Maternal Influenza and Offspring Neurodevelopment




{kind=link}
Abstract
:1. Background
- 1.
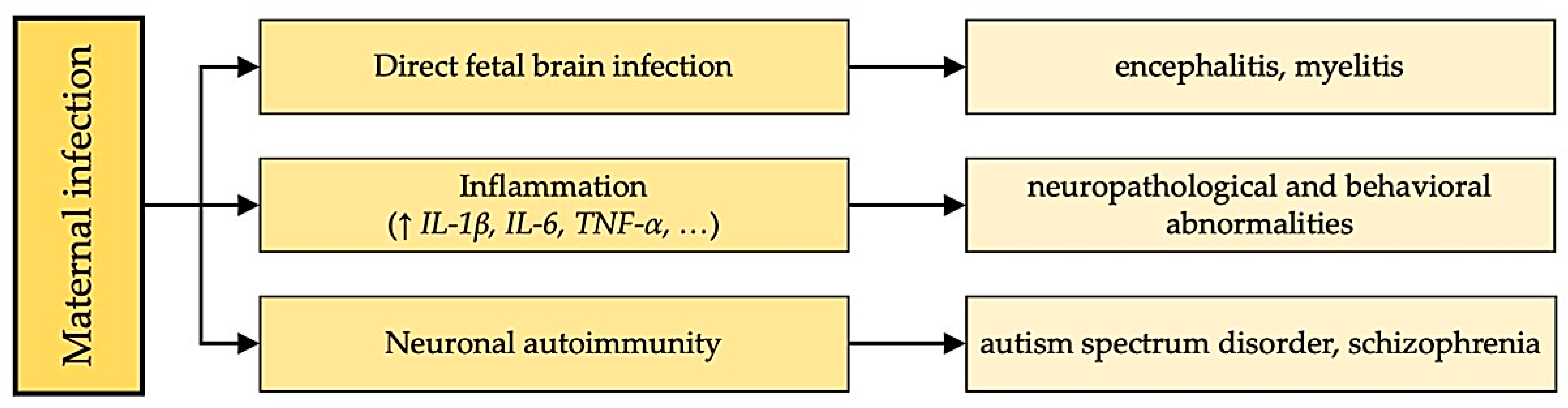
- The live virus can directly enter the fetal brain and infect it. Interestingly, various researchers have obtained conflicting results. One group of researchers confirmed the presence of the virus in the fetal brain when the influenza virus was administered intranasally to pregnant mice [41]. Another study showed simultaneously that viral RNAs are not detectable in fetal mouse brains from infected mothers [11].
- 2.
- Chemical mediators of infection may mediate changes in brain development. During maternal infection, levels of chemical mediators of inflammation, primarily cytokines, interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α, increase in the maternal blood and placenta. Such cytokines can influence fetal brain development by directly affecting the fetal brain, interfering with placental function, or exerting effects through the mother. The fever-like state itself, because of the increased release of maternal cytokines, can affect the development of the fetal nervous system. Studies examining the risks associated with increased maternal body temperature have shown that even short-term exposure of pregnant rodents to high temperatures can lead to abnormalities in the central nervous system [42].
- 3.
- Autoimmune conditions: It has been suggested that immunoglobulins against infectious agents may cross-react with and damage fetal brain structures. There is no evidence yet that such an autoimmune mechanism occurs in schizophrenia, but the possibility of implementing such a mechanism is indirectly confirmed in some studies. For example, there is some experimental support for the idea that antibodies against group A β-hemolytic streptococci may cross-react with the basal ganglia, leading to cases of Tourette’s syndrome or obsessive-compulsive disorder following streptococcal throat infection in patients [43].
2. Fetal Infection
3. The Role of Cytokines
4. Autoimmune Conditions
5. Features of the Course of Neurotropic Influenza in Animal Models
6. Other Factors
7. Prospects
Author Contributions
Funding
Conflicts of Interest
References
- Raj, R.S.; Bonney, E.A.; Phillippe, M. Influenza, Immune System, and Pregnancy. Reprod. Sci. 2014, 21, 1434–1451. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, V.; Kristensen, N.R.; Monz, B.U.; Clinch, B.; Kenwright, A.; Sørensen, H.T. Oseltamivir in Pregnancy and Birth Outcomes. BMC Infect. Dis. 2018, 18, 519. [Google Scholar] [CrossRef] [PubMed]
- Newsome, K.; Alverson, C.J.; Williams, J.; McIntyre, A.F.; Fine, A.D.; Wasserman, C.; Lofy, K.H.; Acosta, M.; Louie, J.K.; Jones-Vessey, K.; et al. Outcomes of Infants Born to Women with Influenza A(H1N1)Pdm09. Birth Defects Res. 2019, 111, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Liong, S.; Miles, M.A.; Mohsenipour, M.; Liong, F.; Hill-Yardin, E.L.; Selemidis, S. Influenza A Virus Infection during Pregnancy Causes Immunological Changes in Gut-Associated Lymphoid Tissues of Offspring Mice. Am. J. Physiol.-Gastrointest. Liver Physiol. 2023, 325, G230–G238. [Google Scholar] [CrossRef] [PubMed]
- Silasi, M.; Cardenas, I.; Kwon, J.; Racicot, K.; Aldo, P.; Mor, G. Viral Infections During Pregnancy. Am. J. Reprod. Immunol. 2015, 73, 199–213. [Google Scholar] [CrossRef]
- Van Riel, D.; Mittrücker, H.-W.; Engels, G.; Klingel, K.; Markert, U.R.; Gabriel, G. Influenza Pathogenicity during Pregnancy in Women and Animal Models. Semin. Immunopathol. 2016, 38, 719–726. [Google Scholar] [CrossRef]
- Zou, S. Potential Impact of Pandemic Influenza on Blood Safety and Availability. Transfus. Med. Rev. 2006, 20, 181–189. [Google Scholar] [CrossRef]
- Irving, W.L.; James, D.K.; Stephenson, T.; Laing, P.; Jameson, C.; Oxford, J.S.; Chakraverty, P.; Brown, D.W.G.; Boon, A.C.M.; Zambon, M.C. Influenza Virus Infection in the Second and Third Trimesters of Pregnancy: A Clinical and Seroepidemiological Study. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 1282–1289. [Google Scholar] [CrossRef]
- Fatemi, S.H.; Earle, J.; Kanodia, R.; Kist, D.; Emamian, E.S.; Patterson, P.H.; Shi, L.; Sidwell, R. Prenatal Viral Infection Leads to Pyramidal Cell Atrophy and Macrocephaly in Adulthood: Implications for Genesis of Autism and Schizophrenia. Cell. Mol. Neurobiol. 2002, 22, 25–33. [Google Scholar] [CrossRef]
- Shi, L.; Fatemi, S.H.; Sidwell, R.W.; Patterson, P.H. Maternal Influenza Infection Causes Marked Behavioral and Pharmacological Changes in the Offspring. J. Neurosci. 2003, 23, 297–302. [Google Scholar] [CrossRef]
- Shi, L.; Tu, N.; Patterson, P.H. Maternal Influenza Infection Is Likely to Alter Fetal Brain Development Indirectly: The Virus Is Not Detected in the Fetus. Int. J. Dev. Neurosci. 2005, 23, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Fung, S.G.; Fakhraei, R.; Condran, G.; Regan, A.K.; Dimanlig-Cruz, S.; Ricci, C.; Foo, D.; Sarna, M.; Török, E.; Fell, D.B. Neuropsychiatric Outcomes in Offspring after Fetal Exposure to Maternal Influenza Infection during Pregnancy: A Systematic Review. Reprod. Toxicol. 2022, 113, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Mon, M.A.; Guillen-Aguinaga, S.; Pereira-Sanchez, V.; Onambele, L.; Al-Rahamneh, M.J.; Brugos-Larumbe, A.; Guillen-Grima, F.; Ortuño, F. Being Born in Winter–Spring and at Around the Time of an Influenza Pandemic Are Risk Factors for the Development of Schizophrenia: The Apna Study in Navarre, Spain. J. Clin. Med. 2021, 10, 2859. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.; Agerbo, E.; Bennedsen, B.; Eaton, W.W.; Mortensen, P.B. Obstetric Conditions and Risk of First Admission with Schizophrenia: A Danish National Register Based Study. Schizophr. Res. 2007, 97, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Dreier, J.W.; Berg-Beckhoff, G.; Andersen, A.M.N.; Susser, E.; Nordentoft, M.; Strandberg-Larsen, K. Fever and Infections during Pregnancy and Psychosis-like Experiences in the Offspring at Age 11. A Prospective Study within the Danish National Birth Cohort. Psychol. Med. 2018, 48, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Zammit, S.; Odd, D.; Horwood, J.; Thompson, A.; Thomas, K.; Menezes, P.; Gunnell, D.; Hollis, C.; Wolke, D.; Lewis, G.; et al. Investigating Whether Adverse Prenatal and Perinatal Events Are Associated with Non-Clinical Psychotic Symptoms at Age 12 Years in the ALSPAC Birth Cohort. Psychol. Med. 2009, 39, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Morgan, V.; Castle, D.; Page, A.; Fazio, S.; Gurrin, L.; Burton, P.; Montgomery, P.; Jablensky, A. Influenza Epidemics and Incidence of Schizophrenia, Affective Disorders and Mental Retardation in Western Australia: No Evidence of a Major Effect. Schizophr. Res. 1997, 26, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Pineda, D.A.; Palacio, L.G.; Puerta, I.C.; Merchán, V.; Arango, C.P.; Galvis, A.Y.; Gómez, M.; Aguirre, D.C.; Lopera, F.; Arcos-Burgos, M. Environmental Influences That Affect Attention Deficit/Hyperactivity Disorder. Eur. Child. Adolesc. Psychiatry 2007, 16, 337–346. [Google Scholar] [CrossRef]
- Canetta, S.E.; Bao, Y.; Co, M.D.T.; Ennis, F.A.; Cruz, J.; Terajima, M.; Shen, L.; Kellendonk, C.; Schaefer, C.A.; Brown, A.S. Serological Documentation of Maternal Influenza Exposure and Bipolar Disorder in Adult Offspring. Am. J. Psychiatry 2014, 171, 557–563. [Google Scholar] [CrossRef]
- Ellman, L.M.; Yolken, R.H.; Buka, S.L.; Torrey, E.F.; Cannon, T.D. Cognitive Functioning Prior to the Onset of Psychosis: The Role of Fetal Exposure to Serologically Determined Influenza Infection. Biol. Psychiatry 2009, 65, 1040–1047. [Google Scholar] [CrossRef]
- Al-Haddad, B.J.S.; Oler, E.; Armistead, B.; Elsayed, N.A.; Weinberger, D.R.; Bernier, R.; Burd, I.; Kapur, R.; Jacobsson, B.; Wang, C.; et al. The Fetal Origins of Mental Illness. Am. J. Obs. Gynecol. 2019, 221, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Ursini, G.; Punzi, G.; Chen, Q.; Marenco, S.; Robinson, J.F.; Porcelli, A.; Hamilton, E.G.; Mitjans, M.; Maddalena, G.; Begemann, M.; et al. Convergence of Placenta Biology and Genetic Risk for Schizophrenia. Nat. Med. 2018, 24, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.C.; Tanskanen, A.; Huttunen, M.; Whittaker, J.C.; Cannon, M. Evidence for an Interaction Between Familial Liability and Prenatal Exposure to Infection in the Causation of Schizophrenia. Am. J. Psychiatry 2009, 166, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Blomström, Å.; Karlsson, H.; Gardner, R.; Jörgensen, L.; Magnusson, C.; Dalman, C. Associations Between Maternal Infection During Pregnancy, Childhood Infections and the Risk of Subsequent Psychotic Disorder—A Swedish Cohort Study of Nearly 2 Million Individuals. Schizophr. Bull. 2015, 42, sbv112. [Google Scholar] [CrossRef] [PubMed]
- Abazyan, B.; Nomura, J.; Kannan, G.; Ishizuka, K.; Tamashiro, K.L.; Nucifora, F.; Pogorelov, V.; Ladenheim, B.; Yang, C.; Krasnova, I.N.; et al. Prenatal Interaction of Mutant DISC1 and Immune Activation Produces Adult Psychopathology. Biol. Psychiatry 2010, 68, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Lipina, T.V.; Zai, C.; Hlousek, D.; Roder, J.C.; Wong, A.H.C. Maternal Immune Activation during Gestation Interacts with Disc1 Point Mutation to Exacerbate Schizophrenia-Related Behaviors in Mice. J. Neurosci. 2013, 33, 7654–7666. [Google Scholar] [CrossRef] [PubMed]
- Mazina, V.; Gerdts, J.; Trinh, S.; Ankenman, K.; Ward, T.; Dennis, M.Y.; Girirajan, S.; Eichler, E.E.; Bernier, R. Epigenetics of Autism-Related Impairment. J. Dev. Behav. Pediatr. 2015, 36, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, C.N.; Tsimis, M.; Burd, I. Infections and Brain Development. Obs. Gynecol. Surv. 2015, 70, 644–655. [Google Scholar] [CrossRef]
- Guma, E.; Bordignon, P.d.C.; Devenyi, G.A.; Gallino, D.; Anastassiadis, C.; Cvetkovska, V.; Barry, A.D.; Snook, E.; Germann, J.; Greenwood, C.M.T.; et al. Early or Late Gestational Exposure to Maternal Immune Activation Alters Neurodevelopmental Trajectories in Mice: An Integrated Neuroimaging, Behavioral, and Transcriptional Study. Biol. Psychiatry 2021, 90, 328–341. [Google Scholar] [CrossRef]
- Janoutová, J.; Janácková, P.; Serý, O.; Zeman, T.; Ambroz, P.; Kovalová, M.; Varechová, K.; Hosák, L.; Jirík, V.; Janout, V. Epidemiology and Risk Factors of Schizophrenia. Neuro Endocrinol. Lett. 2016, 37, 1–8. [Google Scholar]
- Bitanihirwe, B.K.; Peleg-Raibstein, D.; Mouttet, F.; Feldon, J.; Meyer, U. Late Prenatal Immune Activation in Mice Leads to Behavioral and Neurochemical Abnormalities Relevant to the Negative Symptoms of Schizophrenia. Neuropsychopharmacology 2010, 35, 2462–2478. [Google Scholar] [CrossRef] [PubMed]
- Knuesel, I.; Chicha, L.; Britschgi, M.; Schobel, S.A.; Bodmer, M.; Hellings, J.A.; Toovey, S.; Prinssen, E.P. Maternal Immune Activation and Abnormal Brain Development across CNS Disorders. Nat. Rev. Neurol. 2014, 10, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, K.; Hashimoto, K.; Kishimoto, T.; Shimizu, E.; Ishikura, H.; Iyo, M. Immune Activation During Pregnancy in Mice Leads to Dopaminergic Hyperfunction and Cognitive Impairment in the Offspring: A Neurodevelopmental Animal Model of Schizophrenia. Biol. Psychiatry 2006, 59, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Reisinger, S.; Khan, D.; Kong, E.; Berger, A.; Pollak, A.; Pollak, D.D. The Poly(I:C)-Induced Maternal Immune Activation Model in Preclinical Neuropsychiatric Drug Discovery. Pharmacol. Ther. 2015, 149, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Vuillermot, S.; Joodmardi, E.; Perlmann, T.; Ove Ögren, S.; Feldon, J.; Meyer, U. Prenatal Immune Activation Interacts with Genetic Nurr1 Deficiency in the Development of Attentional Impairments. J. Neurosci. 2012, 32, 436–451. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, L.; Rehavi, M.; Nachman, R.; Weiner, I. Immune Activation During Pregnancy in Rats Leads to a PostPubertal Emergence of Disrupted Latent Inhibition, Dopaminergic Hyperfunction, and Altered Limbic Morphology in the Offspring: A Novel Neurodevelopmental Model of Schizophrenia. Neuropsychopharmacology 2003, 28, 1778–1789. [Google Scholar] [CrossRef] [PubMed]
- Boksa, P. Maternal Infection during Pregnancy and Schizophrenia. J. Psychiatry Neurosci. 2008, 33, 183–185. [Google Scholar]
- Brucato, M.; Ladd-Acosta, C.; Li, M.; Caruso, D.; Hong, X.; Kaczaniuk, J.; Stuart, E.A.; Fallin, M.D.; Wang, X. Prenatal Exposure to Fever Is Associated with Autism Spectrum Disorder in the Boston Birth Cohort. Autism Res. 2017, 10, 1878–1890. [Google Scholar] [CrossRef]
- Hornig, M.; Bresnahan, M.A.; Che, X.; Schultz, A.F.; Ukaigwe, J.E.; Eddy, M.L.; Hirtz, D.; Gunnes, N.; Lie, K.K.; Magnus, P.; et al. Prenatal Fever and Autism Risk. Mol. Psychiatry 2018, 23, 759–766. [Google Scholar] [CrossRef]
- Gustavson, K.; Ask, H.; Ystrom, E.; Stoltenberg, C.; Lipkin, W.I.; Surén, P.; Håberg, S.E.; Magnus, P.; Knudsen, G.P.; Eilertsen, E.; et al. Maternal Fever during Pregnancy and Offspring Attention Deficit Hyperactivity Disorder. Sci. Rep. 2019, 9, 9519. [Google Scholar] [CrossRef]
- Aronsson, F.; Lannebo, C.; Paucar, M.; Brask, J.; Kristensson, K.; Karlsson, H. Persistence of Viral RNA in the Brain of Offspring to Mice Infected with Influenza A/WSN/33 Virus during Pregnancy. J. Neurovirol. 2002, 8, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Khan, V.R.; Brown, I.R. The Effect of Hyperthermia on the Induction of Cell Death in Brain, Testis, and Thymus of the Adult and Developing Rat. Cell Stress. Chaperones 2002, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Korf, J.; Anderson, G.M.; Hoekstra, P.J.; Limburg, P.C.; Kallenberg, C.G.M.; Minderaa, R.B. Neurobiology and Neuroimmunology of Tourette’s Syndrome: An Update. Cell. Mol. Life Sci. 2004, 61, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Kępińska, A.P.; Iyegbe, C.O.; Vernon, A.C.; Yolken, R.; Murray, R.M.; Pollak, T.A. Schizophrenia and Influenza at the Centenary of the 1918-1919 Spanish Influenza Pandemic: Mechanisms of Psychosis Risk. Front. Psychiatry 2020, 11, 510689. [Google Scholar] [CrossRef] [PubMed]
- Grossman, J.D. Infections Affecting the Placenta. In the Pathology of the Human Placenta; Benirschke, K., Driscoll, S.G., Eds.; Aspen Publishers: Boston, MA, USA, 1987; pp. 131–154. [Google Scholar]
- Yawn, D.H.; Pyeatte, J.C.; Joseph, J.M.; Eichler, S.L.; Garcia-Bunuel, R. Transplacental Transfer of Influenza Virus. JAMA 1971, 216, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Jewett, J.F. Influenza Pneumonia at Term. N. Engl. J. Med. 1974, 291, 256–257. [Google Scholar] [CrossRef] [PubMed]
- McGregor, J.A.; Burns, J.C.; Levin, M.J.; Burlington, B.; Meiklejohn, G. Transplacental Passage of Influenza A/Bangkok (H3N2) Mimicking Amniotic Fluid Infection Syndrome. Am. J. Obs. Gynecol. 1984, 149, 856–859. [Google Scholar] [CrossRef]
- Gu, J.; Xie, Z.; Gao, Z.; Liu, J.; Korteweg, C.; Ye, J.; Lau, L.T.; Lu, J.; Gao, Z.; Zhang, B.; et al. H5N1 Infection of the Respiratory Tract and beyond: A Molecular Pathology Study. Lancet 2007, 370, 1137–1145. [Google Scholar] [CrossRef]
- Mel’nikova, V.F.; Tsinzerling, V.A.; Aksenov, O.A.; Tsinzerling, A.V. [Chronic Course of Influenza with Extrapulmonary Involvement]. Arkh Patol. 1994, 56, 33–38. [Google Scholar]
- Mel’nikova, V.F.; Tsinzerling, A.V.; Aksenov, O.A.; Vydumkina, S.P.; Kalinina, N.A. [Involvement of the Afterbirth in Influenza]. Arkh Patol. 1987, 49, 19–25. [Google Scholar]
- Rosztóczy, I.; Sweet, C.; Toms, G.L.; Smith, H. Replication of Influenza Virus in Organ Cultures of Human and Simian Urogenital Tissues and Human Foetal Tissues. Br. J. Exp. Pathol. 1975, 56, 322–328. [Google Scholar] [PubMed]
- Khakpour, M.; Saidi, A.; Naficy, K. Proved Viraemia in Asian Influenza (Hong Kong Variant) during Incubation Period. BMJ 1969, 4, 208–209. [Google Scholar] [CrossRef] [PubMed]
- Naficy, K. Human Influenza Infection with Proved Viremia. N. Engl. J. Med. 1963, 269, 964–966. [Google Scholar] [CrossRef] [PubMed]
- Uchide, N.; Ohyama, K.; Bessho, T.; Toyoda, H. Induction of Pro-Inflammatory Cytokine Gene Expression and Apoptosis in Human Chorion Cells of Fetal Membranes by Influenza Virus Infection: Possible Implications for Maintenance and Interruption of Pregnancy during Infection. Med. Sci. Monit. 2005, 11, RA7–RA16. [Google Scholar] [PubMed]
- Uchide, N.; Ohyama, K.; Bessho, T.; Yuan, B.; Yamakawa, T. Apoptosis in Cultured Human Fetal Membrane Cells Infected with Influenza Virus. Biol. Pharm. Bull. 2002, 25, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Collie, M.H.; Sweet, C.; Cavanagh, D.; Smith, H. Association of Foetal Wastage with Influenza Infection during Ferret Pregnancy. Br. J. Exp. Pathol. 1978, 59, 190–195. [Google Scholar] [PubMed]
- Sweet, C.; Collie, M.H.; Toms, G.L.; Smith, H. The Pregnant Guinea-Pig as a Model for Studying Influenza Virus Infection in Utero: Infection of Foetal Tissues in Organ Culture and in Vivo. Br. J. Exp. Pathol. 1977, 58, 133–139. [Google Scholar]
- Kuiken, T.; Taubenberger, J.K. Pathology of Human Influenza Revisited. Vaccine 2008, 26, D59–D66. [Google Scholar] [CrossRef]
- Kwit, K.; Pomorska-Mól, M.; Markowska-Daniel, I. The Influence of Experimental Infection of Gilts with Swine H1N2 Influenza A Virus during the Second Month of Gestation on the Course of Pregnancy, Reproduction Parameters and Clinical Status. BMC Vet. Res. 2014, 10, 123. [Google Scholar] [CrossRef]
- Kwit, K.; Pomorska-Mól, M.; Markowska-Daniel, I. Pregnancy Outcome and Clinical Status of Gilts Following Experimental Infection by H1N2, H3N2 and H1N1pdm09 Influenza A Viruses during the Last Month of Gestation. Arch. Virol. 2015, 160, 2415–2425. [Google Scholar] [CrossRef]
- Wallace, G.D.; Elm, J.L. Transplacental Transmission and Neonatal Infection with Swine Influenza Virus (Hsw1N1) in Swine. Am. J. Vet. Res. 1979, 40, 1169–1172. [Google Scholar] [PubMed]
- Shuid, A.N.; Jayusman, P.A.; Shuid, N.; Ismail, J.; Kamal Nor, N.; Mohamed, I.N. Association between Viral Infections and Risk of Autistic Disorder: An Overview. Int. J. Environ. Res. Public. Health 2021, 18, 2817. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, M.D.; Graham, A.M.; Feczko, E.; Miranda-Dominguez, O.; Rasmussen, J.M.; Nardos, R.; Entringer, S.; Wadhwa, P.D.; Buss, C.; Fair, D.A. Maternal IL-6 during Pregnancy Can Be Estimated from Newborn Brain Connectivity and Predicts Future Working Memory in Offspring. Nat. Neurosci. 2018, 21, 765–772. [Google Scholar] [CrossRef]
- Estes, M.L.; McAllister, A.K. Maternal Immune Activation: Implications for Neuropsychiatric Disorders. Science 2016, 353, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.B.; Yim, Y.S.; Wong, H.; Kim, S.; Kim, H.; Kim, S.V.; Hoeffer, C.A.; Littman, D.R.; Huh, J.R. The Maternal Interleukin-17a Pathway in Mice Promotes Autism-like Phenotypes in Offspring. Science 2016, 351, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Estes, M.L.; McAllister, A.K. Immune Mediators in the Brain and Peripheral Tissues in Autism Spectrum Disorder. Nat. Rev. Neurosci. 2015, 16, 469–486. [Google Scholar] [CrossRef] [PubMed]
- Uchide, N.; Ohyama, K.; Yuan, B.; Sano, T.; Bessho, T.; Yamakawa, T. Differential MRNA Expression of Inflammatory Cytokines in Cultured Human Fetal Membrane Cells Responding to Influenza Virus Infection. Biol. Pharm. Bull. 2002, 25, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, A.H.; Kerr, J.F.R.; Currie, A.R. Cell Death: The Significance of Apoptosis. In International Review of Cytology; Academic Press: Cambridge, MA, USA, 1980; Volume 68, pp. 251–306. [Google Scholar]
- Uchide, N. Antiviral Function of Pyrrolidine Dithiocarbamate against Influenza Virus: The Inhibition of Viral Gene Replication and Transcription. J. Antimicrob. Chemother. 2003, 52, 8–10. [Google Scholar] [CrossRef]
- Uchide, N.; Ohyama, K.; Bessho, T.; Yuan, B.; Yamakawa, T. Effect of Antioxidants on Apoptosis Induced by Influenza Virus Infection: Inhibition of Viral Gene Replication and Transcription with Pyrrolidine Dithiocarbamate. Antivir. Res. 2002, 56, 207–217. [Google Scholar] [CrossRef]
- Uchide, N.; Suzuki, A.; Ohyama, K.; Bessho, T.; Toyoda, H. Secretion of Bioactive Interleukin-6 and Tumor Necrosis Factor-α Proteins from Primary Cultured Human Fetal Membrane Chorion Cells Infected with Influenza Virus. Placenta 2006, 27, 678–690. [Google Scholar] [CrossRef]
- Lappas, M.; Permezel, M.; Georgiou, H.M.; Rice, G.E. Regulation of Proinflammatory Cytokines in Human Gestational Tissues by Peroxisome Proliferator-Activated Receptor-γ: Effect of 15-Deoxy-Δ12,14-PGJ2 and Troglitazone. J. Clin. Endocrinol. Metab. 2002, 87, 4667–4672. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.H.F. The Effects of a Cytokine Suppressive Anti-Inflammatory Drug on the Output of Prostaglandin E2 and Interleukin-1beta from Human Fetal Membranes. Mol. Hum. Reprod. 2002, 8, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Lappas, M.; Permezel, M.; Georgiou, H.M.; Rice, G.E. Nuclear Factor Kappa B Regulation of Proinflammatory Cytokines in Human Gestational Tissues In Vitro1. Biol. Reprod. 2002, 67, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.P.; Klein, S.L. Pregnancy and Pregnancy-Associated Hormones Alter Immune Responses and Disease Pathogenesis. Horm. Behav. 2012, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Szekeres-Bartho, J.; Polgar, B. PIBF: The Double Edged Sword. Pregnancy and Tumor. Am. J. Reprod. Immunol. 2010, 64, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Szekeres-Bartho, J.; Wegmann, T.G. A Progesterone-Dependent Immunomodulatory Protein Alters the Th1Th2 Balance. J. Reprod. Immunol. 1996, 31, 81–95. [Google Scholar] [CrossRef]
- Szekeres-Bartho, J.; Faust, Z.; Varga, P.; Szereday, L.; Kelemen, K. The Immunological Pregnancy Protective Effect of Progesterone Is Manifested via Controlling Cytokine Production. Am. J. Reprod. Immunol. 1996, 35, 348–351. [Google Scholar] [CrossRef]
- Krishnan, L.; Guilbert, L.J.; Russell, A.S.; Wegmann, T.G.; Mosmann, T.R.; Belosevic, M. Pregnancy Impairs Resistance of C57BL/6 Mice to Leishmania Major Infection and Causes Decreased Antigen-Specific IFN-Gamma Response and Increased Production of T Helper 2 Cytokines. J. Immunol. 1996, 156, 644–652. [Google Scholar] [CrossRef]
- Veenstra van Nieuwenhoven, A.L.; Bouman, A.; Moes, H.; Heineman, M.-J.; de Leij, L.F.M.H.; Santema, J.; Faas, M.M. Cytokine Production in Natural Killer Cells and Lymphocytes in Pregnant Women Compared with Women in the Follicular Phase of the Ovarian Cycle. Fertil. Steril. 2002, 77, 1032–1037. [Google Scholar] [CrossRef]
- Sacks, G.P.; Clover, L.M.; Bainbridge, D.R.J.; Redman, C.W.G.; Sargent, I.L. Flow Cytometric Measurement of Intracellular Th1 and Th2 Cytokine Production by Human Villous and Extravillous Cytotrophoblast. Placenta 2001, 22, 550–559. [Google Scholar] [CrossRef]
- Østensen, M. Sex Hormones and Pregnancy in Rheumatoid Arthritis and Systemic Lupus Erythematosus. Ann. N. Y. Acad. Sci. 1999, 876, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Marzi, M.; Vigano, A.; Trabattoni, D.; Villa, M.L.; Salvaggio, A.; Clerici, E.; Clerici, M. Characterization of Type 1 and Type 2 Cytokine Production Profile in Physiologic and Pathologic Human Pregnancy. Clin. Exp. Immunol. 2003, 106, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Mosmann, T.R.; Guilbert, L.; Tuntipopipat, S.; Wegmann, T.G. Synthesis of T Helper 2-Type Cytokines at the Maternal-Fetal Interface. J. Immunol. 1993, 151, 4562–4573. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.P.; Lorenzo, M.E.; Jian, W.; Klein, S.L. Elevated 17β-Estradiol Protects Females from Influenza A Virus Pathogenesis by Suppressing Inflammatory Responses. PLoS Pathog. 2011, 7, e1002149. [Google Scholar] [CrossRef] [PubMed]
- Pazos, M.A.; Kraus, T.A.; Muñoz-Fontela, C.; Moran, T.M. Estrogen Mediates Innate and Adaptive Immune Alterations to Influenza Infection in Pregnant Mice. PLoS ONE 2012, 7, e40502. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, M.M.; Mitzelfelt, J.D.; Yu, L.; Yue, Q.; Duke, B.J.; Harrell, C.S.; Neigh, G.N.; Eaton, D.C. Estradiol Activates Epithelial Sodium Channels in Rat Alveolar Cells through the G Protein-Coupled Estrogen Receptor. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2013, 305, L878–L889. [Google Scholar] [CrossRef]
- Wright, P.; Murray, R.M. Schizophrenia: Prenatal Influenza and Autoimmunity. Ann. Med. 1993, 25, 497–502. [Google Scholar] [CrossRef]
- Brimberg, L.; Mader, S.; Jeganathan, V.; Berlin, R.; Coleman, T.R.; Gregersen, P.K.; Huerta, P.T.; Volpe, B.T.; Diamond, B. Caspr2-Reactive Antibody Cloned from a Mother of an ASD Child Mediates an ASD-like Phenotype in Mice. Mol. Psychiatry 2016, 21, 1663–1671. [Google Scholar] [CrossRef]
- Coutinho, E.; Menassa, D.A.; Jacobson, L.; West, S.J.; Domingos, J.; Moloney, T.C.; Lang, B.; Harrison, P.J.; Bennett, D.L.H.; Bannerman, D.; et al. Persistent Microglial Activation and Synaptic Loss with Behavioral Abnormalities in Mouse Offspring Exposed to CASPR2-Antibodies in Utero. Acta Neuropathol. 2017, 134, 567–583. [Google Scholar] [CrossRef]
- Jones, K.L.; Pride, M.C.; Edmiston, E.; Yang, M.; Silverman, J.L.; Crawley, J.N.; Van de Water, J. Autism-Specific Maternal Autoantibodies Produce Behavioral Abnormalities in an Endogenous Antigen-Driven Mouse Model of Autism. Mol. Psychiatry 2020, 25, 2994–3009. [Google Scholar] [CrossRef]
- Jurek, B.; Chayka, M.; Kreye, J.; Lang, K.; Kraus, L.; Fidzinski, P.; Kornau, H.; Dao, L.; Wenke, N.K.; Long, M.; et al. Human Gestational N-methyl-d-aspartate Receptor Autoantibodies Impair Neonatal Murine Brain Function. Ann. Neurol. 2019, 86, 656–670. [Google Scholar] [CrossRef] [PubMed]
- Becerra-Culqui, T.A.; Getahun, D.; Chiu, V.; Sy, L.S.; Tseng, H.F. Prenatal Influenza Vaccination or Influenza Infection and Autism Spectrum Disorder in Offspring. Clin. Infect. Dis. 2022, 75, 1140–1148. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, S.H.; Folsom, T.D.; Liesch, S.B.; Kneeland, R.E.; Karkhane Yousefi, M.; Thuras, P.D. The Effects of Prenatal H1N1 Infection at E16 on FMRP, Glutamate, GABA, and Reelin Signaling Systems in Developing Murine Cerebellum. J. Neurosci. Res. 2017, 95, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Beraki, S. Influenza A Virus Infection and NMDA Receptor Function: A Behavioral and Molecular Study of Relevance for Schizophrenia; Karolinska Institutet: Stockholm, Sweden, 2008. [Google Scholar]
- Fatemi, S.H.; Emamian, E.S.; Kist, D.; Sidwell, R.W.; Nakajima, K.; Akhter, P.; Shier, A.; Sheikh, S.; Bailey, K. Defective Corticogenesis and Reduction in Reelin Immunoreactivity in Cortex and Hippocampus of Prenatally Infected Neonatal Mice. Mol. Psychiatry 1999, 4, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Oseghale, O.; Vlahos, R.; O’Leary, J.J.; Brooks, R.D.; Brooks, D.A.; Liong, S.; Selemidis, S. Influenza Virus Infection during Pregnancy as a Trigger of Acute and Chronic Complications. Viruses 2022, 14, 2729. [Google Scholar] [CrossRef]
- Elgueta, D.; Murgas, P.; Riquelme, E.; Yang, G.; Cancino, G.I. Consequences of Viral Infection and Cytokine Production During Pregnancy on Brain Development in Offspring. Front. Immunol. 2022, 13, 816619. [Google Scholar] [CrossRef]
- Antonson, A.M.; Kenney, A.D.; Chen, H.J.; Corps, K.N.; Yount, J.S.; Gur, T.L. Moderately Pathogenic Maternal Influenza A Virus Infection Disrupts Placental Integrity but Spares the Fetal Brain. Brain Behav. Immun. 2021, 96, 28–39. [Google Scholar] [CrossRef]
- Hill, R.A. Defining the Absolute Risk of Maternal Infections on Offspring Neurodevelopmental Outcomes: How to Ensure Your Model Is Not Lost in Translation. Brain Behav. Immun. 2021, 97, 6–7. [Google Scholar] [CrossRef]
- San Martín-González, N.; Castro-Quintas, Á.; Marques-Feixa, L.; Ayesa-Arriola, R.; López, M.; Fañanás, L. Maternal Respiratory Viral Infections during Pregnancy and Offspring’s Neurodevelopmental Outcomes: A Systematic Review. Neurosci. Biobehav. Rev. 2023, 149, 105178. [Google Scholar] [CrossRef]
- Juno, J.; Fowke, K.R.; Keynan, Y. Immunogenetic Factors Associated with Severe Respiratory Illness Caused by Zoonotic H1N1 and H5N1 Influenza Viruses. Clin. Dev. Immunol. 2012, 2012, 797180. [Google Scholar] [CrossRef]
- Marques, T.R.; Ashok, A.H.; Pillinger, T.; Veronese, M.; Turkheimer, F.E.; Dazzan, P.; Sommer, I.E.C.; Howes, O.D. Neuroinflammation in Schizophrenia: Meta-Analysis of in Vivo Microglial Imaging Studies. Psychol. Med. 2019, 49, 2186–2196. [Google Scholar] [CrossRef] [PubMed]
- Holmes, S.E.; Hinz, R.; Drake, R.J.; Gregory, C.J.; Conen, S.; Matthews, J.C.; Anton-Rodriguez, J.M.; Gerhard, A.; Talbot, P.S. In Vivo Imaging of Brain Microglial Activity in Antipsychotic-Free and Medicated Schizophrenia: A [11C](R)-PK11195 Positron Emission Tomography Study. Mol. Psychiatry 2016, 21, 1672–1679. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egorova, M.; Egorov, V.; Zabrodskaya, Y. Maternal Influenza and Offspring Neurodevelopment. Curr. Issues Mol. Biol. 2024, 46, 355-366. https://doi.org/10.3390/cimb46010023
Egorova M, Egorov V, Zabrodskaya Y. Maternal Influenza and Offspring Neurodevelopment. Current Issues in Molecular Biology. 2024; 46(1):355-366. https://doi.org/10.3390/cimb46010023
Chicago/Turabian StyleEgorova, Marya, Vladimir Egorov, and Yana Zabrodskaya. 2024. "Maternal Influenza and Offspring Neurodevelopment" Current Issues in Molecular Biology 46, no. 1: 355-366. https://doi.org/10.3390/cimb46010023
APA StyleEgorova, M., Egorov, V., & Zabrodskaya, Y. (2024). Maternal Influenza and Offspring Neurodevelopment. Current Issues in Molecular Biology, 46(1), 355-366. https://doi.org/10.3390/cimb46010023