
Stroke-Associating Acute Limb Ischemia Due to the Rupture of a Hydatid Cyst

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Case Report
4. Discussion
4.1. Paraclinical Diagnostic Tools
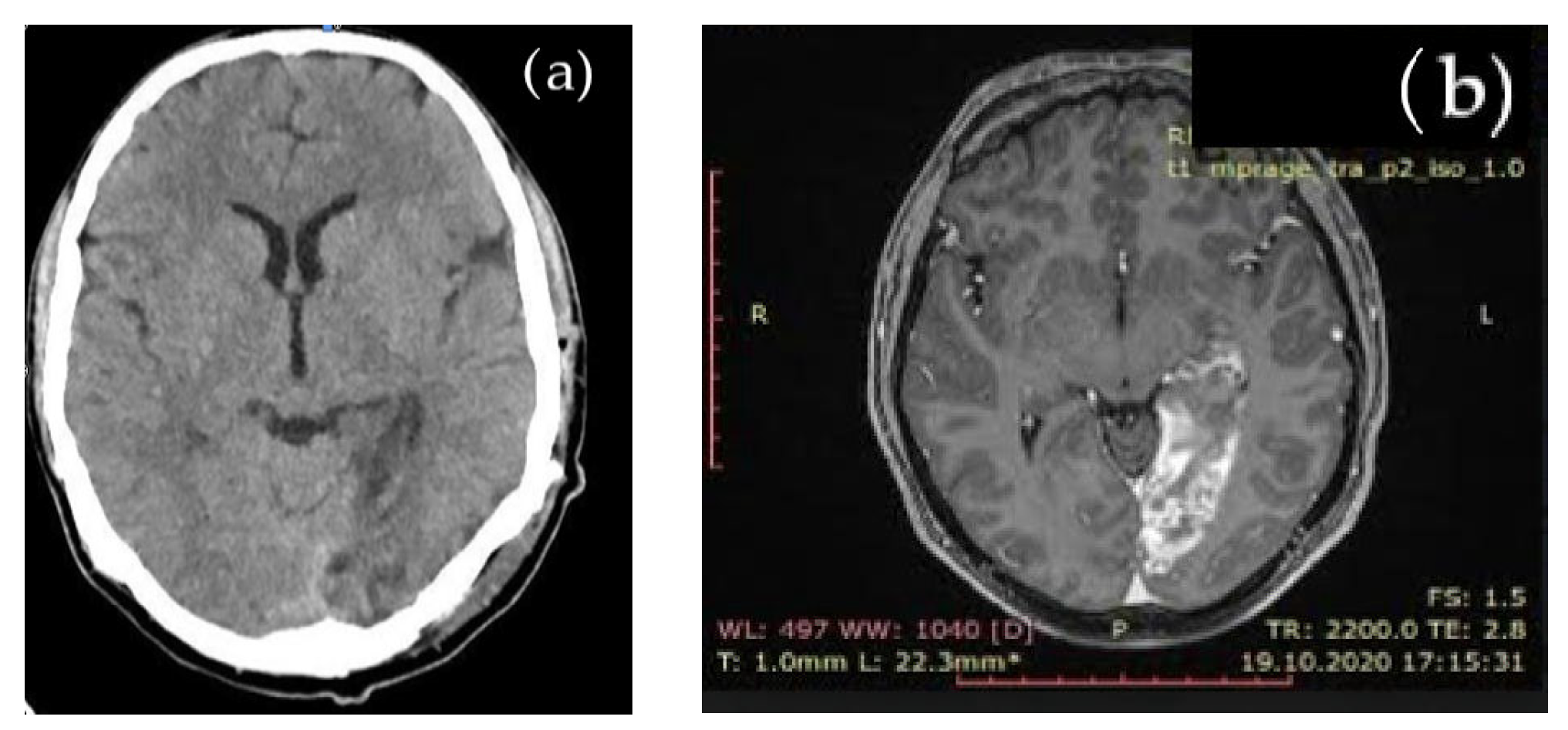
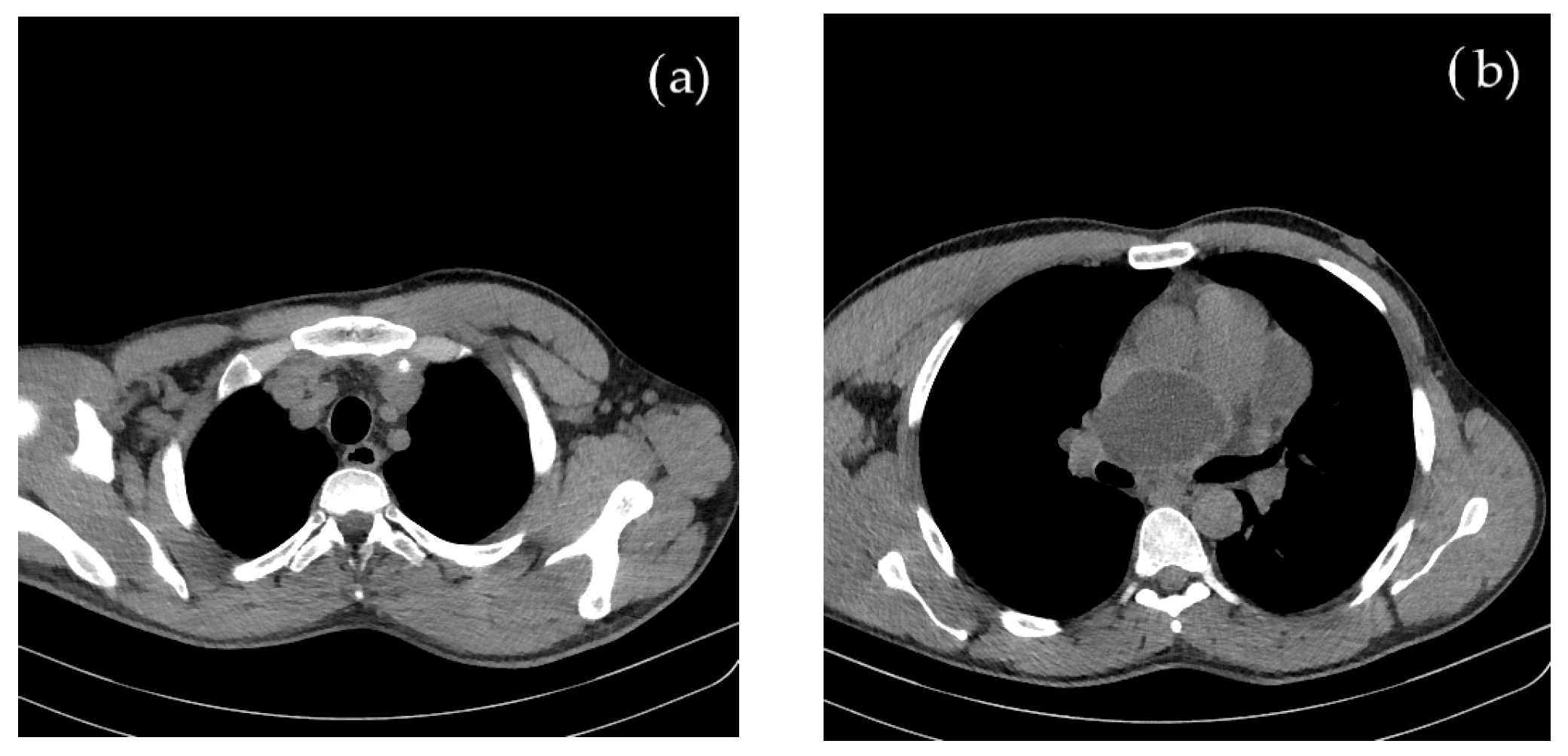
4.1.1. Imaging
4.1.2. Biomarkers and Molecular Biology Characterization
5. Conclusions
- -
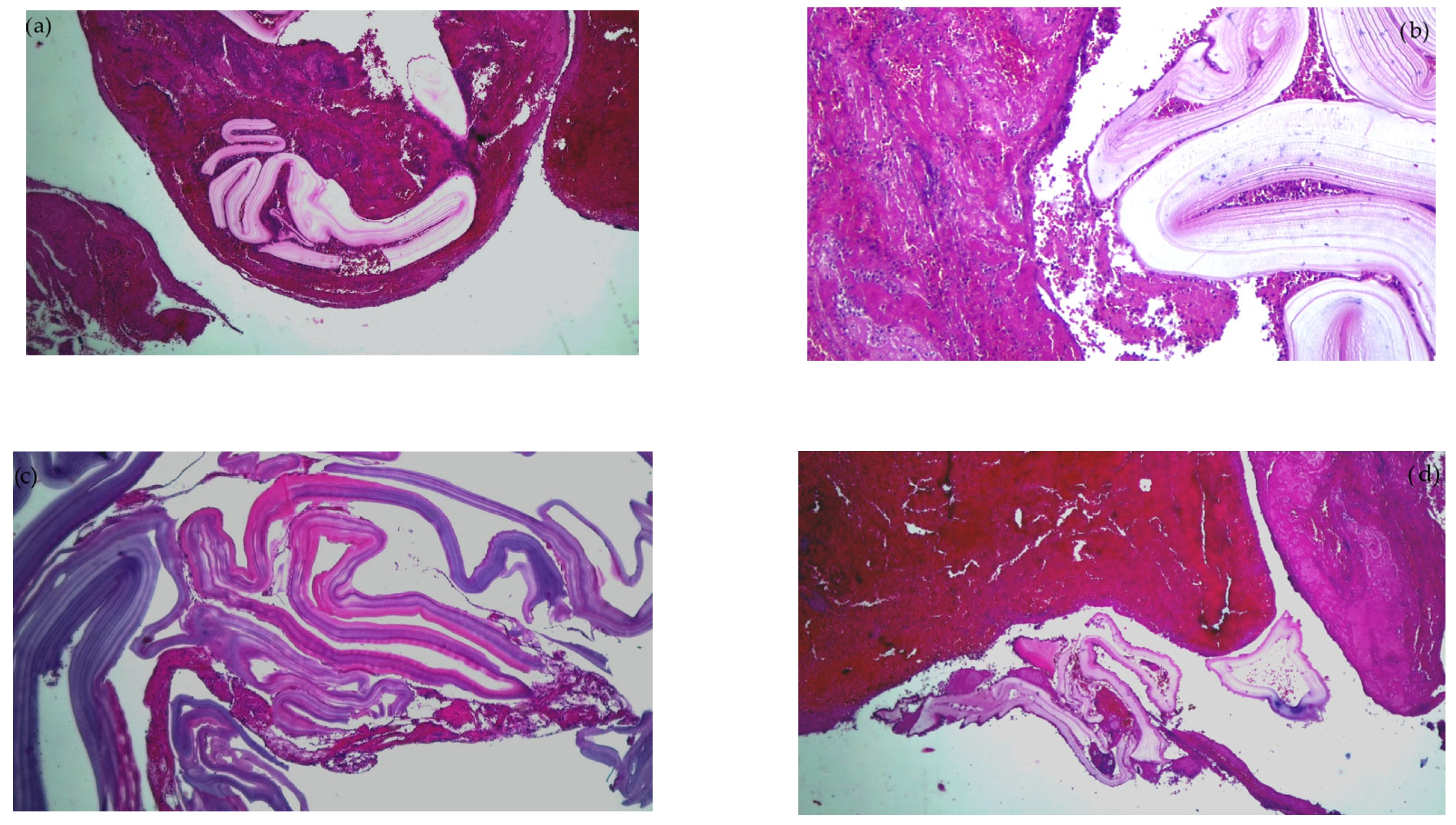
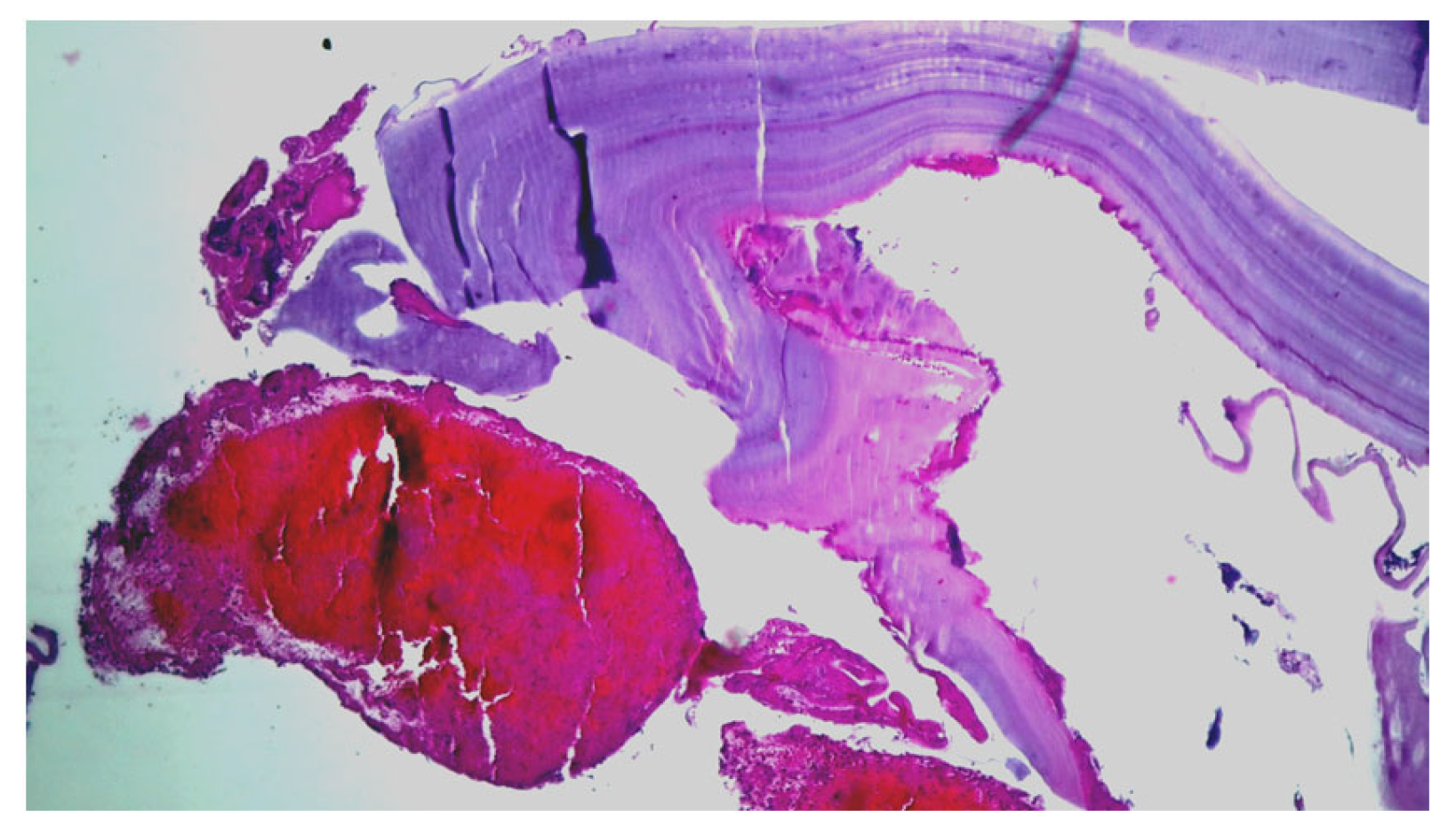
- A never-reported embolism in the right brachial artery with anhistous membrane, histopathologically was confirmed. We found no similar report in the available literature.
- -
- Concomitant cerebral embolism with an acute ischemic stroke, in a patient without other detectable cardiovascular risk factors, was recorded.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Firouzi, A.; Borj, M.N.P.; Ghavidel, A.A. Cardiac hydatid cyst: A rare presentation of echinococcal infection. J. Cardiovasc. Thorac. Res. 2019, 11, 75–77. [Google Scholar] [CrossRef]
- Kardaras, F.; Kardara, D.; Tselikos, D.; Tsoukas, A.; Exadactylos, N.; Anagnostopoulou, M.; Lolas, C.; Anthopoulos, L. Fifteen year surveillance of echinococcal heart disease from a referral hospital in Greece. Eur. Heart J. 1996, 17, 1265–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, M.; Pathania, R.; Jhobta, A.; Thakur, B.R.; Chopra, R. Cystic pulmonary hydatidosis. Lung India 2016, 33, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Madariaga, I.; de la Fuente, A.; Lezaun, R.; Imizcoz, M.A.; Carmona, J.R.; Urquia, M.; Arcos, E.D.L. Cardiac Echinococcosis and Systemic Embolism. Report of a Case. Thorac. Cardiovasc. Surg. 1984, 32, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Borrie, J.; Gemmell, M.; Manktelow, B.W. An experimental approach to evaluate the potential risk of hydatid disease from inhalation of echinococcus ova. Br. J. Surg. 1965, 52, 876–878. [Google Scholar] [CrossRef]
- Ramos, G.; Orduña, A.; García-Yuste, M. Hydatid Cyst of the Lung: Diagnosis and Treatment. World J. Surg. 2001, 25, 46–57. [Google Scholar] [CrossRef]
- Aletras, H.; Symbas, P.N. Hydatid Disease of the Lung. In General Thoracic Surgery, 5th ed.; Shields, T.W., LoCicero, J., Ponn, R.B., Eds.; Lippincot Williams and Wilkins: Philadelphia, PA, USA, 2000; pp. 1113–1122. [Google Scholar]
- Isitmangil, T.; Toker, A.; Sebit, S.; Erdik, O.; Tunc, H.; Gorur, R. A novel terminology and dissemination theory for a subgroup of intrathoracic extrapulmonary hydatid cysts. Med. Hypotheses 2003, 61, 68–71. [Google Scholar] [CrossRef]
- Uysalel, A.; Aral, A.; Atalay, S.; Akalin, H. Cardiac echinococcosis with multivisceral involvement. Pediatr. Cardiol. 1996, 17, 268–270. [Google Scholar] [CrossRef]
- Al-Hakkak, S.M.M.; Al-Faham, F.S.M.; Al-Awwady, A.N. Acute limb ischemia caused by ruptured cardiac hydatid cyst—A case report. Int. J. Surg. Case Rep. 2019, 55, 18–22. [Google Scholar] [CrossRef]
- Maffeis, G.R.; Petrucci, O.; Carandina, R.; Leme, C.A.; Truffa, M.; Vieira, R.; Schelini, F.; Metze, K.; Nogueira, E.A. Cardiac Echinococcosis. Circulation 2000, 101, 1352–1354. [Google Scholar] [CrossRef] [Green Version]
- Acartürk, E.; Özeren, A.; Koç, M.; Yaliniz, H.; Biçakci, S.; Demir, M. Left ventricular hydatid cyst presenting with acute ischemic stroke: Case report. J. Am. Soc. Echocardiogr. 2004, 17, 1009–1010. [Google Scholar] [CrossRef]
- Odev, K.; Acikgözoglu, S.; Gormüs, N.; Aribas, O.; Kiresi, D.; Solak, H. Pulmonary embolism due to cardiac hydatid disease: Imaging findings of unusual complication of hydatid cyst. Eur. Radiol. 2002, 12, 627–633. [Google Scholar] [CrossRef]
- Niarchos, C.; Kounis, G.N.; Frangides, C.R.; Koutsojannis, C.M.; Batsolaki, M.; Gouvelou-Deligianni, G.V.; Kounis, N.G. Large hydatic cyst of the left ventricle associated with syncopal attacks. Int. J. Cardiol. 2007, 118, e24–e26. [Google Scholar] [CrossRef]
- Kammoun, S.; Frikha, I.; Fourati, K.; Fendri, S.; Benyoussef, S.; Sahnoun, Y.; Daoud, M.; Dumesnil, J.G. Hydatid cyst of the heart located in the interventricular septum. Can. J. Cardiol. 2000, 16, 921–924. [Google Scholar]
- Ozturk, M.; Sigirci, A.; Dagli, A.F. A rare cause of embolism in the popliteal artery of an adolescent: Ruptured cardiac hydatid cyst. Anatol. J. Cardiol. 2015, 15, E20. [Google Scholar] [CrossRef]
- Turgut, M.; Benli, K.; Eryilmaz, M. Secondary multiple intracranial hydatid cysts caused by intracerebral embolism of cardiac echinococcosis: An exceptional case of hydatidosis. J. Neurosurg. 1997, 86, 714–718. [Google Scholar] [CrossRef]
- Singh, N.P.; Arora, S.K.; Gupta, A.; Anuradha, S.; Sridhara, G.; Agarwal, S.K.; Gulati, P. Stroke: A rare presentation of cardiac hydatidosis. Neurol. India 2003, 51, 120–121. [Google Scholar]
- Gautam, S.; Sharma, A. Intracranial Hydatid Cyst: A Report of Three Cases in North-West India. J. Pediatr. Neurosci. 2018, 13, 91–95. [Google Scholar]
- Gupta, S.; Desai, K.; Goel, A. Intracranial hydatid cyst: A report of five cases and review of literature. Neurol. India 1999, 47, 214–217. [Google Scholar]
- Mirijello, A.; Pepe, G.; Zampiello, P.; Criconia, G.M.; Mendola, A.; Manfrini, A. A Male Patient with Syncope, Anaphylaxis, and ST-Elevation: Hepatic and Cardiac Echinococcosis Presenting with Kounis Syndrome. J. Emerg. Med. 2016, 51, e73–e77. [Google Scholar] [CrossRef]
- Oliver, J.M.; Sotillo, J.F.; Domínguez, F.J.; de Sá, E.L.; Calvo, L.; Salvador, A.; Paniagua, J.M. Two-dimensional echocardiographic features of echinococcosis of the heart and great blood vessels. Clinical and surgical implications. Circulation 1988, 78, 327–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghadhoune, H.; Chaari, A.; Baccouche, N.; Chelly, H.; Bouaziz, M. Accident vasculaire cérébral ischémique: Une complication rare du kyste hydatique du foie. Ann. Fr. D’Anesth. Réanim. 2013, 32, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Janitschke, K. Parasitic Infections. In Clinic Laboratory Diagnostics—Use and Assessment of Clinical Laboratory Results, 1st ed.; Thomas, L., Ed.; TH-Books; VerlagsgesellschaftmbH: Frankfurt/Main, Germany, 1998; pp. 1293–1294. [Google Scholar]
- Birincioğlu, C.L.; Tarcan, O.; Bardakci, H.; Saritaş, A.; Taşdemir, O. Off-pump technique for the treatment of ventricular myocardial echinococcosis. Ann. Thorac. Surg. 2003, 75, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Sangwan, S.; Sachar, S. Uncommon locations and presentations of hydatid cyst. Ann. Med. Health Sci. Res. 2014, 4, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Di Bello, R.; Menéndez, H. Intracardiac Rupture of Hydatid Cysts of the Heart. A study based on three personal observations and 101 cases in the world literature. Circulation 1963, 27, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Özer, N.; Aytemir, K.; Kuru, G.; Atalar, E.; Özer, Y.; Övünç, K.; Aksöyek, S.; Gököz, A.; Gürsel, G.; Kes, S. Hydatid cyst of the heart as a rare cause of embolization: Report of 5 cases and review of published reports. J. Am. Soc. Echocardiogr. 2001, 14, 299–302. [Google Scholar] [CrossRef]
- Perez-Gomez, F.; Duran, H.; Tamames, S.; Perrote, J.L.; Blanes, A. Cardiac echinococcosis: Clinical picture and complications. Heart 1973, 35, 1326–1331. [Google Scholar] [CrossRef] [Green Version]
- Hèla, B.J.; Abir, B.; Majdi, G.; Aiman, D.; Iheb, S.; Nizar, E.; Sayda, M.; Imed, F. Interventricular septum hydatid cyst presenting with acute lower limb ischemia: A case report. Libyan J. Med. 2015, 10, 28634. [Google Scholar] [CrossRef]
- Yaliniz, H.; Tokcan, A.; Ulus, T.; Kisacikoglu, B.; Salih, O.K.; Topcuoglu, M.S.; Poyrazoglu, H.; Alhan, C. A Rare Presentation of Cardiac Hydatid Cyst: Stroke and Acute Aortic Occlusion. Heart Surg. Forum 2004, 7, E364–E366. [Google Scholar] [CrossRef] [Green Version]
- Arboix, A.; Bechich, S.; Oliveres, M.; Garcia-Eroles, L.; Massons, J.; Targa, C. Ischemic stroke of unusual cause: Clinical features, etiology and outcome. Eur. J. Neurol. 2001, 8, 133–139. [Google Scholar] [CrossRef]
- Rai, N.; Sarkar, U.N.; Bhattacharya, S.; Sengupta, G.; Das, D.; Dutta, S.; Sanki, P.; Mahapatra, S.S. Hydatid cyst of the heart: An uncommon lesion. Indian J. Thorac. Cardiovasc. Surg. 2009, 25, 211–213. [Google Scholar] [CrossRef]
- Unlü, Y.; Ceviz, M.; Karaoğlanoğlu, N.; Becit, N.; Koçak, H. Arterial embolism caused by a ruptured hydatid cyst in the heart: Report of a case. Surg. Today 2002, 32, 989–991. [Google Scholar] [CrossRef]
- Pedrosa, I.; Saiz, A.; Arrazola, J.; Ferreirós, J.; Pedrosa, C.S. Hydatid Disease: Radiologic and Pathologic Features and Complications. RadioGraphics 2000, 20, 795–817. [Google Scholar] [CrossRef]
- Grozavu, C.; Ilias, M.; Pantile, D. Multivisceral echinococcosis: Concept, diagnosis, management. Chirurgia 2014, 109, 758–768. [Google Scholar]
- Ceyran, H.; Tasdemir, K.; Tezcaner, T.; Asgun, F.; Karahan, O.I.; Emirogullari, O.N.; Andac, H. A rare cause of peripheral arterial embolism: Ruptured cardiac hydatid cyst. Vasa 2002, 31, 129–131. [Google Scholar] [CrossRef]
- Hussain, M.A.; Alatawneh, R.; Bhatti, M.O.A.; Randhawa, M.A.; Anwar, A.; Maheshwary, N. Cardiac Hydatid Cyst Rupture and Embolization Causing Lower Limb Ischemia and Multiple Infarcts: A Case Report. Am. J. Cardiovasc. Thorac. Surg. 2017, 2, 1–5. [Google Scholar] [CrossRef]
- Kelle, S.; Köhler, U.; Thouet, T.; Fleck, E.; Nagel, E. Cardiac involvement of Echinococcus granulosus evaluated by multi-contrast CMR imaging. Int. J. Cardiol. 2009, 131, e59–e60. [Google Scholar] [CrossRef]
- Thameur, M.H.; Abdelmoula, M.S.; Chenik, M.S.; Bey, M.M.; Ziadi, M.M.; Mestiri, M.T.; Mechmeche, M.R.; Chaouch, M.H. Cardiopericardial Hydatid Cysts. World J. Surg. 2001, 25, 58–67. [Google Scholar] [CrossRef]
- Padayachy, L.; Ozek, M. Hydatid disease of the brain and spine. Child’s Nerv. Syst. 2022, 39, 751–758. [Google Scholar] [CrossRef]
- Wen, H.; Vuitton, L.; Tuxun, T.; Li, J.; Vuitton, D.A.; Zhang, W.; McManus, D.P. Echinococcosis: Advances in the 21st Century. Clin. Microbiol. Rev. 2019, 32, e00075-18. [Google Scholar] [CrossRef] [Green Version]
- Nabarro, L.E.; Amin, Z.; Chiodini, P.L. Current Management of Cystic Echinococcosis: A Survey of Specialist Practice. Clin. Infect. Dis. 2014, 60, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özek, M. Complications of Central Nervous System Hydatid Disease. Pediatr. Neurosurg. 1994, 20, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Alok, R.; Mahmoud, J. Successful Surgical Treatment of a Brain Stem Hydatid Cyst in a Child. Case Rep. Surg. 2020, 2020, 5645812. [Google Scholar] [CrossRef] [PubMed]
- Padayachy, L.C.; Dattatraya, M. Hydatid disease (Echinococcus) of the central nervous system. Child’s Nerv. Syst. 2018, 34, 1967–1971. [Google Scholar] [CrossRef] [PubMed]
- Altinörs, N.; Bavbek, M.; Caner, H.H.; Erdoğan, B. Central nervous system hydatidosis in Turkey: A cooperative study and literature survey analysis of 458 cases. J. Neurosurg. 2000, 93, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, E.; Kern, P.; Vuitton, D.A.; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef]
- Sioutis, S.; Reppas, L.; Bekos, A.; Soulioti, E.; Saranteas, T.; Koulalis, D.; Sapkas, G.; Mavrogenis, A.F. Echinococcosis of the spine. EFORT Open Rev. 2021, 6, 288–296. [Google Scholar] [CrossRef]
- De Rosa, F.; Teggi, A. Treatment of Echinococcus granulosu shydatid disease with Albendazole. Ann. Trop. Med. Parasitol. 1990, 84, 467–472. [Google Scholar] [CrossRef]
- Turki, O.; Bahloul, M.; Chtara, K.; Regaieg, K.; Haddar, S.; Bouaziz, M. Kyste hydatique du foie compliqué d’un accident vasculaire cérébral ischémique: À propos d’un cas. Pan Afr. Med. J. 2015, 22, 355. [Google Scholar] [CrossRef]
- Hammami, A.; Hellara, O.; Mnari, W.; Loussaief, C.; Bedioui, F.; Safer, L.; Golli, M.; Chakroun, M.; Saffar, H. Unusual presentation of severely disseminated and rapidly progressive hydatic cyst: Malignant hydatidosis. World J. Hepatol. 2015, 7, 633–637. [Google Scholar] [CrossRef]
- Santucciu, C.; Bonelli, P.; Peruzzu, A.; Fancellu, A.; Marras, V.; Carta, A.; Mastrandrea, S.; Bagella, G.; Piseddu, T.; Profili, S.; et al. Cystic Echinococcosis: Clinical, Immunological, and Biomolecular Evaluation of Patients from Sardinia (Italy). Pathogens 2020, 9, 907. [Google Scholar] [CrossRef]
- Zhang, W.; Li, J.; McManus, D. Concepts in Immunology and Diagnosis of Hydatid Disease. Clin. Microbiol. Rev. 2003, 16, 18–36. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.E.; Salim, B.; Grobusch, M.P.; Aradaib, I.E. First molecular characterization of Echinococcus granulosus (sensu stricto) genotype 1 among cattle in Sudan. BMC Vet. Res. 2018, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- De, A.K.; Sujatha, T.; Sunder, J.; Bala, P.; Perumal, P.; Bhattacharya, D.; Chakurkar, E.B. Eg95: A Vaccine against Cystic Echinococcosis. Vaccine Development. Available online: https://www.intechopen.com/chapters/79843 (accessed on 6 April 2022).
- Yucel, N.; Kayaalp, C.; Liceli, A.; Baysal, T.; Yilmaz, M. Blindness following Rupture of Hepatic Hydatid Cyst: A Case Report. Adv. Med. Sci. 2009, 54, 299–301. [Google Scholar] [CrossRef] [Green Version]
- Bajdechi, M.; Manolache, D.; Tudor, A.; Orghidan, M.; Gurghean, A. Cardiac hydatid cysts in a young man: A case report and a literature review. Exp. Ther. Med. 2022, 24, 550. [Google Scholar] [CrossRef]
- Rossetti, E.; Boto, A.; Cambaceres, C.G.; Ruvinsky, S.; Sagray, E.; Centeno, M.; Marti, J.L. Acute arterial embolism as the clinical presentation of a disseminated hydatidosis: Case report. Arch. Argent. Pediatr. 2018, 116, e616–e620. [Google Scholar] [CrossRef]
- Derbel, B.; Ziadi, J.; Besbes, T.; Dougaz, W.; Mleyhi, S.; Zairi, I.; Denguir, R. Intracardiac echinococcosis cyst mimicking a septal cardiac tumor with neurological symptoms. Int. J. Infect. Dis. 2019, 88, 152–153. [Google Scholar] [CrossRef] [Green Version]
- Stiru, O.; Geana, R.C.; Antohi, L.; David, L.; Goicea, M.; Paunescu, A.; Chioncel, O.; Iliescu, V.A. Incidentally Detected Cardiac and Hepatic Hydatid Cyst after Sudden Onset Facial Paralysis: A Case Report. Arch. Clin. Med. Case Rep. 2019, 3, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Zghal, F.M.; Boudiche, S.; Zongo, T.; Rekik, B.; Ouali, S.; Mourali, M.S. An unusual cause of stroke and sudden death: Intracavitary left ventricular echinococcosis. Int. J. Infect. Dis. 2020, 90, 26–27. [Google Scholar] [CrossRef] [Green Version]
- Bussani, R.; Castrichini, M.; Restivo, L.; Fabris, E.; Porcari, A.; Ferro, F.; Pivetta, A.; Korcova, R.; Cappelletto, C.; Manca, P.; et al. Cardiac Tumors: Diagnosis, Prognosis, and Treatment. Curr. Cardiol. Rep. 2020, 22, 169. [Google Scholar] [CrossRef]
- Hadi, M.A.E.; Najari, F.; Soleimani, L. Sudden Death due to Hydatid Cyst Emboli; a Case Report. Emergency (Tehran) 2018, 6, e20. [Google Scholar]
- Casulli, A.; Massolo, A.; Saarma, U.; Umhang, G.; Santolamazza, F.; Santoro, A. Species and genotypes belonging to Echinococcus granulosus sensu lato complex causing human cystic echinococcosis in Europe (2000–2021): A systematic review. Parasites Vectors 2022, 15, 109. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2022 Systematic Review | E. granulosus s.s. | E. canadensis | E. ortleppi | ||||
|---|---|---|---|---|---|---|---|
| Genotype G1 (%) | Genotype G3 (%) | Ungenotyped (%) | Genotype G7 (%) | Genotype G10 (%) | Genotype G6/G10 (%) | Genotype G5 (%) | |
| CE cases circulating Europe | 40.3% | 10.8% | 48.9% | 98.3% | 0.85% | 0.85% | 1.5% |
| CE cases identified Romania | 97.4% | - | 2.6% | - | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lungu, M.; Oprea, V.D.; Zaharia, A.L.; Stan, B.; Rebegea, L.; Mocanu, D.I.; Elkan, E.M.; Niculet, E.; Croitoru, A. Stroke-Associating Acute Limb Ischemia Due to the Rupture of a Hydatid Cyst. Curr. Issues Mol. Biol. 2023, 45, 2597-2608. https://doi.org/10.3390/cimb45030170
Lungu M, Oprea VD, Zaharia AL, Stan B, Rebegea L, Mocanu DI, Elkan EM, Niculet E, Croitoru A. Stroke-Associating Acute Limb Ischemia Due to the Rupture of a Hydatid Cyst. Current Issues in Molecular Biology. 2023; 45(3):2597-2608. https://doi.org/10.3390/cimb45030170
Chicago/Turabian StyleLungu, Mihaela, Violeta Diana Oprea, Andrei Lucian Zaharia, Bianca Stan, Laura Rebegea, Dan Iulian Mocanu, Eva Maria Elkan, Elena Niculet, and Ana Croitoru. 2023. "Stroke-Associating Acute Limb Ischemia Due to the Rupture of a Hydatid Cyst" Current Issues in Molecular Biology 45, no. 3: 2597-2608. https://doi.org/10.3390/cimb45030170
APA StyleLungu, M., Oprea, V. D., Zaharia, A. L., Stan, B., Rebegea, L., Mocanu, D. I., Elkan, E. M., Niculet, E., & Croitoru, A. (2023). Stroke-Associating Acute Limb Ischemia Due to the Rupture of a Hydatid Cyst. Current Issues in Molecular Biology, 45(3), 2597-2608. https://doi.org/10.3390/cimb45030170