The comparison of knee osteoarthritis treatment with single-dose bone marrow-derived mononuclear cells vs. hyaluronic acid injections

Abstract
:1. Introduction
2. Materials and methods
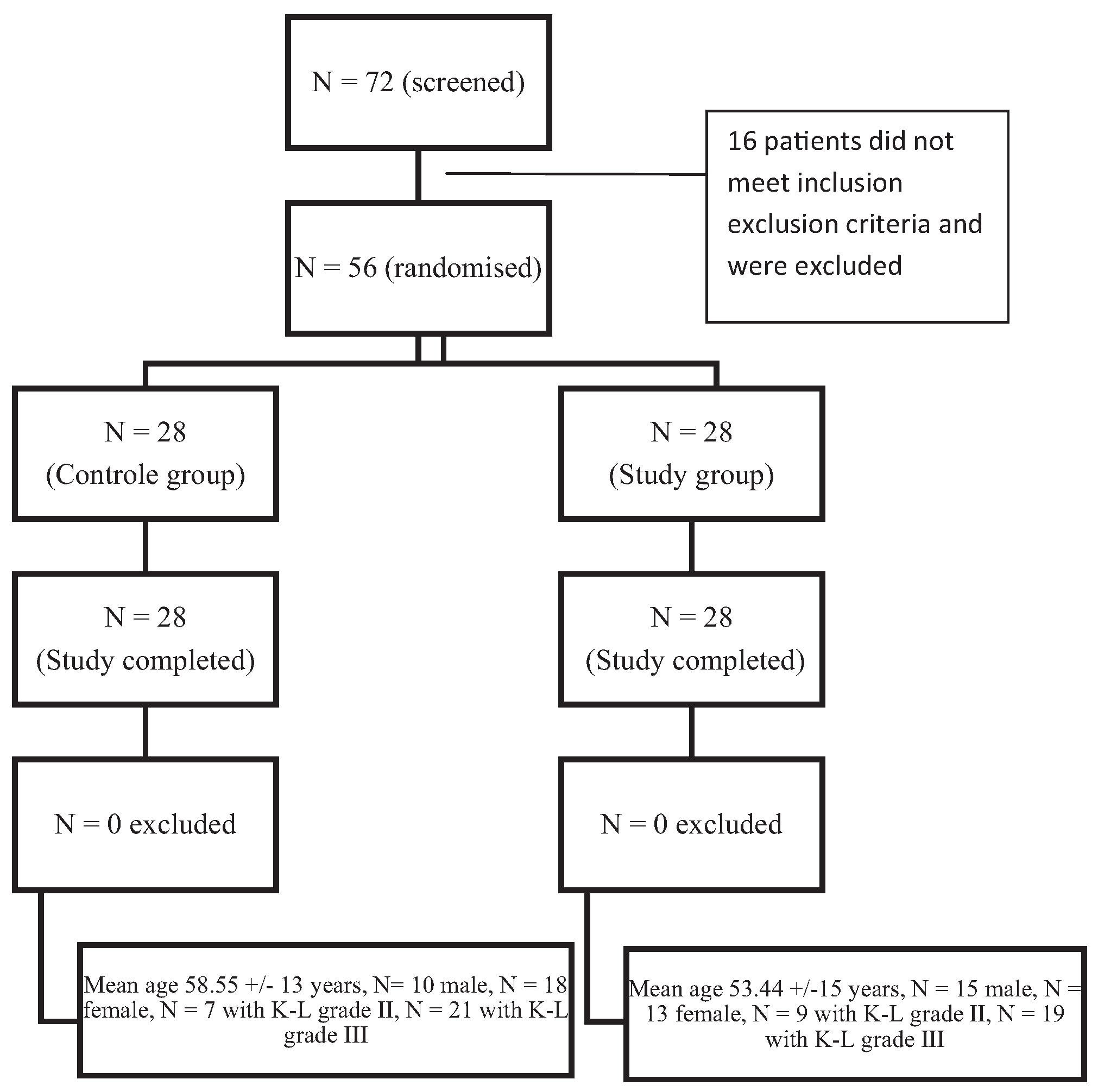
2.1. The patient randomization and the study design
2.2. The bone marrow harvesting and cell preparation
2.3. The flow cytometry
2.4. The intra-articular injection procedure and the follow-up period
2.5. The clinical assessment
2.5.1. Knee Society Score (KSS)
2.5.2. Knee Osteoarthritis Outcome Score (KOOS)
2.5.3. Radiological assessment
2.6. Statistical analysis
3. Results
4. Discussion
5. Conclusions
Conflict of interest
References
- Kon, E; Filardo, G; Di Matteo, B. PRP for cartilage: real hope or just hype? In: 12th World Congress of the International Cartilage Repair Society Main Programme & Extended Abstracts 15.3.5.
- Brittberg, M. Cell carriers as the next generation of cell therapy for cartilage repair: a review of the matrix-induced autologous chondrocyte implantation procedure. Am J Sports Med 2010, 38, 1259–71. http://dx.doi.org/10.1177/0363546509346395. [CrossRef] [PubMed]
- Getgood, A; Brooks, R; Fortier, L; Rushton, N. Articular cartilage tissue engineering: today’s research, tomorrow’s practice? J Bone Jt Surg Br 2009, 91, 565–76. http://dx.doi.org/10.1302/0301-620X.91B5.21832. [CrossRef] [PubMed]
- Caplan, AI; Dennis, JE. Mesenchymal stem cells as trophic mediators. J Cell Biochem 2006, 98, 1076–84. http://dx.doi.org/10.1002/jcb.20886. [CrossRef] [PubMed]
- Friedenstein, AJ; Piatetzky-Shapiro, II; Petrakova, KV. Osteogenesis in transplants of bone marrow cells. J Embryol Exp Morphol 1966, 16, 381–90. [Google Scholar] [PubMed]
- da Silva Meirelles, L; Caplan, AI; Nardi, NB. In search of the in vivo identity of mesenchymal stem cells. Stem Cells 2008, 26, 2287–99. http://dx.doi.org/10.1634/stemcells.2007-1122. [CrossRef] [PubMed]
- Riekstina, U; Cakstina, I; Parfejevs, V; Hoogduijn, M; Jankovskis, G; Muiznieks, I; et al. Embryonic stem cell marker expression pattern in human mesenchymal stem cells derived from bone marrow, adipose tissue, heart and dermis. Stem Cell Rev 2009, 5, 378–86. http://dx.doi.org/10.1007/s12015-009-9094-9. [CrossRef] [PubMed]
- Afizah, H; Yang, Z; Hui, JHP; Ouyang, HW; Lee, EH. A comparison between the chondrogenic potential of human bone marrow stem cells (BMSCs) and adipose-derived stem cells (ADSCs) taken from the same donors. Tissue Eng 2007, 13, 659–66. http://dx.doi.org/10.1089/ten.2006.0118.
- Frisbie, D; Hague, BA; Kisiday, JD. Stem cells as a treatment for osteoarthritis. Proceedings Am College Vet Surg; 2007; pp. 39–42. [Google Scholar]
- Centeno, CJ; Busse, D; Kisiday, J; Keohan, C; Freeman, M; Karli, D. Increased knee cartilage volume in degenerative joint disease using percutaneously implanted, autologous mesenchymal stem cells. Pain Physician 2008, 11, 343–53. [Google Scholar] [PubMed]
- Alvarez-Viejo, M; Menendez-Menendez, Y; Blanco-Gelaz, MA; Ferrero-Gutierrez, A; Fernandez-Rodriguez, MA; Gala, J; et al. Quantifying mesenchymal stem cells in the mononuclear cell fraction of bone marrow samples obtained for cell therapy. Transplant Proc 2013, 45, 434–9. [Google Scholar] [CrossRef] [PubMed]
- Gupta, PK; Das, AK; Chullikana, A; Majumdar, AS. Mesenchymal stem cells for cartilage repair in osteoarthritis. Stem Cell Res Ther 2012, 3, 25. http://dx.doi.org/10.1186/scrt116. [CrossRef] [PubMed]
- Jo, CH; Lee, YG; Shin, WH; Kim, H; Chai, JW; Jeong, EC; et al. Intra-articular injection of mesenchymal stem cells for the treatment of osteoarthritis of the knee: a proof-of-concept clinical trial. Stem Cells 2014, 32, 1254–66. http://dx.doi.org/10.1002/stem.1634. [PubMed]
- John, N; Insall, LDD. Rationale of the knee society clinical rating system. Clin Orthop Relat Res 1989, 248, 13–4. http://dx.doi.org/10.1097/00003086-198911000-00004.
- Roos, EM; Roos, HP; Lohmander, LS; Ekdahl, C; Beynnon, BD. Knee Injury and Osteoarthritis Outcome Score (KOOS) – development of a self-administered outcome measure. J Orthop Sports Phys Ther 1998, 28, 88–96. http://dx.doi.org/10.2519/jospt.1998.28.2.88. [CrossRef] [PubMed]
- Kim, J-D; Lee, GW; Jung, GH; Kim, CK; Kim, T; Park, JH; et al. Clinical outcome of autologous bone marrow aspirates concentrate (BMAC) injection in degenerative arthritis of the knee. Eur J Orthop Surg Traumatol 2014, 24, 1505–11. http://dx.doi.org/10.1007/s00590-013-1393-9. [CrossRef] [PubMed]
- Centeno, C; Pitts, J; Al-Sayegh, H; Freeman, M; Centeno, C; Pitts, J; et al. Efficacy of autologous bone marrow concentrate for knee osteoarthritis with and without adipose graft, efficacy of autologous bone marrow concentrate for knee osteoarthritis with and without adipose graft. BioMed Res Int 2014, 2014, AN e370621. http://dx.doi.org/10.1155/2014/370621. [CrossRef] [PubMed]
- Koh, Y-G; Jo, S-B; Kwon, O-R; Suh, D-S; Lee, S-W; Park, S-H; et al. Mesenchymal stem cell injections improve symptoms of knee osteoarthritis. Arthrosc J Arthrosc Relat Surg 2013, 29, 748–55. http://dx.doi.org/10.1016/j.arthro.2012.11.017. [CrossRef] [PubMed]
- Nejadnik, H; Hui, JH; Feng Choong, EP; Tai, B-C; Lee, EH. Autologous bone marrow-derived mesenchymal stem cells versus autologous chondrocyte implantation: an observational cohort study. Am J Sports Med 2010, 38, 1110–6. http://dx.doi.org/10.1177/0363546509359067. [CrossRef] [PubMed]
- Saw, K-Y; Anz, A; Siew-Yoke Jee, C; Merican, S; Ching-Soong, Ng R; Roohi, SA; et al. Articular cartilage regeneration with autologous peripheral blood stem cells versus hyaluronic acid: a randomized controlled trial. Arthrosc J Arthrosc Relat Surg 2013, 29, 684–94. http://dx.doi.org/10.1016/j.arthro.2012.12.008. [CrossRef] [PubMed]
- Oliver, KS; Bayes, M; Crane, DM; Pathikonda, C. Clinical outcome of bone marrow concentrate in knee osteoarthritis. J Prolother. 2015. http://www.journalofprolotherapy.com/clinical-outcome-of-bone-marrow-concentrate-in-knee-osteoarthritis/ (accessed 07.08.16).
- Jakobsons, EIC. Bone marrow mononuclear cell separation yield in myocardium infarction, coronary disease and type 2 diabetes and dilated cardiomyopathy patient groups. Cytotherapy 2013, 15, S31. http://dx.doi.org/10.1016/j.jcyt.2013.01.117. [CrossRef]
- Scharstuhl, A; Schewe, B; Benz, K; Gaissmaier, C; Bühring, H-J; Stoop, R. Chondrogenic potential of human adult mesenchymal stem cells is independent of age or osteoarthritis etiology. Stem Cells. 2007, 25, pp. 3244–51. http://dx.doi.org/10.1634/stemcells.2007-0300.
- Bannuru, RR; Natov, NS; Dasi, UR; Schmid, CH; McAlindon, TE. Therapeutic trajectory following intra-articular hyaluronic acid injection in knee osteoarthritis – meta-analysis. Osteoarthr Cartil 2010, 19, 611–9. http://dx.doi.org/10.1016/j.joca.2010.09.014. [CrossRef] [PubMed]
- Navarro-Sarabia, F; Coronel, P; Collantes, E; Navarro, FJ; de la Serna, AR; Naranjo, A; et al. A 40-month multicentre, randomised placebo-controlled study to assess the efficacy and carry-over effect of repeated intra-articular injections of hyaluronic acid in knee osteoarthritis: the AMELIA project. Ann Rheum Dis 2011, 70, 1957–62. http://dx.doi.org/10.1136/ard.2011.152017. [CrossRef] [PubMed]
- Richette, P; Chevalier, X; Ea, HK; Eymard, F; Henrotin, Y; Ornetti, P; et al. Hyaluronan for knee osteoarthritis: an updated meta-analysis of trials with low risk of bias. RMD Open 2015, 1. http://dx.doi.org/10.1136/rmdopen-2015-000071. [CrossRef] [PubMed]
- Trigkilidas, D; Anand, A. The effectiveness of hyaluronic acid intra-articular injections in managing osteoarthritic knee pain. Ann R Coll Surg Engl 2013, 95, 545–51. http://dx.doi.org/10.1308/003588413X13629960049432. [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria | Exclusion criteria |
| Degenerative osteoarthritis of the knee Grade 2–3 Kallgren–Lawrence classification At least 6 months of persisting OA symptoms Voluntarily agreed to participate and signed informed consent form | Age over 75 Oncologic diseases. Severe kidney, lungs or liver function disorder Hematologic diseases including anemia and thrombocytopenia. First type diabetes mellitus Severe effusion, contracture and axial deformities in the knee joint |
| Septic arthritis or skin disorders Use of NSAID medication for more than 1 week during observations period. Previous injection in target knee within 2 months before and during observation period Use of corticosteroids and immunosuppressive agents |
| KOOS score subscale | BM MNC group | HA group |
| Symptoms | 5.07 | 12.62* |
| Pain | 25.44* | 11.37* |
| Activity and daily living | 21.36* | 19.09* |
| Sport | 19.00 | 5.97 |
| Quality of life | 28.83* | 18.90* |
| Total | 18.25* | 12.59* |
| KSS score subscale | Improvement at 12 months | |
| BMNC | HA | |
| Knee score | 25.42* | 10.73* |
| Function | 38.32* | 17.5* |
© 2017 The Lithuanian University of Health Sciences. Production and hosting by Elsevier Sp. z o.o. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Share and Cite
Goncars, V.; Jakobsons, E.; Blums, K.; Briede, I.; Patetko, L.; Erglis, K.; Erglis, M.; Kalnberzs, K.; Muiznieks, I.; Erglis, A. The comparison of knee osteoarthritis treatment with single-dose bone marrow-derived mononuclear cells vs. hyaluronic acid injections. Medicina 2017, 53, 101-108. https://doi.org/10.1016/j.medici.2017.02.002
Goncars V, Jakobsons E, Blums K, Briede I, Patetko L, Erglis K, Erglis M, Kalnberzs K, Muiznieks I, Erglis A. The comparison of knee osteoarthritis treatment with single-dose bone marrow-derived mononuclear cells vs. hyaluronic acid injections. Medicina. 2017; 53(2):101-108. https://doi.org/10.1016/j.medici.2017.02.002
Chicago/Turabian StyleGoncars, Valdis, Eriks Jakobsons, Kristaps Blums, Ieva Briede, Liene Patetko, Kristaps Erglis, Martins Erglis, Konstantins Kalnberzs, Indrikis Muiznieks, and Andrejs Erglis. 2017. "The comparison of knee osteoarthritis treatment with single-dose bone marrow-derived mononuclear cells vs. hyaluronic acid injections" Medicina 53, no. 2: 101-108. https://doi.org/10.1016/j.medici.2017.02.002
APA StyleGoncars, V., Jakobsons, E., Blums, K., Briede, I., Patetko, L., Erglis, K., Erglis, M., Kalnberzs, K., Muiznieks, I., & Erglis, A. (2017). The comparison of knee osteoarthritis treatment with single-dose bone marrow-derived mononuclear cells vs. hyaluronic acid injections. Medicina, 53(2), 101-108. https://doi.org/10.1016/j.medici.2017.02.002