2.2. Formulation Developments without API
The formulation development procedure started with the preparation and evaluation of several formulations without cyanocobalamin. As shown in
Table 10, multiple formulations have been developed to investigate the effects of different components and technologies on the tablet properties.
Table 2 presents tablet weight, hardness, and disintegration time. Accordingly, successful formulas have been chosen in which the ideal disintegration time for sublingual tablets is less than three minutes [
18,
25]. All formulas with disintegration times less than one minute were considered successful [
26]. Cyanocobalamin was then added to the successful direct compression formulas to conduct additional tests to determine the best formula for our purpose.
During the tablet preparation using the molding method, a portion of acetonitrile was evaporated, and as a result, the concentration continuously increased. Accordingly, it was difficult to estimate, control, or calculate the concentration precisely and to prepare a homogeneous solution or suspension. Because of the volatility of acetonitrile, it was continuously separated from the mixture. We note that these tablets are very fragile and crumble when handled, and their surfaces are irregular because of the evaporation process (
Figure 2). As stated in a study by Rawas-Qalaji et al., mechanical properties are a challenge faced by this method, which is consistent with our results [
10] (P-737).
It was observed that an increase in the concentration of mucoadhesive polymers resulted in a prolonged disintegration time (
Table 2). The longer disintegration time was attributed to the increased viscosity resulting from the formation of a gel matrix on the tablet, which gradually eroded [
27,
28]. Furthermore, all formulations that achieved less than one minute disintegration times underwent preparation using direct compression or wet granulation methods. The direct compression method was selected as the preferred approach for completing the formulation process. It is simple, cost-effective, and requires fewer steps [
29,
30]. In conclusion, formulas 19, 21, 25, and 27–43 were selected for the next stage.
2.3. Formulation Developments with API
Based on the prior evaluations of prepared tablets without cyanocobalamin, the formulation development process was proceeded by incorporating the API into the formulations. Accordingly, numerous formulations have been developed to prepare cyanocobalamin mucoadhesive sublingual tablets (
Table 11).
Table 3 presents the prepared tablets’ weight, hardness, disintegration time, and residence time.
During the residence time test, it was observed that the EC and Carb polymers (formulas S1, S2, S3, S18, and S19) exhibited rapid swelling, followed by an explosion, resulting in a residence time of less than 6 min. On the other hand, HPMC, HPC, Eudragit, and XG (S4–S17 and S20) exhibited less swelling than the previous polymers, leading to a longer residence time. This is a normal outcome since excessive swelling can create a slippery mucilage, causing easy detachment from the mucosal surface [
14,
31,
32,
33].
The residence time of the preparation increases with increasing polymer concentration, as shown in
Table 3. This relationship is attributed to the characteristic behavior of the polymer. As the polymer concentration increased, more polymer chains penetrated the mucosal surface, leading to substantial mucoadhesive properties. This increase in mucoadhesion strength follows a certain trend until a critical concentration is reached [
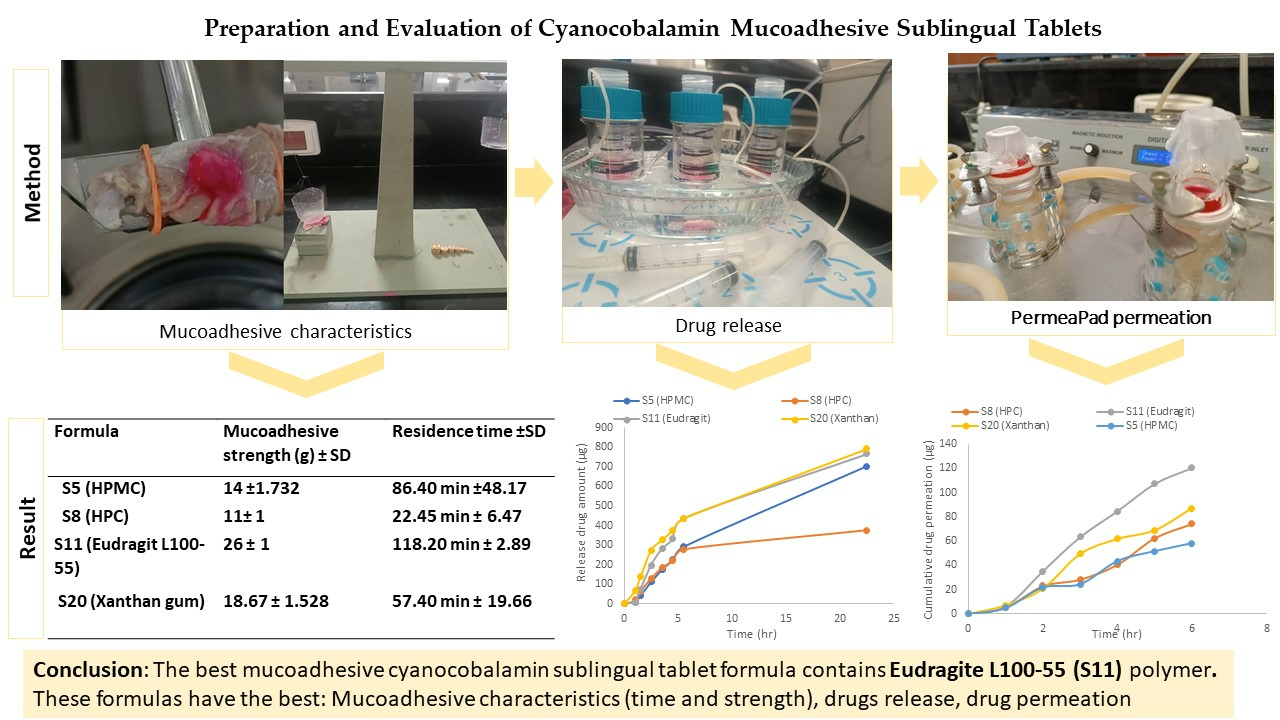
23]. Importantly, among these formulas, S5, S8, S11, and S20 demonstrated significantly longer residence times, exceeding 15 min. These formulas can be considered successful formulations owing to their extended residence times.
2.4. Evaluation of Mucoadhesive Sublingual Tablets
Based on the values presented in
Table 4, the blend exhibited excellent flow characteristics, as indicated by the angle of repose. Additionally, S5, S8, and S20 demonstrated good flow properties, while S11 showed a fair flowability characteristic, as determined by Carr’s index and Hauser ratio. This is related to the presence of a high percentage of microcrystalline cellulose, which exhibits excellent flow properties [
34].
The physical evaluations of the tablets are presented in
Table 5. The weight variation of all formulations was within the range of 49.935 ± 0.668- 50.53 ± 0.591 mg. The diameter and thickness were similar for all formulations except for S5, which contained HPMC polymers and had lower thickness. The average hardness of the formulations ranges from 4.28 to 4.94 kilopascal (KP), with all tablets exhibiting hardness values between 3 and 7. The friability percentage was <1%, ranging from 0.262 ± 0.060 to 0.480 ± 0.078. These results indicate that all formulations exhibit good mechanical properties, making them suitable for mechanical shipping and storage [
26,
35]. The assay confirmed the content uniformity, with values ranging from 93.508 ± 0.001 to 103.910 ± 0.004.
The surface pH test was conducted to assess the potential in vivo side effects associated with alkaline and acidic pH values, which may cause mucosal irritation. The target pH range was determined to be 6.2–7.6 in normal saliva, indicating a nearly neutral pH [
19,
24,
36]. The surface pH of the tablets fell between 5.350 ± 0.026 and 6.630 ± 0.010, with most tablets maintaining a relatively stable surface pH, except for S11, which showed a slight decrease in pH related to acidic properties of EL100-55 polymer [
34,
37]. None of the formulas caused irritation, as observed in vitamin B
12 buccal mucoadhesive films with a pH of 5.1 that did not exhibit any irritation [
38].
All formulations exhibited mucoadhesive strengths within the range of 11 ± 1 to 18.670 ± 1.528 g, representing the force required to detach the tablets from the mucosal layers. The mucoadhesive strength can be arranged in ascending order as follows: S8 < S5 < S20 < S11. Additionally, S11 containing EL100-55 demonstrated the longest mucoadhesive time, lasting 118.2 min in a previous result
Table 3.
As observed in
Table 3 and
Table 5, the S5 formula, containing HPMC, exhibited superior mucoadhesive characteristics in terms of strength and time compared to the S8 formula, which contained HPC polymer. The differences in mucoadhesive characteristics can be attributed to the swelling and viscosity of polymers [
39]. HPMC has a more complex structure than HPC, potentially contributing to superior mucoadhesive properties due to its higher viscosity, facilitating stronger interactions with the mucosal surface [
39,
40,
41]. The presence of hydroxypropyl and methoxyl groups alone increases the polymer’s hydrophilicity with a hydrophobic group. This structure allows for the formation of hydrophobic interactions in addition to fast wetting and spreading that promote the entanglement of polymer chains upon contact with the mucin surface [
40]. Additionally, HPMC possesses the ability to hold fluid within its structure through pores, forming a hydrogel that enhances its ability to form hydrogen bonds with mucin, the major component of mucus. These interactions promoted adhesion and prolonged the residence time of the formulation on the mucosal surface [
35,
42,
43].
The S20 formula (XG) demonstrates superior mucoadhesive characteristics compared to the S8 formula (HPC). The mucoadhesive properties of XG are primarily attributed to its charge, ionization, higher molecular weight, and wetting properties [
10,
21,
44]. XG is a water-soluble hydrophilic polymer that rapidly dissolves in hot and cold water, allowing the polymer chains to quickly diffuse into the mucosal surface. This fast diffusion and wetting process facilitates the creation of a strong interaction between the matrix and mucosa [
19,
44]. Additionally, the anionic nature of XG enhances its electrostatic interactions with mucin, making it a more potent mucoadhesive than HPC, a natural non-ionic polymer [
10,
21,
28,
45]. The high molecular weight of XG (2 × 10
6–20 × 10
6 Dalton) plays a crucial role in its mucoadhesive behavior. Research studies have indicated that polymers with molecular weights exceeding 100,000 generally demonstrate improved mucoadhesive properties. With molecular weights in the range mentioned above, XG exhibits an exceptional capacity for mucoadhesion [
23,
44].
The S11 formula, containing EL100-55, exhibits the best mucoadhesive characteristics. EL100-55 is an anionic, hydrophobic, and soluble polymer derived from acrylic and methacrylic acid. It demonstrates solubility at PH levels above 5.5, such as in saliva [
32,
37,
46]. Due to its anionic nature and charged properties, EL100-55 generates a stronger electrostatic interaction in comparison to natural non-ionic cellulose derivative polymers [
21]. Its mucoadhesive characteristics can be attributed to the presence of carboxylic acid groups in the polymer, which allows it to form strong hydrogen bonds that contribute to the adhesion to the mucin in the mucosa layer. Furthermore, the high molecular weight of EL100-55 with long polymer chains promotes entanglement within the mucus layer, increasing the overall adhesion between the polymer and mucosal surface [
23,
31].
2.5. Drug Release Test
Polysaccharide polymers, such as HPMC, EL100-55, XG, and HPC, are commonly employed to control drug release from polymer matrices. These polymers facilitate drug release through a dissolution process involving solvent diffusion and/or disentanglement of polymer chains [
47].
A comparison of the drug release profiles between the standard cyanocobalamin and the final formulas revealed that the standard cyanocobalamin exhibited detectable absorption after 15 min, whereas in samples S5, S8, and S11, the absorption was delayed until 1 h (
Figure 3 and
Figure 4). In the case of sample S20, the burst effect of the XG polymer resulted in the drug release being detected after 30 min. Therefore, the presence of the polymer in the tablets effectively retards the release of the drug from the tablet matrix [
28,
44]. Throughout the duration of this study (up to 23 h), the release of standard cyanocobalamin remained higher than the release of all samples. However, both the samples and the standard exhibited release percentages lower than 82.75% within this timeframe. This may be attributed to the loss of force that was responsible for transferring the drug from the donor to the acceptor compartment. Additionally, during the stability test conducted for standard cyanocobalamin in SSF at 37 °C, which mimicked the conditions of the drug release test, a loss of approximately 5.34% was observed.
Based on the results of the drug release mathematical kinetic models for the first 5.5 h (
Table 6,
Figure 5), the Peppas–Sahlin model exhibits the best fit to the kinetic release data, with R
2 values exceeding 0.99. Evidently, the drug release mechanisms in the final formulas involve Fickian and non-Fickian diffusion. The presence of mucoadhesive polymers plays a significant role in these release mechanisms.
According to the Peppas–Sahlin model results, the K1 constant represents the contribution of Fickian diffusion to drug release, whereas the K2 constant represents the contribution of non-Fickian (super Case II transport) release mechanisms, which are associated with polymer swelling, chain relaxation, and erosion.
As observed in
Table 6, drug release in all final formulas is controlled by the involvement of both the Fickian and non-Fickian release mechanism. In the case of the S5 formula (5% HPMC), it was observed that K
2 has a higher value than K
1 (which was negative), indicating the dominance of super Case II transport (polymer relaxation-swelling, chain relaxation, or erosion) during drug diffusion release [
48]. When the HPMC polymer matrix came into contact with the dissolution medium, the solvent diffused into the matrix, leading to the swelling of the polymer and hydration, resulting in the formation of a viscous gel. The drug release is controlled by diffusion, where the drug diffuses through the swollen polymer matrix following Fick’s law. Additionally, it was associated with more complex release patterns, including relaxation with the slow erosion of the HPMC polymer matrix. The presence of solid bridges formed between polymers and drugs supports sustained drug release over time [
49,
50].
For S8 (15% HPC), the hydrophilic nature of the polymer results in rapid hydration and swelling. The drug release from the polymer depends on pore formation and the erosion rate of the polymer, which is influenced by the concentration of the polymer and the resulting viscosity. The more viscous hydrophilic polymer leads to slower swelling and resistance to erosion processes, thereby retarding drug release. This behavior was observed in the drug release profile (
Figure 3) [
49,
50].
For S11 (15% EL 100-55), hydrophobic polymers (polymethacrylates) generate hydrogels that entrap the drug within them. When the hydrogels form, the drug is released from the adhesive polymers based on diffusion within the polymer chains, in accordance with Fick’s law. Concurrently, the entrapped drug is slowly released through polymer erosion and degradation, which follows a non-Fickian drug release pattern [
49,
51,
52].
S20 (0.5% XG) demonstrates Fickian diffusion with non-Fickian Case II transport. This is attributed to the swelling with the initial burst drug release effect and relaxation of XG, along with the drug diffusion through the hydrophilic polymeric matrix. As the concentration increases, the viscosity also increases, leading to retarded drug release [
53]. Moreover, XG and EL 100-55 have higher drug release than cellulose derivative polymers (HPMC and HPC) related to higher swelling properties, so more surface area is available for drug release [
21,
44,
53]. This behavior is supported by
Figure 3 and
Figure 6.
Based on the results obtained using the DD solver program within the initial 5.5 h for all formulations, it was observed that all formulations adhered to the Peppas–Sahlin model, exhibiting the highest R
2 values compared to alternative models. Consequently, the Peppas–Sahlin model equation was employed to accurately depict the fitting of these models, allowing us to predict the drug release behavior during this specific time frame.
Figure 6 shows the drug release profiles over the initial 5.5 h, representing the percentage of drug release. The calculated R
2 values from the fit line were as follows: HPMC = 0.9993, HPC = 0.9988, Eudragit L100-55 = 0.9974, and Xanthan = 0.9982. A higher R
2 value obtained from the fitted curve signifies a superior fit of the data and a stronger correlation between the Peppas–Sahlin model and our experimental findings, elucidating the drug release process’s involvement of both Fickian and non-Fickian mechanisms [
54].
2.6. PermeaPad® Permeation Result
The Permeapad
® membrane is an artificial biomimetic membrane commonly employed to investigate drug permeation from dosage forms. It is particularly relevant for studying the permeability of drugs through mucosal surfaces such as the buccal and gastrointestinal mucosa. The Permeapad
® membrane is designed with two supported hydrophilic sheets, and within it is a phospholipid layer “ sandwich structure,” which is formed using soy phosphatidylcholine (PC) S-100 [
55,
56]. The Permeapad
® membrane mimics the lipid composition and structure of biological membranes. This unique characteristic makes it highly suitable for reliably assessing passive drug permeation behavior and evaluating drug delivery systems [
57].
As shown in
Figure 7, the permeation of cyanocobalamin from S5 (HPMC) and S8 (HPC) was lower than that from S11 (EL100-55) and S20 (XG). This was consistent with the drug release profile shown in
Figure 4. The observed difference in permeation can be attributed to the varying amounts of drug available in the donor compartment for permeation through the Permeapad
® membrane.
By referring to the drug release profile in
Figure 4, it can be observed that S20 (XG) initially exhibits slightly higher drug release behavior during the first 5 h, after which the drug release profile becomes similar to that of S11 (EL100-55). This difference in the early drug release behavior could be attributed to a burst effect associated with the higher swelling of XG than that of EL100-55 [
53]. While the permeation test showed that S11 (EL100-55) had higher permeability than S20 (XG), this difference in drug permeability behavior can be attributed to several factors.
First, the higher viscosity of XG compared to that of EL100-55 may play a role; EL100-55 generally has a lower viscosity. The XG viscosity of KG tends to increase at higher pH values and in the presence of salts, such as NaCl or KCl, at elevated temperatures. On the other hand, EL100-55 exhibits solubility at pH values higher than 5.5. Changes in pH can affect the solubility and ionization of polymers [
44,
56]. Additionally, XG has more hydrophilic groups; for the drug to cross this membrane, it should possess a balance of lipophilic and hydrophilic properties that mimic the Permeapad
® membrane.
In contrast, EL100-55 is an amphiphilic methacrylic acid polymer, which contains both hydrophilic and hydrophobic groups with a higher affinity for cyanocobalamin (a weak base). These characteristics promote the migration of the soluble polymer from the SSF (pH 6.8) through the Permeapad
® membrane to PBS (pH 7.4) along with cyanocobalamin. Therefore, EL100-55 exhibits a better balance of these properties than XG, which may enhance the interaction and increase the permeability of cyanocobalamin from the EL100-55 matrix [
37,
44,
56,
58,
59,
60].
The bioavailability of S11 (Eudragit L100-55), estimated by the cumulative amount of drug passing through the Permeapad
® membrane into the donor compartment, is approximately 12.03%. When comparing this bioavailability with that of conventional oral dosage forms (1 mg) by passive diffusion, which typically has a bioavailability of 1.3%, it is evident that the cyanocobalamin mucoadhesive sublingual tablets formula in S11 is a promising approach to significantly increasing the bioavailability of cyanocobalamin and enhancing its therapeutic efficacy [
61,
62].
Table 7 presents the R
2 values for cyanocobalamin permeability, steady-state flux, and apparent permeability coefficient (
Papp) through the Permeapad
® membrane. Notably, the highest values for all parameters were observed for the S11 formula (EL 100-55). This indicates that S11 exhibits the highest cyanocobalamin permeability among the tested formulations. Specifically, the
Papp value of cyanocobalamin for S11 is approximately two-fold higher compared to S5, 1.6-fold higher for S8, and 1.38-fold higher for S20.
The
Papp values for all formulas are higher than 1.5 × 10
−6, with a standard deviation of less than 27%. These values indicate good permeability as they exceed the cut-off value for classifying permeability [
63]. However, it is important to note that the results of all drug permeation parameters consistently demonstrated that the permeation of S11 (EL100-55) was higher than that of S20 (XG) in the tested formulas. This conclusion is supported by the findings presented in
Figure 7 and
Table 7, which show higher permeation levels for S11 than for S20.



 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






