
A Treat-and-Extend Regimen of Intravitreal Brolucizumab for Exudative Age-Related Macular Degeneration Refractory to Aflibercept: A 12-Month Result

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Study Cohort
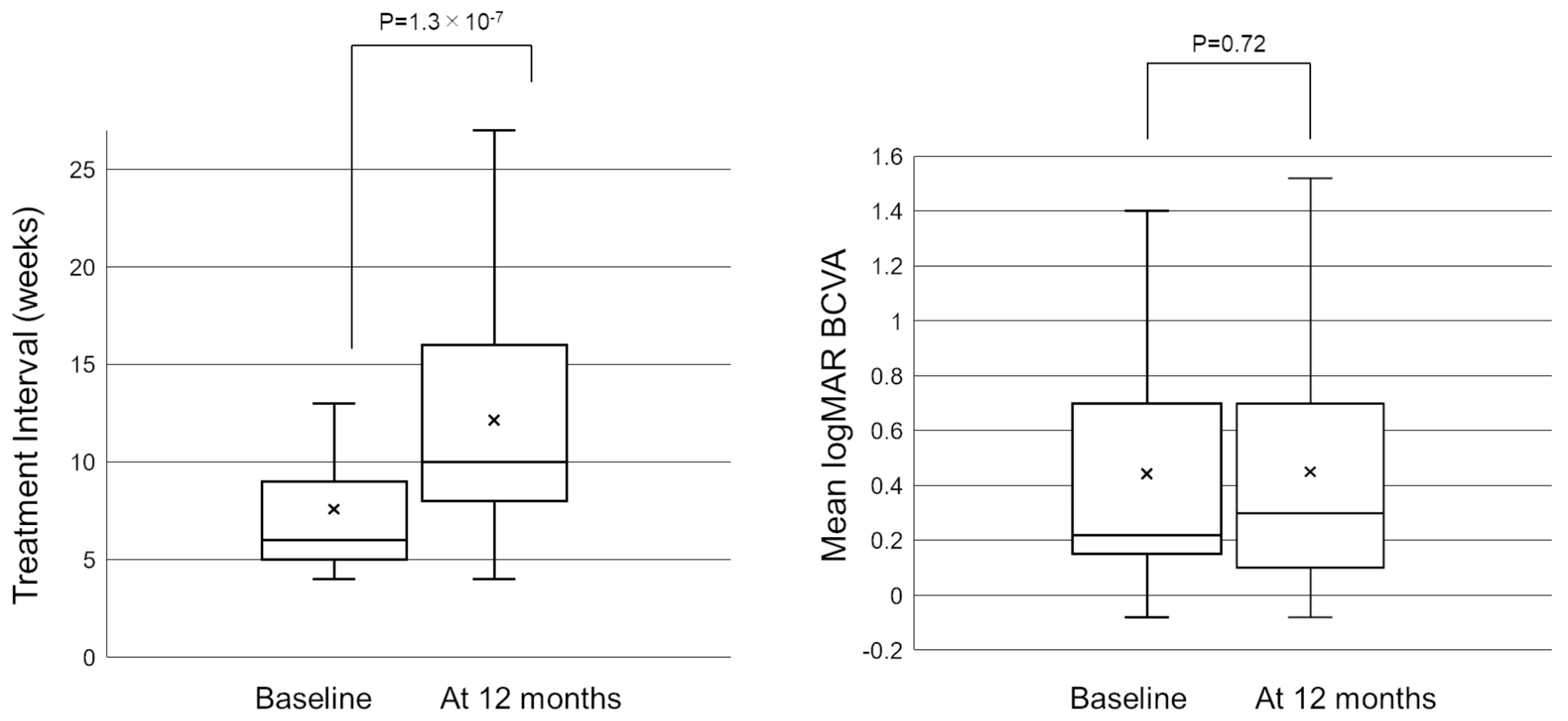
2.2. Treatment Interval
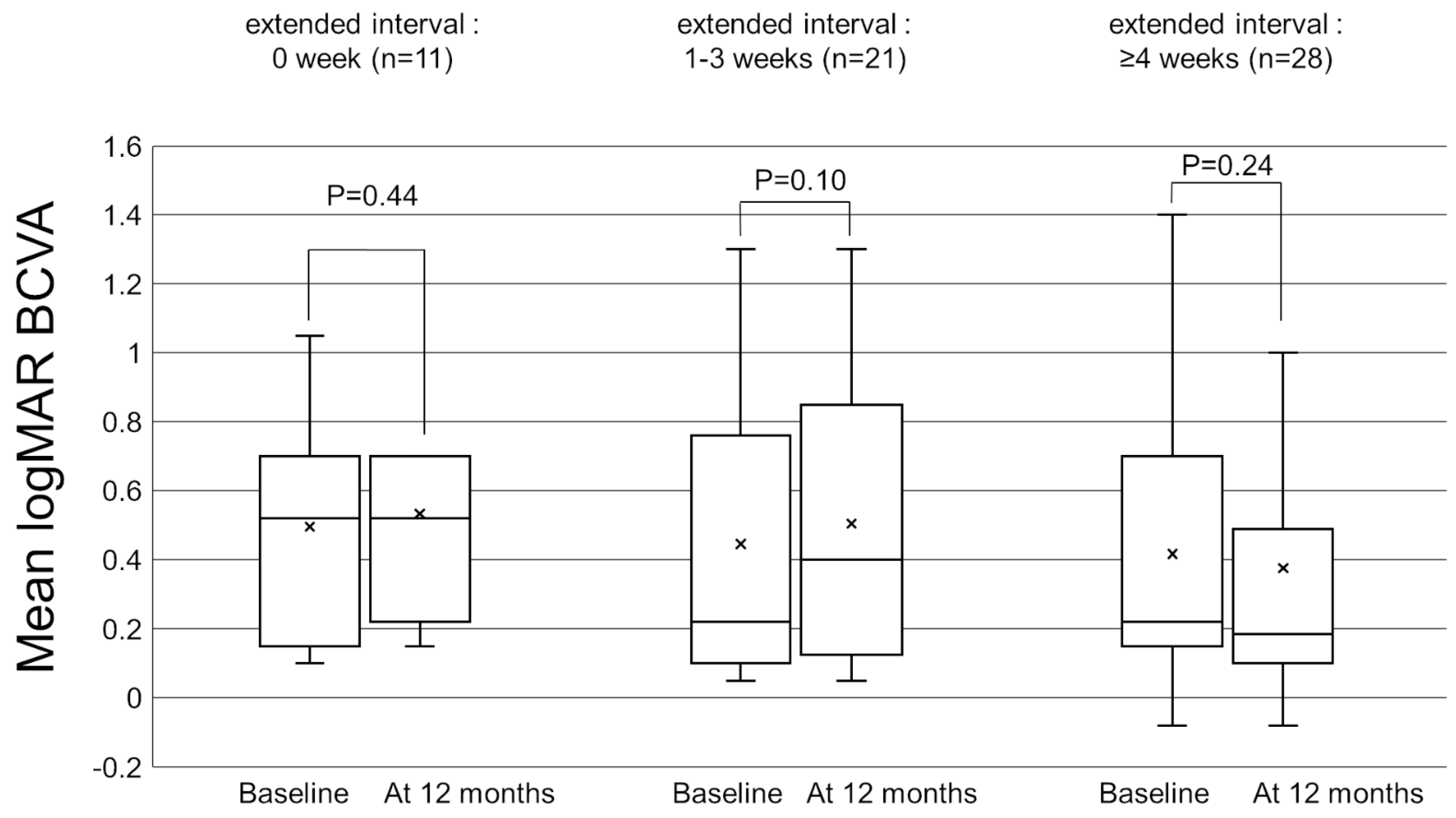
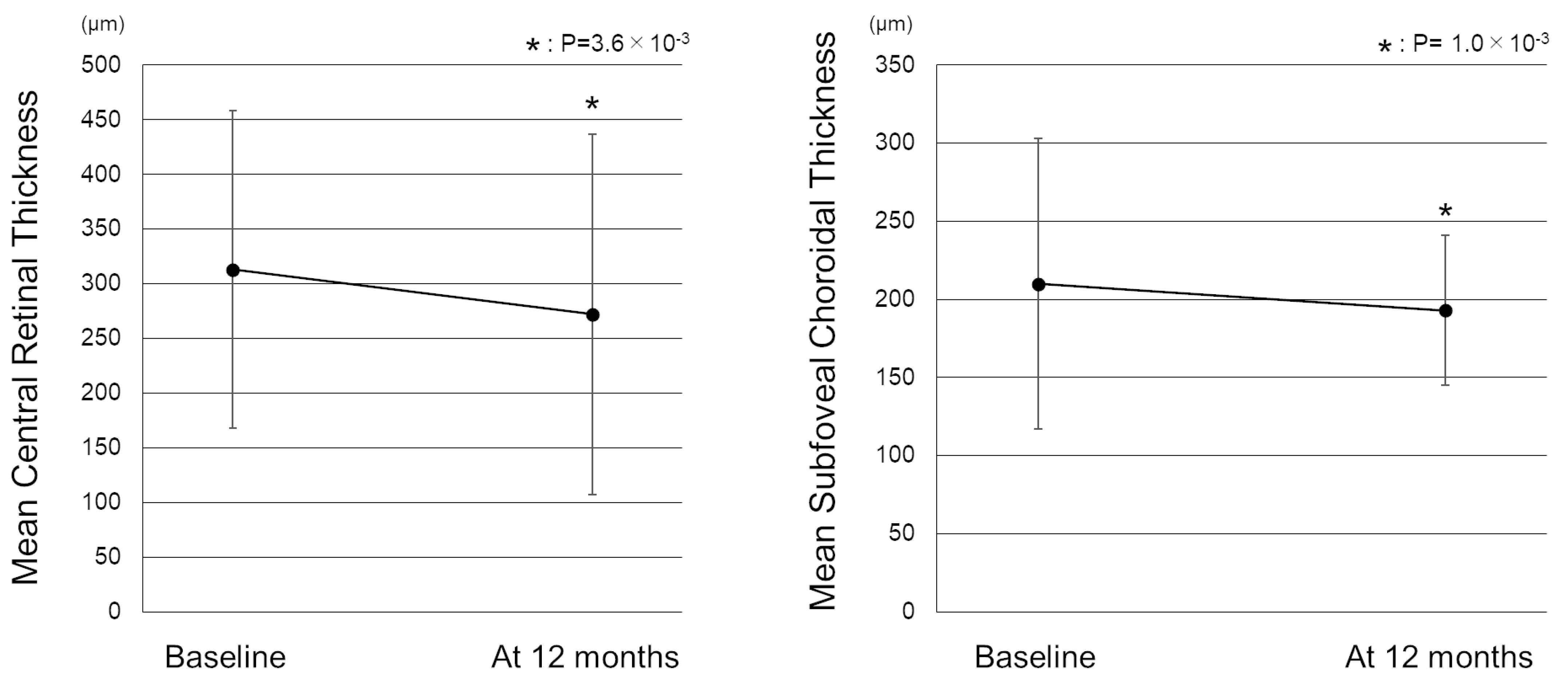
2.3. Visual and Anatomical Outcomes
2.4. Adverse Events
3. Discussion
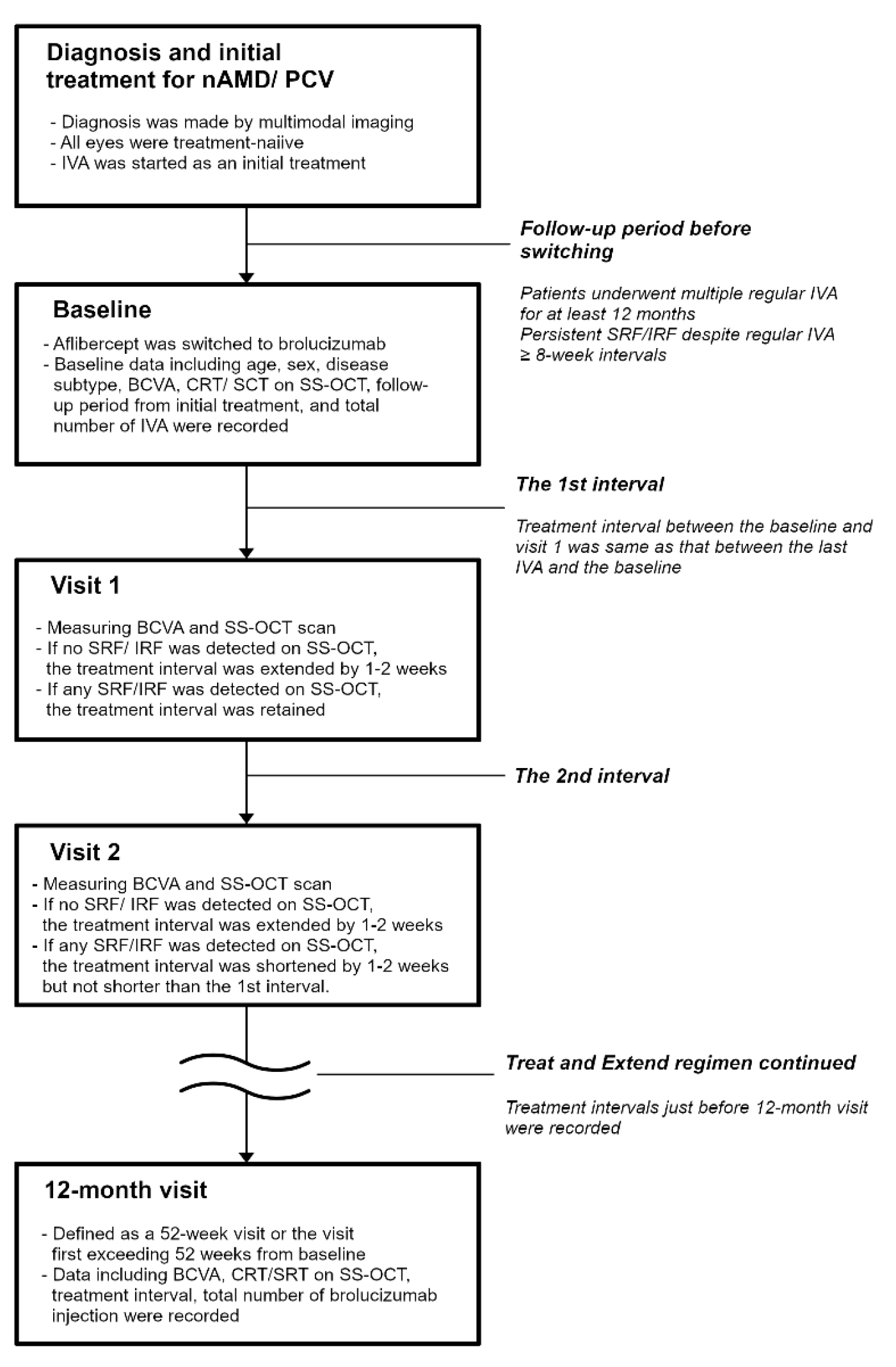
4. Materials and Methods
4.1. Participants
4.2. Diagnosis
4.3. A Treat-and-Extend Regimen
4.4. Follow-Up Examination
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kawasaki, R.; Yasuda, M.; Song, S.J.; Chen, S.J.; Jonas, J.B.; Wang, J.J.; Mitchell, P.; Wong, T.Y. The prevalence of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2010, 117, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.; Klein, B.E.; Cruickshanks, K.J. The prevalence of age-related maculopathy by geographic region and ethnicity. Prog. Retin. Eye Res. 1999, 18, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Chong, E.W.; Wong, W.L.; Rosman, M.; Aung, T.; Loo, J.L.; Shen, S.; Loon, S.C.; Tan, D.T.; Tai, E.S.; et al. Prevalence and causes of low vision and blindness in an urban malay population: The Singapore Malay Eye Study. Arch. Ophthalmol. 2008, 126, 1091–1099. [Google Scholar] [CrossRef] [Green Version]
- Wong, T.Y.; Chakravarthy, U.; Klein, R.; Mitchell, P.; Zlateva, G.; Buggage, R.; Fahrbach, K.; Probst, C.; Sledge, I. The natural history and prognosis of neovascular age-related macular degeneration: A systematic review of the literature and meta-analysis. Ophthalmology 2008, 115, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.; Smith, W.; Attebo, K.; Wang, J.J. Prevalence of age-related maculopathy in Australia. The Blue Mountains Eye Study. Ophthalmology 1995, 102, 1450–1460. [Google Scholar] [CrossRef] [PubMed]
- Sadda, S.R.; Guymer, R.; Holz, F.G.; Schmitz-Valckenberg, S.; Curcio, C.A.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; et al. Consensus Definition for Atrophy Associated with Age-Related Macular Degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology 2018, 125, 537–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- Shijo, T.; Sakurada, Y.; Fukuda, Y.; Yoneyama, S.; Sugiyama, A.; Matsubara, M.; Kikushima, W.; Tanabe, N.; Parikh, R.; Kashiwagi, K. Association of CRP levels with ARMS2 and CFH variants in age-related macular degeneration. Int. Ophthalmol. 2020, 40, 2735–2742. [Google Scholar] [CrossRef]
- Sakurada, Y.; Tanaka, K.; Fragiotta, S. Differentiating drusen and drusenoid deposits subtypes on multimodal imaging and risk of advanced age-related macular degeneration. Jpn. J. Ophthalmol. 2023, 67, 1–13. [Google Scholar] [CrossRef]
- Ferris, F.L.; Davis, M.D.; Clemons, T.E.; Lee, L.Y.; Chew, E.Y.; Lindblad, A.S.; Milton, R.C.; Bressler, S.B.; Klein, R.; Age-Related Eye Disease Study (AREDS) Research Group. A simplified severity scale for age-related macular degeneration: AREDS Report No. 18. Arch. Ophthalmol. 2005, 123, 1570–1574. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Ito, Y.; Yamasaki, T.; Yanagi, Y.; Gemmy Cheung, C.M.; Motomura, K.; Kawakami, S.; Kinoshita, T.; Yuki, K.; Hanyuda, A.; et al. Association of Choroidal Thickness with Intermediate Age-Related Macular Degeneration in a Japanese Population. Ophthalmol. Retina 2021, 5, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sivaprasad, S. Drusen and pachydrusen: The definition, pathogenesis, and clinical significance. Eye 2021, 35, 121–133. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Yoneyama, S.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Tanabe, N.; Iijima, H. Clinical and genetic characteristics of pachydrusen in patients with exudative age-related macular degeneration. Sci. Rep. 2019, 9, 11906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakurada, Y.; Sugiyama, A.; Kikushima, W.; Yoneyama, S.; Tanabe, N.; Matsubara, M.; Iijima, H. Pseudodrusen pattern and development of late age-related macular degeneration in the fellow eye of the unilateral case. Jpn. J. Ophthalmol. 2019, 63, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Parikh, R.; Gal-Or, O.; Balaratnasingam, C.; Leong, B.C.S.; Tanaka, K.; Cherepanoff, S.; Spaide, R.F.; Freund, K.B.; Yannuzzi, L.A. CUTICULAR DRUSEN: Risk of Geographic Atrophy and Macular Neovascularization. Retina 2020, 40, 257–265. [Google Scholar] [CrossRef]
- Zweifel, S.A.; Imamura, Y.; Spaide, T.C.; Fujiwara, T.; Spaide, R.F. Prevalence and significance of subretinal drusenoid deposits (reticular pseudodrusen) in age-related macular degeneration. Ophthalmology 2010, 117, 1775–1781. [Google Scholar] [CrossRef]
- Kume, A.; Ohshiro, T.; Sakurada, Y.; Kikushima, W.; Yoneyama, S.; Kashiwagi, K. Treatment Patterns and Health Care Costs for Age-Related Macular Degeneration in Japan: An Analysis of National Insurance Claims Data. Ophthalmology 2016, 123, 1263–1268. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Okada, A.; Matsui, H.; Yasunaga, H.; Aihara, M.; Obata, R. Recent trends in anti-vascular endothelial growth factor intravitreal injections: A large claims database study in Japan. Jpn. J. Ophthalmol. 2023, 67, 109–118. [Google Scholar] [CrossRef]
- Parikh, R.; Pirakitikulr, N.; Chhablani, J.; Sakurada, Y.; Singh, R.P.; Modi, Y.S. A Multinational Comparison of Anti-Vascular Endothelial Growth Factor Use: The United States, the United Kingdom, and Asia-Pacific. Ophthalmol. Retina 2019, 3, 16–26. [Google Scholar] [CrossRef]
- Parikh, R.; Feng, P.W.; Tainsh, L.; Sakurada, Y.; Balaratnasingam, C.; Khurana, R.N.; Hemmati, H.; Modi, Y.S. Comparison of Ophthalmic Medication Prices Between the United States and Australia. JAMA Ophthalmol. 2019, 137, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, M.; Ogata, N.; Otsuji, T.; Nishimura, T.; Takahashi, K.; Matsumura, M. Expression of pigment epithelium derived factor and vascular endothelial growth factor in choroidal neovascular membranes and polypoidal choroidal vasculopathy. Br. J. Ophthalmol. 2004, 88, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, N. Vascular endothelial growth factor. The trigger for neovascularization in the eye. Lab. Investig. 1995, 72, 615–618. [Google Scholar] [PubMed]
- Parikh, R.; Ross, J.S.; Sangaralingham, L.R.; Adelman, R.A.; Shah, N.D.; Barkmeier, A.J. Trends of Anti-Vascular Endothelial Growth Factor Use in Ophthalmology Among Privately Insured and Medicare Advantage Patients. Ophthalmology 2017, 124, 352–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.M.; Kaiser, P.K.; Michels, M.; Soubrane, G.; Heier, J.S.; Kim, R.Y.; Sy, J.P.; Schneider, S.; Group, A.S. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1432–1444. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y.; Group, M.S. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [Green Version]
- Bayes, M.; Rabasseda, X.; Prous, J.R. Gateways to clinical trials. Methods Find Exp. Clin. Pharm. 2004, 26, 473–503. [Google Scholar]
- Gragoudas, E.S.; Adamis, A.P.; Cunningham, E.T., Jr.; Feinsod, M.; Guyer, D.R.; VEGF Inhibition Study in Ocular Neovascularization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. N. Engl. J. Med. 2004, 351, 2805–2816. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, Q.D.; Das, A.; Do, D.V.; Dugel, P.U.; Gomes, A.; Holz, F.G.; Koh, A.; Pan, C.K.; Sepah, Y.J.; Patel, N.; et al. Brolucizumab: Evolution through Preclinical and Clinical Studies and the Implications for the Management of Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 963–976. [Google Scholar] [CrossRef]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef]
- Tadayoni, R.; Sararols, L.; Weissgerber, G.; Verma, R.; Clemens, A.; Holz, F.G. Brolucizumab: A Newly Developed Anti-VEGF Molecule for the Treatment of Neovascular Age-Related Macular Degeneration. Ophthalmologica 2021, 244, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ferro Desideri, L.; Traverso, C.E.; Nicolo, M. Brolucizumab: A novel anti-VEGF humanized single-chain antibody fragment for treating w-AMD. Expert Opin. Biol. Ther. 2021, 21, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Emanuelli, A.; Bandello, F.; Barranco, J.J.E.; Figueira, J.; Souied, E.; Wolf, S.; Gupta, V.; Ngah, N.F.; Liew, G.; et al. KESTREL and KITE: 52-Week Results From Two Phase III Pivotal Trials of Brolucizumab for Diabetic Macular Edema. Am. J. Ophthalmol. 2022, 238, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Yannuzzi, N.A.; Freund, K.B. Brolucizumab: Evidence to date in the treatment of neovascular age-related macular degeneration. Clin. Ophthalmol. 2019, 13, 1323–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugel, P.U.; Singh, R.P.; Koh, A.; Ogura, Y.; Weissgerber, G.; Gedif, K.; Jaffe, G.J.; Tadayoni, R.; Schmidt-Erfurth, U.; Holz, F.G. HAWK and HARRIER: Ninety-Six-Week Outcomes from the Phase 3 Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2021, 128, 89–99. [Google Scholar] [CrossRef]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G.; et al. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kobori, H.; Nozuki, N.; Kogawa, S.; Kudo, A. A case of intraocular inflammation after intravitreal brolucizumab injection monitored by laser flare-cell photometer. Am. J. Ophthalmol. Case Rep. 2022, 28, 101727. [Google Scholar] [CrossRef]
- Patil, N.S.; Dhoot, A.S.; Popovic, M.M.; Kertes, P.J.; Muni, R.H. Risk of intraocular inflammation after injection of antivascular endothelial growth factor agents: A Meta-analysis. Retina 2022, 42, 2134–2142. [Google Scholar] [CrossRef]
- Hikichi, T. Sub-Tenon’s capsule triamcinolone acetonide injection to prevent brolucizumab-associated intraocular inflammation. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 2529–2535. [Google Scholar] [CrossRef]
- Mukai, R.; Matsumoto, H.; Akiyama, H. Risk factors for emerging intraocular inflammation after intravitreal brolucizumab injection for age-related macular degeneration. PLoS ONE 2021, 16, e0259879. [Google Scholar] [CrossRef]
- Shigemoto, Y.; Sakurada, Y.; Fukuda, Y.; Matsubara, M.; Parikh, R.; Kashiwagi, K. The combination therapy of subtenon triamcinolone acetonide injection and intravitreal brolucizumab for brolucizumab-related intraocular inflammation. Medicine 2021, 100, e27580. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Horiguchi, E.; Kawano, K.; Ushida, H.; Nakano, Y.; Ito, Y.; Terasaki, H. Three cases of brolucizumab-associated retinal vasculitis treated with systemic and local steroid therapy. Jpn. J. Ophthalmol. 2021, 65, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Hikichi, T. Three Japanese cases of intraocular inflammation after intravitreal brolucizumab injections in one clinic. Jpn. J. Ophthalmol. 2021, 65, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Baumal, C.R.; Bodaghi, B.; Singer, M.; Tanzer, D.J.; Seres, A.; Joshi, M.R.; Feltgen, N.; Gale, R. Expert Opinion on Management of Intraocular Inflammation, Retinal Vasculitis, and Vascular Occlusion after Brolucizumab Treatment. Ophthalmol. Retina 2021, 5, 519–527. [Google Scholar] [CrossRef]
- Baumal, C.R.; Spaide, R.F.; Vajzovic, L.; Freund, K.B.; Walter, S.D.; John, V.; Rich, R.; Chaudhry, N.; Lakhanpal, R.R.; Oellers, P.R.; et al. Retinal Vasculitis and Intraocular Inflammation after Intravitreal Injection of Brolucizumab. Ophthalmology 2020, 127, 1345–1359. [Google Scholar] [CrossRef]
- Awh, C.C.; Davis, E.C.; Thomas, M.K.; Thomas, A.S. Short-Term Outcomes after Interim Treatment with Brolucizumab: A Retrospective Case Series of a Single Center Experience. Retina 2022, 42, 899–905. [Google Scholar] [CrossRef]
- Saitta, A.; D’Eliseo, L.A.; D’Eliseo, D. Efficacy and safety of brolucizumab for serous drusenoid pigment epithelium detachment non-responder to bevacizumab and aflibercept. Eur. J. Ophthalmol. 2022, 11206721221143154. [Google Scholar] [CrossRef]
- Viggiano, P.; Grassi, M.O.; Boscia, G.; Pignataro, M.; Petruzzella, G.; Borrelli, E.; Molfetta, T.; Alessio, G.; Boscia, F. Short-Term Morphofunctional Changes in Previously Treated Neovascular AMD Eyes Switched to Brolucizumab. J. Clin. Med. 2022, 11, 5517. [Google Scholar] [CrossRef]
- Kitajima, Y.; Maruyama-Inoue, M.; Ikeda, S.; Ito, A.; Inoue, T.; Yanagi, Y.; Kadonosono, K. Short-term outcomes of switching to brolucizumab in japanese patients with neovascular age-related macular degeneration. Jpn. J. Ophthalmol. 2022, 66, 511–517. [Google Scholar] [CrossRef]
- Ueda-Consolvo, T.; Tanigichi, A.; Numata, A.; Oiwake, T.; Nakamura, T.; Ishida, M.; Yanagisawa, S.; Hayashi, A. Switching to brolucizumab from aflibercept in age-related macular degeneration with type 1 macular neovascularization and polypoidal choroidal vasculopathy: An 18-month follow-up study. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 345–352. [Google Scholar] [CrossRef]
- Boltz, A.; Radunsky, K.; Weingessel, B.; Vecsei-Marlovits, V.P. Brolucizumab for pre-treated patients with choroidal neovascularization and signs of tachyphylaxis to aflibercept and bevacizumab. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 2561–2566. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, A.; Kodjikian, L.; Srivastava, S.; Dwivedi, S.; Banker, A.S.; Abukashabah, A.; Sudhalkar, A.; Mathis, T. Initial Pro Re Nata Brolucizumab for Exudative AMD: The PROBE Study. J. Clin. Med. 2021, 10, 4153. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.B.; Baumal, C.R.; Crane, A.M.; Witkin, A.J.; Lally, D.R.; Liang, M.C.; Enriquez, J.R.; Eichenbaum, D.A. Early Experience With Brolucizumab Treatment of Neovascular Age-Related Macular Degeneration. JAMA Ophthalmol. 2021, 139, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Khanani, A.M.; Brown, D.M.; Jaffe, G.J.; Wykoff, C.C.; Adiguzel, E.; Wong, R.; Meng, X.; Heier, J.S.; Investigators, M. MERLIN: Phase 3a, Multicenter, Randomized, Double-Masked Trial of Brolucizumab in Participants with Neovascular Age-Related Macular Degeneration and Persistent Retinal Fluid. Ophthalmology 2022, 129, 974–985. [Google Scholar] [CrossRef] [PubMed]
- Khanani, A.M.; Zarbin, M.A.; Barakat, M.R.; Albini, T.A.; Kaiser, P.K.; Guruprasad, B.; Agashivala, N.; Yu, J.S.; Wykoff, C.C.; MacCumber, M.W. Safety Outcomes of Brolucizumab in Neovascular Age-Related Macular Degeneration: Results From the IRIS Registry and Komodo Healthcare Map. JAMA Ophthalmol. 2022, 140, 20–28. [Google Scholar] [CrossRef]
- Ota, H.; Takeuchi, J.; Nakano, Y.; Horiguchi, E.; Taki, Y.; Ito, Y.; Terasaki, H.; Nishiguchi, K.M.; Kataoka, K. Switching from aflibercept to brolucizumab for the treatment of refractory neovascular age-related macular degeneration. Jpn. J. Ophthalmol. 2022, 66, 278–284. [Google Scholar] [CrossRef]
- Villegas, N.C.; Mishra, K.; Steinle, N.; Liu, W.; Beadle, B.; Mruthyunjaya, P. Intravitreal brolucizumab as treatment of early onset radiation retinopathy secondary to plaque brachytherapy for choroidal melanoma. Am. J. Ophthalmol. Case Rep. 2022, 27, 101581. [Google Scholar] [CrossRef]
- Abdin, A.D.; Aljundi, W.; El Jawhari, K.; Suffo, S.; Weinstein, I.; Seitz, B. First Year Real Life Experience With Intravitreal Brolucizumab for Treatment of Refractory Neovascular Age-Related Macular Degeneration. Front. Pharmacol. 2022, 13, 860784. [Google Scholar] [CrossRef]
- Haensli, C.; Pfister, I.B.; Garweg, J.G. Switching to Brolucizumab in Neovascular Age-Related Macular Degeneration Incompletely Responsive to Ranibizumab or Aflibercept: Real-Life 6 Month Outcomes. J. Clin. Med. 2021, 10, 2666. [Google Scholar] [CrossRef]
- Bilgic, A.; Kodjikian, L.; March de Ribot, F.; Vasavada, V.; Gonzalez-Cortes, J.H.; Abukashabah, A.; Sudhalkar, A.; Mathis, T. Real-World Experience with Brolucizumab in Wet Age-Related Macular Degeneration: The REBA Study. J. Clin. Med. 2021, 10, 2758. [Google Scholar] [CrossRef]
- Chakraborty, D.; Maiti, A.; Sheth, J.U.; Mondal, S.; Boral, S.; Nandi, K.; Sinha, T.K.; Das, A. Brolucizumab in Neovascular Age-Related Macular Degeneration—Indian Real-World Experience: The BRAILLE Study—Fifty-Two-Week Outcomes. Clin. Ophthalmol. 2022, 16, 4303–4313. [Google Scholar] [CrossRef] [PubMed]
- Baumal, C.R.; Sorensen, T.L.; Karcher, H.; Freitas, R.L.; Becher, A.; Balez, S.; Clemens, A.; Singer, M.; Kodjikian, L. Efficacy and safety of brolucizumab in age-related macular degeneration: A systematic review of real-world studies. Acta Ophthalmol. 2022, 101, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Guymer, R.H.; Markey, C.M.; McAllister, I.L.; Gillies, M.C.; Hunyor, A.P.; Arnold, J.J.; Investigators, F. Tolerating Subretinal Fluid in Neovascular Age-Related Macular Degeneration Treated with Ranibizumab Using a Treat-and-Extend Regimen: FLUID Study 24-Month Results. Ophthalmology 2019, 126, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, T.; Koizumi, H.; Yamagishi, T.; Kinoshita, S. Subfoveal choroidal thickness after ranibizumab therapy for neovascular age-related macular degeneration: 12-month results. Ophthalmology 2012, 119, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, H.; Kano, M.; Yamamoto, A.; Saito, M.; Maruko, I.; Sekiryu, T.; Okada, A.A.; Iida, T. Subfoveal Choroidal Thickness during Aflibercept Therapy for Neovascular Age-Related Macular Degeneration: Twelve-Month Results. Ophthalmology 2016, 123, 617–624. [Google Scholar] [CrossRef]
- Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kume, A.; Iijima, H. Comparison of initial treatment between 3-monthly intravitreal aflibercept monotherapy and combined photodynamic therapy with single intravitreal aflibercept for polypoidal choroidal vasculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 311–316. [Google Scholar] [CrossRef]
- Morimoto, M.; Matsumoto, H.; Mimura, K.; Akiyama, H. Two-year results of a treat-and-extend regimen with aflibercept for polypoidal choroidal vasculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1891–1897. [Google Scholar] [CrossRef]
- Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Kume, A.; Iijima, H. Choroidal Thickness as a Prognostic Factor of Photodynamic Therapy with Aflibercept or Ranibizumab for Polypoidal Choroidal Vasculopathy. Retina 2017, 37, 1866–1872. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Matsubara, M.; Hasebe, Y.; Sugiyama, A.; Kikushima, W.; Kashiwagi, K. Comparison of Outcomes between 3 Monthly Brolucizumab and Aflibercept Injections for Polypoidal Choroidal Vasculopathy. Biomedicines 2021, 9, 1164. [Google Scholar] [CrossRef]
- Sakurada, Y.; Yoneyama, S.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Mabuchi, F.; Kume, A.; Kubota, T.; Iijima, H. Prevalence and Genetic Characteristics of Geographic Atrophy among Elderly Japanese with Age-Related Macular Degeneration. PLoS ONE 2016, 11, e0149978. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Eyes | 60 |
|---|---|
| Age | 76.2 ± 7.4 |
| Male gender | 51 (85.0%) |
| Disease subtype (nAMD:PCV) | 20:40 |
| Baseline BCVA | 0.44 ± 0.39 |
| Baseline CRT on SS-OCT (µm) | 313 ± 145 |
| Baseline SCT on SS-OCT (µm) | 210 ± 93 |
| Mean follow-up period (month) | 67.9 ± 34.5 |
| Mean number of total injections | 30.1 ± 17.8 |
| Number of the patients with the past history of PDT (%) | 14 (23.3%) |
| Dry Macula | SRF Only | IRF Only | SRF and IRF | |
|---|---|---|---|---|
| At baseline | 0/60 | 51 (85.0%) | 4 (6.7%) | 5 (8.3%) |
| At Visit 1 | 16/60 (26.7%) | 35 (58.3%) | 6 (10.0%) | 3 (5.0%) |
| At 12 months | 26/60 (43.3%) | 25 (41.7%) | 6 (10.0%) | 3 (5.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikushima, W.; Sakurada, Y.; Fukuda, Y.; Matsubara, M.; Kotoda, Y.; Sugiyama, A.; Kashiwagi, K. A Treat-and-Extend Regimen of Intravitreal Brolucizumab for Exudative Age-Related Macular Degeneration Refractory to Aflibercept: A 12-Month Result. Pharmaceuticals 2023, 16, 562. https://doi.org/10.3390/ph16040562
Kikushima W, Sakurada Y, Fukuda Y, Matsubara M, Kotoda Y, Sugiyama A, Kashiwagi K. A Treat-and-Extend Regimen of Intravitreal Brolucizumab for Exudative Age-Related Macular Degeneration Refractory to Aflibercept: A 12-Month Result. Pharmaceuticals. 2023; 16(4):562. https://doi.org/10.3390/ph16040562
Chicago/Turabian StyleKikushima, Wataru, Yoichi Sakurada, Yoshiko Fukuda, Mio Matsubara, Yumi Kotoda, Atsushi Sugiyama, and Kenji Kashiwagi. 2023. "A Treat-and-Extend Regimen of Intravitreal Brolucizumab for Exudative Age-Related Macular Degeneration Refractory to Aflibercept: A 12-Month Result" Pharmaceuticals 16, no. 4: 562. https://doi.org/10.3390/ph16040562
APA StyleKikushima, W., Sakurada, Y., Fukuda, Y., Matsubara, M., Kotoda, Y., Sugiyama, A., & Kashiwagi, K. (2023). A Treat-and-Extend Regimen of Intravitreal Brolucizumab for Exudative Age-Related Macular Degeneration Refractory to Aflibercept: A 12-Month Result. Pharmaceuticals, 16(4), 562. https://doi.org/10.3390/ph16040562