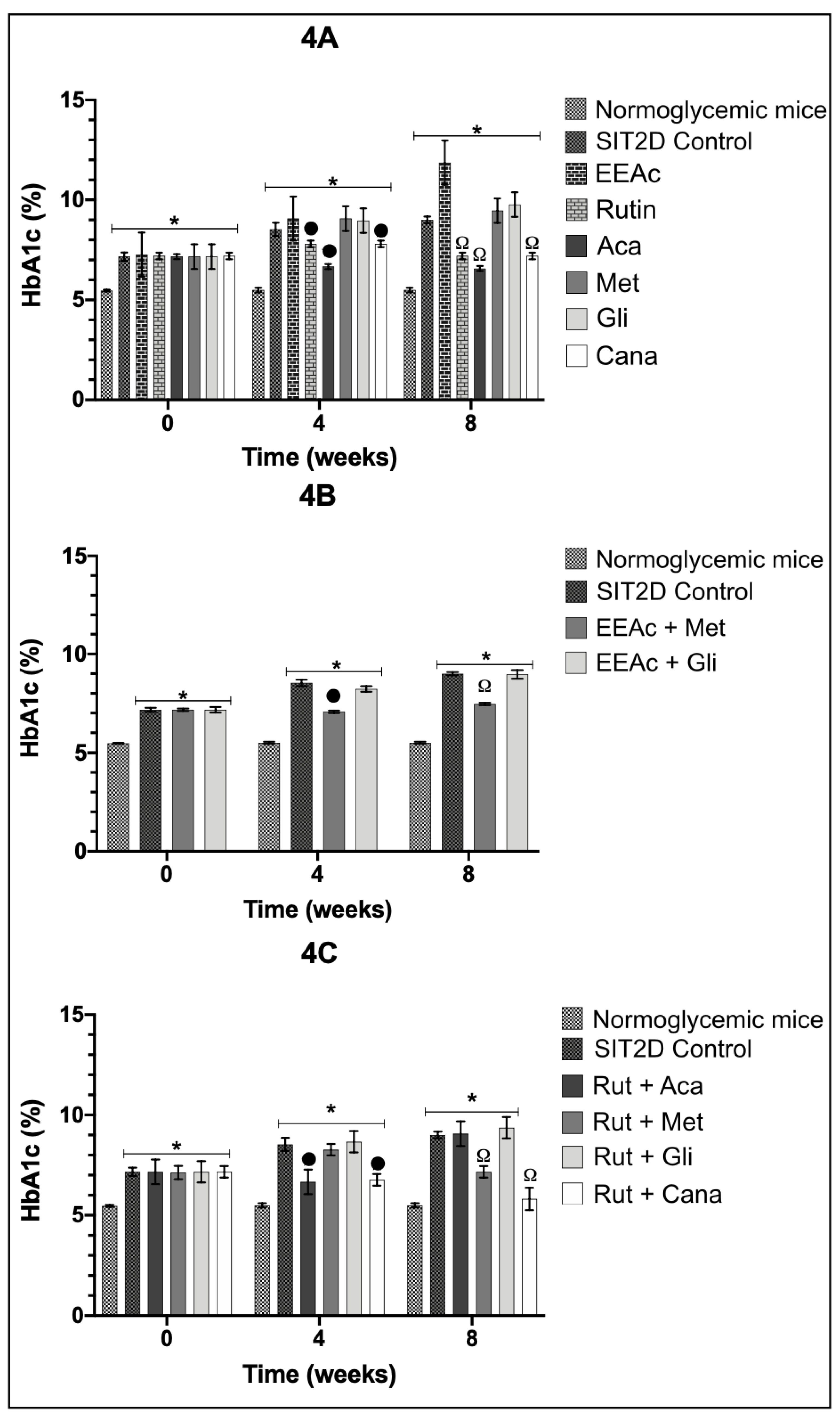
2.3. Effects over Glycated Hemoglobin Levels after Chronical Administration of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
2.4. Effects over Lipid Profile Levels after Chronical Administration of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
3. Discussion
4. Materials and Methods
4.1. Chemicals, Reagents and Drugs
4.2. Plant Material
4.3. Ethanolic Extract Preparation
4.4. Animals
4.5. Induction of Experimental Type 2 Diabetes
4.6. Grouping
4.6.1. Acute Evaluation of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
4.6.2. Subchronic Evaluation of Ethanolic Extract from Annona cherimola, Rutin, and Oral Antidiabetic Drugs on SIT2D Mice Model
4.6.3. % HbA1c Measurement
4.6.4. Lipid Profile Measurement
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guthrie, R.; Guthrie, D. Pathophysiology of diabetes mellitus. Crit. Care Nurs. Q. 2004, 27, 113–125. [Google Scholar] [CrossRef]
- International Diabetes Federation (IDF). Diabetes Atlas 9th Edition. Available online: https://www.diabetesatlas.org/en/ (accessed on 18 August 2022).
- World Health Organization. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 22 August 2022).
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes 2020. Diabetes Care 2021, 43, S14–S31. [Google Scholar]
- DeFronzo, R. From the Triumvirate to the Ominous Octet: A New Paradigm for the Treatment of Type 2 Diabetes Mellitus. Diabetes 2009, 58, 773–795. [Google Scholar] [CrossRef] [Green Version]
- Strain, W.; Paldánius, P. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc. Diabetol. 2018, 17, 57. [Google Scholar] [CrossRef] [Green Version]
- Maritin, A.; Sanders, R.; Watkins, J. Diabetes, oxidative stress, and antioxidants: A review. J. Biochem. Mol. Toxicol. 2003, 17, 24–38. [Google Scholar] [CrossRef]
- Gan, T.; Liao, B.; Xu, G. The clinical usefulness of glycated albumin in patients with diabetes and chronic kidney disease: Progress and challenges. J. Diabetes Complicat. 2018, 32, 876–884. [Google Scholar] [CrossRef]
- Kovatchev, B. Metrics for glycaemic control—From HbA1c to continuous glucose monitoring. Nat. Rev. Endocrinol. 2017, 13, 425–436. [Google Scholar] [CrossRef]
- Wong, N.; Nicholls, S.; Tan, J.; Bursill, C. The Role of High-Density Lipoproteins in Diabetes and Its Vascular Complications. Int. J. Mol. Sci. 2018, 19, 1680. [Google Scholar] [CrossRef] [Green Version]
- Association, A. Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S7–S13. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.; Mei, J.; Sim, Y. Type 1 and 2 diabetes mellitus: A review on current treatment approach and gene therapy as potential intervention. Diabetes Metab. Syndr. 2019, 13, 364–372. [Google Scholar] [CrossRef]
- Khursheed, R.; Singh, S.; Wadhwa, S. Treatment strategies against diabetes: Success so far and challenges ahead. Eur. J. Pharmacol. 2019, 862, 172625. [Google Scholar] [CrossRef] [PubMed]
- El-Tantawy, W.; Temraz, A. Management of diabetes using herbal extracts: Review. Arch. Physiol. Biochem. 2018, 124, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, P.; Howes, M.; Edwards, S. Medicinal plants used in the traditional management of diabetes and its sequelae in Central America: A review. J. Ethnopharmacol. 2016, 184, 58–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhury, H.; Pandey, M.; Hua, C. An update on natural compounds in the remedy of diabetes mellitus: A systematic review. J. Tradit. Complement. Med. 2017, 8, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Quilez, A.M.; Fernández-Arche, M.A.; García-Giménez, M.M.; De la Puerta, R. Potential therapeutic applications of the genus Annona Local and traditional uses and pharmacology. J. Ethnopharmacol. 2018, 225, 244–270. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Ramírez, N.; Calzada, F.; Alquisiras-Burgos, I. Antioxidant Properties and Protective Effects of Some Species of the Annonaceae, Lamiaceae, and Geraniaceae Families against Neuronal Damage Induced by Excitotoxicity and Cerebral Ischemia. Antioxidants 2020, 9, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larranaga, N.; Albertazzi, F.; Fontecha, G. A Mesoamerican origin of cherimoya (Annona cherimola Mill.): Implications for the conservation of plant genetic resources. Mol. Ecol. 2017, 26, 4116–4130. [Google Scholar] [CrossRef]
- Andrade-Cetto, A.; Heinrich, M. Mexican plants with hypoglycaemic effect used in the treatment of diabetes. J. Ethnopharmacol. 2005, 99, 325–348. [Google Scholar] [CrossRef]
- González, M. Chirimoya (Annona cherimola Miller), fruit-bearing tropical and sub-tropical of promissory values. Cul. Trop 2012, 34, 52–63. [Google Scholar]
- Calzada, F.; Correa-Basurto, J.; Barbosa, E.; Mendez-Luna, D.; Yepez-Mulia, L. Antiprotozoal Constituents from Annona cherimola Miller, a Plant Used in Mexican Traditional Medicine for the Treatment of Diarrhea and Dysentery. Pharmacogn. Mag. 2017, 13, 148–152. [Google Scholar]
- Martínez-Vázquez, M.; Estrada-Reyes, R.; Araujo, A. Antidepressant-like effects of an alkaloid extract of the aerial parts of Annona cherimolia in mice. J. Ethnopharmacol. 2012, 139, 164–170. [Google Scholar] [CrossRef]
- Ammoury, C.; Younes, M.; El-Khoury, M. The pro-apoptotic effect of a Terpene-rich Annona cherimola leaf extract on leukemic cell lines. BMC Complement. Altern. Med. 2019, 19, 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Solís, J.; Calzada, F.; Barbosa, E.; Valdés, M. Antihyperglycemic and Antilipidemic Properties of a Tea Infusion of the Leaves from Annona cherimola Miller on Streptozocin-Induced Type 2 Diabetic Mice. Molecules 2021, 9, 2408. [Google Scholar] [CrossRef]
- Díaz-de-Cerio, E.; Aguilera-Saez, L.; Gómez-Caravaca, A. Characterization of bioactive compounds of Annona cherimola L. leaves using a combined approach based on HPLC-ESI-TOF-MS and NMR. Anal. Bioanal. Chem. 2018, 410, 3607–3619. [Google Scholar] [CrossRef] [PubMed]
- Mannino, G.; Gentile, C.; Porcu, A.; Agliassa, C.; Caradonna, F.; Bertea, C. Chemical Profile and Biological Activity of Cherimoya (Annona cherimola Mill.) and Atemoya (Annona atemoya) Leaves. Molecules 2020, 25, 2612. [Google Scholar] [CrossRef] [PubMed]
- Calzada, F.; Solares-Pascasio, J.I.; Ordoñez-Razo, R.M.; Velázquez, C.; Barbosa, E.; García-Hernández, N. Antihyperglucemic Activity of the leaves from Annona chermiola Miller on Alloxan-induced Diabetic Rats. Pharmacogn. Res. 2017, 9, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asgharpour, F.; Pouramir, M.; Khalilpour, A.; Asgharpour, A.; Rezaei, M. Antioxidant activity and glucose diffusion relationship of traditional medicinal antihyperglycemic plant extracts. Int. J. Mol. Cell Med. 2013, 2, 169–176. [Google Scholar] [PubMed]
- Jo, S.; Ka, E.; Lee, H.; Apostolidis, E.; Jang, H.-D.; Kwon, Y.-I. Comparison of Antioxidant Potential and Rat intestinal α-Glucosidases inhibitory Activities of Quercetin, Rutin, and Isoquercetin. Int. J. Appl. Res. Nat. Prod. 2009, 2, 52–60. [Google Scholar]
- Sharma, S.; Ali, A.; Ali, J.; Sahni, J.; Baboota, S. Rutin: Therapeutic potential and recent advances in drug delivery. Expert Opin. Investig. Drugs 2013, 22, 1063–1079. [Google Scholar] [CrossRef]
- Ghorbani, A. Mechanisms of antidiabetic effects of flavonoid rutin. Biomed Pharmacother. 2017, 96, 305–312. [Google Scholar] [CrossRef]
- Verma, A.; Kumar, A.; Shekar, R.; Kumar, K.; Chakrapani, R. Pharmacological Screening of Annona cherimola for Antihyperlipidemic Potential. J. Basic Clin. Pharm. 2011, 2, 63–69. [Google Scholar] [PubMed]
- Wada, J.; Makino, H. Inflammation and the pathogenesis of diabetic nephropathy. Clin. Sci. 2013, 124, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, N.; Aung, T.; Madeiros, F. The Pathophysiology and Treatment of Glaucoma. JAMA 2014, 18, 1901–1911. [Google Scholar]
- Brajendra, K.; Arvind, K. Diabetes mellitus: Complications and therapeutics. Med. Sci. Monit 2006, 7, RA130–RA147. [Google Scholar]
- Oki, J. Dyslipidemias in Patients with Diabetes Mellitus: Classification and Risks and Benefits of Therapy. Pharmacotherapy 1995, 3, 317–337. [Google Scholar]
- Valdés, M.; Calzada, F.; Mendieta-Wejebe, J. Structure-activity relationship study of acyclic terpenes in blood glucose levels: Potential α-glucosidase and sodium glucose cotransporter (SGLT-1) inhibitors. Molecules 2019, 24, 4020. [Google Scholar] [CrossRef] [Green Version]
- Hsu, J.; Wu, C.; Hung, C.; Wang, C.; Huang, H. Myrciaria cauliflora extract improves diabetic nephropathy via suppression of oxidative stress and inflammation in streptozotocin-nicotinamide mice. J. Food Drug Anal. 2016, 24, 730–737. [Google Scholar] [CrossRef]
- Mata, R.; Sol, C.; Sonia, E.; Krzkaya, J.; Rivero, C. Mexican antidiabetic herbs: Valuable sources of inhibitors of a-glucosidases. J. Nat. Prod. 2013, 3, 468–483. [Google Scholar] [CrossRef]
- Kanter, M.; Aktas, C.; Erborga, M. Protective effects of quercetin against apoptosis and oxidative stress in streptozocin-induced diabetic rat testis. Food Chem. Toxicol. 2012, 50, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Chua, L.S. A review on plant-based rutin extraction methods and its pharmacological activities. J. Ethnopharmacol. 2013, 150, 805–817. [Google Scholar] [CrossRef]
- Chaudhury, A.; Duvoor, C.; Reddy, V.; Kraleti, S.; Chada, A.; Ravilla, R.; Marco, A.; Shekhawat, N.; Montales, M.; Kuriakose, K.; et al. Clinical Review of Antidiabetic Drugs: Implications for Type 2 diabetes Mellitus Management. Front. Endocrinol. 2017, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, E.; Schen, J. Canagliflozin: A Reviewin Type 2 Diabetes. Adis Drug Eval. 2017, 77, 1577–1592. [Google Scholar] [CrossRef] [PubMed]
- Valdés, M.; Calzada, F.; Mendieta-Wejebe, J.; Merlín-Lucas, V.; Velázquez, C.; Barbosa, E. Antihyperglycemic Effects of Annona diversifolia Safford and Its Acyclic Terpenoids: α-Glucosidase and Selective SGLT1 Inhibitiors. Molecules 2020, 25, 3361. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Barden, A.; Mori, T.; Bellin, L. Advanced glycation end-products: A review. Diabetologia 2001, 44, 129–146. [Google Scholar] [CrossRef] [Green Version]
- Snelson, M.; Coughlan, M. Dietary Advanced Glycation End Products: Digestion, Metabolism and Modulation of Gut Microbial Ecology. Nutrients 2019, 2, 215. [Google Scholar] [CrossRef] [Green Version]
- Falé, P.; Ferreira, C.; Maruzzella, F.; Florêncio, M.; Farazâo, F.; Serralheiro, M. Evaluation of cholesterol absorption and biosynthesis by decoctions of Annona cherimola leaves. J. Ethnopharmacol. 2013, 150, 718–723. [Google Scholar] [CrossRef]
- Miranda-Pérez, M.; Ortega-Camarillo, C.; Escobar-Villanueva, M.; Blancas-Flores, G.; Alarcon-Aguilar, F. Cucurbita fiicifolia Bouché increases insulin secretion in RINm5F cells through an influx of Ca2+ from the endoplasmic reticulum. J. Ethnopharmacol. 2016, 188, 159–166. [Google Scholar] [CrossRef]
- Un, J.; Mi-Kyung, L.; Yong, B.; Mi, A.; Myung-Sook, C. Effect of citrus flavonoids on lipid metabolism and glucose-regulating enzyme mRNA levels in type-2 diabetic mice. Int. Biochem. Cell Biol. 2006, 38, 1134–1145. [Google Scholar]
- Stee, M.; Graaf, A.; Groen, A. Actions of Metformin and statins on lipid and glucose metabolism and possible benefit of combination therapy. Cardiovasc. Diabetol. 2018, 17, 94. [Google Scholar] [CrossRef]
- Duncan, M.; Alkizim, F. Complementary and alternative medicine for type 2 diabetes mellitus: Role of medicinal herbs. J. Diabetes Endocrinol. 2012, 3, 44–56. [Google Scholar]
- Calzada, F.; Valdés, M.; García-Hernández, N.; Velázquez, C.; Barbosa, E.; Bustos-Brito, C.; Quijano, L.; Pina-Jimenez, E.; Mendieta-Wejebe, J. Antihyperglycemic activity of the leaves from Annona diversifolia Safford. and farnesol on normal and alloxan-induced diabetic mice. Phcog. Mag. 2019, 15, S5–S11. [Google Scholar]
- Norma Oficial Mexicana (NOM). Especificaciones Técnicas Para la Producción, Cuidado y Uso de los Animales de Laboratorio. Available online: https://www.fmvz.unam.mx/fmvz/principal/archivos/062ZOO.PDF (accessed on 12 July 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Glycemia (mg/dL) | ||
|---|---|---|---|
| 0 h | 2 h | 4 h | |
| NM Control | 119 ± 5.2 | 132 ± 3.8 | 135 ± 4.1 |
| SIT2D Control | 385.7 ± 28.4 | 404.3 ± 15.3 | 404.7 ± 9.6 |
| EEAc | 368.3 ± 16 | 230 ± 15.9 *,ψ | 342 ± 3.3 ψψ |
| Rut | 358 ± 7.9 | 323 ± 6.6 *,ψ | 266.3 ± 14.4 *,ψψ |
| Aca | 365.7 ± 15 | 302.6 ± 21.9 *,ψ | 283.7 ± 10.3 * |
| Met | 368 ± 14.3 | 388 ± 15.9 * | 363.6 ± 12.6 |
| Gli | 373.7 ± 11.4 | 267.5 ± 30.3 *,ψ | 353 ± 3.4 ψψ |
| Cana | 412.3 ± 2.2 | 242 ± 28.5 *,ψ | 257.3 ± 46.3 *,ψψ |
| EEAc + Aca | 350.7 ± 14.9 | 212.9 ± 36.7 *,ψ | 219.4 ± 35.9 *,ψψ |
| EEAc + Met | 353 ± 9.3 | 178.3 ± 12.7 *,ψ | 156 ± 6 *,ψψ |
| EEAc + Glib | 339.3 ± 14.2 | 145.7 ± 24.3 *,ψ | 202 ± 42.3 *,ψψ |
| EEAc + Cana | 348 ± 6.5 | 140 ± 48.5 *,ψ | 135.3 ± 51 *,ψψ |
| Rut + Aca | 340 ± 13.4 | 311.2 ± 19.4 | 250.7 ± 28.9 *,ψψ |
| Rut + Met | 326 ± 8.4 | 366.7 ± 38.3 | 327.7 ± 34.7 ψψ |
| Rut + Glib | 316.3 ± 5.2 | 317.7 ± 9.1 | 272.4 ± 9.8 *,ψψ |
| Rut + Cana | 337 ± 17.3 | 103.7 ± 9.4 *,ψ | 117.7 ± 2.5 *,ψψ |
| Treatment | Parameter | ||||
|---|---|---|---|---|---|
| Chol (mg/dL) | Tri (mg/dL) | HDL-c (mg/dL) | LDL-c (mg/dL) | AIP | |
| NM Control | 92 ± 1 ♦ | 88.9 ± 0.2 ♦ | 62.9 ± 0.7 ♦ | 79.4 ± 1.1 | 1.46 ± 0.02 |
| SIT2D Control | 163.7 ± 7.1 * | 127 ± 5.5 * | 29.9 ± 1 * | 157.7 ± 6.9 * | 5.4 ± 0.04 * |
| EEAc | 113 ± 8.8 ♦ | 65.9 ± 4.6 ♦ | 111 ± 9.5 *,♦ | 90.7 ± 6.9 ♦ | 1.02 ± 0.008 *,♦ |
| Rut | 125 ± 3.3 *,♦ | 118 ± 8 ♦ | 91.9 ± 6.4 *,♦ | 107.4 ± 2 *,♦ | 1.3 ± 0.06 ♦ |
| Aca | 80.7 ± 2.1 ♦ | 201.7 ± 23.4 *,♦ | 78.9 ± 6.4 *,♦ | 64.9 ± 1.6 ♦ | 1.04 ± 0.07 ♦ |
| Met | 171 ± 9 * | 203.7 ± 18.1 *,♦ | 77.9 ± 7.3 *,♦ | 155.4 ± 7.6 * | 2.2 ± 0.09 *,♦ |
| Gli | 160 ± 4 * | 87 ± 7.5 ♦ | 86 ± 6.2 *,♦ | 142.6 ± 5.2 * | 1.8 ± 0.1 *,♦ |
| Cana | 98.9 ± 3 ♦ | 84.3 ± 2.6 ♦ | 64.9 ± 3.9 ♦ | 85.9 ± 2.2 ♦ | 1.5 ± 0.04 ♦ |
| Treatment | Parameter | ||||
|---|---|---|---|---|---|
| Chol (mg/dL) | Tri (mg/dL) | HDL-c (mg/dL) | LDL-c (mg/dL) | AIP | |
| NM Control | 92 ± 1 ♦ | 88.9 ± 0.2 ♦ | 62.9 ± 0.7 ♦ | 79.4 ± 1.1 | 1.46 ± 0.02 |
| SIT2D Control | 163.7 ± 7.1 * | 127 ± 5.5 * | 29.9 ± 1 * | 157.7 ± 6.9 * | 5.4 ± 0.04 * |
| EEAc + Met | 77 ± 2.4 ♦ | 240 ± 26.8 *,♦ | 78.6 ± 4.6 ♦ | 62.2 ± 1.5 ♦ | 0.99 ± 0.02 *,♦ |
| EEAc + Gli | 208 ± 13.2 *,♦ | 102 ± 5.9 *,♦ | 38.9 ± 9.8 * | 184 ± 11.2 *,♦ | 1.7 ± 0.03 *,♦ |
| Treatment | Parameter | ||||
|---|---|---|---|---|---|
| Chol (mg/dL) | Tri (mg/dL) | HDL-c (mg/dL) | LDL-c (mg/dL) | AIP | |
| NM Control | 92 ± 1 ♦ | 88.9 ± 0.2 ♦ | 62.9 ± 0.7 ♦ | 79.4 ± 1.1 | 1.46 ± 0.02 |
| SIT2D Control | 163.7 ± 7.1 * | 127 ± 5.5 * | 29.9 ± 1 * | 157.7 ± 6.9 * | 5.4 ± 0.04 * |
| Rut + Aca | 88.9 ± 1.1 ♦ | 81.9 ± 3.8 ♦ | 79.5 ± 3.8 *,♦ | 73 ± 0.6 ♦ | 1.1 ± 0.04 ♦ |
| Rut + Met | 163 ± 7.3 * | 69.9 ± 2.1 ♦ | 39.9 ± 3.3 | 155 ± 6.6 * | 4.1 ± 0.1 *,♦ |
| Rut + Gli | 114 ± 2.3 ♦ | 91.9 ± 5.3 ♦ | 72.9 ± 4.1 *,♦ | 99.3 ± 1.5 ♦ | 1.5 ± 0.05 ♦ |
| Rut + Cana | 110 ± 1.7 ♦ | 107 ± 3.9 ♦ | 94.9 ± 6.7 *,♦ | 90.9 ± 0.3 ♦ | 1.1 ± 0.06 ♦ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdes, M.; Calzada, F.; Martínez-Solís, J.; Martínez-Rodríguez, J. Antihyperglycemic Effects of Annona cherimola Miller and the Flavonoid Rutin in Combination with Oral Antidiabetic Drugs on Streptozocin-Induced Diabetic Mice. Pharmaceuticals 2023, 16, 112. https://doi.org/10.3390/ph16010112
Valdes M, Calzada F, Martínez-Solís J, Martínez-Rodríguez J. Antihyperglycemic Effects of Annona cherimola Miller and the Flavonoid Rutin in Combination with Oral Antidiabetic Drugs on Streptozocin-Induced Diabetic Mice. Pharmaceuticals. 2023; 16(1):112. https://doi.org/10.3390/ph16010112
Chicago/Turabian StyleValdes, Miguel, Fernando Calzada, Jesús Martínez-Solís, and Julita Martínez-Rodríguez. 2023. "Antihyperglycemic Effects of Annona cherimola Miller and the Flavonoid Rutin in Combination with Oral Antidiabetic Drugs on Streptozocin-Induced Diabetic Mice" Pharmaceuticals 16, no. 1: 112. https://doi.org/10.3390/ph16010112
APA StyleValdes, M., Calzada, F., Martínez-Solís, J., & Martínez-Rodríguez, J. (2023). Antihyperglycemic Effects of Annona cherimola Miller and the Flavonoid Rutin in Combination with Oral Antidiabetic Drugs on Streptozocin-Induced Diabetic Mice. Pharmaceuticals, 16(1), 112. https://doi.org/10.3390/ph16010112