
COVID-19 Survivor Patients Carrying the Rs35705950 Risk Allele in MUC5B Have Higher Plasma Levels of Mucin 5B


 ,
,  ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of the Study Population
2.2. DNA Extraction and Quantification
2.3. Genotyping
2.4. Plasma Mucin 5B Measurement
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Genotype and Allele Association
3.3. Linkage Disequilibrium
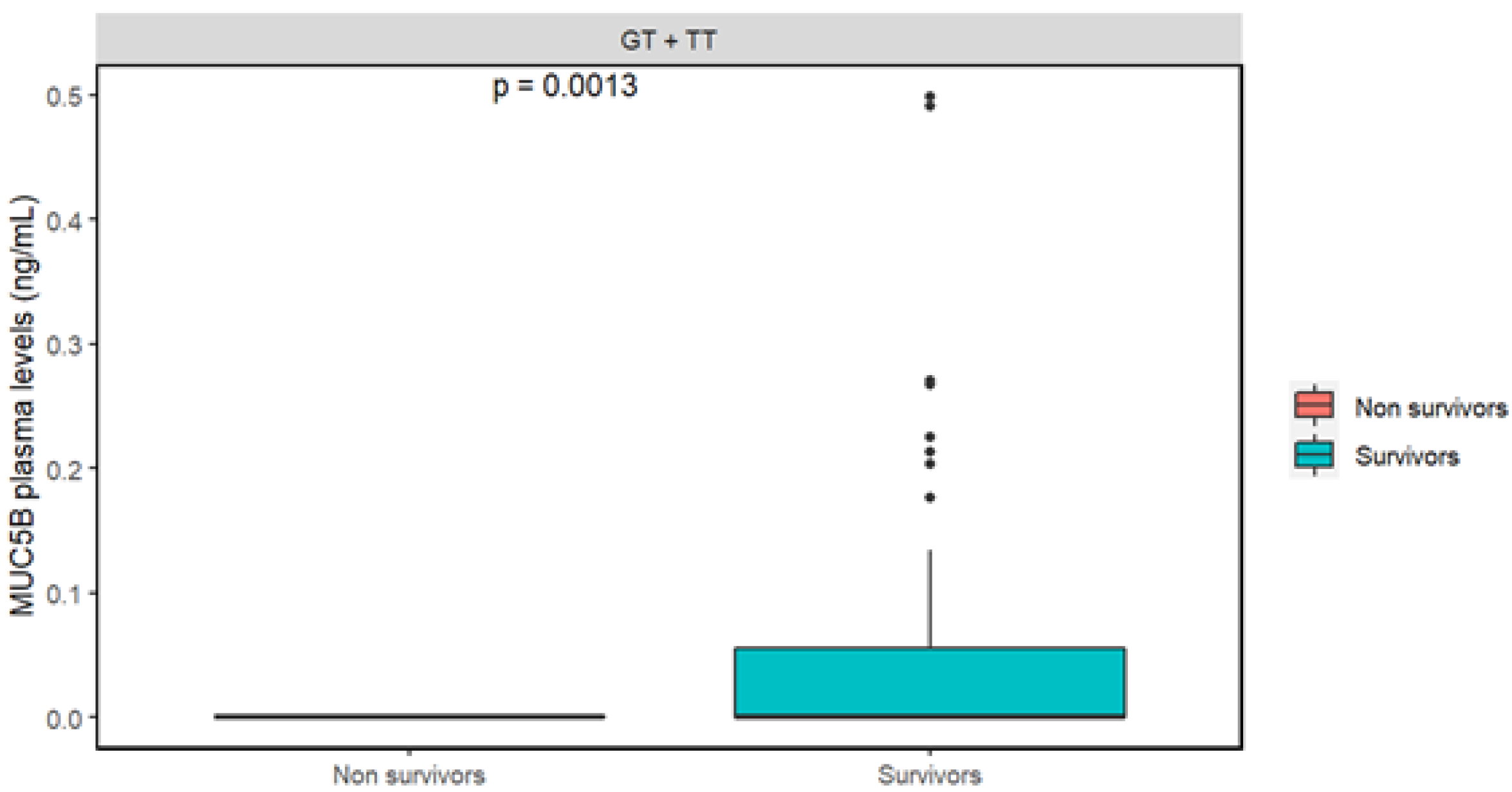
3.4. Evaluation of Mucin 5B Plasma Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Organización Panamericana de la Salud (OPS). Coronavirus. 2022. Available online: https://www.paho.org/es/temas/coronavirus (accessed on 17 May 2022).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- The Severe COVID-19 GWAS Group. Genomewide Association Study of Severe COVID-19 with Respiratory Failure. J. Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef]
- Asgari, S.; Pousaz, A.L. Human Genetic Variants Identified that Affect COVID Susceptibility and Severity. Nature. 2021, 600, 390–391. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rubio, G.; Cordoba-Lanus, E.; Cupertino, P.; Cartujano-Barrera, F.; Campos, A.M.; Falfan-Valencia, R. Role of genetic susceptibility in nicotine addiction and chronic obstructive pulmonary disease. Rev. Investig. Clin. 2019, 71, 36–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gally, F.; Sasse, S.K.; Kurche, J.S.; Gruca, M.A.; Cardwell, J.H.; Okamoto, T.; Chu, H.W.; Hou, X.; Poirion, O.B.; Buchanan, J.; et al. The MUC5B-associated variant rs35705950 resides within an enhancer subject to lineage- and disease-dependent epigenetic remodeling. JCI Insight 2021, 6, e144294. [Google Scholar] [CrossRef] [PubMed]
- Seixas, S.; Marques, P.I. Known mutations at the cause of Alpha-1 antitrypsin deficiency an updated overview of SERPINA1 Variation spectrum. Appl. Clin. Genet. 2021, 14, 173–194. [Google Scholar] [CrossRef]
- Casas-Rojo, J.M.; Antón-Santos, J.M.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clin. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Vaira, L.A.; Salzano, G.; Deiana, G.; De Riu, G. Anosmia and Ageusia: Common Findings in COVID-19 Patients. Laryngoscope 2020, 130, 1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guven, B.B.; Erturk, T.; Kompe, Ö.; Ersoy, A. Serious complications in COVID-19 ARDS cases: Pneumothorax, pneumomediastinum, subcutaneous emphysema and haemothorax. Epidemiol. Infect. 2021, 149, E137. [Google Scholar] [CrossRef] [PubMed]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2020, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Elhabyan, A.; Elyaacoub, S.; Sanad, E.; Abukhadra, A.; Elhabyan, A.; Dinu, V. The role of host genetics in susceptibility to severe viral infections in humans and insights into host genetics of severe COVID-19: A systematic review. Virus Res. 2020, 289, 198163. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Chapman, K.R.; Wong, A.; Liu, M. α1-Antitrypsin deficiency and the risk of COVID-19: An urgent call to action. Lancet Respir. Med. 2021, 9, 337–339. [Google Scholar] [CrossRef]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Choileáin, O.N.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the inflammatory response to severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef]
- Wettstein, L.; Weil, T.; Conzelmann, C.; Müller, J.A.; Groß, R.; Hirschenberger, M.; Seidel, A.; Klute, S.; Zech, F.; Prelli Bozzo, C.; et al. Alpha-1 antitrypsin inhibits TMPRSS2 protease activity and SARS-CoV-2 infection. Nat. Commun. 2021, 12, 1726. [Google Scholar] [CrossRef]
- de Loyola, M.B.; dos Reis, T.T.A.; Argañaraz, G.A.; Argañaraz, E.R. Alpha-1-antitrypsin: A possible host protective factor against COVID-19. Rev. Med. Virol. 2020, 31, e2157. [Google Scholar] [CrossRef]
- Fadista, J.; Kraven, L.M.; Karjalainen, J.; Andrews, S.J.; Geller, F.; Baillie, J.K.; Wain, L.V.; Jenkins, R.G.; Feenstra, B. Shared genetic etiology between idiopathic pulmonary fibrosis and COVID-19 severity. EBioMedicine 2021, 65, 103277. [Google Scholar] [CrossRef]
- van Moorsel, C.H.M.; van der Vis, J.J.; Duckworth, A.; Scotton, C.J.; Benschop, C.; Ellinghaus, D.; Ruven, H.J.T.; Quanjel, M.J.R.; Grutters, J.C. The MUC5B Promoter Polymorphism Associates with Severe COVID-19 in the European Population. Front. Med. 2021, 8, 668024. [Google Scholar] [CrossRef]
- Roy, M.G.; Livraghi-Butrico, A.; Fletcher, A.A.; McElwee, M.M.; Evans, S.E.; Boerner, R.M.; Alexander, S.N.; Bellinghausen, L.K.; Song, A.S.; Petrova, Y.M.; et al. Muc5b is required for airway defence. Nature 2014, 505, 412–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, W.; Cao, W.; Zhou, G.; Wang, L.; Sun, J.; Zhu, A.; Wang, Z.; Zhou, Y.; Liu, X.; Li, Y.; et al. Analysis of pathological changes in the epithelium in COVID-19 patient airways. ERJ Open Res. 2021, 7, 00690-2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Non-Survivors n = 460 | Survivors n = 798 | p |
|---|---|---|---|
| Age (years) | 63 (48–64) | 56 (48–64) | <0.001 |
| Male, n (%) | 331 (71.9) | 509 (63.8) | 0.003 |
| BMI (kg/m2) | 29 (26–33) | 30 (27–33) | 0.004 |
| Comorbidities % | |||
| Obesity | 41.7 | 47.2 | 0.068 |
| T2DM | 31.1 | 27.1 | 0.150 |
| CRD | 9.3 | 5.9 | 0.029 |
| IHC | 6.3 | 3.0 | 0.007 |
| SAH | 38.2 | 33.7 | 0.122 |
| Onset of symptoms (days) | 9 (7–14) | 9 (7–12) | 0.574 |
| Symptoms % | |||
| Fever | 66.4 | 73.3 | 0.012 |
| Cough | 68.2 | 67.4 | 0.836 |
| Dyspnea | 84.7 | 83.9 | 0.760 |
| Myalgia | 60.1 | 65.6 | 0.057 |
| Arthralgias | 58.9 | 62.3 | 0.251 |
| Headache | 42.7 | 45.9 | 0.295 |
| Rhinorrhea | 17.6 | 14.9 | 0.245 |
| Odynophagia | 22.4 | 26.1 | 0.570 |
| Diarrhea | 8.5 | 11.3 | 0.138 |
| Vomiting | 2.4 | 3.1 | 0.559 |
| Chest pain | 7.4 | 10.9 | 0.536 |
| Anosmia | 3.9 | 8.6 | 0.002 |
| Ageusia | 9.3 | 14.8 | 0.006 |
| Hospitalization (days) | 20 (13–30) | 19 (12–30) | 0.029 |
| mmHg PaO2/FiO2 | 128 (86–169) | 166 (114–212) | <0.001 |
| IMV, n (%) | 93.0 | 60.9 | <0.001 |
| Genotypes/ Alleles | Non-Survivors n = 458 (%) | Survivors n = 793 (%) | p-Value | OR | CI, 95% |
|---|---|---|---|---|---|
| rs17580 | |||||
| TT | 96.47 | 95.96 | 0.587 | 1 (Reference) | |
| TA | 3.53 | 3.91 | 0.89 | 0.48–1.65 | |
| AA | 0 | 0.13 | |||
| T | 98.23 | 97.92 | 0.690 | ||
| A | 1.77 | 2.08 | 0.84 | 0.46–1.54 | |
| rs28929474 | |||||
| CC | 99.74 | 98.99 | 0.550 | 1 (Reference) | |
| CT | 0.13 | 1.01 | 0.21 | 0.02–1.72 | |
| TT | 0.13 | 0 | |||
| C | 99.74 | 99.50 | 0.213 | ||
| T | 0.26 | 0.50 | 0.21 | 0.02–1.72 | |
| rs35705950 | |||||
| GG | 93.01 | 93.57 | 0.735 | 1 (Reference) | |
| GT | 6.77 | 6.18 | 1.10 | 0.69–1.75 | |
| TT | 0.22 | 0.25 | 0.87 | 0.07–9.63 | |
| G | 96.39 | 96.66 | 0.817 | ||
| T | 3.60 | 3.34 | 1.08 | 0.69–1.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Carmona, S.; Falfán-Valencia, R.; Verónica-Aguilar, A.; Buendía-Roldán, I.; Chávez-Galán, L.; Hernández-Zenteno, R.d.J.; Martínez-Morales, A.; Fricke-Galindo, I.; Alanis-Ponce, J.; Valencia-Pérez Rea, D.; et al. COVID-19 Survivor Patients Carrying the Rs35705950 Risk Allele in MUC5B Have Higher Plasma Levels of Mucin 5B. Curr. Issues Mol. Biol. 2022, 44, 3283-3290. https://doi.org/10.3390/cimb44080226
García-Carmona S, Falfán-Valencia R, Verónica-Aguilar A, Buendía-Roldán I, Chávez-Galán L, Hernández-Zenteno RdJ, Martínez-Morales A, Fricke-Galindo I, Alanis-Ponce J, Valencia-Pérez Rea D, et al. COVID-19 Survivor Patients Carrying the Rs35705950 Risk Allele in MUC5B Have Higher Plasma Levels of Mucin 5B. Current Issues in Molecular Biology. 2022; 44(8):3283-3290. https://doi.org/10.3390/cimb44080226
Chicago/Turabian StyleGarcía-Carmona, Salvador, Ramcés Falfán-Valencia, Abigail Verónica-Aguilar, Ivette Buendía-Roldán, Leslie Chávez-Galán, Rafael de Jesús Hernández-Zenteno, Alfonso Martínez-Morales, Ingrid Fricke-Galindo, Jesús Alanis-Ponce, Daniela Valencia-Pérez Rea, and et al. 2022. "COVID-19 Survivor Patients Carrying the Rs35705950 Risk Allele in MUC5B Have Higher Plasma Levels of Mucin 5B" Current Issues in Molecular Biology 44, no. 8: 3283-3290. https://doi.org/10.3390/cimb44080226
APA StyleGarcía-Carmona, S., Falfán-Valencia, R., Verónica-Aguilar, A., Buendía-Roldán, I., Chávez-Galán, L., Hernández-Zenteno, R. d. J., Martínez-Morales, A., Fricke-Galindo, I., Alanis-Ponce, J., Valencia-Pérez Rea, D., Gutiérrez-Pérez, I. A., Zaragoza-García, O., Nava-Quiroz, K. J., Camarena, A., Mejía, M., Guzmán-Guzmán, I. P., & Pérez-Rubio, G. (2022). COVID-19 Survivor Patients Carrying the Rs35705950 Risk Allele in MUC5B Have Higher Plasma Levels of Mucin 5B. Current Issues in Molecular Biology, 44(8), 3283-3290. https://doi.org/10.3390/cimb44080226