
The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases


Abstract
:1. Introduction
2. The Unique Clinical Characteristics of Deferiprone
3. The Pharmacological and Metabolic Properties of Deferiprone
4. The Unique Effects on Proteins by Deferiprone and Therapeutic Implications
5. The High Clinical Antioxidant Potential of Deferiprone
6. Repurposing of Deferiprone for the Treatment of Non-Iron-Loaded Diseases
7. Future Challenges and Potential New Clinical Uses of Deferiprone
8. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADMET | absorption, distribution, metabolism, elimination, and toxicity |
| L1 | deferiprone |
| HPLC | high performance liquid chromatography |
| HIF | hypoxia-inducible factor |
| DF | deferoxamine |
| DFRA | deferasirox |
| HIF PHD | hypoxia-inducible factor propyl hydroxylases |
| LVEF | left ventricular ejection fraction |
| MRI | magnetic resonance imaging |
| NBIA | neurodegeneration with brain iron accumulation |
| NDRG1 | N-MYC downstream-regulated gene-1 |
| PKAN | pantothenate kinase 2-associated neurodegeneration |
| STEAP4 | six transmembrane epithelial antigen of prostate, family member 4 |
| UPAGE | urea polyacrylamide gel electrophoresis |
References
- Ahmed, F.; Samantasinghar, A.; Soomro, A.M.; Kim, S.; Choi, K.H. A systematic review of computational approaches to understand cancer biology for informed drug repurposing. J. Biomed. Inform. 2023, 142, 104373. [Google Scholar] [CrossRef]
- Servidei, T.; Sgambato, A.; Lucchetti, D.; Navarra, P.; Ruggiero, A. Drug Repurposing in Pediatric Brain Tumors: Posterior Fossa Ependymoma and Diffuse Midline Glioma under the Looking Glass. Front. Biosci.-Landmark 2023, 28, 77. [Google Scholar] [CrossRef] [PubMed]
- Famurewa, A.C.; Mukherjee, A.G.; Wanjari, U.R.; Sukumar, A.; Murali, R.; Renu, K.; Vellingiri, B.; Dey, A.; Gopalakrishnan, A.V. Repurposing FDA-approved drugs against the toxicity of platinum-based anticancer drugs. Life Sci. 2022, 305, 120789. [Google Scholar] [CrossRef] [PubMed]
- Delroba, K.; Alaei, M.; Khalili, H. Treatment options for infections caused by multidrug-resistant Gram-negative bacteria: A guide to good clinical practice. Future Microbiol. 2023, 18, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Nikam, R.V.; Gowtham, M.; More, P.S.; Shinde, A.S. Current and emerging prospects in the psoriatic treatment. Int. Immunopharmacol. 2023, 120, 110331. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, H.C.; Bezerra, B.T.; Rodrigues, M.L. Antifungal Development and the Urgency of Minimizing the Impact of Fungal Diseases on Public Health. ACS Bio. Med. Chem. Au. 2022, 3, 137–146. [Google Scholar] [CrossRef]
- Wang, R.S.; Loscalzo, J. Repurposing Drugs for the Treatment of COVID-19 and Its Cardiovascular Manifestations. Circ. Res. 2023, 132, 1374–1386. [Google Scholar] [CrossRef]
- Augustin, Y.; Staines, H.M.; Velavan, T.P.; Kamarulzaman, A.; Kremsner, P.G.; Krishna, S. Drug repurposing for COVID-19: Current evidence from randomized controlled adaptive platform trials and living systematic reviews. Br. Med. Bull. 2023, ldac037. [Google Scholar] [CrossRef]
- Manai, F.; Govoni, S.; Amadio, M. The Challenge of Dimethyl Fumarate Repurposing in Eye Pathologies. Cells 2022, 11, 4061. [Google Scholar] [CrossRef]
- McGowan, E.; Sanjak, J.; Math, E.A.; Zhu, Q. Integrative Rare Disease Biomedical Profile based Network Supporting Drug Repurposing, a case study of Glioblastoma. Res. Sq. 2023, rs.3.rs-2809689. [Google Scholar] [CrossRef]
- de Poel, E.; Spelier, S.; Hagemeijer, M.C.; van Mourik, P.; Suen, S.W.F.; Vonk, A.M.; Brunsveld, J.E.; Ithakisiou, G.N.; Kruisselbrink, E.; Oppelaar, H.; et al. FDA-approved drug screening in patient-derived organoids demonstrates potential of drug repurposing for rare cystic fibrosis genotypes. J. Cyst. Fibrosis 2023, 22, 548–559. [Google Scholar] [CrossRef]
- Kontoghiorghe, C.N.; Andreou, N.; Constantinou, K.; Kontoghiorghes, G.J. World health dilemmas: Orphan and rare diseases, orphan drugs and orphan patients. World J. Methodol. 2014, 4, 163–188. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, A.; Pantopoulos, K. Basics and principles of cellular and systemic iron homeostasis. Mol. Aspects Med. 2020, 75, 00866. [Google Scholar] [CrossRef]
- Gozzelino, R.; Arosio, P. Iron Homeostasis in Health and Disease. Int. J. Mol. Sci. 2016, 17, 130. [Google Scholar] [CrossRef] [Green Version]
- Cairo, G.; Bernuzzi, F.; Recalcati, S.A. A precious metal: Iron, an essential nutrient for all cells. Genes Nutr. 2006, 1, 25–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, N.C. Disorders of iron metabolism. N. Engl. J. Med. 1999, 341, 1986–1995, Erratum in N. Engl. J. Med. 2000, 342, 364. [Google Scholar] [CrossRef]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; De Benoist, B. Worldwide Prevalence of Anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasricha, S.R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Anonymous. Community control of hereditary anaemias: Memorandum from a WHO meeting. Bull World Health Organ 1983, 61, 63–80. [Google Scholar]
- Weatherall, D.J.; Clegg, J.B. Inherited haemoglobin disorders: An increasing global health problem. Bull World Health Organ 2001, 79, 704–712. [Google Scholar]
- Weatherall, D.J.; Clegg, J.B. Genetic disorders of hemoglobin. Semin Hematol. 1999, 36, 24–37. [Google Scholar] [PubMed]
- Modell, B.; Berdoukas, V. The Clinical Approach to Thalassaemia; Grune and Stratton: New York, NY, USA, 1984; pp. 165–169. [Google Scholar]
- Barton, J.C.; Edwards, C.Q. (Eds.) Hemochromatosis: Genetics, Pathophysiology, Diagnosis and Treatment; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Feder, J.N.; Gnirke, A.; Thomas, W.; Tsuchihashi, Z.; Ruddy, D.A.; Basava, A.; Dormishian, F.; Domingo, R., Jr.; Ellis, M.C.; Fullan, A.; et al. A novel MHC class I-like gene is mutated in patients with hereditary haemochromatosis. Nat. Genet. 1996, 13, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Pietrangelo, A. Hereditary hemochromatosis—A new look at an old disease. New Engl. J. Med. 2004, 350, 2383–2397. [Google Scholar] [CrossRef] [Green Version]
- Denisov, E.T.; Afanas’ev, I.B. Oxidation and Antioxidants in Organic Chemistry and Biology. CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2005. [Google Scholar]
- Halliwell, B.; Gutteridge, J.M.C.; Cross, C.E. Free radicals, antioxidants and human disease: Where are we now? J. Lab. Clin. Med. 1992, 119, 598–620. [Google Scholar] [PubMed]
- Nousis, L.; Kanavaros, P.; Barbouti, A. Oxidative Stress-Induced Cellular Senescence: Is Labile Iron the Connecting Link? Antioxidants 2023, 12, 1250. [Google Scholar] [CrossRef] [PubMed]
- Galaris, D.; Pantopoulos, K. Oxidative stress and iron homeostasis: Mechanistic and health aspects. Crit. Rev. Clin. Lab. Sci. 2008, 45, 1–23. [Google Scholar] [CrossRef]
- Reeder, B.J.; Wilson, M.T. Hemoglobin and myoglobin associated oxidative stress: From molecular mechanisms to disease states. Curr. Med. Chem. 2005, 12, 2741–2751. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, J.L. Clinical Challenges with Iron Chelation in Beta Thalassemia. Hematol. Oncol. Clin. North Am. 2023, 37, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Hokland, P.; Daar, S.; Khair, W.; Sheth, S.; Taher, A.T.; Torti, L.; Hantaweepant, C.; Rund, D. Thalassaemia-A global view. Br. J. Haematol. 2023, 201, 199–214. [Google Scholar] [CrossRef]
- Bruzzese, A.; Martino, E.A.; Mendicino, F.; Lucia, E.; Olivito, V.; Bova, C.; Filippelli, G.; Capodanno, I.; Neri, A.; Morabito, F.; et al. Iron chelation therapy. Eur. J. Haematol. 2023, 110, 490–497. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J.; Eracleous, E.; Economides, C.; Kolnagou, A. Advances in iron overload therapies. Prospects for effective use of deferiprone (L1), deferoxamine, the new experimental chelators ICL670, GT56–252, L1NAll and their combination. Curr. Med. Chem. 2005, 12, 2663–2681. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghe, C.N.; Kontoghiorghes, G.J. Efficacy and safety of iron-chelation therapy with deferoxamine, deferiprone, and deferasirox for the treatment of iron-loaded patients with non-transfusion-dependent thalassemia syndromes. Drug Des. Devel. Ther. 2016, 10, 465–481. [Google Scholar] [CrossRef] [Green Version]
- Sandoval-Acuña, C.; Torrealba, N.; Tomkova, V.; Jadhav, S.B.; Blazkova, K.; Merta, L.; Lettlova, S.; Adamcová, M.K.; Rosel, D.; Brábek, J.; et al. Targeting Mitochondrial Iron Metabolism Suppresses Tumor Growth and Metastasis by Inducing Mitochondrial Dysfunction and Mitophagy. Cancer Res. 2021, 81, 2289–2303. [Google Scholar] [CrossRef] [PubMed]
- Al-Khabori, M.; Bhandari, S.; Al-Huneini, M.; Al-Farsi, K.; Panjwani, V.; Daar, S. Side effects of Deferasirox Iron Chelation in Patients with Beta Thalassemia Major or Intermedia. Oman Med. J. 2013, 28, 121–124. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. A record number of fatalities in many categories of patients treated with deferasirox: Loopholes in regulatory and marketing procedures undermine patient safety and misguide public funds? Expert Opin. Drug Saf. 2013, 12, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Exjade (Deferasirox) Tablets for Oral Suspension. Prescribing Information. (Novartis Pharmaceutical Corporation USA (NDA 21–882). October, 2006; pp. 1–12. Changes to the Warnings and Adverse Reactions Sections 2006 and 2007). Available online: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4177B1_02_b.pdf (accessed on 1 December 2015).
- Anonymous. Exjade (Deferasirox) Tablets for Oral Suspension (Highlights of Prescribing Information. Novartis Pharmaceutical Corp. USA (T2011-106). August 2011; pp. 1–16). Available online: http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021882s010lbl.pdf (accessed on 1 December 2015).
- Kontoghiorghes, G.J.; Kolnagou, A.; Peng, C.T.; Shah, S.V.; Aessopos, A. Safety issues of iron chelation therapy in patients with normal range iron stores including thalassaemia, neurodegenerative, renal and infectious diseases. Expert Opin. Drug Saf. 2010, 9, 201–206. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. The Design of Orally Active Iron Chelators for the Treatment of Thalassaemia. Ph.D. Thesis, University of Essex, Colchester, UK, 1982. British Library Microfilm No D66194/86. pp. 1–243. Available online: https://www.pri.ac.cy/files/KGJ_thesis_1982.pdf (accessed on 16 July 2023).
- Hadjidemetriou, M. Thalassemia: Yesterday, Today, Tomorrow. Am J. Hematol. 2017, 92, 490–492. [Google Scholar] [CrossRef] [Green Version]
- Neufeld, E.J. Oral chelators deferasirox and deferiprone for transfusional iron overload in thalassemia major: New data, new questions. Blood 2006, 107, 3436–3441. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghes, G.J.; Kleanthous, M.; Kontoghiorghe, C.N. The History of Deferiprone (L1) and the Paradigm of the Complete Treatment of Iron Overload in Thalassaemia. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020011. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. Deferiprone and Iron-Maltol: Forty Years since Their Discovery and Insights into Their Drug Design, Development, Clinical Use and Future Prospects. Int. J. Mol. Sci. 2023, 24, 4970. [Google Scholar] [CrossRef]
- The History of Deferiprone. Available online: https://www.youtube.com/watch?v=ZcvSLyIgYd8 (accessed on 1 October 2019).
- Kontoghiorghes, G.J. (Ed.) Oral chelation in the treatment of thalassaemia and other diseases. Drugs Today 1992, 28, 1–187. [Google Scholar]
- Kontoghiorghes, G.J.; Aldouri, M.A.; Hoffbrand, A.V.; Barr, J.; Wonke, B.; Kourouclaris, T.; Sheppard, L. Effective chelation of iron in beta thalassaemia with the oral chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Br. Med. J. (Clin. Res. Ed.) 1987, 295, 1509–1512. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghes, G.J.; Aldouri, M.A.; Sheppard, L.; Hoffbrand, A.V. 1,2-Dimethyl-3-hydroxypyrid-4-one, an orally active chelator for treatment of iron overload. Lancet 1987, 1, 1294–1295. [Google Scholar] [CrossRef] [PubMed]
- Vullo, C.; Di Palma, A.; De Sanctis, V.; Borgatti, L.; Atti, G. Trattamento ferrochelante [Iron-chelating treatment]. Haematologica 1989, 74 (Suppl. 5), 241–251. (In Italian) [Google Scholar] [PubMed]
- Agarwal, M.B.; Viswanathan, C.; Ramanathan, J.; Massil, D.E.; Shah, S.; Gupte, S.S.; Vasandani, D.; Puniyani, R.R. Oral iron chelation with L1. Lancet 1990, 335, 601. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.B.; Gupte, S.S.; Viswanathan, C.; Vasandani, D.; Ramanathan, J.; Desai, N.; Puniyani, R.R.; Chhablani, A.T. Long-term assessment of efficacy and safety of L1, an oral iron chelator, in transfusion dependent thalassaemia: Indian trial. Br. J. Haematol. 1992, 82, 460–466. [Google Scholar] [CrossRef]
- Nielsen, P.; Fischer, R.; Engelhardt, R.; Tondüry, P.; Gabbe, E.E.; Janka, G.E. Liver iron stores in patients with secondary haemosiderosis under iron chelation therapy with deferoxamine or deferiprone. Br. J. Haematol. 1995, 91, 827–833. [Google Scholar] [CrossRef]
- Olivieri, N.F.; Koren, G.; St Louis, P.; Freedman, M.H.; McClelland, R.A.; Templeton, D.M. Studies of the oral chelator 1,2-dimethyl-3-hydroxypyrid-4-one in thalassemia patients. Semin. Hematol. 1990, 27, 101–104. [Google Scholar]
- Goudsmit, R. Long-term treatment of patients with transfusion hemosiderosis using oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one (L1). Ned. Tijdschr. Geneeskd. 1991, 135, 2133–2136. [Google Scholar]
- Carnelli, V.; Terzoli, S.; Fossati, G.; Careddu, G.; Perri, M.; Pedrotti, L.; Mirra, N. New therapeutic trends in thalassemia: Oral chelating agents. Pediatr. Med. Chir. 1992, 14, 273–275. [Google Scholar]
- Cermák, J.; Brabec, V. Treatment of iron overload states with oral administration of the chelator agent, L1 (Deferiprone). Vnitr. Lek. 1994, 40, 586–590. [Google Scholar]
- Kersten, M.J.; Lange, R.; Smeets, M.E.; Vreugdenhil, G.; Roozendaal, K.J.; Lameijer, W.; Goudsmit, R. Long-term treatment of transfusional iron overload with the oral iron chelator deferiprone (L1): A Dutch multicenter trial. Ann. Hematol. 1996, 73, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Sheppard, L. Simple synthesis of the potent iron chelators 1-alkyl-3-hydroxy-2-methylpyrid-4-ones. Inorg. Chim. Acta 1987, 136, L11–L12. [Google Scholar] [CrossRef]
- Cohen, A.R.; Galanello, R.; Piga, A.; De Sanctis, V.; Tricta, F. Safety and effectiveness of long-term therapy with the oral iron chelator deferiprone. Blood 2003, 102, 1583–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elalfy, M.S.; Hamdy, M.; El Beshlawy, A.; Ebeid, F.S.E.; Badr, M.; Kanter, J.; Inusa, B.P.; Adly, A.; Williams, S.; Kilinc, Y.; et al. Deferiprone for transfusional iron overload in sickle cell disease and other anemias: Open-label study of up to 3 years. Blood Adv. 2023, 7, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.R.; Galanello, R.; Piga, A.; Dipalma, A.; Vullo, C.; Tricta, F. Safety profile of the oral iron chelator deferiprone: A multicentre study. Br. J. Haematol. 2000, 108, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Barman Balfour, J.A.; Foster, R.H. Deferiprone: A review of its clinical potential in iron overload in beta-thalassaemia major and other transfusion-dependent diseases. Drugs 1999, 58, 553–578. [Google Scholar] [CrossRef]
- Kolnagou, A.; Kleanthous, M.; Kontoghiorghes, G.J. Benefits and Risks in Polypathology and Polypharmacotherapy Challenges in the Era of the Transition of Thalassaemia from a Fatal to a Chronic or Curable Disease. Front. Biosci.-Elite 2022, 14, 18. [Google Scholar] [CrossRef]
- AlRefai, F.N.; Wonke, B.; Wickens, D.G.; Aydinok, Y.; Fielding, A.; Hoffbrand, A.V. Zinc concentration in patients with iron overload receiving oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one or desferrioxamine. J. Clin. Pathol. 1994, 47, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghes, G.J. New orally active iron chelators. Lancet 1985, 325, 817. [Google Scholar] [CrossRef]
- van der Kraaij, A.M.; van Eijk, H.G.; Koster, J.F. Prevention of postischemic cardiac injury by the orally active iron chelator 1,2-dimethyl-3-hydroxy-4-pyridone (L1) and the antioxidant (+)-cyanidanol-3. Circulation 1989, 80, 158–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brissot, P.; Zanninelli, G.; Guyader, D.; Zeind, J.; Gollan, J. Biliary excretion of plasma non-transferrin-bound iron in rats: Pathogenetic importance in iron-overload disorders. Am. J. Physiol. 1994, 267, G135–G142. [Google Scholar] [CrossRef] [PubMed]
- Gale, G.R.; Litchenberg, W.H.; Smith, A.B.; Singh, P.K.; Campbell, R.A.; Jones, M.M. Comparative iron mobilizing actions of deferoxamine, 1,2-dimethyl-3-hydroxypyrid-4-one, and pyridoxal isonicotinoyl hydrazone in iron hydroxamate-loaded mice. Res. Commun. Chem. Pathol. Pharmacol. 1991, 73, 299–313. [Google Scholar] [PubMed]
- Hershko, C.; Link, G.; Konijn, A.M.; Huerta, M.; Rosenmann, E.; Reinus, C. The iron-loaded gerbil model revisited: Effects of deferoxamine and deferiprone treatment. J. Lab. Clin. Med. 2002, 139, 50–58. [Google Scholar] [CrossRef]
- Anonymous. Oral iron chelators. Lancet 1989, 2, 1016–1017. [Google Scholar]
- Kontoghiorghes, G.J.; Barr, J.; Nortey, P.; Sheppard, L. Selection of a new generation of orally active alpha-ketohydroxypyridine iron chelators intended for use in the treatment of iron overload. Am. J. Hematol. 1993, 42, 340–349. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J.; Bartlett, A.N.; Hoffbrand, A.V.; Goddard, J.G.; Sheppard, L.; Barr, J.; Nortey, P. Long-term trial with the oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one (L1). I. Iron chelation and metabolic studies. Br. J. Haematol. 1990, 76, 295–300. [Google Scholar] [CrossRef]
- Berdoukas, V.; Nord, A.; Carson, S.; Puliyel, M.; Hofstra, T.; Wood, J.; Coates, T.D. Tissue iron evaluation in chronically transfused children shows significant levels of iron loading at a very young age. Am. J. Hematol. 2013, 88, E283–E285. [Google Scholar] [CrossRef]
- Zurlo, M.G.; De Stefano, P.; Borgna-Pignatti, C.; Di Palma, A.; Piga, A.; Melevendi, C.; Di Gregorio, F.; Burattini, M.G.; Terzoli, S. Survival and causes of death in thalassaemia major. Lancet 1989, 2, 27–30. [Google Scholar] [CrossRef]
- Kolnagou, A.; Michaelides, Y.; Kontos, C.; Kyriacou, K.; Kontoghiorghes, G.J. Myocyte damage and loss of myofibers is the potential mechanism of iron overload toxicity in congestive cardiac failure in thalassemia. Complete reversal of the cardiomyopathy and normalization of iron load by deferiprone. Hemoglobin 2008, 32, 17–28. [Google Scholar] [CrossRef]
- Modell, B.; Khan, M.; Darlison, M. Survival in β-thalassaemia major in the UK: Data from the UK Thalassaemia Register. Lancet 2000, 355, 2051–2052. [Google Scholar] [CrossRef] [PubMed]
- Telfer, P.; Coen, P.G.; Christou, S.; Hadjigavriel, M.; Kolnakou, A.; Pangalou, E.; Pavlides, N.; Psiloines, M.; Simamonian, K.; Skordos, G.; et al. Survival of medically treated thalassemia patients in Cyprus. Trends and risk factors over the period 1980-2004. Haematologica 2006, 91, 1187–1192. [Google Scholar] [PubMed]
- Telfer, P.T.; Warburton, F.; Christou, S.; Hadjigavriel, M.; Sitarou, M.; Kolnagou, A.; Angastiniotis, M. Improved survival in thalassemia major patients on switching from desferrioxamine to combined chelation therapy with desferrioxamine and deferiprone. Haematologica 2009, 94, 1777–1778. [Google Scholar] [CrossRef] [Green Version]
- Au, W.Y.; Lee, V.; Lau, C.W.; Yau, J.; Chan, D.; Chan, E.Y.; Cheung, W.W.; Ha, S.Y.; Kho, B.; Lee, C.Y.; et al. A synopsis of current care of thalassaemia major patients in Hong Kong. Hong Kong Med. J. 2011, 17, 261–266. [Google Scholar]
- Kolnagou, A.; Kontoghiorghe, C.N.; Kontoghiorghes, G.J. Transition of thalassaemia and Friedreich ataxia from fatal to chronic diseases. World J. Methodol. 2014, 4, 197–218. [Google Scholar] [CrossRef]
- Borgna-Pignatti, C.; Cappellini, M.D.; De Stefano, P.; Del Vecchio, G.C.; Forni, G.L.; Gamberini, M.R.; Ghilardi, R.; Piga, A.; Romeo, M.A.; Zhao, H.; et al. Cardiac morbidity and mortality in deferoxamine- or deferiprone-treated patients with thalassemia major. Blood 2006, 107, 3733–3737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, M.A.; Galanello, R.; Dessi, C.; Smith, G.C.; Westwood, M.A.; Agus, A.; Pibiri, M.; Nair, S.V.; Walker, J.M.; Pennell, D.J. Combined chelation therapy in thalassemia major for the treatment of severe myocardial siderosis with left ventricular dysfunction. J. Cardiovasc. Magn. Reson. 2008, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danjou, F.; Origa, R.; Anni, F.; Saba, L.; Cossa, S.; Podda, G.; Galanello, R. Longitudinal analysis of heart and liver iron in thalassemia major patients according to chelation treatment. Blood Cells Mol. Dis. 2013, 51, 142–145. [Google Scholar] [CrossRef]
- Filosa, A.; Vitrano, A.; Rigano, P.; Calvaruso, G.; Barone, R.; Capra, M.; Cuccia, L.; Gagliardotto, F.; Pitrolo, L.; Prossomariti, L.; et al. Long-term treatment with deferiprone enhances left ventricular ejection function when compared to deferoxamine in patients with thalassemia major. Blood Cells Mol. Dis. 2013, 51, 85–88. [Google Scholar] [CrossRef] [Green Version]
- Pepe, A.; Meloni, A.; Capra, M.; Cianciulli, P.; Prossomariti, L.; Malaventura, C.; Putti, M.C.; Lippi, A.; Romeo, M.A.; Bisconte, M.G.; et al. Deferasirox, deferiprone and desferrioxamine treatment in thalassemia major patients: Cardiac iron and function comparison determined by quantitative magnetic resonance imaging. Haematologica 2011, 96, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Maggio, A.; Vitrano, A.; Lucania, G.; Capra, M.; Cuccia, L.; Gagliardotto, F.; Pitrolo, L.; Prossomariti, L.; Filosa, A.; Caruso, V.; et al. Long-term use of deferiprone significantly enhances left-ventricular ejection function in thalassemia major patients. Am. J. Hematol. 2012, 87, 732–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, A.; Meloni, A.; Rossi, G.; Cuccia, L.; D’Ascola, G.D.; Santodirocco, M.; Cianciulli, P.; Caruso, V.; Romeo, M.A.; Filosa, A.; et al. Cardiac and hepatic iron and ejection fraction in thalassemia major: Multicentre prospective comparison of combined deferiprone and deferoxamine therapy against deferiprone or deferoxamine monotherapy. J. Cardiovasc. Magn. Reson. 2013, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggio, A.; Kattamis, A.; Felisi, M.; Reggiardo, G.; El-Beshlawy, A.; Bejaoui, M.; Sherief, L.; Christou, S.; Cosmi, C.; Della Pasqua, O.; et al. Evaluation of the efficacy and safety of deferiprone compared with deferasirox in paediatric patients with transfusion-dependent haemoglobinopathies (DEEP-2): A multicentre, randomised, open-label, non-inferiority, phase 3 trial. Lancet Haematol. 2020, 7, e469–e478. [Google Scholar] [CrossRef]
- Perrimond, H.; Chagnon, C.; Moulanier, I.; Michel, G.; Guidicelli, H.; Bernard, P.J. The value of nuclear magnetic resonance in the study of iron overload in thalassemia patients. Ann. Pediatr. 1991, 38, 175–184. [Google Scholar]
- Mavrogeni, S.I.; Gotsis, E.D.; Markussis, V.; Tsekos, N.; Politis, C.; Vretou, E.; Kermastinos, D. T2 relaxation time study of iron overload in b-thalassemia. MAGMA 1998, 6, 7–12. [Google Scholar] [CrossRef]
- Anderson, L.J.; Holden, S.; Davis, B.; Prescott, E.; Charrier, C.C.; Bunce, N.H.; Firmin, D.N.; Wonke, B.; Porter, J.; Walker, J.M.; et al. Cardiovascular T2-star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur. Heart J. 2001, 22, 2171–2179. [Google Scholar] [CrossRef] [Green Version]
- Pennell, D.J. T2* magnetic resonance and myocardial iron in thalassemia. Ann N. Y. Acad. Sci. 2005, 1054, 373–378. [Google Scholar] [CrossRef]
- Papakonstantinou, O.; Alexopoulou, E.; Economopoulos, N.; Benekos, O.; Kattamis, A.; Kostaridou, S.; Ladis, V.; Efstathopoulos, E.; Gouliamos, A.; Kelekis, N.L. Assessment of iron distribution between liver, spleen, pancreas, bone marrow, and myocardium by means of R2 relaxometry with MRI in patients with beta-thalassemia major. J. Magn. Reson. Imaging 2009, 29, 853–859. [Google Scholar] [CrossRef]
- Kolnagou, A.; Natsiopoulos, K.; Kleanthous, M.; Ioannou, A.; Kontoghiorghes, G.J. Liver iron and serum ferritin levels are misleading for estimating cardiac, pancreatic, splenic and total body iron load in thalassemia patients: Factors influencing the heterogenic distribution of excess storage iron in organs as identified by MRI T2*. Toxicol. Mech. Methods 2013, 23, 48–56. [Google Scholar] [CrossRef]
- Kolnagou, A.; Kontoghiorghes, G.J. Effective combination therapy of deferiprone and deferoxamine for the rapid clearance of excess cardiac IRON and the prevention of heart disease in thalassemia. The Protocol of the International Committee on Oral Chelators. Hemoglobin 2006, 30, 239–249. [Google Scholar] [CrossRef]
- Olivieri, N.F.; Koren, G.; Matsui, D.; Liu, P.P.; Blendis, L.; Cameron, R.; McClelland, R.A.; Templeton, D.M. Reduction of tissue iron stores and normalization of serum ferritin during treatment with the oral iron chelator L1 in thalassemia intermedia. Blood 1992, 79, 2741–2748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmaki, K.; Tzoumari, I.; Pappa, C.; Chouliaras, G.; Berdoukas, V. Normalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia major. Br. J. Haematol. 2010, 148, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Kolnagou, A.; Kontoghiorghe, C.N.; Kontoghiorghes, G.J. Prevention of Iron Overload and Long Term Maintenance of Normal Iron Stores in Thalassaemia Major Patients using Deferiprone or Deferiprone Deferoxamine Combination. Drug Res. 2017, 67, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Kolnagou, A.; Kontoghiorghes, G.J. New golden era of chelation therapy in thalassaemia: The achievement and maintenance of normal range body iron stores. Br. J. Haematol. 2010, 150, 489–490. [Google Scholar] [CrossRef]
- Ricchi, P.; Meloni, A.; Pistoia, L.; Gamberini, M.R.; Cuccia, L.; Allò, M.; Putti, M.C.; Spasiano, A.; Rosso, R.; Cecinati, V.; et al. Longitudinal prospective comparison of pancreatic iron by magnetic resonance in thalassemia patients transfusion-dependent since early childhood treated with combination deferiprone-desferrioxamine vs deferiprone or deferasirox monotherapy. Blood Transfus. 2023. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. A new era in iron chelation therapy: The design of optimal, individually adjusted iron chelation therapies for the complete removal of iron overload in thalassemia and other chronically transfused patients. Hemoglobin 2009, 33, 332–338. [Google Scholar] [CrossRef]
- Kolnagou, A.; Kontoghiorghes, G.J. Chelation protocols for the elimination and prevention of iron overload in thalassaemia. Front. Biosci.-Landmark 2018, 23, 1082–1098. [Google Scholar]
- Lin, C.H.; Chen, X.; Wu, C.C.; Wu, K.H.; Song, T.S.; Weng, T.F.; Hsieh, Y.W.; Peng, C.T. Therapeutic mechanism of combined oral chelation therapy to maximize efficacy of iron removal in transfusion-dependent thalassemia major—A pilot study. Expert Rev. Hematol. 2019, 12, 265–272. [Google Scholar] [CrossRef]
- Olivieri, N.F.; Sabouhanian, A.; Gallie, B.L. Single-center retrospective study of the effectiveness and toxicity of the oral iron chelating drugs deferiprone and deferasirox. PLoS ONE 2019, 14, e0211942. [Google Scholar] [CrossRef]
- Lal, A.; Porter, J.; Sweeters, N.; Ng, V.; Evans, P.; Neumayr, L.; Kurio, G.; Harmatz, P.; Vichinsky, E. Combined chelation therapy with deferasirox and deferoxamine in thalassemia. Blood Cells Mol. Dis. 2013, 50, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghes, G.J.; Goddard, J.G.; Bartlett, A.N.; Sheppard, L. Pharmacokinetic studies in humans with the oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Clin. Pharmacol. Ther. 1990, 48, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Matsui, D.; Klein, J.; Hermann, C.; Grunau, V.; McClelland, R.; Chung, D.; St-Louis, P.; Olivieri, N.; Koren, G. Relationship between the pharmacokinetics and iron excretion pharmacodynamics of the new oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one in patients with thalassemia. Clin. Pharmacol. Ther. 1991, 50, 294–298. [Google Scholar] [CrossRef]
- Soulières, D.; Mercier-Ross, J.; Fradette, C.; Rozova, A.; Tsang, Y.C.; Tricta, F. The pharmacokinetic and safety profile of single-dose deferiprone in subjects with sickle cell disease. Ann. Hematol. 2022, 101, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Kontoghiorghe, C.N. Iron and Chelation in Biochemistry and Medicine: New Approaches to Controlling Iron Metabolism and Treating Related Diseases. Cells 2020, 9, 1456. [Google Scholar] [CrossRef] [PubMed]
- Pope, E.; Berkovitch, M.; Klein, J.; Fassos, F.; Koren, G. Salivary measurement of deferiprone concentrations and correlation with serum levels. Ther. Drug Monit. 1997, 19, 95–97. [Google Scholar] [CrossRef]
- Drugs and Lactation Database (LactMed®) [Internet]; National Institute of Child Health and Human Development: Bethesda, MD, USA, 2006; Deferiprone. 2022 August 15.
- Fassos, F.F.; Klein, J.; Fernandes, D.; Matsui, D.; Olivieri, N.F.; Koren, G. The pharmacokinetics and pharmacodynamics of the oral iron chelator deferiprone (L1) in relation to hemoglobin levels. Int. J. Clin. Pharmacol. Ther. 1996, 34, 288–292. [Google Scholar]
- Bellanti, F.; Di Iorio, V.L.; Danhof, M.; Della Pasqua, O. Sampling Optimization in Pharmacokinetic Bridging Studies: Example of the Use of Deferiprone in Children With β-Thalassemia. J. Clin. Pharmacol. 2016, 56, 1094–1103. [Google Scholar] [CrossRef]
- Sheppard, L.; Kontoghiorghes, G.J. Synthesis and metabolism of L1 and other novel alpha-ketohydroxypyridine iron chelatorsand their metal complexes. Drugs Today 1992, 28 (Suppl. A), 3–10. [Google Scholar]
- Kontoghiorghes, G.J.; Bartlett, A.N.; Sheppard, L.; Barr, J.; Nortey, P. Oral iron chelation therapy with deferiprone. Monitoring of biochemical, drug and iron excretion changes. Arzneimittelforschung 1995, 45, 65–69. [Google Scholar]
- Kontoghiorghes, G.J. Chemical, pharmacological, toxicological and therapeutic advances of deferiprone (L1) and other iron and aluminium chelators. Arch. Toxicol. Suppl. 1996, 18, 202–214. [Google Scholar]
- Kontoghiorghes, G.J. Comparative efficacy and toxicity of desferrioxamine, deferiprone and other iron and aluminium chelating drugs. Toxicol. Lett. 1995, 80, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.M.; Langenickel, T.; Cain, M.; Kulkarni, S.; Shah, B.; Vemula, J.; Rahmanzadeh, G.; Poller, B. Clinical Investigation of Metabolic and Renal Clearance Pathways Contributing to the Elimination of Fevipiprant Using Probenecid as Perpetrator. Drug Metab. Dispos. 2021, 49, 389–394. [Google Scholar] [CrossRef]
- Sattar, H.; Jadoon, S.S.; Yang, N.; Li, S.; Xu, M.; Han, Y.; Ramzan, A.; Li, W. Role of Glucuronidation Pathway in Quetiapine Metabolism: An In vivo Drug-Drug Interaction Study between Quetiapine and Probenecid. Saudi J. Med. Med. Sci. 2020, 8, 196–200. [Google Scholar] [PubMed]
- Hussaarts, K.G.A.M.; van Doorn, L.; Eechoute, K.; Damman, J.; Fu, Q.; van Doorn, N.; Eisenmann, E.D.; Gibson, A.A.; Oomen-de Hoop, E.; de Bruijn, P.; et al. Influence of Probenecid on the Pharmacokinetics and Pharmacodynamics of Sorafenib. Pharmaceutics 2020, 12, 788. [Google Scholar] [CrossRef]
- Olivieri, N.F.; Koren, G.; Hermann, C.; Bentur, Y.; Chung, D.; Klein, J.; St Louis, P.; Freedman, M.H.; McClelland, R.A.; Templeton, D.M. Comparison of oral iron chelator L1 and desferrioxamine in iron-loaded patients. Lancet 1990, 336, 1275–1279. [Google Scholar] [CrossRef]
- Galanello, R.; Piga, A.; Forni, G.L.; Bertrand, Y.; Foschini, M.L.; Bordone, E.; Leoni, G.; Lavagetto, A.; Zappu, A.; Longo, F.; et al. Phase II clinical evaluation of deferasirox, a once-daily oral chelating agent, in pediatric patients with beta-thalassemia major. Haematologica 2006, 91, 1343–1351. [Google Scholar]
- Galanello, R. Evaluation of ICL670, a once-daily oral iron chelator in a phase III clinical trial of beta-thalassemia patients with transfusional iron overload. Ann. N. Y. Acad. Sci. 2005, 1054, 183–185. [Google Scholar] [CrossRef]
- Wei, W.; Schon, K.R.; Elgar, G.; Orioli, A.; Tanguy, M.; Giess, A.; Tischkowitz, M.; Caulfield, M.J.; Chinnery, P.F. Nuclear-embedded mitochondrial DNA sequences in 66,083 human genomes. Nature 2022, 611, 105–114. [Google Scholar] [CrossRef]
- Mora, C.; McKenzie, T.; Gaw, I.M.; Dean, J.M.; von Hammerstein, H.; Knudson, T.A.; Setter, R.O.; Smith, C.Z.; Webster, K.M.; Patz, J.A.; et al. Over half of known human pathogenic diseases can be aggravated by climate change. Nat. Clim. Chang 2022, 12, 869–875. [Google Scholar] [CrossRef]
- Bamborough, P. System-based drug discovery within the human kinome. Expert Opin. Drug Discov. 2012, 7, 1053–1070. [Google Scholar] [CrossRef]
- Schulthess, D.; Chlebus, M.; Bergström, R.; Baelen, K.V. Medicine adaptive pathways to patients (MAPPs): Using regulatory innovation to defeat Eroom’s law. Chin. Clin. Oncol. 2014, 3, 21. [Google Scholar]
- Kawabata, H. Transferrin and transferrin receptors update. Free Radic. Biol. Med. 2019, 133, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Sargent, P.J.; Farnaud, S.; Evans, R.W. Structure/function overview of proteins involved in iron storage and transport. Curr. Med. Chem. 2005, 12, 2683–2693. [Google Scholar] [CrossRef] [PubMed]
- Makey, D.G.; Seal, U.S. The detection of four molecular forms of human transferrin during the iron binding process. Biochim. Biophys. Acta. 1976, 453, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Pantopoulos, K. TfR2 links iron metabolism and erythropoiesis. Blood 2015, 125, 1055–1056. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghe, C.N.; Kolnagou, A.; Kontoghiorghes, G.J. Potential clinical applications of chelating drugs in diseases targeting transferrin-bound iron and other metals. Expert Opin. Investig. Drugs 2013, 22, 591–618. [Google Scholar] [CrossRef]
- Li, Y.; Harris, W.R. Iron removal from monoferric human serum transferrins by 1,2-dimethyl-3-hydroxypyridin-4-one, 1-hydroxypyridin-2-one and acetohydroxamic acid. Biochim. Biophys. Acta 1998, 1387, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J. Iron mobilization from transferrin and non-transferrin-bound-iron by deferiprone. Implications in the treatment of thalassemia, anemia of chronic disease, cancer and other conditions. Hemoglobin 2006, 30, 183–200. [Google Scholar] [CrossRef]
- Gomme, P.T.; McCann, K.B.; Bertolini, J. Transferrin: Structure, function and potential therapeutic actions. Drug Discov. Today 2005, 10, 267–273. [Google Scholar] [CrossRef]
- Luna, B.M.; Ershova, K.; Yan, J.; Ulhaq, A.; Nielsen, T.B.; Hsieh, S.; Pantapalangkoor, P.; Vanscoy, B.; Ambrose, P.; Rudin, S.; et al. Adjunctive transferrin to reduce the emergence of antibiotic resistance in Gram-negative bacteria. J. Antimicrob. Chemother. 2019, 74, 2631–2639. [Google Scholar] [CrossRef]
- Wang, B.; Timilsena, Y.P.; Blanch, E.; Adhikari, B. Lactoferrin: Structure, function, denaturation and digestion. Crit. Rev. Food Sci. Nutr. 2019, 59, 580–596. [Google Scholar] [CrossRef] [PubMed]
- Rosa, L.; Cutone, A.; Lepanto, M.S.; Paesano, R.; Valenti, P. Lactoferrin: A Natural Glycoprotein Involved in Iron and Inflammatory Homeostasis. Int. J. Mol. Sci. 2017, 18, 1985. [Google Scholar] [CrossRef] [Green Version]
- González-Chávez, S.A.; Arévalo-Gallegos, S.; Rascón-Cruz, Q. Lactoferrin: Structure, function and applications. Int. J. Antimicrob. Agents 2009, 33, 301.e1–301.e8. [Google Scholar] [CrossRef]
- Fernandes, K.E.; Weeks, K.; Carter, D.A. Lactoferrin Is Broadly Active against Yeasts and Highly Synergistic with Amphotericin B. Antimicrob. Agents Chemother. 2020, 64, e02284-19. [Google Scholar] [CrossRef] [Green Version]
- Kontoghiorghes, G.J. Iron mobilisation from lactoferrin by chelators at physiological pH. Biochim. Biophys. Acta. 1986, 882, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J. The study of iron mobilisation from transferrin using α-ketohydroxy heteroaromatic chelators. Biochim. Biophys. Acta. 1986, 869, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Evans, R.W. Site specificity of iron removal from transferrin by alpha-ketohydroxypyridine chelators. FEBS Lett. 1985, 189, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Evans, R.W.; Sharma, M.; Ogwang, W.; Patel, K.J.; Bartlett, A.N.; Kontoghiorghes, G.J. The effect of α-ketohydroxypyridine chelators on transferrin saturation in vitro and in vivo. Drugs Today 1992, 28 (Suppl. A), 9–23. [Google Scholar]
- Arosio, P.; Elia, L.; Poli, M. Ferritin, cellular iron storage and regulation. IUBMB Life 2017, 69, 414–422. [Google Scholar] [CrossRef] [Green Version]
- Theil, E.C. Ferritin: The protein nanocage and iron biomineral in health and in disease. Inorg. Chem. 2013, 52, 12223–12233. [Google Scholar] [CrossRef]
- Saito, H. Storage Iron Turnover from a New Perspective. Acta Haematol. 2019, 141, 201–208. [Google Scholar] [CrossRef] [PubMed]
- La, A.; Nguyen, T.; Tran, K.; Sauble, E.; Tu, D.; Gonzalez, A.; Kidane, T.Z.; Soriano, C.; Morgan, J.; Doan, M.; et al. Mobilization of iron from ferritin: New steps and details. Metallomics 2018, 10, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Knovich, M.A.; Coffman, L.G.; Torti, F.M.; Torti, S.V. Serum ferritin: Past, present and future. Biochim. Biophys. Acta 2010, 1800, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iancu, T.C. Ferritin and hemosiderin in pathological tissues. Electron. Microsc. Rev. 1992, 5, 209–229. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. Iron mobilization from ferritin using alpha-oxohydroxy heteroaromatic chelators. Biochem. J. 1986, 233, 299–302. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J.; Chambers, S.; Hoffbrand, A.V. Comparative study of iron mobilization from haemosiderin, ferritin and iron(III) precipitates by chelators. Biochem. J. 1987, 241, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Settakorn, K.; Kongkarnka, S.; Chompupoung, A.; Svasti, S.; Fucharoen, S.; Porter, J.B.; Srichairatanakool, S.; Koonyosying, P. Effects of green tea extract treatment on erythropoiesis and iron parameters in iron-overloaded β-thalassemic mice. Front. Physiol. 2022, 13, 1053060. [Google Scholar] [CrossRef]
- Jacobs, A. An intracellular transit iron pool. Ciba. Found. Symp. 1976, 51, 91–106. [Google Scholar]
- Mostert, L.J.; Van Dorst, J.A.; Koster, J.F.; Van Eijk, H.G.; Kontoghiorghes, G.J. Free radical and cytotoxic effects of chelators and their iron complexes in the hepatocyte. Free Radic. Res. Commun. 1987, 3, 379–388. [Google Scholar] [CrossRef]
- Chakraborty, D.; Bhattacharrya, M. Deferiprone (L1) induced conformation change of hemoglobin: A fluorescence and CD spectroscopic study. Mol. Cell. Biochem. 2000, 204, 17–20. [Google Scholar] [CrossRef]
- Tran, N.T.; Akkawat, B.; Morales, N.P.; Rojnuckarin, P.; Luechapudiporn, R. Antiplatelet activity of deferiprone through cyclooxygenase-1 inhibition. Platelets 2020, 31, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, S. Ferroptosis Signaling Pathways: Alzheimer’s Disease. Horm. Metab. Res. 2023. [Google Scholar] [CrossRef] [PubMed]
- Simonart, T.; Degraef, C.; Andrei, G.; Mosselmans, R.; Hermans, P.; Van Vooren, J.P.; Noel, J.C.; Boelaert, J.R.; Snoeck, R.; Heenen, M. Iron chelators inhibit the growth and induce the apoptosis of Kaposi’s sarcoma cells and of their putative endothelial precursors. J. Investig. Dermatol. 2000, 115, 893–900. [Google Scholar] [CrossRef]
- Hoque, M.; Hanauske-Abel, H.M.; Palumbo, P.; Saxena, D.; D’Alliessi Gandolfi, D.; Park, M.H.; Pe’ery, T.; Mathews, M.B. Inhibition of HIV-1 gene expression by Ciclopirox and Deferiprone, drugs that prevent hypusination of eukaryotic initiation factor 5A. Retrovirology 2009, 6, 90. [Google Scholar] [CrossRef] [Green Version]
- Andrus, L.; Szabo, P.; Grady, R.W.; Hanauske, A.R.; Huima-Byron, T.; Slowinska, B.; Zagulska, S.; Hanauske-Abel, H.M. Antiretroviral effects of deoxyhypusyl hydroxylase inhibitors: A hypusine-dependent host cell mechanism for replication of human immunodeficiency virus type 1 (HIV-1). Biochem. Pharmacol. 1998, 55, 1807–1818. [Google Scholar] [CrossRef]
- Vu, V.V.; Emerson, J.P.; Martinho, M.; Kim, Y.S.; Münck, E.; Park, M.H.; Que, L. Human deoxyhypusine hydroxylase, an enzyme involved in regulating cell growth, activates O 2 with a nonheme diiron center. Proc. Natl. Acad. Sci. USA 2009, 106, 14814–14819. [Google Scholar] [CrossRef]
- Hirota, K. HIF-α Prolyl Hydroxylase Inhibitors and Their Implications for Biomedicine: A Comprehensive Review. Biomedicines 2021, 9, 468. [Google Scholar] [CrossRef]
- Orfanou, I.-M.; Argyros, O.; Papapetropoulos, A.; Tseleni-Balafouta, S.; Vougas, K.; Tamvakopoulos, C. Discovery and Pharmacological Evaluation of STEAP4 as a Novel Target for HER2 Overexpressing Breast Cancer. Front. Oncol. 2021, 11, 608201. [Google Scholar] [CrossRef]
- Chekmarev, J.; Azad, M.G.; Richardson, D.R. The Oncogenic Signaling Disruptor, NDRG1: Molecular and Cellular Mechanisms of Activity. Cells 2021, 10, 2382. [Google Scholar] [CrossRef]
- Zhang, P.; Tchou-Wong, K.M.; Costa, M. Egr-1 mediates hypoxia-inducible transcription of the NDRG1 gene through an overlapping Egr-1/Sp1 binding site in the promoter. Cancer Res. 2007, 67, 9125–9133. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.S. Zinc: An overview. Nutrition 1995, 11, 93–99. [Google Scholar] [PubMed]
- Coleman, J.E. Zinc Proteins: Enzymes, Storage Proteins, Transcription Factors, and Replication Proteins. Annu. Rev. Biochem. 1992, 61, 897–946. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, P.; Vidal, C.; Dey, S.; Zhang, L. Mitochondria Targeting as an Effective Strategy for Cancer Therapy. Int. J. Mol. Sci. 2020, 21, 3363. [Google Scholar] [CrossRef]
- Beinert, H.; Kennedy, M.C. Aconitase, a two-faced protein: Enzyme and iron regulatory factor. FASEB J. 1993, 7, 1442–1449. [Google Scholar] [CrossRef]
- Forman, H.J. Redox signaling: An evolution from free radicals to aging. Free Radic. Biol. Med. 2016, 97, 398–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stangherlin, A.; Reddy, A.B. Regulation of circadian clocks by redox homeostasis. J. Biol. Chem. 2013, 288, 26505–26511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arevalo, J.A.; Vázquez-Medina, J.P. The Role of Peroxiredoxin 6 in Cell Signaling. Antioxidants 2018, 7, 172. [Google Scholar] [CrossRef] [Green Version]
- Duracková, Z. Some current insights into oxidative stress. Physiol. Res. 2010, 59, 459–469. [Google Scholar] [CrossRef]
- Gutteridge, J.M. Lipid peroxidation and antioxidants as biomarkers of tissue damage. Clin. Chem. 1995, 41, 1819–1828. [Google Scholar] [CrossRef]
- Stadtman, E.R.; Levine, R.L. Free radical-mediated oxidation of free amino acids and amino acid residues in proteins. Amino. Acids. 2003, 25, 207–218. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J.; Kontoghiorghe, C.N. Prospects for the introduction of targeted antioxidant drugs for the prevention and treatment of diseases related to free radical pathology. Expert Opin. Investig. Drugs 2019, 28, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Jackson, M.J.; Lunec, J. In vitro screening of iron chelators using models of free radical damage. Free Radic. Res. Commun. 1986, 2, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J. Prospects for introducing deferiprone as potent pharmaceutical antioxidant. Front. Biosci.-Elite 2009, 1, 161–178. [Google Scholar]
- Sripetchwandee, J.; Pipatpiboon, N.; Chattipakorn, N.; Chattipakorn, S. Combined therapy of iron chelator and antioxidant completely restores brain dysfunction induced by iron toxicity. PLoS ONE 2014, 9, e85115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, S.; Fox, J.; Thyagarajan, B.; Fox, J.H. Brain mitochondrial iron accumulates in Huntington’s disease, mediates mitochondrial dysfunction, and can be removed pharmacologically. Free Radic. Biol. Med. 2018, 120, 317–329. [Google Scholar] [CrossRef]
- Maher, P.; Kontoghiorghes, G.J. Characterization of the neuroprotective potential of derivatives of the iron chelating drug deferiprone. Neurochem. Res. 2015, 40, 609–620. [Google Scholar] [CrossRef]
- Timoshnikov, V.A.; Kobzeva, T.V.; Polyakov, N.E.; Kontoghiorghes, G.J. Inhibition of Fe2+- and Fe3+- induced hydroxyl radical production by the iron-chelating drug deferiprone. Free Radic. Biol. Med. 2015, 78, 118–122. [Google Scholar] [CrossRef]
- Bortolami, M.; Pandolfi, F.; Messore, A.; Rocco, D.; Feroci, M.; Di Santo, R.; De Vita, D.; Costi, R.; Cascarino, P.; Simonetti, G.; et al. Design, synthesis and biological evaluation of a series of iron and copper chelating deferiprone derivatives as new agents active against Candida albicans. Bioorg. Med. Chem. Lett. 2021, 42, 128087. [Google Scholar] [CrossRef]
- Nurchi, V.M.; Crisponi, G.; Pivetta, T.; Donatoni, M.; Remelli, M. Potentiometric, spectrophotometric and calorimetric study on iron(III) and copper(II) complexes with 1,2-dimethyl-3-hydroxy-4-pyridinone. J. Inorg. Biochem. 2008, 102, 684–692. [Google Scholar] [CrossRef]
- Dixon, S.J.; Lemberg, K.M.; Lamprecht, M.R.; Skouta, R.; Zaitsev, E.M.; Gleason, C.E.; Patel, D.N.; Bauer, A.J.; Cantley, A.M.; Yang, W.S.; et al. Ferroptosis: An iron-dependent form of nonapoptotic cell death. Cell 2012, 149, 1060–1072. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.Y.; Dixon, S.J. Mechanisms of ferroptosis. Cell Mol. Life Sci. 2016, 73, 2195–2209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, M.; Monian, P.; Pan, Q.; Zhang, W.; Xiang, J.; Jiang, X. Ferroptosis is an autophagic cell death process. Cell Res. 2016, 26, 1021–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, E.; Chung, S.W. ROS-mediated autophagy increases intracellular iron levels and ferroptosis by ferritin and transferrin receptor regulation. Cell Death Dis. 2019, 10, 822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, W.; Xie, Y.; Song, X.; Sun, X.; Zeh, H.J., 3rd; Kang, R.; Tang, D. Autophagy promotes ferroptosis by degradation of ferritin. Autophagy 2016, 12, 1425–1428. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Chen, X.B.; Ying, M.D.; He, Q.J.; Cao, J.; Yang, B. The Role of Ferroptosis in Cancer Development and Treatment Response. Front. Pharmacol. 2018, 8, 992. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Liang, Y.; Yang, H.; Zhang, W.; Xie, T. The Research Landscape of Ferroptosis in Cancer: A Bibliometric Analysis. Front. Cell Dev. Biol. 2022, 10, 841724. [Google Scholar] [CrossRef]
- Gao, W.; Wang, X.; Zhou, Y.; Wang, X.; Yu, Y. Autophagy, ferroptosis, pyroptosis, and necroptosis in tumor immunotherapy. Signal Transduct. Target. Ther. 2022, 7, 196. [Google Scholar] [CrossRef]
- Lei, G.; Zhuang, L.; Gan, B. Targeting ferroptosis as a vulnerability in cancer. Nat. Cancer 2022, 22, 381–396. [Google Scholar] [CrossRef]
- Wang, D.; Le Tang, L.; Zhang, Y.; Ge, G.; Jiang, X.; Mo, Y.; Wu, P.; Deng, X.; Li, L.; Zuo, S.; et al. Regulatory pathways and drugs associated with ferroptosis in tumors. Cell Death Dis. 2022, 13, 544. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, Q.; Song, H.; Zhang, Y.; Chen, H.; Liu, P.; Sun, T.; Jiang, C. A Triple Therapeutic Strategy with Antiexosomal Iron Efflux for Enhanced Ferroptosis Therapy and Immunotherapy. Small 2022, 18, 2201704. [Google Scholar] [CrossRef]
- Liu, L.; Li, L.; Li, M.; Luo, Z. Autophagy-Dependent Ferroptosis as a Therapeutic Target in Cancer. ChemMedChem 2021, 16, 2942–2950. [Google Scholar] [CrossRef]
- Xiao, L.; Huang, H.; Fan, S.; Zheng, B.; Wu, J.; Zhang, J.; Pi, J.; Xu, J.-F. Ferroptosis: A mixed blessing for infectious diseases. Front. Pharmacol. 2022, 13, 992734. [Google Scholar] [CrossRef]
- Lin, Y.; Xu, W.; Hou, Y.; Wang, S.; Zhang, H.; Ran, M.; Huang, Y.; Wang, Y.; Yang, G. The multifaceted role of ferroptosis in kidney diseases. Chem. Interactions 2022, 365, 110107. [Google Scholar] [CrossRef]
- Thapa, K.; Khan, H.; Kanojia, N.; Singh, T.G.; Kaur, A.; Kaur, G. Therapeutic Insights on Ferroptosis in Parkinson’s disease. Eur J Pharmacol. 2022, 930, 175133. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Chen, X.-Z.; Wang, Y.-H.; Cheng, X.-L.; Zhao, Y.; Zhou, L.-Y.; Wang, K. Emerging roles of ferroptosis in cardiovascular diseases. Cell Death Discov. 2022, 8, 394. [Google Scholar] [CrossRef]
- Jacobs, W.; Lammens, M.; Kerckhofs, A.; Voets, E.; Van San, E.; Van Coillie, S.; Peleman, C.; Mergeay, M.; Sirimsi, S.; Matheeussen, V.; et al. Fatal lymphocytic cardiac damage in coronavirus disease 2019 (COVID-19): Autopsy reveals a ferroptosis signature. ESC Heart Fail. 2020, 7, 3772–3781. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, L.; Zhou, F. Cuproptosis: A new form of programmed cell death. Cell. Mol. Immunol. 2022, 19, 867–868. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, V. Selective Targeting of Cancer Cells by Copper Ionophores: An Overview. Front. Mol. Biosci. 2022, 9, 841814. [Google Scholar] [CrossRef]
- Cobine, P.A.; Moore, S.A.; Leary, S.C. Getting out what you put in: Copper in mitochondria and its impacts on human disease. Biochim. Biophys. Acta Mol. Cell Res. 2021, 1868, 118867. [Google Scholar] [CrossRef]
- Tang, D.; Chen, X.; Kroemer, G. Cuproptosis: A copper-triggered modality of mitochondrial cell death. Cell Res. 2022, 32, 417–418. [Google Scholar] [CrossRef] [PubMed]
- Ke, D.; Zhang, Z.; Liu, J.; Chen, P.; Li, J.; Sun, X.; Chu, Y.; Li, L. Ferroptosis, necroptosis and cuproptosis: Novel forms of regulated cell death in diabetic cardiomyopathy. Front. Cardiovasc. Med. 2023, 10, 1135723. [Google Scholar] [CrossRef]
- Wang, Z.; Jin, D.; Zhou, S.; Dong, N.; Ji, Y.; An, P.; Wang, J.; Luo, Y.; Luo, J. Regulatory roles of copper metabolism and cuproptosis in human cancers. Front. Oncol. 2023, 13, 1123420. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.J.; Xue, Y.T.; Liu, Y. Cuproptosis, the novel therapeutic mechanism for heart failure: A narrative review. Cardiovasc. Diagn. Ther. 2022, 12, 681–692. [Google Scholar] [CrossRef]
- Timoshnikov, V.A.; Kobzeva, T.V.; Polyakov, N.E.; Kontoghiorghes, G.J. Redox Interactions of Vitamin C and Iron: Inhibition of the Pro-Oxidant Activity by Deferiprone. Int. J. Mol. Sci. 2020, 21, 3967. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Kolnagou, A.; Kontoghiorghe, C.N.; Mourouzidis, L.; Timoshnikov, V.A.; Polyakov, N.E. Trying to Solve the Puzzle of the Interaction of Ascorbic Acid and Iron: Redox, Chelation and Therapeutic Implications. Medicines 2020, 7, 45. [Google Scholar] [CrossRef]
- Fredenburg, A.M.; Sethi, R.K.; Allen, D.D.; Yokel, R.A. The pharmacokinetics and blood-brain barrier permeation of the chelators 1,2 dimethly-, 1,2 diethyl-, and 1-[ethan-1’ol]-2-methyl-3-hydroxypyridin-4-one in the rat. Toxicology 1996, 108, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Arthur, A.S.; Fergus, A.H.; Lanzino, G.; Mathys, J.; Kassell, N.F.; Lee, K.S. Systemic administration of the iron chelator deferiprone attenuates subarachnoid hemorrhage-induced cerebral vasospasm in the rabbit. Neurosurgery 1997, 41, 1385–1391; discussion 1391–1392. [Google Scholar] [CrossRef]
- Zhang, Q.; Feng, S.; Zhao, Y.; Jin, B.; Peng, R. Design and synthesis of N-hydroxyalkyl substituted deferiprone: A kind of iron chelating agents for Parkinson’s disease chelation therapy strategy. J. Biol. Inorg. Chem. 2021, 26, 467–478. [Google Scholar] [CrossRef]
- Flores Martin, A.; Shanmugarajah, P.; Hoggard, N.; Hadjivassiliou, M. Treatment Response of Deferiprone in Infratentorial Superficial Siderosis: A Systematic Review. Cerebellum 2021, 20, 454–461. [Google Scholar] [CrossRef]
- Morales, N.P.; Rodrat, S.; Piromkraipak, P.; Yamanont, P.; Paiboonsukwong, K.; Fucharoen, S. Iron chelation therapy with deferiprone improves oxidative status and red blood cell quality and reduces redox-active iron in β-thalassemia/hemoglobin E patients. Biomed. Pharmacother. 2022, 145, 112381. [Google Scholar] [CrossRef]
- Badat, M.; Kaya, B.; Telfer, P. Combination-therapy with concurrent deferoxamine and deferiprone is effective in treating resistant cardiac iron-loading in aceruloplasminaemia. Br. J. Haematol. 2015, 171, 430–432. [Google Scholar] [CrossRef] [Green Version]
- Tauchenová, L.; Křížová, B.; Kubánek, M.; Fraňková, S.; Melenovský, V.; Tintěra, J.; Kautznerová, D.; Malušková, J.; Jirsa, M.; Kautzner, J. Successful Treatment of Iron-Overload Cardiomyopathy in Hereditary Hemochromatosis With Deferoxamine and Deferiprone. Can. J. Cardiol. 2016, 32, 1574.e1–1574.e3. [Google Scholar] [CrossRef]
- Fabio, G.; Minonzio, F.; Delbini, P.; Bianchi, A.; Cappellini, M.D. Reversal of cardiac complications by deferiprone and deferoxamine combination therapy in a patient affected by a severe type of juvenile hemochromatosis (JH). Blood 2007, 109, 362–364. [Google Scholar] [CrossRef]
- Sudmantaitė, V.; Čelutkienė, J.; Glaveckaite, S.; Katkus, R. Difficult diagnosis of cardiac haemochromatosis: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tanner, M.A.; Galanello, R.; Dessi, C.; Smith, G.C.; Westwood, M.A.; Agus, A.; Roughton, M.; Assomull, R.; Nair, S.V.; Walker, J.M.; et al. A randomized, placebo-controlled, double-blind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonance. Circulation 2007, 115, 1876–1884. [Google Scholar] [CrossRef]
- Chan, S.; Lian, Q.; Chen, M.P.; Jiang, D.; Ho, J.T.K.; Cheung, Y.F.; Chan, G.C. Deferiprone inhibits iron overload-induced tissue factor bearing endothelial microparticle generation by inhibition oxidative stress induced mitochondrial injury, and apoptosis. Toxicol. Appl. Pharmacol. 2018, 338, 148–158. [Google Scholar] [CrossRef]
- Sadrzadeh, S.M.; Nanji, A.A.; Price, P.L. The oral iron chelator, 1,2-dimethyl-3-hydroxypyrid-4-one reduces hepatic-free iron, lipid peroxidation and fat accumulation in chronically ethanol-fed rats. J. Pharmacol. Exp. Ther. 1994, 269, 632–636. [Google Scholar] [PubMed]
- Vreugdenhil, G.; Swaak, A.J.; Kontoghiorghes, G.J.; Van Eijk, H.G. Efficacy and Safety of Oral Iron Chelator L1 in Anaemic Rheumatoid Arthritis Patients. Lancet 1989, 334, 1. [Google Scholar] [CrossRef]
- Vreugdenhil, G.; Swaak, A.J.; de Jeu-Jaspers, C.; van Eijk, H.G. Correlation of iron exchange between the oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one(L1) and transferrin and possible antianaemic effects of L1 in rheumatoid arthritis. Ann. Rheum. Dis. 1990, 49, 956–957. [Google Scholar] [CrossRef] [PubMed]
- Vreugdenhil, G.; Kontoghiorghes, G.J.; Van Eijk, H.G.; Swaak, A.J. Impaired erythropoietin responsiveness to the anaemia in rheumatoid arthritis. A possible inverse relationship with iron stores and effects of the oral iron chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Clin. Exp. Rheumatol. 1991, 9, 35–40. [Google Scholar] [PubMed]
- Kontoghiorghes, G.J.; Barr, J.; Baillod, R.A. Studies of aluminium mobilization in renal dialysis patients using the oral chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Arzneimittelforschung 1994, 44, 522–526. [Google Scholar] [PubMed]
- Matthews, A.J.; Vercellotti, G.M.; Menchaca, H.J.; Bloch, P.H.; Michalek, V.N.; Marker, P.H.; Murar, J.; Buchwald, H. Iron and atherosclerosis: Inhibition by the iron chelator deferiprone (L1). J. Surg. Res. 1997, 73, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Neocleous, K.; Kolnagou, A. Benefits and risks of deferiprone in iron overload in Thalassaemia and other conditions: Comparison of epidemiological and therapeutic aspects with deferoxamine. Drug Saf. 2003, 26, 553–584. [Google Scholar] [CrossRef] [PubMed]
- Reuter, D.G.; Tacker, W.A., Jr.; Babbs, C.F.; Badylak, S.F.; Voorhees, W.D., 3rd; Konrad, P.E. Preliminary results of deferoxamine and L1 treatment of spinal cord ischemia. J. Thorac. Cardiovasc. Surg. 1995, 109, 1017–1019. [Google Scholar] [CrossRef] [Green Version]
- Venkataram, S.; Rahman, Y.E. Studies of an oral iron chelator: 1,2-dimethyl-3-hydroxy-pyrid-4-one. I. Iron excretion in rats: Development of a new rapid microwave method for iron analysis in faeces. Br. J. Haematol. 1990, 75, 274–277. [Google Scholar] [CrossRef]
- Chang, Y.H.; Shaw, C.F.; Wu, K.H.; Hsieh, K.H.; Su, Y.N.; Lu, P.J. Treatment with deferiprone for iron overload alleviates bone marrow failure in a Fanconi anemia patient. Hemoglobin 2009, 33, 346–351. [Google Scholar] [CrossRef]
- Smeets, M.E.; Vreugdenhil, G.; Holdrinet, R.S. Improvement of erythropoiesis during treatment with deferiprone in a patient with myelofibrosis and transfusional hemosiderosis. Am. J. Hematol. 1996, 51, 243–244. [Google Scholar] [CrossRef]
- Umeno, A.; Biju, V.; Yoshida, Y. In vivo ROS production and use of oxidative stress-derived biomarkers to detect the onset of diseases such as Alzheimer’s disease, Parkinson’s disease, and diabetes. Free Radic. Res. 2017, 51, 413–427. [Google Scholar] [CrossRef]
- Brar, S.; Henderson, D.; Schenck, J.; Zimmerman, E.A. Iron accumulation in the substantia nigra of patients with Alzheimer disease and parkinsonism. Arch. Neurol. 2009, 66, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Wallis, L.I.; Paley, M.N.; Graham, J.M.; Grünewald, R.A.; Wignall, E.L.; Joy, H.M.; Griffiths, P.D. MRI assessment of basal ganglia iron deposition in Parkinson’s disease. J. Magn. Reson. Imaging 2008, 28, 1061–1067. [Google Scholar] [CrossRef]
- Waldvogel, D.; van Gelderen, P.; Hallett, M. Increased iron in the dentate nucleus of patients with Friedrich’s ataxia. Ann. Neurol. 1999, 46, 123–125. [Google Scholar] [CrossRef]
- Iankova, V.; Karin, I.; Klopstock, T.; Schneider, S.A.; Iankova, V.; Karin, I.; Klopstock, T.; Schneider, S.A. Emerging Disease-Modifying Therapies in Neurodegeneration With Brain Iron Accumulation (NBIA) Disorders. Front. Neurol. 2021, 12, 629414. [Google Scholar] [CrossRef] [PubMed]
- Rajapurkar, M.M.; Lele, S.S.; Malavade, T.S.; Kansara, M.R.; Hegde, U.N.; Gohel, K.D.; Gang, S.D.; Shah, S.V.; Mukhopadhyay, B.N. Serum catalytic Iron: A novel biomarker for coronary artery disease in patients on maintenance hemodialysis. Indian J. Nephrol. 2013, 23, 332–337. [Google Scholar] [CrossRef]
- Li, J.Y.; Liu, S.Q.; Yao, R.Q.; Tian, Y.P.; Yao, Y.M. A Novel Insight Into the Fate of Cardiomyocytes in Ischemia-Reperfusion Injury: From Iron Metabolism to Ferroptosis. Front. Cell Dev. Biol. 2021, 9, 799499. [Google Scholar] [CrossRef]
- Boddaert, N.; Le Quan Sang, K.H.; Rötig, A.; Leroy-Willig, A.; Gallet, S.; Brunelle, F.; Sidi, D.; Thalabard, J.C.; Munnich, A.; Cabantchik, Z.I. Selective iron chelation in Friedreich ataxia: Biologic and clinical implications. Blood 2007, 110, 401–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbruzzese, G.; Cossu, G.; Balocco, M.; Marchese, R.; Murgia, D.; Melis, M.; Galanello, R.; Barella, S.; Matta, G.; Ruffinengo, U.; et al. A pilot trial of deferiprone for neurodegeneration with brain iron accumulation. Haematologica 2011, 96, 1708–1711. [Google Scholar] [CrossRef] [Green Version]
- Cossu, G.; Abbruzzese, G.; Matta, G.; Murgia, D.; Melis, M.; Ricchi, V.; Galanello, R.; Barella, S.; Origa, R.; Balocco, M.; et al. Efficacy and safety of deferiprone for the treatment of pantothenate kinase-associated neurodegeneration (PKAN) and neurodegeneration with brain iron accumulation (NBIA): Results from a four years follow-up. Park. Relat. Disord.. 2014, 20, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, G.; Zibordi, F.; Chiapparini, L.; Bertini, E.; Russo, L.; Piga, A.; Longo, F.; Garavaglia, B.; Aquino, D.; Savoiardo, M.; et al. Iron-related MRI images in patients with pantothenate kinase-associated neurodegeneration (PKAN) treated with deferiprone: Results of a phase II pilot trial. Mov. Disord. 2011, 26, 1756–1759. [Google Scholar] [CrossRef]
- Forni, G.L.; Balocco, M.; Cremonesi, L.; Abbruzzese, G.; Parodi, R.C.; Marchese, R. Regression of symptoms after selective iron chelation therapy in a case of neurodegeneration with brain iron accumulation. Mov. Disord. 2008, 23, 904–907. [Google Scholar] [CrossRef]
- Rohani, M.; Razmeh, S.; Shahidi, G.A.; Alizadeh, E.; Orooji, M. A pilot trial of deferiprone in pantothenate kinase-associated neurodegeneration patients. Neurol. Int. 2018, 9, 7279. [Google Scholar] [CrossRef]
- Devos, D.; Cabantchik, Z.I.; Moreau, C.; Danel, V.; Mahoney-Sanchez, L.; Bouchaoui, H.; Gouel, F.; Rolland, A.S.; Duce, J.A.; Devedjian, J.C.; et al. Conservative iron chelation for neurodegenerative diseases such as Parkinson’s disease and amyotrophic lateral sclerosis. J. Neural. Transm. 2020, 127, 189–203. [Google Scholar] [CrossRef]
- Martin-Bastida, A.; Ward, R.J.; Newbould, R.; Piccini, P.; Sharp, D.; Kabba, C.; Patel, M.C.; Spino, M.; Connelly, J.; Tricta, F.; et al. Brain iron chelation by deferiprone in a phase 2 randomised double-blinded placebo controlled clinical trial in Parkinson’s disease. Sci. Rep. 2017, 7, 1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devos, D.; Labreuche, J.; Rascol, O.; Corvol, J.C.; Duhamel, A.; Guyon Delannoy, P.; Poewe, W.; Compta, Y.; Pavese, N.; Růžička, E.; et al. Trial of Deferiprone in Parkinson’s Disease. N. Engl. J. Med. 2022, 387, 2045–2055. [Google Scholar] [CrossRef] [PubMed]
- Rajapurkar, M.M.; Hegde, U.; Bhattacharya, A.; Alam, M.G.; Shah, S.V. Effect of deferiprone, an oral iron chelator, in diabetic and non-diabetic glomerular disease. Toxicol. Mech. Methods 2013, 23, 5–10. [Google Scholar] [CrossRef]
- Saxena, D.; Spino, M.; Tricta, F.; Connelly, J.; Cracchiolo, B.M.; Hanauske, A.R.; D’Alliessi Gandolfi, D.; Mathews, M.B.; Karn, J.; Holland, B.; et al. Drug-Based Lead Discovery: The Novel Ablative Antiretroviral Profile of Deferiprone in HIV-1-Infected Cells and in HIV-Infected Treatment-Naive Subjects of a Double-Blind, Placebo-Controlled, Randomized Exploratory Trial. PLoS ONE 2016, 11, e0154842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohanty, D.; Ghosh, K.; Pathare, A.V.; Karnad, D. Deferiprone (L1) as an adjuvant therapy for Plasmodium falciparum malaria. Indian J. Med. Res. 2002, 115, 17–21. [Google Scholar]
- Thuma, P.E.; Olivieri, N.F.; Mabeza, G.F.; Biemba, G.; Parry, D.; Zulu, S.; Fassos, F.F.; McClelland, R.A.; Koren, G.; Brittenham, G.M.; et al. Assessment of the effect of the oral iron chelator deferiprone on asymptomatic Plasmodium falciparum parasitemia in humans. Am. J. Trop. Med. Hyg. 1998, 58, 358–364. [Google Scholar] [CrossRef]
- Blanusa, M.; Varnai, V.M.; Piasek, M.; Kostial, K. Chelators as Antidotes of Metal Toxicity: Therapeutic and Experimental Aspects. Curr. Med. Chem. 2005, 12, 2771–2794. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. Advances on Chelation and Chelator Metal Complexes in Medicine. Int. J. Mol. Sci. 2020, 21, 2499. [Google Scholar] [CrossRef] [Green Version]
- Ritacca, A.G.; Malacaria, L.; Algieri, V.; De Nino, A.; Russo, N.; Furia, E.; Maiuolo, L.; Sicilia, E. Sequestering Ability of a Synthetic Chelating Agent towards Copper(II) and Iron(III): A Detailed Theoretical and Experimental Analysis. Chem. Asian J. 2020, 15, 3266–3274. [Google Scholar] [CrossRef]
- Baldari, S.; Di Rocco, G.; Toietta, G. Current Biomedical Use of Copper Chelation Therapy. Int. J. Mol. Sci. 2020, 21, 1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barve, A.; Kumbhar, A.; Bhat, M.; Joshi, B.; Butcher, R.; Sonawane, U.; Joshi, R. Mixed-ligand copper(II) maltolate complexes: Synthesis, characterization, DNA binding and cleavage, and cytotoxicity. Inorg. Chem. 2009, 48, 9120–9132. [Google Scholar] [CrossRef] [PubMed]
- Imberti, C.; Adumeau, P.; Blower, J.E.; Al Salemee, F.; Torres, J.B.; Lewis, J.S.; Zeglis, B.M.; Terry, S.Y.A.; Blower, P.J. Manipulating the In Vivo Behaviour of 68Ga with Tris(Hydroxypyridinone) Chelators: Pretargeting and Blood Clearance. Int. J. Mol. Sci. 2020, 21, 1496. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Yao, Y.N.; Wu, S.D.; Dong, H.J.; Feng, G.C.; Yuan, X.Y. The efficacy of deferiprone on tissues aluminum removal and copper, zinc, manganese level in rabbits. J. Inorg. Biochem. 2005, 99, 1733–1737. [Google Scholar] [CrossRef]
- Weinberg, E.D. Iron depletion: A defense against intracellular infection and neoplasm. Life Sci. 1992, 50, 1289–1297. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J.; Weinberg, E.D. Iron: Mammalian defense systems, mechanisms of disease, and chelation therapy approaches. Blood Rev. 1995, 9, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Kolnagou, A.; Skiada, A.; Petrikkos, G. The role of iron and chelators on infections in iron overload and non iron loaded conditions: Prospects for the design of new antimicrobial therapies. Hemoglobin 2010, 34, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Lai, X.; Fu, J.; Yang, J.; Zhao, B.; Shang, H.; Huang, R.; Chen, X. A novel C19ORF12 mutation in two MPAN sisters treated with deferiprone. BMC Neurol. 2023, 23, 134. [Google Scholar] [CrossRef]
- Ammendola, S.; Secli, V.; Pacello, F.; Bortolami, M.; Pandolfi, F.; Messore, A.; Di Santo, R.; Scipione, L.; Battistoni, A. Salmonella Typhimurium and Pseudomonas aeruginosa Respond Differently to the Fe Chelator Deferiprone and to Some Novel Deferiprone Derivatives. Int. J. Mol. Sci. 2021, 22, 10217. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. New Iron Metabolic Pathways and Chelation Targeting Strategies Affecting the Treatment of All Types and Stages of Cancer. Int. J. Mol. Sci. 2022, 23, 13990. [Google Scholar] [CrossRef]
- Voest, E.E.; Vreugdenhil, G.; Marx, J.J.M. Iron-chelating agents in non-iron overload conditions. Ann. Intern. Med. 1994, 120, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghe, C.N.; Kolnagou, A.; Kontoghiorghes, G.J. Phytochelators Intended for Clinical Use in Iron Overload, Other Diseases of Iron Imbalance and Free Radical Pathology. Molecules 2015, 20, 20841–20872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athanassiou-Metaxa, M.; Kousi, A.; Hatzipantelis, E.S.; Tsatra, I.; Ikonomou, M.; Perifanis, V.; Tsantali, H. Combined chelation therapy with deferiprone and desferrioxamine in iron overloaded beta-thalassemia patients. Haematologica 2004, 89, ELT07. [Google Scholar] [PubMed]
- Chuang, T.Y.; Li, J.P.; Weng, T.F.; Wu, K.H.; Chao, Y.H. Combined chelation with high-dose deferiprone and deferoxamine to improve survival and restore cardiac function effectively in patients with transfusion-dependent thalassemia presenting severe cardiac complications. Ann. Hematol. 2020, 99, 2289–2294. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghes, G.J.; Kolnagou, A. Effective new treatments of iron overload in thalassaemia using the ICOC combination therapy protocol of deferiprone (L1) and deferoxamine and of new chelating drugs. Haematologica 2006, 91, ELT04. [Google Scholar] [PubMed]
- Kontoghiorghes, G.J. Advances in oral iron chelation in man. Int. J. Hematol. 1992, 55, 27–38. [Google Scholar]
- Elalfy, M.S.; Adly, A.M.; Wali, Y.; Tony, S.; Samir, A.; Elhenawy, Y.I. Efficacy and safety of a novel combination of two oral chelators deferasirox/deferiprone over deferoxamine/deferiprone in severely iron overloaded young beta thalassemia major patients. Eur. J. Haematol. 2015, 95, 411–420. [Google Scholar] [CrossRef]
- Eghbali, A.; Shokri, P.; Afzal, R.R.; Bagheri, B. A 1-year randomized trial of deferasirox alone versus deferasirox and deferoxamine combination for the treatment of iron overload in thalassemia major. Transfus. Apher. Sci. 2019, 58, 429–433. [Google Scholar] [CrossRef]
- Cassinerio, E.; Orofino, N.; Roghi, A.; Duca, L.; Poggiali, E.; Fraquelli, M.; Zanaboni, L.; Cappellini, M.D. Combination of deferasirox and deferoxamine in clinical practice: An alternative scheme of chelation in thalassemia major patients. Blood Cells Mol. Dis. 2014, 53, 164–167. [Google Scholar] [CrossRef]
- Song, T.S.; Hsieh, Y.W.; Peng, C.T.; Chen, T.L.; Lee, H.Z.; Chung, J.G.; Hour, M.J. Combined versus monotherapy or concurrent therapy for treatment of thalassaemia. In Vivo 2014, 28, 645–649. [Google Scholar]
- Lai, Y.W.; Campbell, L.T.; Wilkins, M.R.; Pang, C.N.; Chen, S.; Carter, D.A. Synergy and antagonism between iron chelators and antifungal drugs in Cryptococcus. Int. J. Antimicrob. Agents 2016, 48, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Lamas, G.A.; Anstrom, K.J.; Navas-Acien, A.; Boineau, R.; Kim, H.; Rosenberg, Y.; Stylianou, M.; Jones, T.L.Z.; Joubert, B.R.; Santella, R.M.; et al. The trial to assess chelation therapy 2 (TACT2): Rationale and design. Am. Heart J. 2022, 252, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Alam, Z.H.; Ujueta, F.; Arenas, I.A.; Nigra, A.E.; Navas-Acien, A.; Lamas, G.A. Urinary Metal Levels after Repeated Edetate Disodium Infusions: Preliminary Findings. Int. J. Environ. Res. Public Health 2020, 17, 4684. [Google Scholar] [CrossRef]
- Pippard, M.J.; Jackson, M.J.; Hoffman, K.; Petrou, M.; Modell, C.B. Iron chelation using subcutaneous infusion of diethylene triamine penta-acetic acid (DTPA). Scand. J. Haematol. 1986, 36, 466–472. [Google Scholar] [CrossRef]
- Grémy, O.; Devilliers, K.; Miccoli, L. Chelation therapy with 3,4,3-Li(1,2-HOPO) after pulmonary exposure to plutonium in rats. Chem. Biol. Interact. 2023, 378, 110488. [Google Scholar] [CrossRef]
- Dumit, S.; Miller, G.; Poudel, D.; Bertelli, L.; Klumpp, J. Chelation Model Validation: Modeling of a Plutonium-238 Inhalation Incident Treated with DTPA at Los Alamos National Laboratory. Health Phys. 2023, 124, 113–124. [Google Scholar] [CrossRef]
- Rahimi, P.; Barootkoob, B.; ElHashash, A.; Nair, A. Efficacy of Dexrazoxane in Cardiac Protection in Pediatric Patients Treated With Anthracyclines. Cureus 2023, 15, e37308. [Google Scholar] [CrossRef]
- Mody, H.; Vaidya, T.R.; Ait-Oudhia, S. In vitro to clinical translational pharmacokinetic/pharmacodynamic modeling of doxorubicin (DOX) and dexrazoxane (DEX) interactions: Safety assessment and optimization. Sci. Rep. 2023, 13, 3100. [Google Scholar] [CrossRef] [PubMed]
- de Baat, E.C.; van Dalen, E.C.; Mulder, R.L.; Hudson, M.M.; Ehrhardt, M.J.; Engels, F.K.; Feijen, E.A.M.; Grotenhuis, H.B.; Leerink, J.M.; Kapusta, L.; et al. Primary cardioprotection with dexrazoxane in patients with childhood cancer who are expected to receive anthracyclines: Recommendations from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Child Adolesc. Health 2022, 6, 885–894. [Google Scholar] [CrossRef]
- Barnabé, N.; Zastre, J.A.; Venkataram, S.; Hasinoff, B.B. Deferiprone protects against doxorubicin-induced myocyte cytotoxicity. Free Radic. Biol. Med. 2002, 33, 266–275. [Google Scholar] [CrossRef]
- Mancuso, A.; Maggio, A.; Renda, D.; Di Marzo, R.; Rigano, P. Treatment with hydroxycarbamide for intermedia thalassaemia: Decrease of efficacy in some patients during long-term follow up. Br. J. Haematol. 2006, 133, 105–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinou, E.; Pashalidis, I.; Kolnagou, A.; Kontoghiorghes, G.J. Interactions of hydroxycarbamide (hydroxyurea) with iron and copper: Implications on toxicity and therapeutic strategies. Hemoglobin 2011, 35, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Manganas, K.; Delicou, S.; Xydaki, A.; Koskinas, J. Iron Chelators, Such as Deferasirox, When Combined With Hydroxyurea, Provide an Additional Benefit of Iron Chelation in Patients Receiving Chronic Transfusion Therapy. Hemoglobin 2022, 46, 114–117. [Google Scholar] [CrossRef]
- Djaldetti, M.; Fishman, P.; Notti, I.; Bessler, H. The effect of tetracycline administration on iron absorption in mice. Biomed. J. 1981, 35, 150–152. [Google Scholar]
- Elalfy, M.S.; Saber, M.M.; Adly, A.A.; Ismail, E.A.; Tarif, M.; Ibrahim, F.; Elalfy, O.M. Role of vitamin C as an adjuvant therapy to different iron chelators in young β-thalassemia major patients: Efficacy and safety in relation to tissue iron overload. Eur. J. Haematol. 2016, 96, 318–326. [Google Scholar] [CrossRef]
- Conte, D.; Brunelli, L.; Ferrario, L.; Mandelli, C.; Quatrini, M.; Velio, P.; Bianchi, P.A. Effect of ascorbic acid on desferrioxamine-induced urinary iron excretion in idiopathic hemochromatosis. Acta Haematol. 1984, 72, 117–120. [Google Scholar] [CrossRef]
- De Virgilis, S.; Cognia, M.; Turco, M.P.; Frau, F.; Dessi, C.; Argiolou, F.; Sorcinelli, R.; Sitzia, A.; Cao, A. Depletion of trace elements and acute occular toxicity induced by desferrioxamine in patients with thalassaemia. Arch. Dis. Child. 1988, 63, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Binding, A.; Ward, R.; Tomlinson, G.; Kuo, K.H.M. Deferiprone exerts a dose-dependent reduction of liver iron in adults with iron overload. Eur. J. Haematol. 2019, 103, 80–87. [Google Scholar] [CrossRef]
- Aessopos, A.; Kati, M.; Farmakis, D.; Polonifi, E.; Deftereos, S.; Tsironi, M. Intensive chelation therapy in beta-thalassemia and possible adverse cardiac effects of desferrioxamine. Int. J. Hematol. 2007, 86, 212–215. [Google Scholar] [CrossRef]
- Yao, F.; Peng, J.; Zhang, E.; Ji, D.; Gao, Z.; Tang, Y.; Yao, X.; Xia, X. Pathologically high intraocular pressure disturbs normal iron homeostasis and leads to retinal ganglion cell ferroptosis in glaucoma. Cell Death Differ. 2023, 30, 69–81. [Google Scholar] [CrossRef]
- Simões, R.V.; Veeraperumal, S.; Serganova, I.S.; Kruchevsky, N.; Varshavsky, J.; Blasberg, R.G.; Ackerstaff, E.; Koutcher, J.A. Inhibition of prostate cancer proliferation by Deferiprone. NMR Biomed. 2017, 30, 3712. [Google Scholar] [CrossRef]
- Fiorillo, M.; Tóth, F.; Brindisi, M.; Sotgia, F.; Lisanti, M.P. Deferiprone (DFP) Targets Cancer Stem cell (CSC) Propagation by Inhibiting Mitochondrial Metabolism and Inducing ROS Production. Cells 2020, 9, 1529. [Google Scholar] [CrossRef]
- Kontoghiorghes, G.J. How to manage iron toxicity in post-allogeneic hematopoietic stem cell transplantation? Expert Rev. Hematol. 2020, 13, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vroegindeweij, L.H.P.; Boon, A.J.W.; Wilson, J.H.P.; Langendonk, J.G. Effects of iron chelation therapy on the clinical course of aceruloplasminemia: An analysis of aggregated case reports. Orphanet. J. Rare Dis. 2020, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dessì, C.; Leoni, G.; Moi, P.; Danjou, F.; Follesa, I.; Foschini, M.L.; Morittu, M.; Zappu, A.; Defraia, E.; Bina, P.; et al. Thalassemia major between liver and heart: Where we are now. Blood Cells Mol. Dis. 2015, 55, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.C.; Wang, N.N.; Li, R.; Sun, X.C.; Liao, J.W.; Yang, G.; Liu, S. Ferritinophagy activation and sideroflexin1-dependent mitochondrial iron overload contribute to patulin-induced cardiac inflammation and fibrosis. Sci. Total. Environ. 2023, 892, 164472. [Google Scholar] [CrossRef] [PubMed]
- Lupu, M.; Coada, C.A.; Tudor, D.V.; Baldea, I.; Florea, A.; Toma, V.A.; Lupsor, A.; Moldovan, R.; Decea, N.; Filip, G.A. Iron chelation alleviates multiple pathophysiological pathways in a rat model of cardiac pressure overload. Free Radic. Biol. Med. 2023, 200, 1–10. [Google Scholar] [CrossRef]
- Park, M.; Cho, Y.L.; Choi, Y.; Min, J.K.; Park, Y.J.; Yoon, S.J.; Kim, D.S.; Son, M.Y.; Chung, S.W.; Lee, H.; et al. Particulate matter induces ferroptosis by accumulating iron and dysregulating the antioxidant system. BMB Rep. 2023, 56, 96–101. [Google Scholar] [CrossRef]
- Campbell, N.R.; Hasinoff, B.B. Iron supplements: A common cause of drug interactions. Br. J. Clin. Pharmacol. 1991, 31, 251–255. [Google Scholar] [CrossRef]
- Flora, S.J.; Mittal, M.; Mehta, A. Heavy metal induced oxidative stress its possible reversal by chelation therapy. Indian J. Med. Res. 2008, 128, 501–523. [Google Scholar]
- Kontoghiorghes, G.J. Regulatory molecules and chelators used for the control of essential and toxic metals in health and disease: From molecular interactions to clinical effects and applications. Curr. Med. Chem. 2005, 12, 2661–2662. [Google Scholar] [CrossRef]
- Petrova, E.; Gluhcheva, Y.; Pavlova, E.; Vladov, I.; Dorkov, P.; Schaier, M.; Pashkunova-Martic, I.; Helbich, T.H.; Keppler, B.; Ivanova, J. Effects of Salinomycin and Deferiprone on Lead-Induced Changes in the Mouse Brain. Int. J. Mol. Sci. 2023, 24, 2871. [Google Scholar] [CrossRef] [PubMed]
- Hodková, A.; Cerná, P.; Kotyzová, D.; Eybl, V. The effect of iron(III) on the activity of selenoenzymes and oxidative damage in the liver of rats. Interaction with natural antioxidants and deferiprone. Hemoglobin 2010, 34, 278–283. [Google Scholar] [CrossRef] [PubMed]
- el-Jammal, A.; Howell, P.L.; Turner, M.A.; Li, N.; Templeton, D.M. Copper complexation by 3-hydroxypyridin-4-one iron chelators: Structural and iron competition studies. J. Med. Chem. 1994, 37, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Talukdar, H.; Gogoi, S.R.; Sultana, S.Y.; Begum, R.; Dowerah, D.; Sarma, B.; Islam, N.S. Oxido- and mixed-ligand peroxido complexes of niobium(V) as potent phosphatase inhibitors and efficient catalysts for eco-friendly styrene epoxidation. Dalton Trans. 2023. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.; Arora, G.; Dickson, K.; Lehmann, C. Iron Chelation in Local Infection. Molecules 2021, 26, 189. [Google Scholar] [CrossRef]
- Richter, K.; Ramezanpour, M.; Thomas, N.; Prestidge, C.A.; Wormald, P.J.; Vreugde, S. Mind “De GaPP”: In vitro efficacy of deferiprone and gallium-protoporphyrin against Staphylococcus aureus biofilms. Int. Forum. Allergy Rhinol. 2016, 6, 737–743. [Google Scholar] [CrossRef]
- Botzenhardt, S.; Li, N.; Chan, E.W.; Sing, C.W.; Wong, I.C.; Neubert, A. Safety profiles of iron chelators in young patients with haemoglobinopathies. Eur. J. Haematol. 2017, 98, 198–217. [Google Scholar] [CrossRef] [Green Version]
- Kearney, M.; Orrell, R.W.; Fahey, M.; Brassington, R.; Pandolfo, M. Pharmacological treatments for Friedreich ataxia. Cochrane Database Syst. Rev. 2016, 2016, CD007791. [Google Scholar] [CrossRef] [Green Version]
- Diamantidis, M.D.; Neokleous, N.; Agapidou, A.; Vetsiou, E.; Manafas, A.; Fotiou, P.; Vlachaki, E. Iron chelation therapy of transfusion-dependent β-thalassemia during pregnancy in the era of novel drugs: Is deferasirox toxic? Int. J. Hematol. 2016, 103, 537–544. [Google Scholar] [CrossRef]
- Piga, A.; Longo, F.; Musallam, K.M.; Cappellini, M.D.; Forni, G.L.; Quarta, G.; Chiavilli, F.; Commendatore, F.; Mulas, S.; Caruso, V.; et al. Assessment and management of iron overload in β-thalassaemia major patients during the 21st century: A real-life experience from the Italian WEBTHAL project. Br. J. Haematol. 2013, 161, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Ruivard, M. Iron chelating therapy in adults: How and when ? Rev. Med. Interne. 2013, 34, 32–38. (In French) [Google Scholar] [CrossRef]
- Ha, S.Y.; Mok, A.S.; Chu, W.C.; Rasalkar, D.D.; Cheuk, D.K.; Chiang, A.K.; Ho, M.H.; Chan, G.C. Intermediate-term evaluation of a pratical chelation protocol based on stratification of thalassemic patients by serum ferritin and magnetic resonance imaging cardiac t2*. Hemoglobin 2011, 35, 199–205. [Google Scholar] [CrossRef] [PubMed]
- ElAlfy, M.S.; Sari, T.T.; Lee, C.L.; Tricta, F.; El-Beshlawy, A. The safety, tolerability, and efficacy of a liquid formulation of deferiprone in young children with transfusional iron overload. J. Pediatr. Hematol. Oncol. 2010, 32, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Bortolami, M.; Pandolfi, F.; De Vita, D.; Carafa, C.; Messore, A.; Di Santo, R.; Feroci, M.; Costi, R.; Chiarotto, I.; Bagetta, D.; et al. New deferiprone derivatives as multi-functional cholinesterase inhibitors: Design, synthesis and in vitro evaluation. Eur. J. Med. Chem. 2020, 198, 112350. [Google Scholar] [CrossRef]
- Geneen, L.J.; Dorée, C.; Estcourt, L.J. Interventions for improving adherence to iron chelation therapy in people with sickle cell disease or thalassaemia. Cochrane Database Syst. Rev. 2023, 3, CD012349. [Google Scholar]
- Marchand, F.; Moreau, C.; Kuchcinski, G.; Huin, V.; Defebvre, L.; Devos, D. Conservative Iron Chelation for Neuroferritinopathy. Mov. Disord. 2022, 37, 1948–1952. [Google Scholar] [CrossRef]
- Fisher, S.A.; Brunskill, S.J.; Doree, C.; Gooding, S.; Chowdhury, O.; Roberts, D.J. Desferrioxamine mesylate for managing transfusional iron overload in people with transfusion-dependent thalassaemia. Cochrane Database Syst Rev. 2013, CD004450. [Google Scholar] [CrossRef]
- Malcovati, L. Red blood cell transfusion therapy and iron chelation in patients with myelodysplastic syndromes. Clin. Lymphoma Myeloma 2009, 9 (Suppl. 3), S305–S311. [Google Scholar] [CrossRef]
- Peng, C.T.; Tsai, C.H.; Wu, K.H. Effects of chelation therapy on cardiac function improvement in thalassemia patients: Literature review and the Taiwanese experience. Hemoglobin 2008, 32, 49–62. [Google Scholar] [CrossRef]
- Anonymous. Deferasirox: For iron overload: Only a third-line option. Prescrire Int. 2007, 16, 196. [Google Scholar]
- Cario, H.; Janka-Schaub, G.; Janssen, G.; Jarisch, A.; Strauss, G.; Kohne, E. Recent developments in iron chelation therapy. Klin. Padiatr. 2007, 219, 158–165. [Google Scholar] [CrossRef] [PubMed]






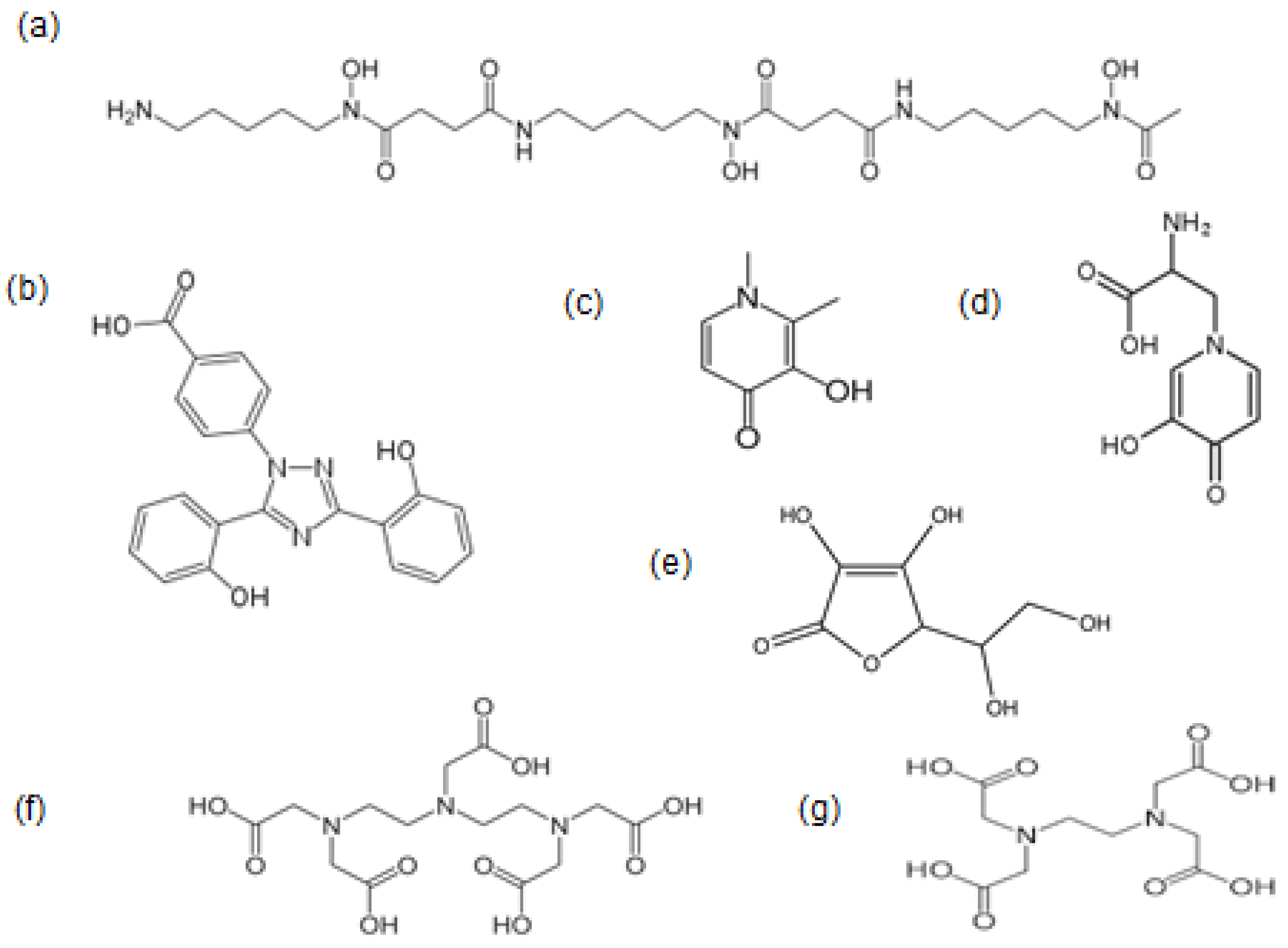{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chemical and physicochemical properties Physical state: white crystalline solid. Molecular weight: 139. Molecular weight of iron complex: 470. Charge of L1 and iron complex at pH 7.4: neutral. Partition coefficient (n-octanol/water) of L1: 0.19 and iron complex: 0.05 (both hydrophilic). Stability constant (Log β) of the tris L1 iron complex: 35. |
| Effects on the proteins of iron transport and storage Iron removal from diferric transferrin in iron-loaded patients: removal of about 40% of iron at L1 concentrations of greater than 0.15 mM. Iron donation to apo-transferrin by the L1 iron complex. Iron removal from and donation to lactoferrin similar to that observed in transferrin. Dose-dependent iron removal from ferritin and hemosiderin. |
| Clinical characteristics Efficacy in iron removal is related to dose. Recommended dose in transfusional iron overload: 75–100 mg/kg/day. Recommended dose in different categories of non-iron-loaded patients: minimum single dose 25 mg/kg/day and repeated doses up to a maximum 100 mg/kg/day. Decrease of iron absorption. Differential iron removal from various organs of iron-loaded patients: preferential iron removal of excess iron from the heart but also from the liver, spleen, and pancreas in iron-loaded patients. Iron redistribution in diseases of iron metabolism: deferiprone can cause iron redistribution from iron deposits and also through transferrin from the reticuloendothelial system to the erythron in the anaemia of chronic disease. Similar effect of excess iron redistribution is observed in patients with neurodegenerative diseases with excess iron in the brain treated with L1. Increased excretion of metals other than iron: increased zinc excretion in iron-loaded patients following long-term treatments. Increased aluminium excretion in aluminium-loaded renal dialysis patients. Deferiprone glucuronide metabolite: no iron binding and no increase in iron excretion. Combination chelation therapy: combination therapies of all chelating drugs are more effective in iron excretion than monotherapies. The International Committee on Chelation of L1 and DF combination protocol causes normalization of the iron stores in thalassemia patients. |
| Metabolism and pharmacokinetics Metabolite: the L1 glucuronide conjugate. T1/2 of absorption: 0.7–32 min. T max: mostly within 1 h on empty stomach. T1/2 elimination: 47–134 min at a 35–71 mg/kg dose. T1/2 elimination of the L1 iron complex: estimated within 47–134 min. T max of the L1 iron complex: within 1 h. T max of the metabolite L1-glucuronide: 1–3 h. Route of elimination of L1-glucuronide conjugate, L1, and its iron complex: urine. |
| The unique drug properties of deferiprone Simple, inexpensive, one-step synthesis and wide availability worldwide. White crystalline solid; stable at room temperature for more than 15 years. Orally effective and good compliance. Rapid absorption, appearance in blood, and wide body and organ distribution. Daily use in iron-loaded patients at high doses (75–100 mg/kg) for many years with no serious toxicity. Iron removal from all organs and especially the hearts of iron-loaded patients. Ability to cross the blood–brain barrier and remove excess iron from the brain and treat malignant, neurological, and microbial diseases affecting the brain. Iron removal from transferrin in iron-loaded patients and iron donation in non-iron-loaded patients. Potent antioxidant activity through inhibition of Fe and Cu catalytic production of free radicals. Inhibition of ferroptosis and cuproptosis involved in many diseases of free radical pathology. Use in metal intoxication diseases, including those related to Fe, Cu, Al, Zn, Ga, In, U, and Pu. Drug combination therapies with DF, DFRA, EDTA, DTPA, ascorbate, mimosine, and other chelators. |
| Clinical effects of deferiprone in transfusional iron-loaded thalassaemia patients Complete iron removal as monotherapy or combination therapy with DF from all iron storage organs. Maintenance of normal iron stores in ex-iron-loaded patients. Efficient excess iron removal from the heart and reduction of congestive cardiac failure. Improvements in the antioxidant status, including increases in glutathione levels and in cellular function. Improvement of LVEF and endothelial cell function. Decrease in the mortality rate of thalassaemia patients and transition of thalassaemia from a fatal to a chronic disease. |
| Clinical effects of deferiprone in non-iron-loaded patient categories Renal dialysis: removal of excess iron and aluminium. Rheumatoid arthritis: increase in haemoglobin and improvement of anaemia. Malaria: fast resolution of fever and coma and rapid parasitaemia clearance. HIV: antiretroviral action. Release of innate apoptotic defense of HIV-infected cells from viral blockade. Aceruloplasminemia: removal of excess cardiac iron and improvement of cardiac function. Parkinson’s disease: removal of excess iron from the brain and improvement in motor scores (30 mg/kg). Alzheimer’s disease: removal of excess iron from the brain. Friedreich’s ataxia: removal of excess iron from the brain. Reduction in neuropathy and ataxic gait. NBIA: removal of excess iron from the brain and slowing of disease progression. PKAN: removal of excess iron from the brain. Stability of the overall clinical neurological picture. Glomerulonephritis: significant reduction in urinary protein; no significant changes in serum creatinine. Diabetic nephropathy: persistent drop in mean albumin/creatinine ratio; 9-month stable renal function. Breast cancer: eradication of cancer stem cells through selective targeting of mitochondria. Prostate cancer: inhibition of prostate cancer proliferation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontoghiorghes, G.J. The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases. Pharmaceuticals 2023, 16, 1016. https://doi.org/10.3390/ph16071016
Kontoghiorghes GJ. The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases. Pharmaceuticals. 2023; 16(7):1016. https://doi.org/10.3390/ph16071016
Chicago/Turabian StyleKontoghiorghes, George J. 2023. "The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases" Pharmaceuticals 16, no. 7: 1016. https://doi.org/10.3390/ph16071016
APA StyleKontoghiorghes, G. J. (2023). The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases. Pharmaceuticals, 16(7), 1016. https://doi.org/10.3390/ph16071016