Retrospective Study on the Clinical Superiority of the Vacuum-Assisted Closure System with a Silicon-Based Dressing over the Conventional Tie-over Bolster Technique in Skin Graft Fixation


Abstract
:1. Introduction
2. Methods
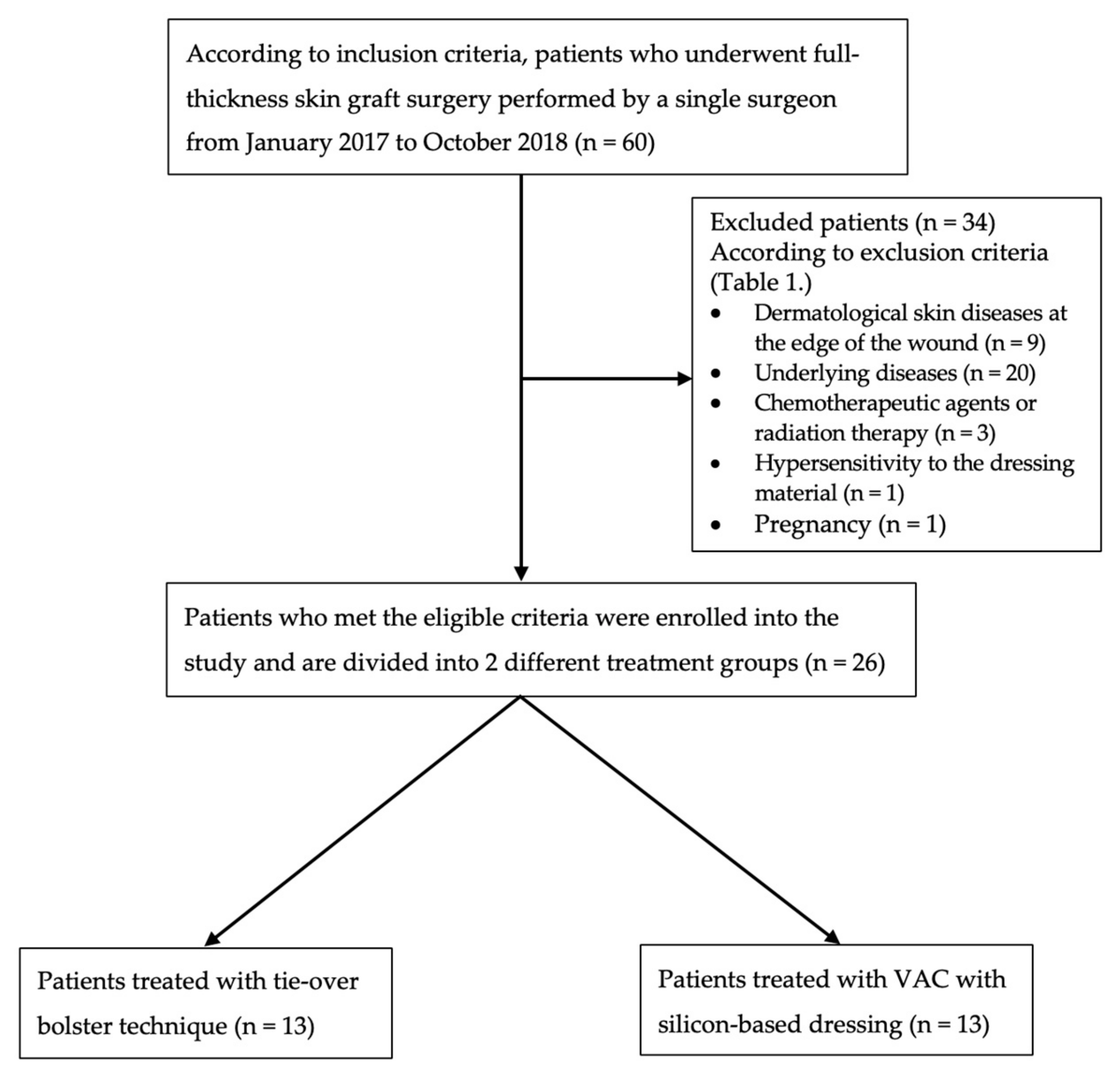
2.1. Patient Selection
2.2. Surgical Technique
2.2.1. Tie-over Bolster Technique
2.2.2. VAC Therapy with Silicon-based Dressing
2.3. Operative Time
2.4. Pain Assessment
2.5. Skin Graft Take Rate
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics
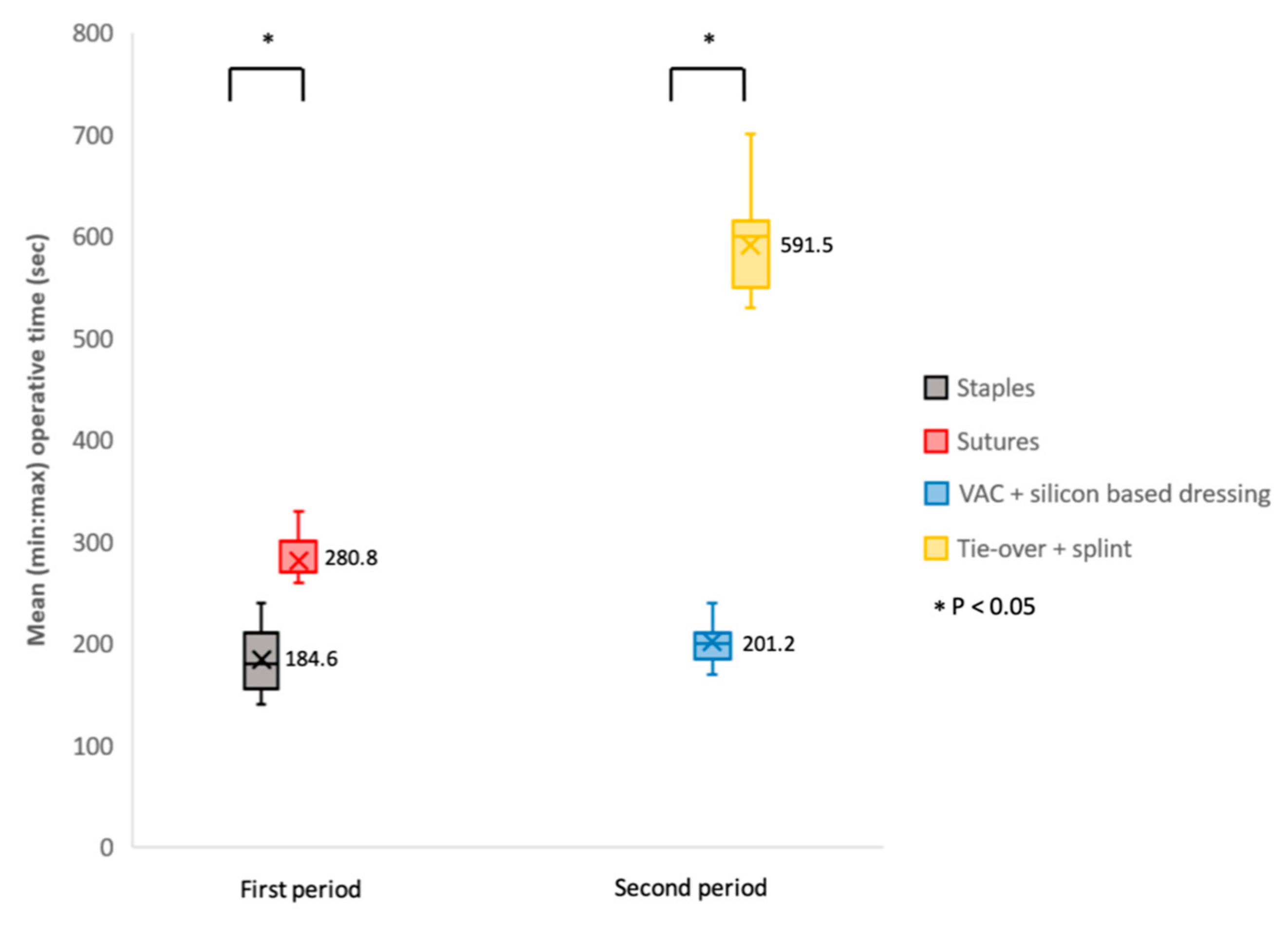
3.2. Operative Time
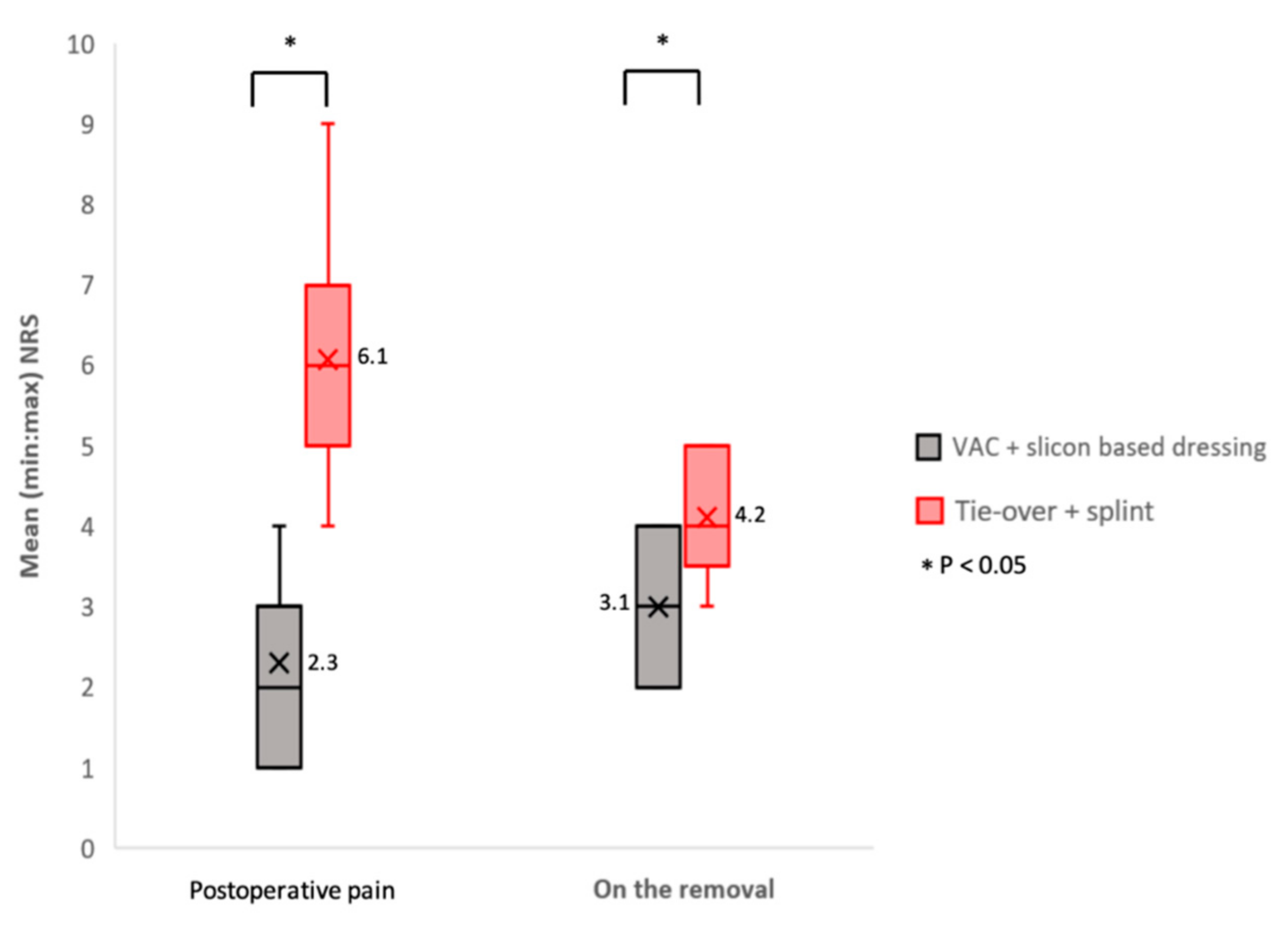
3.3. Pain
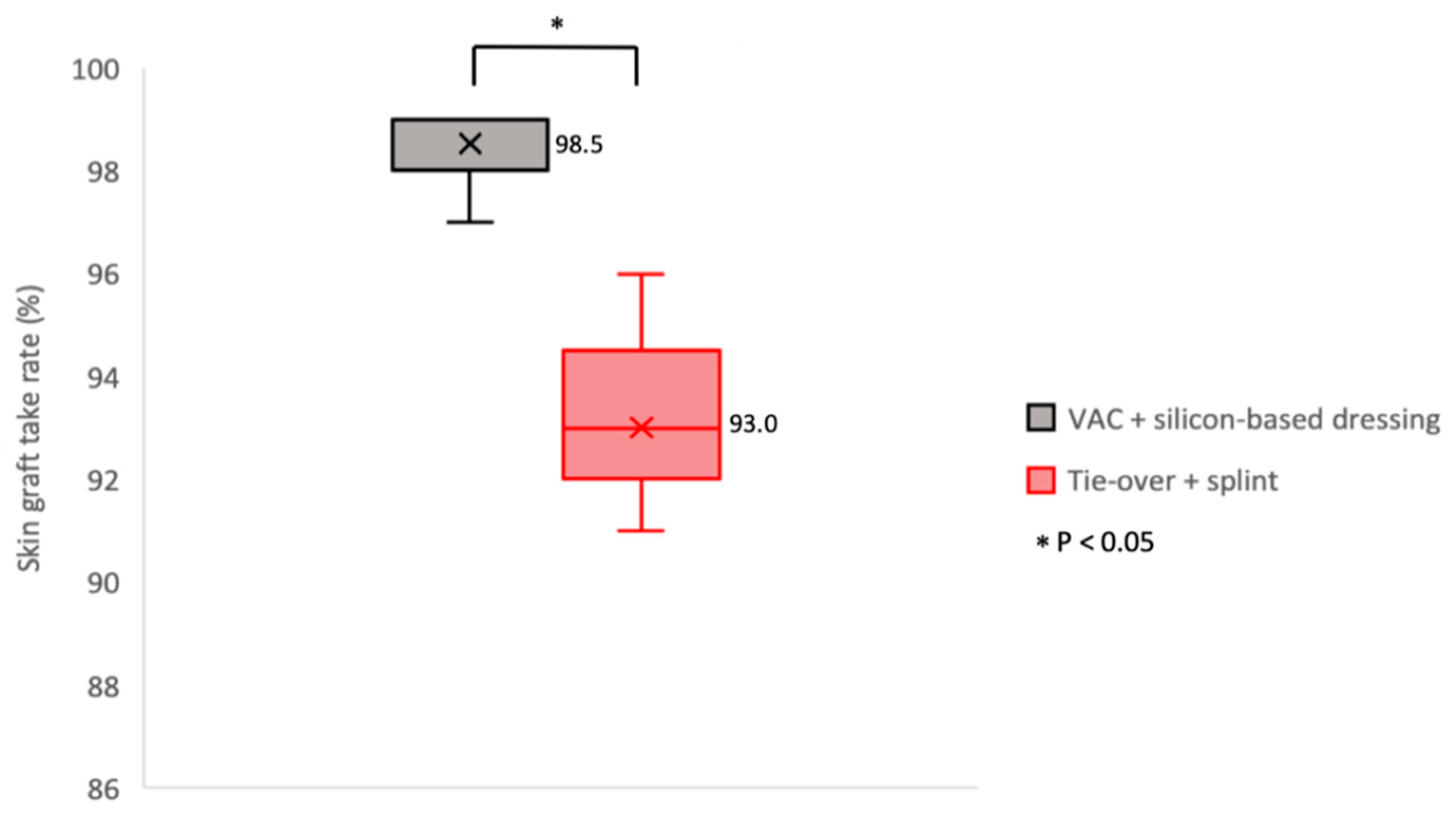
3.4. Skin Graft Take Rate
4. Discussion
Restrictions of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Thorne, C.H. Techniques and Principles in Plastic Surgery. In Grabb & Smith’s Plastic Surgery, 6th ed.; LWW: Philadelaphia, PA, USA, 2007; pp. 7–8. [Google Scholar]
- Patton, M.L.; Mullins, R.F.; Smith, D.; Korentager, R. An open, prospective, randomized pilot investigation evaluating pain with the use of a soft silicone wound contact layer vs bridal veil and staples on split thickness skin grafts as a primary dressing. J. Burn Care Res. 2013, 34, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Struk, S.; Correia, N.; Guenane, Y.; Revol, M.; Cristofari, S. Full-thickness skin grafts for lower leg defects coverage: Interest of postoperative immobilization. Ann. Chir. Plast. Esthet. 2018, 63, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Yen, Y.H.; Lin, C.M.; Hsu, H.; Chen, Y.C.; Chen, Y.W.; Li, W.Y.; Hsieh, C.N.; Huang, C.C. Skin Graft Fixation Using Hydrofiber (Aquacel(R) Extra). Ann. Plast. Surg. 2018, 80, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Gardner, S.E.; Abbott, L.I.; Fiala, C.A.; Rakel, B.A. Factors associated with high pain intensity during wound care procedures: A model. Wound Repair Regen. 2017, 25, 558–563. [Google Scholar] [CrossRef]
- Joyce, C.W.; Joyce, K.M.; Mahon, N.; Chan, J.C.; Sugrue, C.M.; Dockery, P.; Carroll, S.M.; Kelly, J.L. A novel barbed suture tie-over dressing for skin grafts: A comparison with traditional techniques. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1237–1241. [Google Scholar] [CrossRef]
- White, R.; Morris, C. Mepitel: A non-adherent wound dressing with Safetac technology. Br. J. Nurs. 2009, 18, 58–64. [Google Scholar] [CrossRef]
- Kantak, N.A.; Mistry, R.; Halvorson, E.G. A review of negative-pressure wound therapy in the management of burn wounds. Burns 2016, 42, 1623–1633. [Google Scholar] [CrossRef]
- Körber, A.; Franckson, T.; Grabbe, S.; Dissemond, J. Vacuum assisted closure device improves the take of mesh grafts in chronic leg ulcer patients. Dermatology 2008, 216, 250–256. [Google Scholar] [CrossRef]
- Yanaral, F.; Balci, C.; Ozgor, F.; Simsek, A.; Onuk, O.; Aydin, M.; Nuhoglu, B. Comparison of conventional dressings and vacuum-assisted closure in the wound therapy of Fournier’s gangrene. Arch. Ital. Urol. Androl. 2017, 89, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, R.; Ballantyne, D.L. Skin Grafts. Plast. Surg. 1990, 1, 221–271. [Google Scholar]
- Nemakayala, D.R.; Ramphul, K. Caplan Syndrome; StatPearls Publishing LLC: Treasure Island, FL, USA, 2018. [Google Scholar]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: A systematic literature review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef]
- Langtry, J.A.; Kirkham, P.; Martin, I.C.; Fordyce, A. Tie-over bolster dressings may not be necessary to secure small full thickness skin grafts. Dermatol. Surg. 1998, 24, 1350–1353. [Google Scholar] [CrossRef] [PubMed]
- Kromka, W.; Cameron, M.; Fathi, R. Tie-Over Bolster Dressings vs Basting Sutures for the Closure of Full-Thickness Skin Grafts: A Review of the Literature. J. Cutan. Med. Surg. 2018, 22, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Petkar, K.S.; Dhanraj, P.; Kingsly, P.M.; Sreekar, H.; Lakshmanarao, A.; Lamba, S.; Shetty, R.; Zachariah, J.R. A prospective randomized controlled trial comparing negative pressure dressing and conventional dressing methods on split-thickness skin grafts in burned patients. Burns 2011, 37, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Bi, H.; Khan, M.; Li, J.; Pestana, I.A. Use of Incisional Negative Pressure Wound Therapy in Skin-Containing Free Tissue Transfer. J. Reconstr. Microsurg. 2018, 34, 200–205. [Google Scholar] [CrossRef]
- Waltzman, J.T.; Bell, D.E. Vacuum-assisted closure device as a split-thickness skin graft bolster in the burn population. J. Burn Care Res. 2014, 35, e338–e342. [Google Scholar] [CrossRef]
- Scherer, L.A.; Shiver, S.; Chang, M.; Meredith, J.W.; Owings, J.T. The vacuum assisted closure device: A method of securing skin grafts and improving graft survival. Arch. Surg. 2002, 137, 930–933. [Google Scholar] [CrossRef]
- Nakamura, Y.; Fujisawa, Y.; Ishitsuka, Y.; Tanaka, R.; Maruyama, H.; Okiyama, N.; Watanabe, R.; Fujimoto, M. Negative-pressure closure was superior to tie-over technique for stabilization of split-thickness skin graft in large or muscle-exposing defects: A retrospective study. J. Dermatol. 2018, 45, 1207–1210. [Google Scholar] [CrossRef]
- Shin, S.H.; Kim, C.; Lee, Y.S.; Kang, J.W.; Chung, Y.G. Feasibility and Advantages of Full Thickness Skin Graft from the Anterolateral Thigh. J. Hand Surg. (Asian Pac. Vol.) 2017, 22, 497–502. [Google Scholar] [CrossRef]
- Wang, D.S. Re: How Slow is Too Slow? Correlation of Operative Time to Complications: An Analysis from the Tennessee Surgical Quality Collaborative. J. Urol. 2016, 195, 1510–1511. [Google Scholar] [CrossRef]
- Maoz, G.; Phillips, M.; Bosco, J.; Slover, J.; Stachel, A.; Inneh, I.; Iorio, R. The Otto Aufranc Award: Modifiable versus nonmodifiable risk factors for infection after hip arthroplasty. Clin. Orthop. Relat. Res. 2015, 473, 453–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.; Clymer, J.W.; Qadeer, R.A.; Ferko, N.; Sadeghirad, B.; Cameron, C.G.; Amaral, J.F. Procedure costs associated with the use of Harmonic devices compared to conventional techniques in various surgeries: A systematic review and meta-analysis. Clin. Outcomes Res. 2018, 10, 399–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuki, A.; Takenouchi, T.; Takatsuka, S.; Fujikawa, H.; Abe, R. Investigating the use of tie-over dressing after skin grafting. J. Dermatol. 2017, 44, 1317–1319. [Google Scholar] [CrossRef] [PubMed]
- David, F.; Wurtz, J.L.; Breton, N.; Bisch, O.; Gazeu, P.; Kerihuel, J.C.; Guibon, O. A randomised, controlled, non-inferiority trial comparing the performance of a soft silicone-coated wound contact layer (Mepitel One) with a lipidocolloid wound contact layer (UrgoTul) in the treatment of acute wounds. Int. Wound J. 2018, 15, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.; Weinshenker, B.; Mikail, S.; Edgley, K. Depression before and after diagnosis of multiple sclerosis. Mult. Scler. J. 1995, 1, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Cutting, K.F. Impact of adhesive surgical tape and wound dressings on the skin, with reference to skin stripping. J. Wound Care 2008, 17, 157–158. [Google Scholar] [CrossRef]
- Moore, Z.E.; Webster, J. Dressings and topical agents for preventing pressure ulcers. Cochrane Database Syst. Rev. 2018, 12, CD009362. [Google Scholar] [CrossRef] [Green Version]
- Asghari, S.; Logsetty, S.; Liu, S. Imparting commercial antimicrobial dressings with low-adherence to burn wounds. Burns 2016, 42, 877–883. [Google Scholar] [CrossRef]
- Platt, A.J.; Phipps, A.; Judkins, K. A comparative study of silicone net dressing and paraffin gauze dressing in skin-grafted sites. Burns 1996, 22, 543–545. [Google Scholar] [CrossRef]
- Vloemans, A.F.; Kreis, R.W. Fixation of skin grafts with a new silicone rubber dressing (Mepitel). Scand. J. Plast. Reconstr. Surg. Hand Surg. 1994, 28, 75–76. [Google Scholar] [CrossRef]
- Burton, F. An evaluation of non-adherent wound-contact layers for acute traumatic and surgical wounds. J. Wound Care 2004, 13, 371–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamietz, I.A.; Mose, S.; Haberl, A.; Saran, F.H.; Thilmann, C.; Böttcher, H.D. Effect of self-adhesive, silicone-coated polyamide net dressing on irradiated human skin. Radiat. Oncol. Investig. 1995, 2, 277–282. [Google Scholar] [CrossRef]
- Gotschall, C.S.; Morrison, M.I.; Eichelberger, M.R. Prospective, randomized study of the efficacy of Mepitel on children with partial-thickness scalds. J. Burn Care Rehabil. 1998, 19, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Robert, N. Negative pressure wound therapy in orthopaedic surgery. Orthop. Traumatol. Surg. Res. 2017, 103, S99–S103. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria |
|
| Exclusion criteria |
|
| Variables | VAC with Silicon-based Dressing (n = 13) | Tie-Over Bolster Technique (n = 13) | p |
|---|---|---|---|
| Age (yrs) | |||
| Mean | 48.8 | 50.7 | 0.8 |
| SD | 21.6 | 22.5 | |
| Gender (cts) | 0.67 | ||
| Male | 10 | 9 | |
| Female | 3 | 4 | |
| Graft area (cm2) | |||
| Mean | 23.5 | 19.3 | 0.23 |
| SD | 8.3 | 9.3 | |
| Graft fixation on wound bed (case cts) | |||
| Staple | 13 | 0 | |
| Suture | 0 | 13 | |
| Splint using | 0 | 13 | |
| First operative time (secs) | |||
| Mean | 184.6 | 280.8 | < 0.05* |
| SD | 33.6 | 51.7 | |
| Second operative time (secs) | |||
| Mean | 201.2 | 591.5 | < 0.05* |
| SD | 54.4 | 162.9 | |
| Postoperative pain (NRS) | |||
| Mean | 2.3 | 6.1 | < 0.05* |
| SD | 3.0 | 2.3 | |
| Pain on the removal (NRS) | |||
| Mean | 3.1 | 4.2 | < 0.05* |
| SD | 2.8 | 2.4 | |
| Skin graft take rate (%) | |||
| Mean | 98.5 | 93.0 | < 0.05* |
| SD | 22.9 | 21.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, P.-R.; Wu, S.-H.; Hsieh, M.-C.; Huang, S.-H. Retrospective Study on the Clinical Superiority of the Vacuum-Assisted Closure System with a Silicon-Based Dressing over the Conventional Tie-over Bolster Technique in Skin Graft Fixation. Medicina 2019, 55, 781. https://doi.org/10.3390/medicina55120781
Chou P-R, Wu S-H, Hsieh M-C, Huang S-H. Retrospective Study on the Clinical Superiority of the Vacuum-Assisted Closure System with a Silicon-Based Dressing over the Conventional Tie-over Bolster Technique in Skin Graft Fixation. Medicina. 2019; 55(12):781. https://doi.org/10.3390/medicina55120781
Chicago/Turabian StyleChou, Ping-Ruey, Sheng-Hua Wu, Meng-Chien Hsieh, and Shu-Hung Huang. 2019. "Retrospective Study on the Clinical Superiority of the Vacuum-Assisted Closure System with a Silicon-Based Dressing over the Conventional Tie-over Bolster Technique in Skin Graft Fixation" Medicina 55, no. 12: 781. https://doi.org/10.3390/medicina55120781
APA StyleChou, P. -R., Wu, S. -H., Hsieh, M. -C., & Huang, S. -H. (2019). Retrospective Study on the Clinical Superiority of the Vacuum-Assisted Closure System with a Silicon-Based Dressing over the Conventional Tie-over Bolster Technique in Skin Graft Fixation. Medicina, 55(12), 781. https://doi.org/10.3390/medicina55120781