
Stabilization of Acne Vulgaris-Associated Microbial Dysbiosis with 2% Supramolecular Salicylic Acid

 ,
, 

Abstract
:1. Introduction
2. Results
2.1. Total Lesion Count and GAGS Score Comparison before and after Treatment
2.2. Observation of Adverse Reactions
2.3. Metagenomic Results
2.4. Effect of 2% SSA Treatment on Microbial Diversity
2.4.1. Alpha Diversity
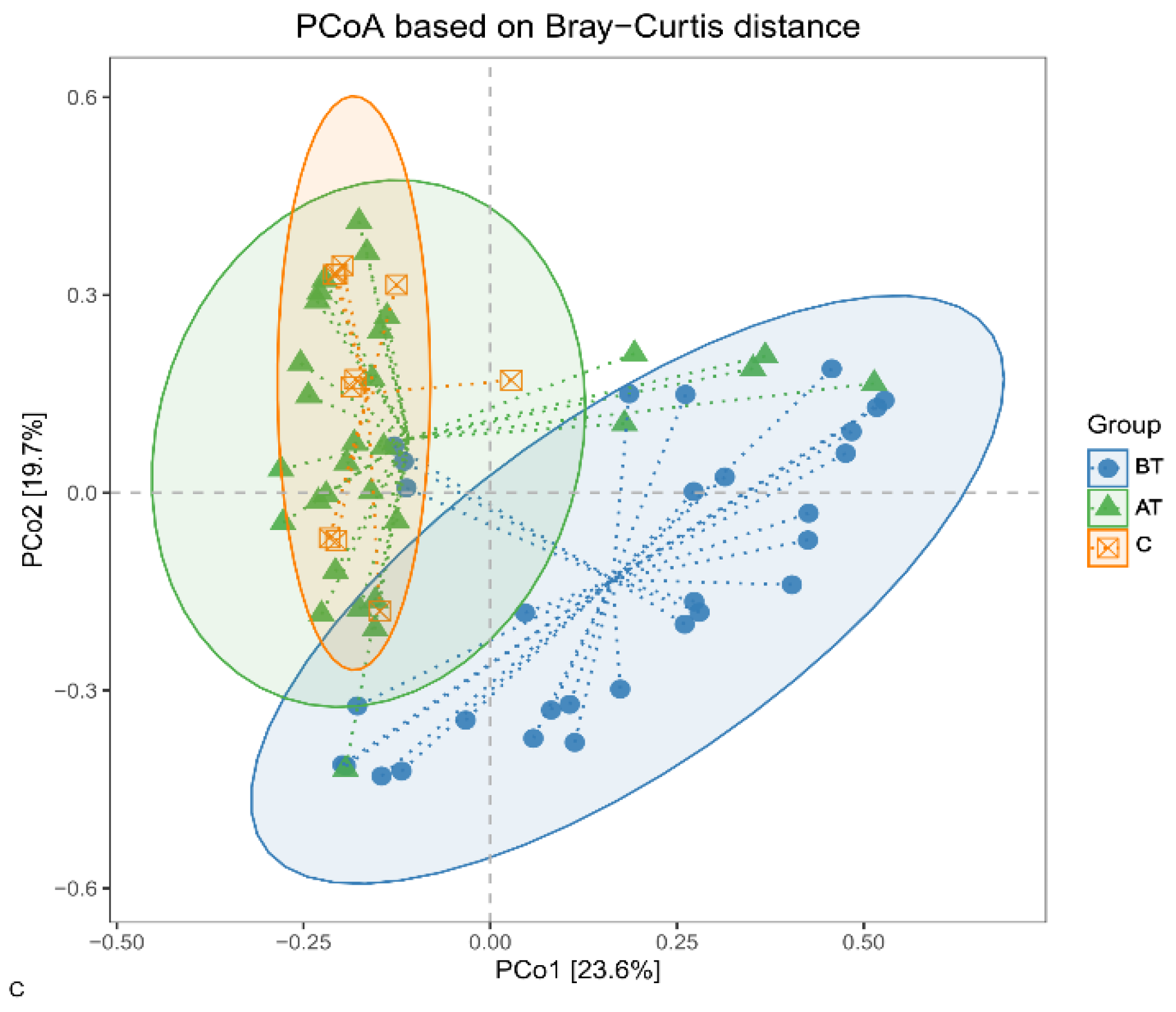
2.4.2. Beta Diversity
2.5. Effect of 2% SSA on Bacterial Communities
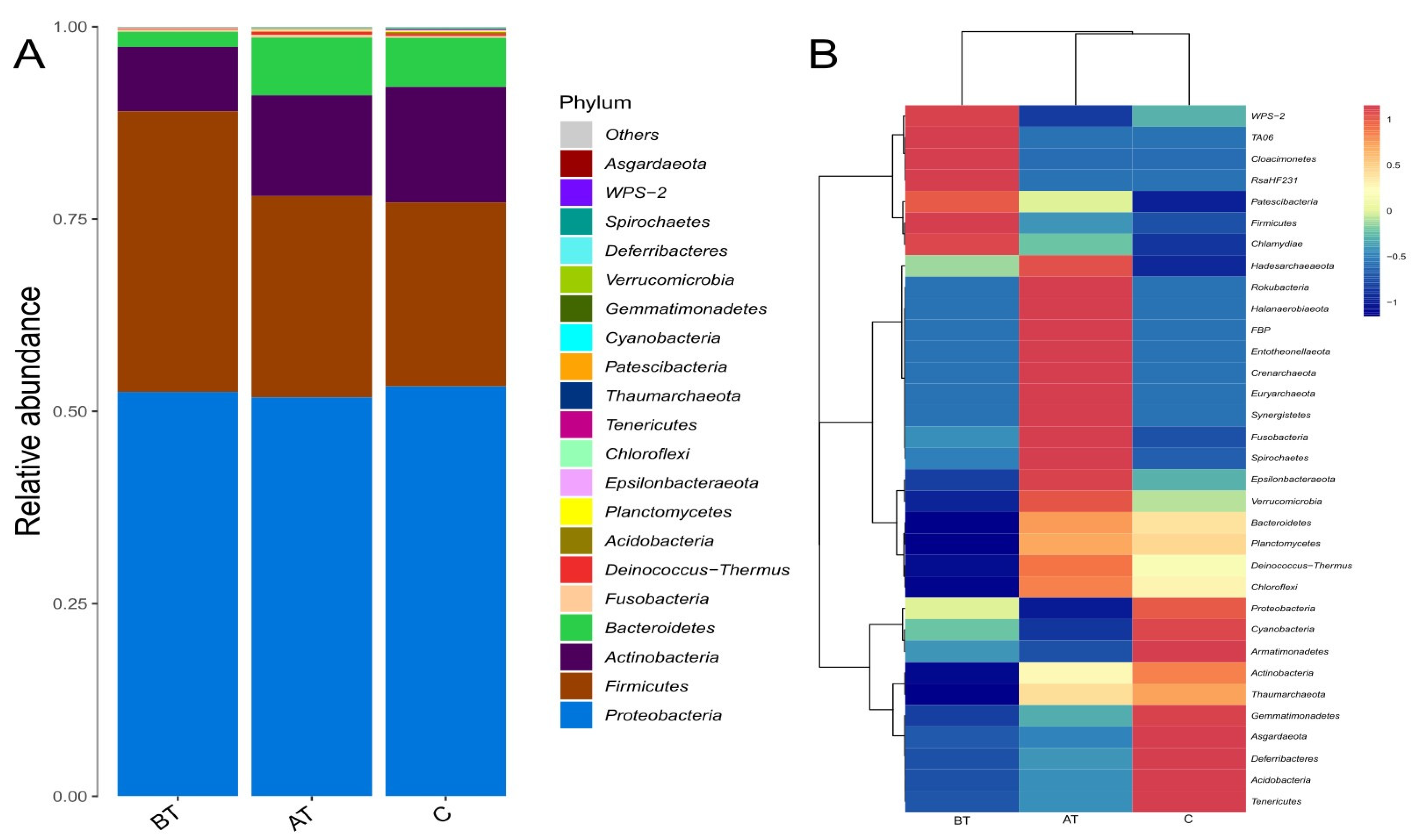
2.6. Diversity at the Phylum Level
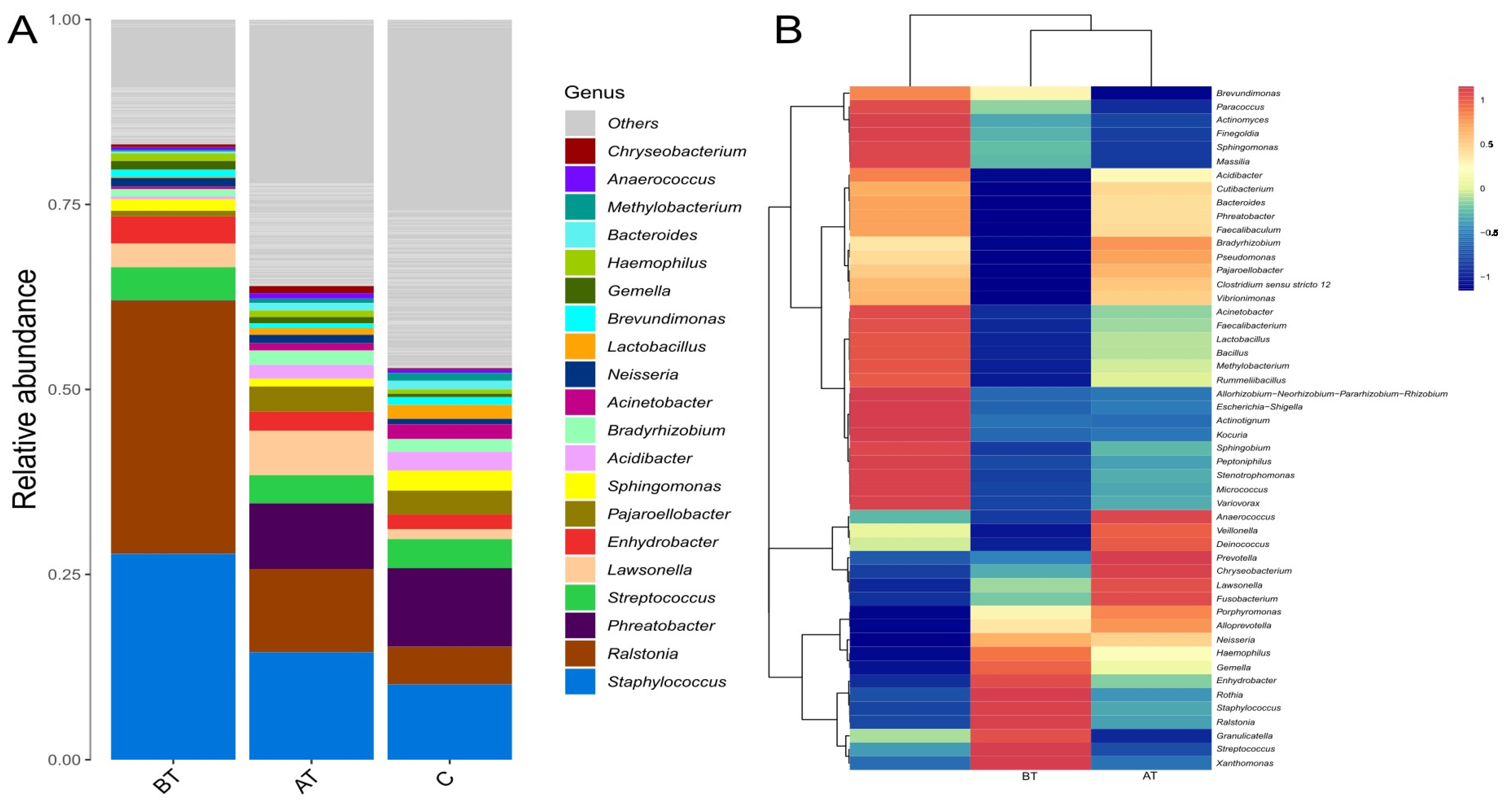
2.7. Diversity at the Genus Level
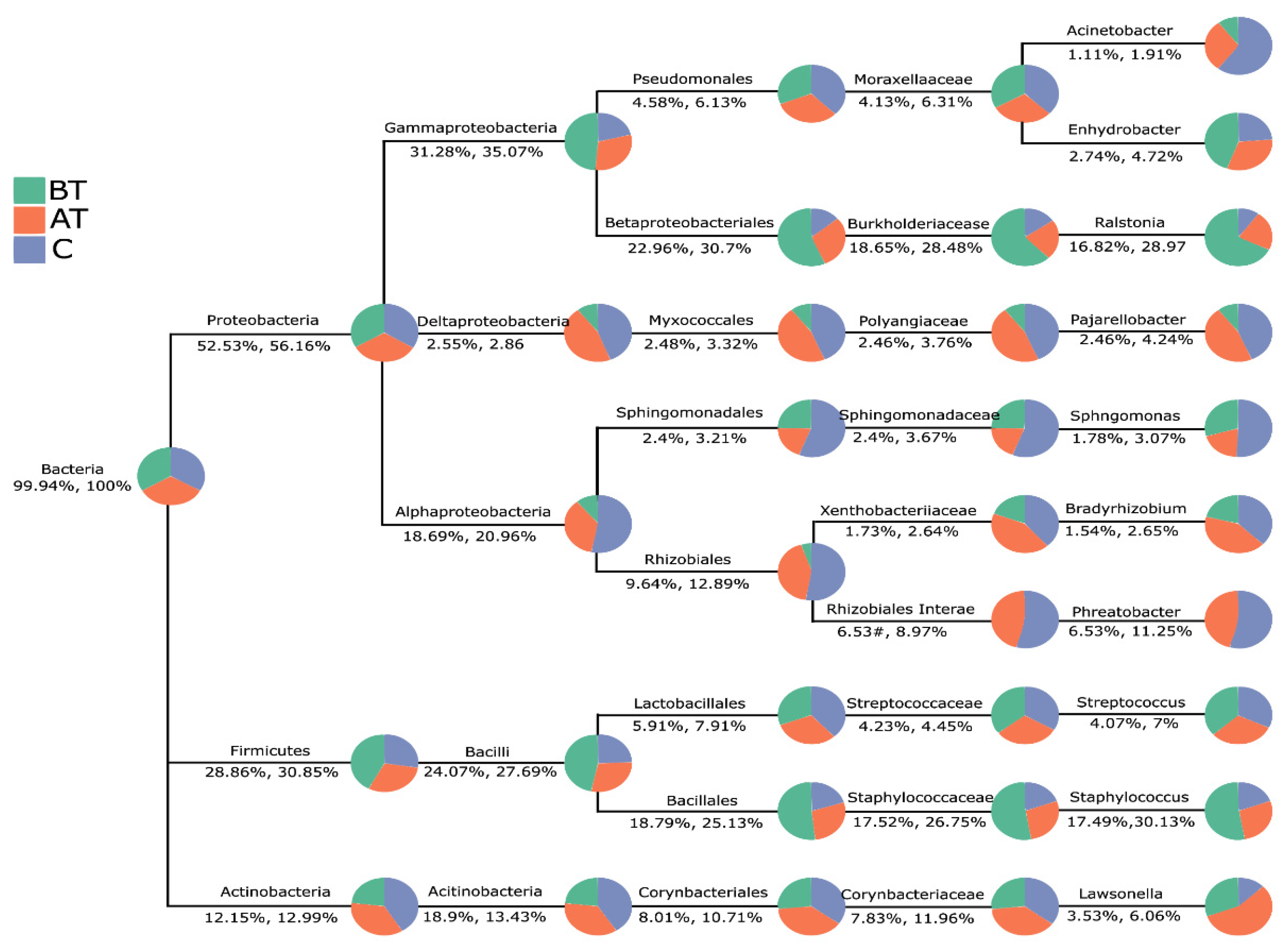
2.8. The Pattern of Microbiota Changes in Response to 2% SSA Treatment
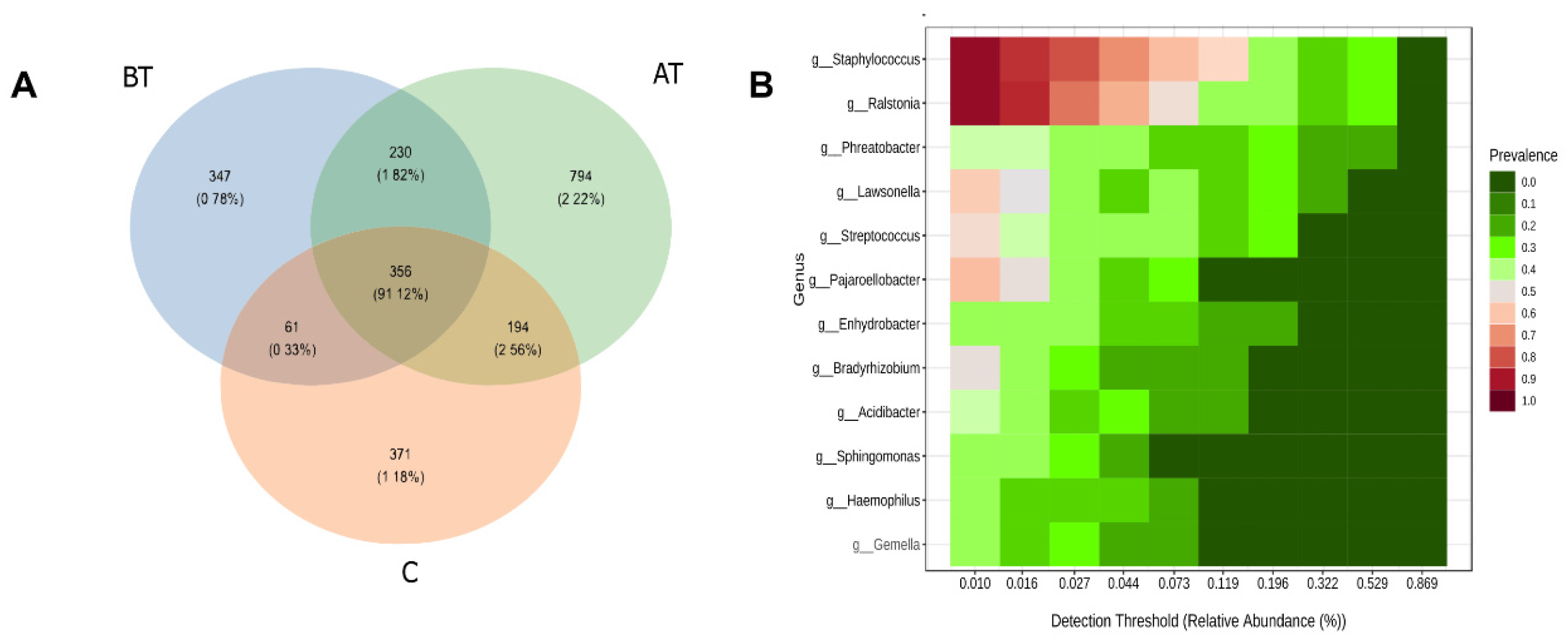
2.9. Core and Unique Microbiota
3. Discussion
4. Materials and Methods
4.1. Subject and Selection Criteria
4.2. Data and Samples Collection
4.3. The Amplified DNA Extraction, Amplification, and High-Throughput Sequencing
4.4. Data Analysis
4.5. Reference Standard
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parvizi, M.M.; Fatehi, N.; Jaladat, A.M.; Gholampour, Z.; Shahriarirad, R.; Erfani, A. Epidemiological factors in patients with dermatologic conditions referring to the clinic of traditional Persian Medicine: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14788. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Yin, S.; Xia, Y.; Chen, J.; Ye, C.; Zeng, Q.; Lai, W. Efficacy and safety of 2% supramolecular salicylic acid compared with 5% benzoyl peroxide/0.1% adapalene in the acne treatment: A randomized, split-face, open-label, single-center study. Cutan. Ocul. Toxicol. 2019, 38, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Liang, H.; Zhou, M.; Song, L.; He, C. Skin bacterial structure of young females in China: The relationship between skin bacterial structure and facial skin types. Exp. Dermatol. 2021, 30, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.U.; Schlosser, B.J.; Paller, A.S. A review of diagnosis and treatment of acne in adult female patients. Int. J. Women’s Dermatol. 2018, 4, 56–71. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.; Lim, J.; Zaenglein, A.L. Acne Vulgaris: Treatment Made Easy for the Primary Care Physician. Pediatr. Ann. 2020, 49, e109–e115. [Google Scholar] [CrossRef] [PubMed]
- van Steensel, M.A.M. Acne in the 21st century. Br. J. Dermatol. 2019, 181, 647–648. [Google Scholar] [CrossRef] [Green Version]
- Ochsendorf, F.R. Cutibacterium acnes in acne pathophysiology—The chicken or the egg? Br. J. Dermatol. 2019, 181, 657–658. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, S.; Barnard, E.; Dawson, T.L., Jr.; Li, H. The role of the skin microbiota in acne pathophysiology. Br. J. Dermatol. 2019, 181, 691–699. [Google Scholar] [CrossRef]
- Dréno, B.; Dagnelie, M.A.; Khammari, A.; Corvec, S. The Skin Microbiome: A New Actor in Inflammatory Acne. Am. J. Clin. Dermatol. 2020, 21, 18–24. [Google Scholar] [CrossRef]
- Sánchez-Pellicer, P.; Navarro-Moratalla, L.; Núñez-Delegido, E.; Ruzafa-Costas, B.; Agüera-Santos, J.; Navarro-López, V. Acne, Microbiome, and Probiotics: The Gut-Skin Axis. Microorganisms 2022, 10, 1303. [Google Scholar] [CrossRef]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Rusztowicz, M.; Nowicka, D. Efficacy of Oxybrasion in the Treatment of Acne Vulgaris: A Preliminary Report. J. Clin. Med. 2022, 11, 3824. [Google Scholar] [CrossRef] [PubMed]
- Chilicka, K.; Rusztowicz, M.; Rogowska, A.M.; Szyguła, R.; Asanova, B.; Nowicka, D. Efficacy of Hydrogen Purification and Cosmetic Acids in the Treatment of Acne Vulgaris: A Preliminary Report. J. Clin. Med. 2022, 11, 6296. [Google Scholar] [CrossRef] [PubMed]
- Ye, D.; Xue, H.; Huang, S.; He, S.; Li, Y.; Liu, J.; Wang, Z.; Zeng, W. A prospective, randomized, split-face study of concomitant administration of low-dose oral isotretinoin with 30% salicylic acid chemical peeling for the treatment of acne vulgaris in Asian population. Int. J. Dermatol. 2022, 61, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Al-Talib, H.; Al-Khateeb, A.; Hameed, A.; Murugaiah, C. Efficacy and safety of superficial chemical peeling in treatment of active acne vulgaris. An. Bras. De Dermatol. 2017, 92, 212–216. [Google Scholar] [CrossRef] [Green Version]
- Kligman, D.E.; Draelos, Z.D. Combination Superficial Peels With Salicylic Acid and Post-Peel Retinoids. J. Drugs Dermatol. 2016, 15, 442–450. [Google Scholar]
- Alsulaimani, H.; Kokandi, A.; Khawandanh, S.; Hamad, R. Severity of Acne Vulgaris: Comparison of Two Assessment Methods. Clin. Cosmet. Investig. Dermatol. 2020, 13, 711–716. [Google Scholar] [CrossRef]
- Doshi, A.; Zaheer, A.; Stiller, M.J. A comparison of current acne grading systems and proposal of a novel system. Int. J. Dermatol. 1997, 36, 416–418. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Holmes, S.P. Exact sequence variants should replace operational taxonomic units in marker-gene data analysis. ISME J. 2017, 11, 2639–2643. [Google Scholar] [CrossRef] [Green Version]
- Chua, W.; Poh, S.E.; Li, H. Secretory Proteases of the Human Skin Microbiome. Infect. Immun. 2022, 90, e0039721. [Google Scholar] [CrossRef]
- Skowron, K.; Bauza-Kaszewska, J.; Kraszewska, Z.; Wiktorczyk-Kapischke, N.; Grudlewska-Buda, K.; Kwiecińska-Piróg, J.; Wałecka-Zacharska, E.; Radtke, L.; Gospodarek-Komkowska, E. Human Skin Microbiome: Impact of Intrinsic and Extrinsic Factors on Skin Microbiota. Microorganisms 2021, 9, 543. [Google Scholar] [CrossRef]
- Ferček, I.; Lugović-Mihić, L.; Tambić-Andrašević, A.; Ćesić, D.; Grginić, A.G.; Bešlić, I.; Mravak-Stipetić, M.; Mihatov-Štefanović, I.; Buntić, A.M.; Čivljak, R. Features of the Skin Microbiota in Common Inflammatory Skin Diseases. Life 2021, 11, 962. [Google Scholar] [CrossRef] [PubMed]
- Dreno, B.; Martin, R.; Moyal, D.; Henley, J.B.; Khammari, A.; Seité, S. Skin microbiome and acne vulgaris: Staphylococcus, a new actor in acne. Exp. Dermatol. 2017, 26, 798–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, E.; Shi, B.; Kang, D.; Craft, N.; Li, H. Author Correction: The balance of metagenomic elements shapes the skin microbiome in acne and health. Sci. Rep. 2020, 10, 6037. [Google Scholar] [CrossRef] [Green Version]
- Bay, L.; Ring, H.C. Human skin microbiota in health and disease: The cutaneous communities’ interplay in equilibrium and dysbiosis: The cutaneous communities’ interplay in equilibrium and dysbiosis. APMIS Acta Pathol. Microbiol. Et Immunol. Scand. 2021, 130, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Dagnelie, M.A.; Corvec, S.; Saint-Jean, M.; Nguyen, J.M.; Khammari, A.; Dréno, B. Cutibacterium acnes phylotypes diversity loss: A trigger for skin inflammatory process. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2340–2348. [Google Scholar] [CrossRef] [PubMed]
- Li, C.X.; You, Z.X.; Lin, Y.X.; Liu, H.Y.; Su, J. Skin microbiome differences relate to the grade of acne vulgaris. J. Dermatol. 2019, 46, 787–790. [Google Scholar] [CrossRef]
- Kwon, M.S.; Lim, S.K.; Jang, J.Y.; Lee, J.; Park, H.K.; Kim, N.; Yun, M.; Shin, M.Y.; Jo, H.E.; Oh, Y.J.; et al. Lactobacillus sakei WIKIM30 Ameliorates Atopic Dermatitis-Like Skin Lesions by Inducing Regulatory T Cells and Altering Gut Microbiota Structure in Mice. Front. Immunol. 2018, 9, 1905. [Google Scholar] [CrossRef] [Green Version]
- Hertzman, R.J.; Deshpande, P.; Leary, S.; Li, Y.; Ram, R.; Chopra, A.; Cooper, D.; Watson, M.; Palubinsky, A.M.; Mallal, S.; et al. Visual Genomics Analysis Studio as a Tool to Analyze Multiomic Data. Front. Genet. 2021, 12, 642012. [Google Scholar] [CrossRef]
- Liu, C.; Du, M.X.; Abuduaini, R.; Yu, H.Y.; Li, D.H.; Wang, Y.J.; Zhou, N.; Jiang, M.Z.; Niu, P.X.; Han, S.S.; et al. Enlightening the taxonomy darkness of human gut microbiomes with a cultured biobank. Microbiome 2021, 9, 119. [Google Scholar] [CrossRef]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [Green Version]
- Shade, A.; Handelsman, J. Beyond the Venn diagram: The hunt for a core microbiome. Environ. Microbiol. 2012, 14, 4–12. [Google Scholar] [CrossRef]
- Lee, H.J.; Jeong, S.E.; Lee, S.; Kim, S.; Han, H.; Jeon, C.O. Effects of cosmetics on the skin microbiome of facial cheeks with different hydration levels. MicrobiologyOpen 2018, 7, e00557. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Mitra, R.; Maitra, A.; Gupta, S.; Kumaran, S.; Chakrabortty, A.; Majumder, P.P. Sebum and Hydration Levels in Specific Regions of Human Face Significantly Predict the Nature and Diversity of Facial Skin Microbiome. Sci. Rep. 2016, 6, 36062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichenfield, D.Z.; Sprague, J.; Eichenfield, L.F. Management of Acne Vulgaris: A Review. JAMA 2021, 326, 2055–2067. [Google Scholar] [CrossRef] [PubMed]
- Ramam, M. Skin: Clinical Dermatology. Indian J. Dermatol. Venereol. Leprol. 2020, 86, 468. [Google Scholar] [CrossRef]
- Clark, A.K.; Saric, S.; Sivamani, R.K. Acne Scars: How Do We Grade Them? Am. J. Clin. Dermatol. 2018, 19, 139–144. [Google Scholar] [CrossRef]
- Anantanawat, K.; Pitsch, N.; Fromont, C.; Janitz, C. High-throughput Quant-iT PicoGreen assay using an automated liquid handling system. BioTechniques 2019, 66, 290–294. [Google Scholar] [CrossRef] [Green Version]
- Katz, R.; Ahmed, M.A.; Safadi, A.; Abu Nasra, W.; Visoki, A.; Huckim, M.; Elias, I.; Nuriel-Ohayon, M.; Neuman, H. Characterization of fecal microbiome in biopsy positive prostate cancer patients. BJUI Compass 2022, 3, 55–61. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | BT | AT | t-Value | p-Value |
|---|---|---|---|---|
| Lesion count | 39.67 ± 7.18 | 25.90 ± 8.40 | 8.06 | <0.0001 |
| GAGS scoring | 14.20 ± 2.71 | 10.37 ± 3.12 | 7.95 | <0.0001 |
| Constituencies | Index | R-Value | p-Value |
|---|---|---|---|
| Anosim analysis | |||
| BT versus AT | Bray–Curtis | 0.289 | <0.001 |
| BT versus C | Bray–Curtis | 0.577 | <0.001 |
| AT versus C | Bray–Curtis | −0.028 | 0.6 |
| BT versus AT versus C | Bray–Curtis | 0.293 | <0.001 |
| perMANOVA analysis | |||
| BT versus AT | Bray–Curtis | 0.125 | <0.001 |
| BT versus C | Bray–Curtis | 0.173 | <0.001 |
| AT versus C | Bray–Curtis | 0.031 | 0.257 |
| BT versus AT versus C | Bray–Curtis | 0.150 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilal, H.; Xiao, Y.; Khan, M.N.; Chen, J.; Wang, Q.; Zeng, Y.; Lin, X. Stabilization of Acne Vulgaris-Associated Microbial Dysbiosis with 2% Supramolecular Salicylic Acid. Pharmaceuticals 2023, 16, 87. https://doi.org/10.3390/ph16010087
Bilal H, Xiao Y, Khan MN, Chen J, Wang Q, Zeng Y, Lin X. Stabilization of Acne Vulgaris-Associated Microbial Dysbiosis with 2% Supramolecular Salicylic Acid. Pharmaceuticals. 2023; 16(1):87. https://doi.org/10.3390/ph16010087
Chicago/Turabian StyleBilal, Hazrat, Yuanyuan Xiao, Muhammad Nadeem Khan, Jinyu Chen, Qian Wang, Yuebin Zeng, and Xinyu Lin. 2023. "Stabilization of Acne Vulgaris-Associated Microbial Dysbiosis with 2% Supramolecular Salicylic Acid" Pharmaceuticals 16, no. 1: 87. https://doi.org/10.3390/ph16010087
APA StyleBilal, H., Xiao, Y., Khan, M. N., Chen, J., Wang, Q., Zeng, Y., & Lin, X. (2023). Stabilization of Acne Vulgaris-Associated Microbial Dysbiosis with 2% Supramolecular Salicylic Acid. Pharmaceuticals, 16(1), 87. https://doi.org/10.3390/ph16010087