Predictive Factors of Adrenal Insufficiency in Outpatients with Indeterminate Serum Cortisol Levels: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. ACTH Stimulation Test Protocol
2.2. Data Collection
2.3. Definitions
2.4. Statistical Analysis
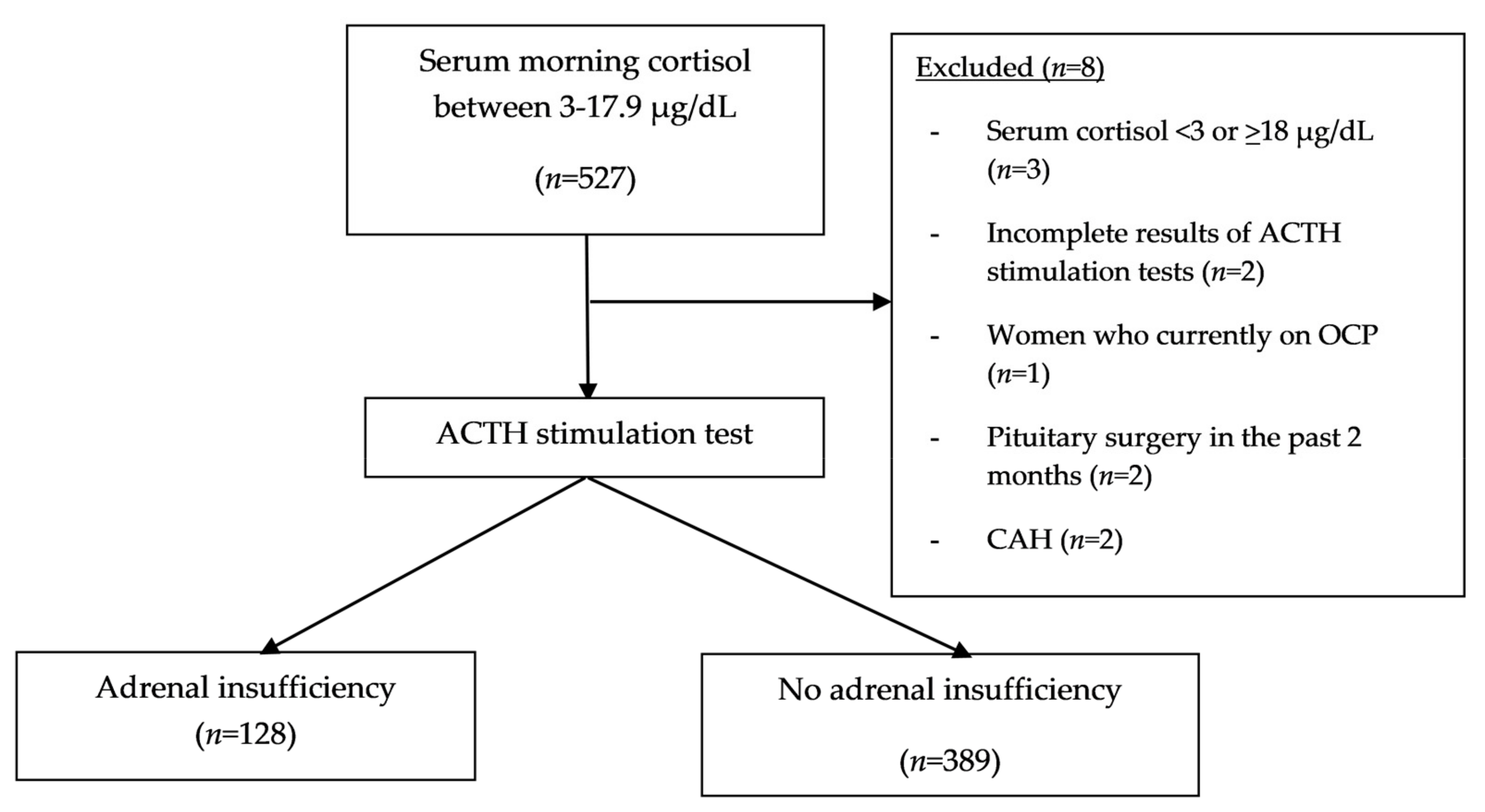
3. Results
3.1. Baseline Characteristics and Univariable Analysis of Factors Associated with AI
3.2. Multivariable Analysis for Clinical and Biochemical Factors Related to AI
3.3. Subgroup Analysis of Patients with and without Pituitary/Adrenal Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chabre, O.; Goichot, B.; Zenaty, D.; Bertherat, J. Group 1. Epidemiology of primary and secondary adrenal insufficiency: Prevalence and incidence, acute adrenal insufficiency, long-term morbidity and mortality. Ann. D’endocrinol. 2017, 78, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Kamrat, N. Adrenal insufficiency from over-the-counter medicine as a cause of shock in rural area of Thailand: A study at Sisaket Provincial Hospital during October 2012--October 2013. Trop. Dr. 2015, 45, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Weravut Mingkuan, S.D. Prevalence and Predictive Factors of Adrenal Insufficiency in Septic Shock Patients. J. Med. Assoc. Thail. 2018, 101, 1591–1597. [Google Scholar]
- Pazderska, A.; Pearce, S.H. Adrenal insufficiency—Recognition and management. Clin. Med. 2017, 17, 258–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagg, E.; Asplund, K.; Lithner, F. Value of basal plasma cortisol assays in the assessment of pituitary-adrenal insufficiency. Clin. Endocrinol. 1987, 26, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, H.K.; Walker, B.R.; Seckl, J.R.; Padfield, P.L. Ten years on: Safety of short synacthen tests in assessing adrenocorticotropin deficiency in clinical practice. J. Clin. Endocrinol. Metab. 2003, 88, 2106–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odeniyi, I.A.; Fasanmade, O.A.; Ajala, M.O.; Ohwovoriole, A.E. CD4 count as a predictor of adrenocortical insufficiency in persons with human immunodeficiency virus infection: How useful? Indian J. Endocrinol. Metab. 2013, 17, 1012–1017. [Google Scholar] [CrossRef]
- Ben-Shlomo, A.; Mirocha, J.; Gwin, S.M.; Khine, A.K.; Liu, N.A.; Sheinin, R.C.; Melmed, S. Clinical factors associated with biochemical adrenal-cortisol insufficiency in hospitalized patients. Am. J. Med. 2014, 127, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Verbeeten, K.C.; Ahmet, A.H. The role of corticosteroid-binding globulin in the evaluation of adrenal insufficiency. J. Pediatr. Endocrinol. Metab. 2018, 31, 107–115. [Google Scholar] [CrossRef]
- Annane, D.; Pastores, S.M.; Arlt, W.; Balk, R.A.; Beishuizen, A.; Briegel, J.; Carcillo, J.; Christ-Crain, M.; Cooper, M.S.; Marik, P.E.; et al. Critical illness-related corticosteroid insufficiency (CIRCI): A narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM). Intensive Care Med. 2017, 43, 1781–1792. [Google Scholar] [CrossRef]
- Perton, F.T.; Mijnhout, G.S.; Kollen, B.J.; Rondeel, J.M.; Franken, A.A.; Groeneveld, P.H. Validation of the 1 mug short synacthen test: An assessment of morning cortisol cut-off values and other predictors. Neth. J. Med. 2017, 75, 14–20. [Google Scholar] [PubMed]
- Manosroi, W.; Phimphilai, M.; Khorana, J.; Atthakomol, P. Diagnostic performance of basal cortisol level at 0900-1300h in adrenal insufficiency. PLoS ONE 2019, 14, e0225255. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, S.R.; Allolio, B.; Arlt, W.; Barthel, A.; Don-Wauchope, A.; Hammer, G.D.; Husebye, E.S.; Merke, D.P.; Murad, M.H.; Stratakis, C.A.; et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 364–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaddey, H.L.; Holder, K. Unintentional weight loss in older adults. Am. Fam. Physician 2014, 89, 718–722. [Google Scholar]
- Bacon, G.E.; Kenny, F.M.; Murdaugh, H.V.; Richards, C. Prolonged serum half-life of cortisol in renal failure. Johns Hopkins Med. J. 1973, 132, 127–131. [Google Scholar]
- Nolan, G.E.; Smith, J.B.; Chavre, V.J.; Jubiz, W. Spurious overestimation of plasma cortisol in patients with chronic renal failure. J. Clin. Endocrinol. Metab. 1981, 52, 1242–1245. [Google Scholar] [CrossRef]
- Rosman, P.M.; Benn, R.; Kay, M.; Wallace, E.Z. Cortisol binding in uremic plasma. II. Decreased cortisol binding to albumin. Nephron 1984, 37, 229–231. [Google Scholar] [CrossRef]
- Siamopoulos, K.C.; Dardamanis, M.; Kyriaki, D.; Pappas, M.; Sferopoulos, G.; Alevisou, V. Pituitary adrenal responsiveness to corticotropin-releasing hormone in chronic uremic patients. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 1990, 10, 153–156. [Google Scholar]
- Clodi, M.; Riedl, M.; Schmaldienst, S.; Vychytil, A.; Kotzmann, H.; Kaider, A.; Bieglmayer, C.; Mayer, G.; Waldhausl, W.; Luger, A. Adrenal function in patients with chronic renal failure. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 1998, 32, 52–55. [Google Scholar] [CrossRef] [Green Version]
- Raff, H.; Trivedi, H. Circadian rhythm of salivary cortisol, plasma cortisol, and plasma ACTH in end-stage renal disease. Endocr. Connect. 2013, 2, 23–31. [Google Scholar] [CrossRef]
- Suzuki, R.; Morita, H.; Nishiwaki, H.; Yoshimura, A. Adrenal insufficiency in a haemodialysis patient. NDT Plus 2010, 3, 99–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broersen, L.H.; Pereira, A.M.; Jorgensen, J.O.; Dekkers, O.M. Adrenal Insufficiency in Corticosteroids Use: Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2015, 100, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Finken, M.J.; Mul, D. Cushing’s syndrome and adrenal insufficiency after intradermal triamcinolone acetonide for keloid scars. Eur. J. Pediatr. 2010, 169, 1147–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bockle, B.C.; Jara, D.; Nindl, W.; Aberer, W.; Sepp, N.T. Adrenal insufficiency as a result of long-term misuse of topical corticosteroids. Dermatolgy 2014, 228, 289–293. [Google Scholar] [CrossRef]
- Bancos, I.; Hahner, S.; Tomlinson, J.; Arlt, W. Diagnosis and management of adrenal insufficiency. Lancet. Diabetes Endocrinol. 2015, 3, 216–226. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Joo, M.S.; Kim, B.H.; Yoo, H.N.; Kim, S.E.; Kim, J.B.; Jang, M.K.; Kim, D.J.; Lee, M.S. Clinical characteristics and prevalence of adrenal insufficiency in hemodynamically stable patients with cirrhosis. Medicine 2018, 97, e11046. [Google Scholar] [CrossRef]
- Spadaro, L.; Noto, D.; Privitera, G.; Tomaselli, T.; Fede, G.; Scicali, R.; Piro, S.; Fayer, F.; Altieri, I.; Averna, M.; et al. Apolipoprotein AI and HDL are reduced in stable cirrhotic patients with adrenal insufficiency: A possible role in glucocorticoid deficiency. Scand. J. Gastroenterol. 2015, 50, 347–354. [Google Scholar] [CrossRef]
- Ouweneel, A.B.; van der Sluis, R.J.; Nahon, J.E.; Van Eck, M.; Hoekstra, M. Simvastatin treatment aggravates the glucocorticoid insufficiency associated with hypocholesterolemia in mice. Atherosclerosis 2017, 261, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, B.; Manning, R.W.; Davis, L.G.; Arentzen, R.; Baldino, F., Jr. Co-localization of corticotropin releasing factor and vasopressin mRNA in neurones after adrenalectomy. Nature 1985, 315, 59–61. [Google Scholar] [CrossRef]
- Oelkers, W. Hyponatremia and inappropriate secretion of vasopressin (antidiuretic hormone) in patients with hypopituitarism. N. Engl. J. Med. 1989, 321, 492–496. [Google Scholar] [CrossRef]
- Le Roux, C.W.; Meeran, K.; Alaghband-Zadeh, J. Is a 0900-h serum cortisol useful prior to a short synacthen test in outpatient assessment? Ann. Clin. Biochem. 2002, 39, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Struja, T.; Briner, L.; Meier, A.; Kutz, A.; Mundwiler, E.; Huber, A.; Mueller, B.; Bernasconi, L.; Schuetz, P. Diagnostic accuracy of basal cortisol level to predict adrenal insufficiency in cosyntropin testing: results from an observational cohort study with 804 patients. Endocr. Pract. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2017, 23, 949–961. [Google Scholar] [CrossRef] [PubMed]
- Chu, X.Y.; Zhang, L.; Yang, X.X.; Zhu, T.N. Primary Adrenal Insufficiency Due to Bilateral Adrenal Hematomas in a Patient with Primary Antiphospholipid Syndrome. Chin. Med. J. 2017, 130, 2517–2518. [Google Scholar] [CrossRef] [PubMed]
- Di Dalmazi, G.; Berr, C.M.; Fassnacht, M.; Beuschlein, F.; Reincke, M. Adrenal function after adrenalectomy for subclinical hypercortisolism and Cushing’s syndrome: A systematic review of the literature. J. Clin. Endocrinol. Metab. 2014, 99, 2637–2645. [Google Scholar] [CrossRef]
- Ajlan, A.; Almufawez, K.A.; Albakr, A.; Katznelson, L.; Harsh, G.R.t. Adrenal Axis Insufficiency After Endoscopic Transsphenoidal Resection of Pituitary Adenomas. World Neurosurg. 2018, 112, e869–e875. [Google Scholar] [CrossRef]
- Klose, M.; Lange, M.; Kosteljanetz, M.; Poulsgaard, L.; Feldt-Rasmussen, U. Adrenocortical insufficiency after pituitary surgery: An audit of the reliability of the conventional short synacthen test. Clin. Endocrinol. 2005, 63, 499–505. [Google Scholar] [CrossRef]
- Crowley, R.K.; Argese, N.; Tomlinson, J.W.; Stewart, P.M. Central hypoadrenalism. J. Clin. Endocrinol. Metab. 2014, 99, 4027–4036. [Google Scholar] [CrossRef]
- Chaudhuri, S.; Rao, K.N.; Patil, N.; Ommurugan, B.; Varghese, G. Addison’s Disease Mimicking as Acute Pancreatitis: A Case Report. J. Clin. Diagn. Res. 2017, 11, OD12–OD13. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Adrenal Insufficiency | No Adrenal Insufficiency | RR * | 95% CI * | p-Value |
|---|---|---|---|---|---|
| (n = 128) | (n = 389) | ||||
| Age, (mean ± SD) (yr) | 56.61 ± 16.97 | 48.80 ± 17.32 | <0.001 | ||
| Age group | |||||
| - <50 years old, n (%) | 40 (31.25) | 174 (44.73) | (Ref) | ||
| - ≥50 years old, n (%) | 88 (68.75) | 215 (55.27) | 1.55 | 1.06–2.25 | 0.024 |
| Male, n (%) | 68 (53.13) | 197 (50.64) | 1.07 | 0.87–1.68 | 0.673 |
| Weight, (mean ± SD) (kgs) | 58.23 ± 13.02 | 61.41 ± 16.07 | 0.98 | 0.97–1.00 | 0.083 |
| BMI, (mean ± SD) (kg/m2) | 22.87 ± 5.30 | 24.14 ± 6.65 | 0.97 | 0.96–1.00 | 0.065 |
| ACTH stimulation dose, n (%) | |||||
| - 1 µg | 41 (32.03) | 150 (38.56) | (Ref) | ||
| - 250 µg | 87 (67.97) | 239 (61.44) | 1.24 | 0.85–1.80 | 0.25 |
| Systolic blood pressure, (mean ± SD) (mmHg) | 121.37 ± 21.96 | 121.40 ± 9.93 | 0.99 | 0.99–1.00 | 0.99 |
| Diastolic blood pressure, (mean ± SD) (mmHg) | 71.99 ± 15.46 | 73.74 ± 12.84 | 0.99 | 0.98–1.00 | 0.271 |
| Underlying disease, n (%) | |||||
| - Diabetes mellitus | 21 (16.41) | 57 (14.69) | 1.1 | 0.69–1.75 | 0.684 |
| - Hypertension | 41 (32.03) | 83 (21.39) | 1.48 | 1.11–2.69 | 0.035 |
| - Chronic kidney disease | 11 (8.59) | 5 (1.29) | 2.94 | 1.58–5.46 | 0.001 |
| - Autoimmune disease | 24 (18.75) | 55 (14.14) | 1.27 | 0.82–1.99 | 0.271 |
| - Cancer | 4 (3.13) | 12 (3.08) | 1.01 | 0.37–2.73 | 0.984 |
| Symptom, n (%) | |||||
| - Fatigue | 36 (28.13) | 71 (18.25) | 1.49 | 1.01–2.20 | 0.039 |
| - Weight loss | 4 (3.13) | 22 (5.66) | 0.6 | 0.22–1.64 | 0.329 |
| - Orthostatic hypotension | 14 (10.94) | 36 (9.25) | 1.14 | 0.65–1.99 | 0.628 |
| - Nausea/vomiting | 4 (3.13) | 5 (1.29) | 1.82 | 0.67–4.92 | 0.238 |
| Indication for ACTH testing, n (%) | |||||
| - Exogenous steroid use | 59 (46.09) | 73 (18.77) | 2.49 | 1.76–3.53 | <0.001 |
| - Post-surgery of pituitary | 19 (14.84) | 86 (22.11) | 0.68 | 0.42–1.11 | 0.127 |
| - Pituitary tumor | 20 (17.09) | 97 (82.91) | 0.63 | 0.39–1.02 | 0.06 |
| - Pituitary hormonal deficiencies | 32 (25.0) | 119 (30.59) | 0.8 | 0.54–1.20 | 0.296 |
| - Adrenal disease | 11 (8.59) | 7 (1.80) | 2.6 | 1.40–4.83 | 0.002 |
| - Symptoms of adrenal insufficiency | 40 (31.25) | 131 (33.68) | 0.91 | 0.63–1.33 | 0.666 |
| - Other indications | |||||
| - Hyponatremia | 9 (22.5) | 9 (6.87) | 2.22 | 1.16–4.23 | 0.015 |
| - Hypoglycemia | 2 (5.00) | 12 (9.16) | 0.57 | 0.14–2.30 | 0.431 |
| Cushingoid appearance in exogenous steroid use | 51 (39.8) | 15 (3.86) | 4.52 | 3.17–6.44 | <0.001 |
| Dose of glucocorticoids equivalent to prednisolone, n (%) | |||||
| - Unknown | 28 (47.46) | 30 (41.10) | (Ref) | ||
| - 0.5–5.0 mg | 23 (38.98) | 32 (43.84) | 1.9 | 1.21–3.00 | 0.005 |
| - >5.0–20 mg | 7 (11.86) | 9 (12.33) | 1.99 | 0.92–4.30 | 0.077 |
| - >20 mg | 1 (1.69) | 2 (2.74) | 1.52 | 0.21–10.91 | 0.076 |
| Type of steroid use, n (%) | |||||
| - Prednisolone | 18 (47.37) | 25 (54.35) | 1.58 | 0.93–2.65 | 0.085 |
| - Dexamethasone | 3 (11.54) | 2 (7.14) | 2.23 | 0.70–7.10 | 0.172 |
| - Triamcinolone | 1 (1.69) | 5 (6.85) | 0.67 | 0.09–4.79 | 0.691 |
| - Traditional medicine or herbal use | 36 (76.60) | 41 (82.00) | 1.87 | 1.23–2.83 | 0.003 |
| History of pituitary surgery, n (%) | |||||
| - Microadenoma | 3 (15.79) | 9 (10.47) | (Ref) | ||
| - Macroadenoma | 16 (84.21) | 77 (89.53) | 1.09 | 0.45–2.64 | 0.832 |
| Other hormonal deficiencies, n (%) | |||||
| - Gonadotropin | 10 (41.67) | 45 (55.56) | 0.61 | 0.31–1.18 | 0.148 |
| - Thyroid | 26 (96.30) | 1 (3.70) | 0.92 | 0.58–1.47 | 0.746 |
| - Growth hormone | 4 (20.00) | 12 (20.34) | 0.82 | 0.30–2.26 | 0.714 |
| - Diabetes insipidus | 5 (27.78) | 29 (42.03) | 0.5 | 0.20–1.24 | 0.139 |
| Characteristic | Adrenal Insufficiency | No Adrenal Insufficiency | RR * | 95% CI * | p-Value |
|---|---|---|---|---|---|
| (n = 128) | (n = 389) | ||||
| Serum morning cortisol (mean ± SD) (µg/dL) | 7.75 ± 2.78 | 9.55 ± 3.31 | <0.001 | ||
| <9 µg/dL, n (%) | 84 (65.53) | 188 (48.33) | (Ref) | ||
| ≥9 µg/dL, n (%) | 44 (34.38) | 201 (51.67) | 1.71 | 1.19–2.47 | 0.004 |
| Serum basal cortisol (mean ±SD) (µg/dL) | 6.15 ± 3.14 | 10.80 ± 0.26 | <0.001 | ||
| <9 µg/dL, n (%) | 104 (81.25) | 165 (42.42) | (Ref) | ||
| ≥9 µg/dL, n (%) | 24 (18.75) | 224 (57.58) | 0.25 | 0.16–0.39 | <0.001 |
| Serum potassium (mean ± SD) (mEq/L) | 3.98 ± 0.58 | 4.05 ± 0.47 | 0.188 | ||
| <3 mEq/L, n (%) | 2 (1.56) | 4 (1.03) | (Ref) | ||
| ≥3 mEq/L, n (%) | 126 (98.44) | 385 (98.97) | 0.99 | 0.83–1.18 | 0.99 |
| Serum sodium (mean ± SD) (mEq/L) | 138.51 ± 5.54 | 138.17 ± 12.45 | 0.761 | ||
| <135 mEq/L, n (%) | 20 (15.63) | 55 (14.14) | (Ref) | ||
| ≥135 mEq/L, n (%) | 108 (84.38) | 334 (85.86) | 0.91 | 0.56–1.47 | 0.72 |
| Eosinophilia, n (%) | 11 (10.58) | 93 (89.42) | 0.91 | 0.48–1.70 | 0.768 |
| Lymphocytosis, n (%) | 66 (63.46) | 223 (75.08) | 0.83 | 0.59–1.18 | 0.324 |
| Serum albumin (mean ± SD) (g/dL) | 3.73 ± 0.72 | 3.97 ± 0.55 | <0.001 | ||
| <3 g/dL | 20 (15.63) | 108 (84.38) | (Ref) | ||
| ≥3 g/dL | 17 (4.37) | 372 (95.63) | 0.41 | 0.25–0.67 | <0.001 |
| Total cholesterol (mean ± SD) (mg/dL) | 177.86 ± 51.17 | 183.75 ± 50.37 | 0.252 | ||
| <150 mg/dL | 39 (30.47) | 81 (20.82) | (Ref) | ||
| ≥150 mg/dL | 81 (20.82) | 308 (19.18) | 0.68 | 0.47–1.00 | 0.053 |
| Factor | RR | 95% CI | p-Value |
|---|---|---|---|
| Chronic kidney disease | 2.52 | 2.02–3.14 | <0.001 |
| Cushingoid appearance in exogenous steroid and/or herbal medicine use | 3.44 | 2.16–5.47 | <0.001 |
| Nausea and/or vomiting | 1.84 | 1.24–2.75 | 0.003 |
| Fatigue | 1.23 | 1.11–1.37 | <0.001 |
| Serum basal cortisol < 9 µg/dL | 3.36 | 3.23–3.49 | <0.001 |
| Cholesterol < 150 mg/dL | 1.26 | 1.20–1.32 | <0.001 |
| Serum sodium < 135 mEq/L | 1.09 | 1.04–1.15 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manosroi, W.; Phimphilai, M.; Khorana, J.; Atthakomol, P.; Pipanmekaporn, T. Predictive Factors of Adrenal Insufficiency in Outpatients with Indeterminate Serum Cortisol Levels: A Retrospective Study. Medicina 2020, 56, 23. https://doi.org/10.3390/medicina56010023
Manosroi W, Phimphilai M, Khorana J, Atthakomol P, Pipanmekaporn T. Predictive Factors of Adrenal Insufficiency in Outpatients with Indeterminate Serum Cortisol Levels: A Retrospective Study. Medicina. 2020; 56(1):23. https://doi.org/10.3390/medicina56010023
Chicago/Turabian StyleManosroi, Worapaka, Mattabhorn Phimphilai, Jiraporn Khorana, Pichitchai Atthakomol, and Tanyong Pipanmekaporn. 2020. "Predictive Factors of Adrenal Insufficiency in Outpatients with Indeterminate Serum Cortisol Levels: A Retrospective Study" Medicina 56, no. 1: 23. https://doi.org/10.3390/medicina56010023
APA StyleManosroi, W., Phimphilai, M., Khorana, J., Atthakomol, P., & Pipanmekaporn, T. (2020). Predictive Factors of Adrenal Insufficiency in Outpatients with Indeterminate Serum Cortisol Levels: A Retrospective Study. Medicina, 56(1), 23. https://doi.org/10.3390/medicina56010023