Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies


Abstract
:1. Introduction
2. Methods
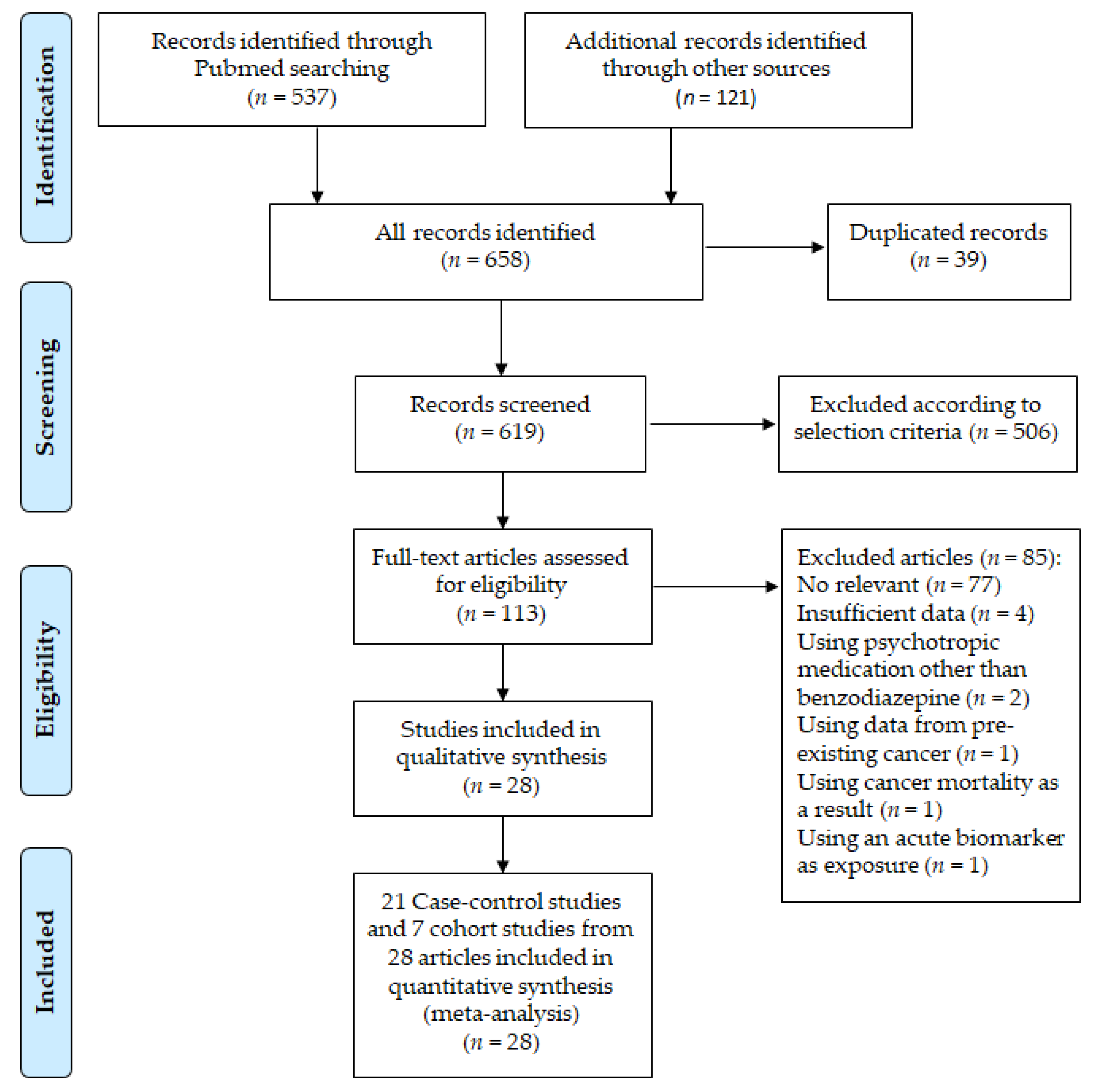
2.1. Literature Search Strategy
2.2. Selection Relevant Studies and Criteria
2.3. Data Extraction
2.4. Risk of Bias of Included Studies
2.5. Statistical Analyses
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
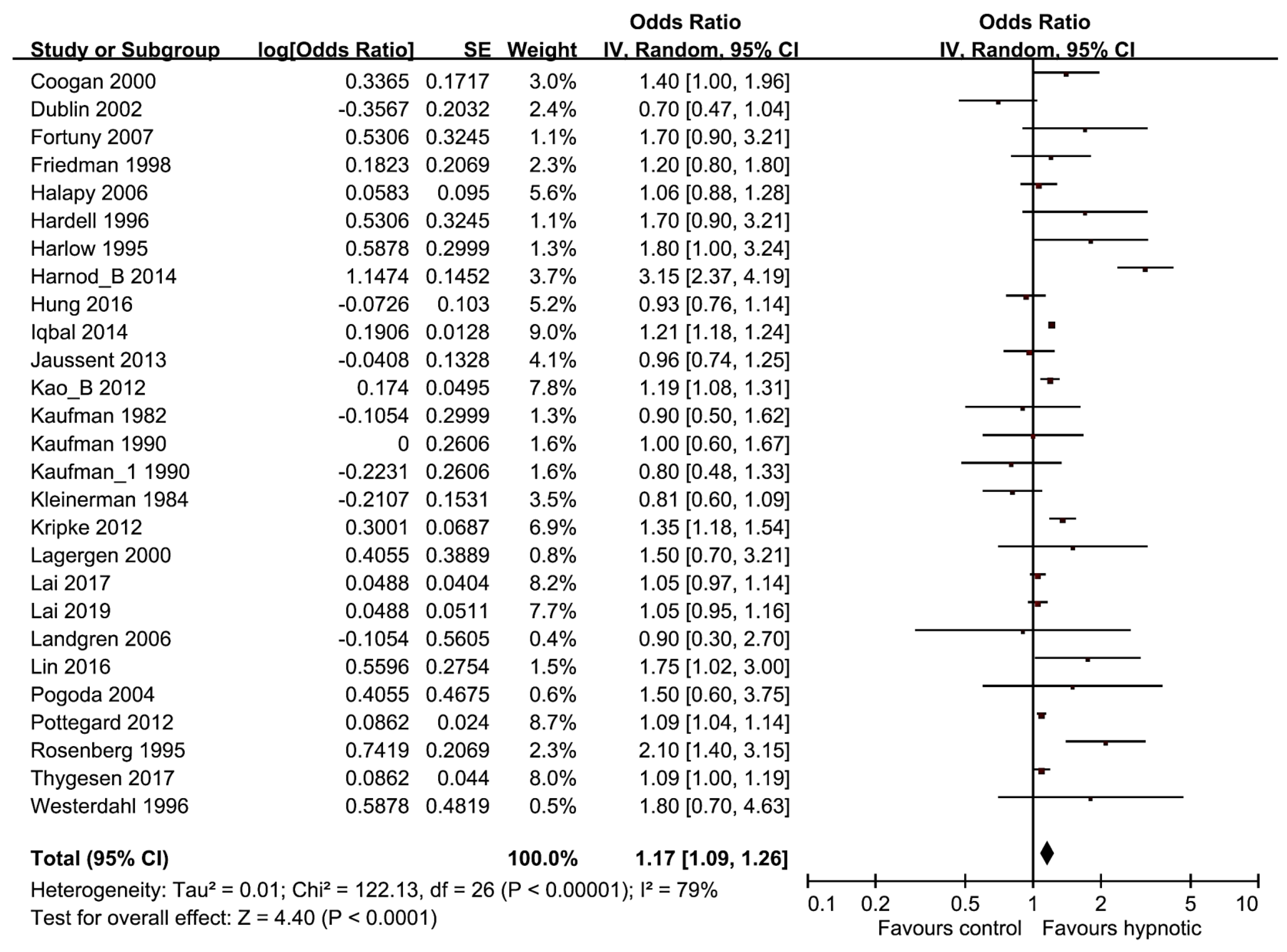
3.3. Meta-Analysis and Subgroup Analysis
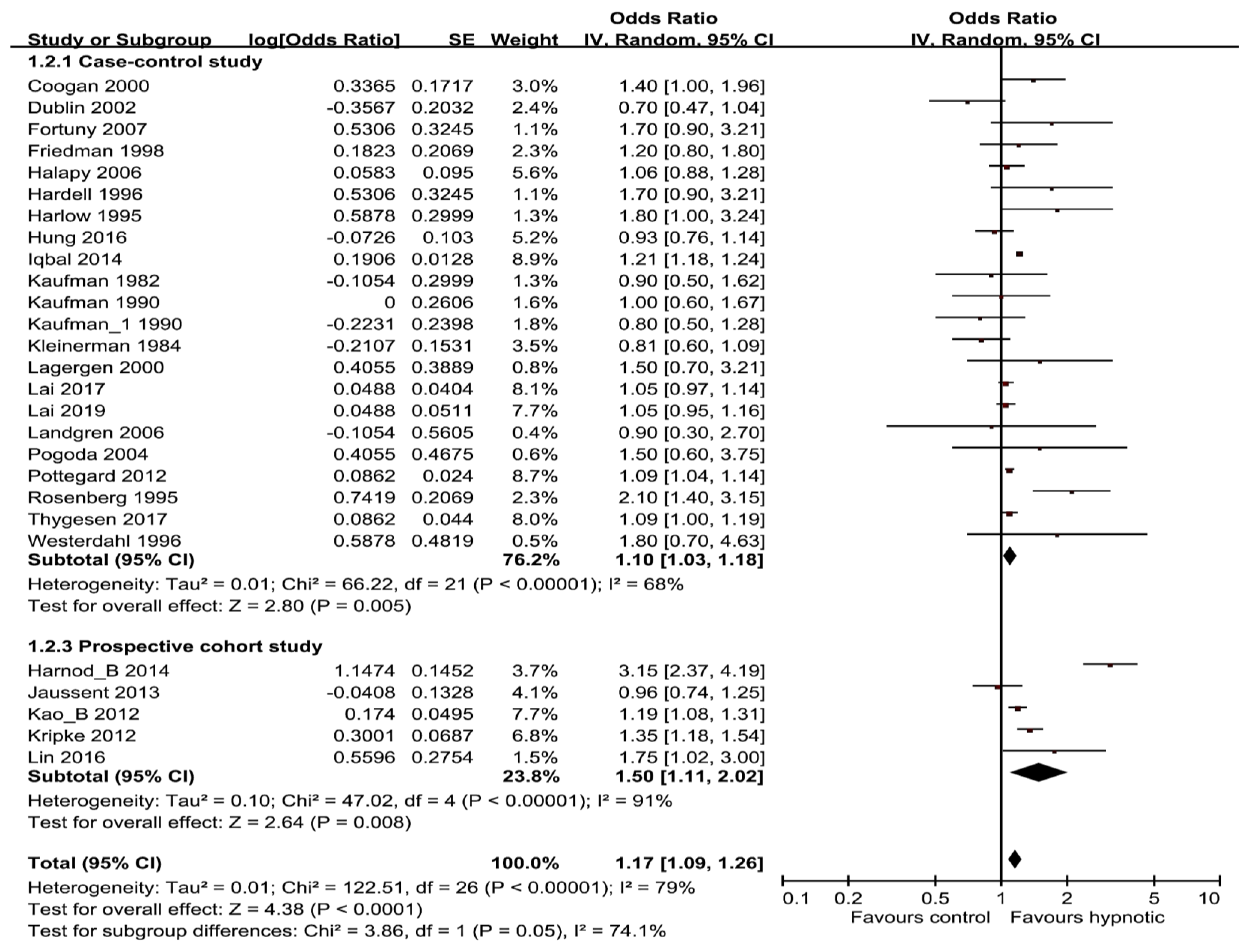
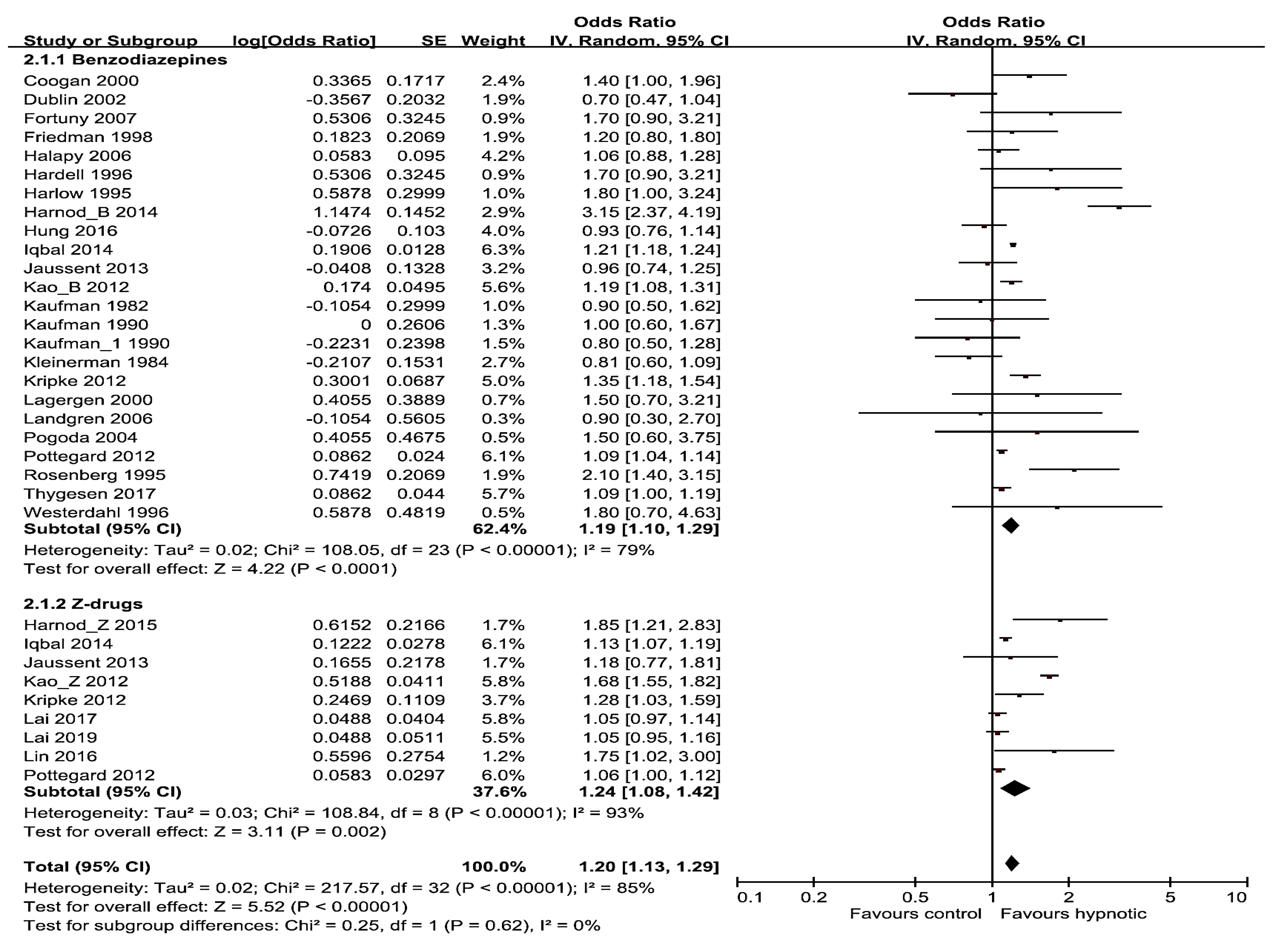
3.4. Subgroup Meta-Analyses by Different Factors
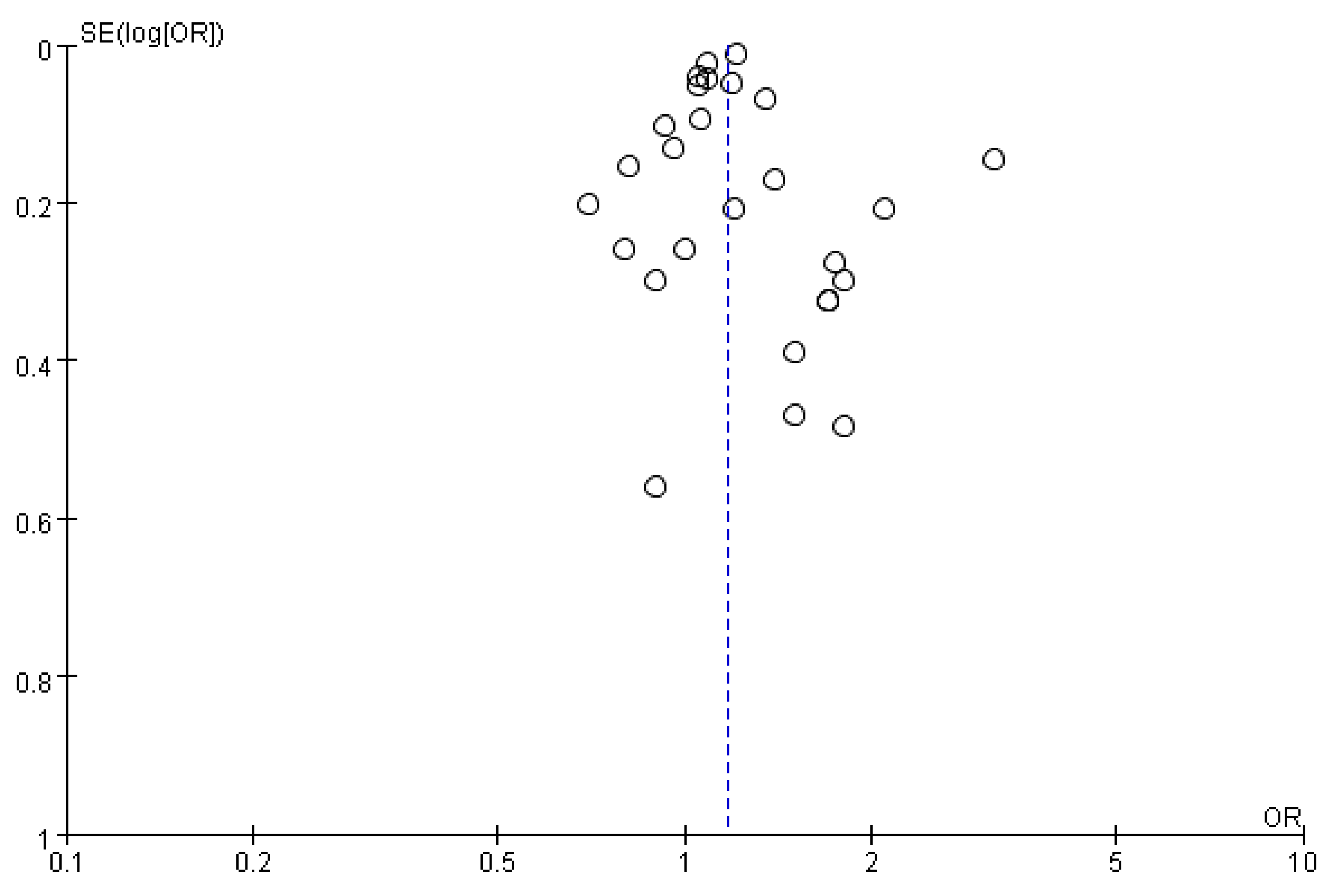
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Deoras, K.; Moul, D. Hypnotics. In Encyclopedia of the Neurological Sciences, 2nd ed.; Academic Press: Cambridge, MA, USA, 2014; pp. 646–649. [Google Scholar]
- Zhang, T.; Yang, X.; Zhou, J.; Liu, P.; Wang, H.; Li, A.; Zhou, Y. Benzodiazepine drug use and cancer risk: A dose-response meta analysis of prospective cohort studies. Oncotarget 2017, 8, 102381–102391. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. National Institutes of Health State of the Science Conference statement on Manifestations and Management of Chronic Insomnia in Adults. Sleep 2005, 28, 1049. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, N.; Vandermeer, B.; Friesen, C.; Bialy, L.; Tubman, M.; Ospina, M.; Klassen, T.P.; Witmans, M. The efficacy and safety of drug treatments for chronic insomnia in adults: A meta-analysis of RCTs. J. Gen Intern Med. 2007, 22, 1335. [Google Scholar] [CrossRef]
- Holbrook, A.M.; Crowther, R.; Lotter, A.; Cheng, C.; King, D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000, 162, 225. [Google Scholar]
- Nowell, P.D.; Mazumdar, S.; Buysse, D.J.; Dew, M.A.; Reynolds, C.F.; Kupfer, D.J. Benzodiazepines and zolpidem for chronic insomnia: A meta-analysis of treatment efficacy. JAMA 1997, 278, 2170. [Google Scholar] [CrossRef]
- Kunert-Radek, J.; Stepien, H.; Pawlikowski, M. Inhibition of rat pituitary tumor cell proliferation by benzodiazepines in vitro. Neuroendocrinology 1994, 59, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.; Deeks, J.J.; Altman, D.G. Special Topics in Statistics. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Book Series; Wiley & Sons: London, UK, 2008; pp. 48–529. [Google Scholar]
- Kaufman, D.W.; Shapiro, S.; Slone, D.; Rosenberg, L.; Helmrich, S.P.; Miettinen, O.S.; Stolley, P.D.; Levy, M.; Schottenfeld, D. Diazepam and the risk of breast cancer. Lancet 1982, 6, 537–539. [Google Scholar] [CrossRef]
- Kleinerman, R.A.; Brinton, L.A.; Hoover, R.; Fraumeni, J.F. Diazepam use and progression of breast cancer. Cancer Res. 1984, 44, 1223–1225. [Google Scholar]
- Kaufman, D.W.; Werler, M.M.; Palmer, J.R.; Rosenberg, L.; Stolley, P.D.; Shapiro, S.; Warshauer, M.E.; Clarke, E.A.; Miller, D.R. Diazepam use in relation to breast cancer: Results from two case-control studies. Am. J. Epidemiol. 1990, 131, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Harlow, B.L.; Cramer, D.W. Self-reported use of antidepressants or benzodiazepine tranquilizers and risk of epithelial ovarian cancer: Evidence from two combined case-control studies (Massachusetts, United States). Cancer Causes Control 1995, 6, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; Palmer, J.R.; Zauber, A.G.; Warshauer, M.A.; Strom, B.L.; Hariap, S.; Shapiro, S. Relation of benzodiazepine use to the risk of selected cancers: Breast, large bowel, malignant melanoma, lung, endometrium, ovary, non-Hodgkin’s lymphoma, testis, Hodgkin’s disease, thyroid, and liver. Am. J. Epidemiol. 1995, 141, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Hardell, L.; Fredrikson, M.; Axelson, O. Case-control study on colon cancer regarding previous diseases and drug intake. Int. J. Oncol. 1996, 8, 439–444. [Google Scholar] [CrossRef]
- Westerdahl, J.; Olsson, H.; Måskback, A.; Ingvar, C.; Jonsson, N. Risk of malignant melanoma in relation to drug intake, alcohol, smoking and hormonal factors. Br. J. Cancer 1996, 73, 1126–1131. [Google Scholar] [CrossRef]
- Friedman, G.D.; Coates, A.O.; Potter, J.D.; Slattery, M.L. Drugs and colon cancer. Pharmacoepidemiol. Drug Saf. 1998, 7, 99–106. [Google Scholar] [CrossRef]
- Coogan, P.F.; Rosenberg, L.; Palmer, J.R.; Strom, B.L.; Stolley, P.D.; Zauber, A.G.; Shapiro, S. Risk of ovarian cancer according to use of antidepressants, phenothiazines, and benzodiazepines (United States). Cancer Causes Control 2000, 11, 839–845. [Google Scholar] [CrossRef]
- Lagergren, J.; Bergstrom, R.; Adami, H.O.; Nyrén, O. Association between medications that relax the lower esophageal sphincter and risk for esophageal adenocarcinoma. Ann. Intern. Med. 2000, 133, 165–175. [Google Scholar] [CrossRef]
- Dublin, S.; Rossing, M.A.; Heckbert, S.R.; Goff, B.A.; Weiss, N.S. Risk of epithelial ovarian cancer in relation to use of antidepressants, benzodiazepines, and other centrally acting medications. Cancer Causes Control 2002, 13, 35–45. [Google Scholar] [CrossRef]
- Pogoda, J.M.; Katz, J.; McKean-Cowdin, R.; Nichols, P.W.; Ross, R.K.; Preston-Martin, S. Prescription drug use and risk of acute myeloid leukemia by French-American-British subtype: Results from a Los Angeles County case-control study. Int. J. Cancer 2005, 114, 634–638. [Google Scholar] [CrossRef]
- Halapy, E.; Kreiger, N.; Cotterchio, M.; Sloan, M. Benzodiazepines and risk for breast cancer. Ann. Epidemiol. 2006, 16, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Zhang, Y.; Zahm, S.H.; Inskip, P.; Zheng, T.; Baris, D. Risk of multiple myeloma following medication use and medical conditions: A case-control study in Connecticut women. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2342–2347. [Google Scholar] [CrossRef] [PubMed]
- Fortuny, J.; Johnson, C.C.; Bohlke, K.; Chow, W.-H.; Hart, G.; Kucera, G.; Mujumdar, U.; Ownby, D.; Wells, K.; Engel, L.S.; et al. Use of anti-inflammatory drugs and lower esophageal sphincter-relaxing drugs and risk of esophageal and gastric cancers. Clin. Gastroenterol. Hepatol. 2007, 5, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Kripke, D.F.; Langer, R.D.; Kline, L.E. Hypnotics’ association with mortality or cancer: A matched cohort study. BMJ Open 2012, 2, e000850. [Google Scholar] [CrossRef]
- Kao, C.H.; Sun, L.M.; Su, K.P.; Chang, S.N.; Sung, F.C.; Muo, C.H.; Liang, J.A. Benzodiazepine use possibly increases cancer risk: A population-based retrospective cohort study in Taiwan. J. Clin. Psychiatr. 2012, 73, e555–e560. [Google Scholar] [CrossRef]
- Kao, C.H.; Sun, L.M.; Liang, J.A.; Chang, S.N.; Sung, F.C.; Muo, C.H. Relationship of zolpidem and cancer risk: A Taiwanese population-based cohort study. Mayo Clin. Proc. 2012, 87, 430–436. [Google Scholar] [CrossRef]
- Pottegård, A.; Friis, S.; Andersen, M.; Hallas, J. Use of benzodiazepines or benzodiazepine related drugs and the risk of cancer: A population-based case control study. Br. J. Clin. Pharmacol. 2013, 75, 1356–1364. [Google Scholar] [CrossRef]
- Jaussent, I.; Ancelin, M.L.; Berr, C.; Pérès, K.; Scali, J.; Besset, A.; Ritchie, K.; Dauvilliers, Y. Hypnotics and mortality in an elderly general population: A 12-year prospective study. BMC Med. 2013, 11, 212. [Google Scholar] [CrossRef]
- Harnod, T.; Lin, C.L.; Sung, F.C.; Kao, C.H. An association between benzodiazepine use and occurrence of benign brain tumors. J. Neurol. Sci. 2014, 336, 8–12. [Google Scholar] [CrossRef]
- Harnod, T.; Li, Y.F.; Lin, C.L.; Chang, S.N.; Sung, F.C.; Kao, C.H. Higher-dose uses of zolpidem will increase the subsequent risk of developing benign brain tumors. J. Neuropsychiatr. Clin. Neurosci. 2015, 27, e107–e111. [Google Scholar] [CrossRef]
- Iqbal, U.; Nguyen, P.A.; Syed-Abdul, S.; Yang, H.-S.; Huang, C.-H.; Jian, W.-E.; Hsu, M.-I.; Yen, Y.; Li, Y.-C. Is longterm use of benzodiazepine a risk for cancer? Medicine 2015, 94, e483. [Google Scholar] [CrossRef] [PubMed]
- Hung, D.Z.; Lin, C.L.; Li, Y.W. Association between antiepileptic drugs and hepatocellular carcinoma in patients with epilepsy: A population-based case-control study. Brain Behav. 2016, 6, e00554. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Su, Y.C.; Huang, Y.S.; Lee, C.C. Zolpidem increased cancer risk in patients with sleep disorder: A 3-year follow-up study. J. Med. Sci. 2016, 36, 68–74. [Google Scholar]
- Lai, S.W.; Lin, C.L.; Liao, K.F. Zolpidem administration and risk of hepatocellular carcinoma: A case-control study in Taiwan. Front. Pharmacol. 2017, 8, 767. [Google Scholar] [CrossRef]
- Thygesen, L.C.; Pottegård, A.; Ersbøll, A.K.; Friis, S.; Stürmer, T.; Hallas, J. External adjustment of unmeasured confounders in a case-control study of benzodiazepine use and cancer risk. Br. J. Clin. Pharmacol. 2017, 83, 2517–2527. [Google Scholar] [CrossRef]
- Lai, S.W.; Lin, C.L.; Liao, K.F. Association between colorectal cancer and zolpidem use in a case-control study. Medicine 2019, 98, e18127. [Google Scholar] [CrossRef]
- Brandt, J.; Leong, C. Benzodiazepines and Z-drugs: An updated review of major adverse outcomes reported on in epidemiologic research. Drugs R D. 2017, 17, 493–507. [Google Scholar] [CrossRef]
- Brambilla, G.; Carrozzino, R.; Martelli, A. Genotoxicity and carcinogenicity studies of benzodiazepines. Pharmacol. Res. 2007, 56, 443–458. [Google Scholar] [CrossRef]
- Massoco, C.; Palermo-Neto, J. Effects of midazolam on equine innate immune response: A flow cytometric study. Vet. Immunol. Immunopathol. 2003, 95, 11–19. [Google Scholar] [CrossRef]
- Massoco, C.O.; Palermo-Neto, J. Diazepam effects of peritoneal macrophage activity and corticosterone serum levels in Balb/C mice. Life Sci. 1999, 65, 2157–2165. [Google Scholar] [CrossRef]
- Torres, S.R.; Frode, T.S.; Nardi, G.M.; Vita, N.; Reeb, R.; Ferrara, P.; Farges, R.C.; Ribeiro-do-Valle, R.M. Anti-inflammatory effects of peripheral benzodiazepine receptor ligands in two mouse models of inflammation. Eur. J. Pharmacol. 2000, 408, 199–211. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, H.B.; Kim, Y.H.; Kim, J.Y. Use of Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Korean J. Fam. Med. 2018, 39, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Enna, S.J. Role of gamma-aminobutyric acid in anxiety. Psychopathology 1984, 17, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Jezewska, E.; Scinska, A.; Kukwa, W.; Sobolewska, A.; Turzynska, D.; Samochowiec, J.; Bienkowski, P. Gamma-aminobutyric acid concentrations in benign parotid tumours and unstimulated parotid saliva. J. Laryngol. Otol. 2011, 125, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.B.; Myung, S.K.; Park, Y.C.; Park, B. Use of benzodiazepine and risk of cancer: A meta-analysis of observational studies. Int. J. Cancer 2017, 140, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.B. The Environment and Disease: Association or Causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef]
- Schutte-Rodin, S.; Broch, L.; Buysse, D.; Dorsey, C.; Sateya, M. Clinical guideline for the evaluation and chronic management of chronic insomnia in adults. J. Clin. Sleep Med. 2008, 4, 487–504. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Caulet, M.; Priest, R.G.; Guilleminault, C. Psychotropic medication consumption patterns in the UK general population. J. Clin. Epidemiol. 1998, 51, 273–283. [Google Scholar] [CrossRef]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46, S7–S15. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case-Control Studies (n= 21) | Selection | Comparability Control for Important Factor or Additional Factor | Exposure | Total | |||||
| Adequate Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Ascertainment of Exposure | Same Method of Ascertainment for Participants | Nonresponse Rate | |||
| Kaufman (1982) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 |
| Kleinerman (1984) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Kaufman (1990) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Harlow (1995) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Rosenberg (1995) | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Hardell (1996) | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 5 |
| Westerdahl (1996) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Friedman (1998) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Coogan (2000) | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 |
| Lagergen (2000) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Dublin (2002) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Pogoda (2004) | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Halapy (2006) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Landgren (2006) | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Fortuny (2007) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| Pottegard (2012) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Iqbal (2014) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Hung (2016) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Lai (2017) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Thygesen (2017) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Lai (2019) | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Cohort Studies (n= 7) | Selection | Comparability Control for Important Factor or Additional Factor | Outcome | Total | |||||
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest Was Not Present at Start of Study | Assessment of Outcome | Follow-up Long Enough for Outcomes to Occur | Adequacy of Follow-up of Cohorts | |||
| Kripke (2012) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Kao_B (2012) | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 6 |
| Jaussent (2013) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Harnod_B (2014) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Kao_Z (2012) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Harnod (2015) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Lin (2016) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Author (year) | Study type | Country | Years Enrolled | Population (Hypnotic /Control) | Cancer Type | Definition of Hypnotic use | OR/RR (95% CI) |
|---|---|---|---|---|---|---|---|
| Kaufman (1982) [11] | Case-control | Canada, United States and Israel | 1976–1980 | 1236/728 | Breast | Diazepam ≥ 6 month vs. never-use | 0.9 (0.5–1.6) |
| Kleinerman (1984) [12] | Case-control | United States | 1973–1977 | 1075/1146 | Breast | Diazepam ≥ 6 month vs. never-use | 0.81 (0.6–1.1) |
| Kaufman (1990) [13] | Case-control | United States | 1981–1987 | 3078/1931 | Breast | Diazepam ≥ 6 month vs. never-use | 1.0 (0.6–1.7) |
| Kaufman_1 (1990) [13] | Case-control | Canada | 1982–1986 | 607/1214 | Breast | Diazepam ≥ 6 month vs. never-use | 0.8 (0.5–1.3) |
| Harlow (1995) [14] | Case-control | United States | 1978–1987 | 450/454 | Ovarian | Benzodiazepine vs. never-use | 1.8 (1.0–3.1) |
| Rosenberg (1995) [15] | Case-control | United States | 1977–1991 | 382/5695 | Non-Hodgkin’s lymphoma | Benzodiazepine ≥ 1 month vs. never- use | 2.1 (1.4–3.3) |
| Hardell (1996) [16] | Case-control | Sweden | 1984–1986 | 329/658 | Colon | Benzodiazepine vs. never-use | 1.7 (0.9-3.3) |
| Westerdahl (1996) [17] | Case-control | Sweden | 1988–1990 | 400/640 | Malignant melanoma | Benzodiazepine vs. never-use | 1.8 (0.7–4.4) |
| Friedman (1998) [18] | Case-control | United States | 1991–1994 | 1993/2410 | Colon | Diazepam ≥ 12 month vs. never-use | 1.2 (0.8–1.8) |
| Coogan (2000) [19] | Case-control | United States | 1976–1998 | 748/2992 | Ovarian | Benzodiazepine < 12 month vs. never-use | 1.4 (1.0–2.1) |
| Lagergen (2000) [20] | Case-control | Sweden | 1995–1997 | 189/820 | Esophageal | Benzodiazepine vs. never-use | 1.5 (0.7–2.9) |
| Dublin (2002) [21] | Case-control | United States | 1981–1997 | 314/790 | Ovarian | Benzodiazepine < 6 month vs. never-use | 0.70 (0.47–1.0) |
| Pogoda (2004) [22] | Case-control | United States | 1987–1994 | 412/412 | Acute myeloid leukemia | Benzodiazepine ≥ 6 month vs. never-use | 1.5 (0.6–3.7) |
| Halapy (2006) [23] | Case-control | Canada | 1996–1998 | 3133/3062 | Breast | Benzodiazepine vs. never-use | 1.06 (0.88–1.27) |
| Landgren (2006) [24] | Case-control | United States | 1997–2002 | 179/691 | Multiple myeloma | Benzodiazepine ≥ 6 month vs. never-use | 0.9 (0.3–2.6) |
| Fortuny (2007) [25] | Case-control | United States | 1980–2002 | 114/3996 | Esophageal | Benzodiazepine vs. never-use | 1.7 (0.9–3.1) |
| Kripke (2012) [26] | Prospective cohort | United States | 2002–2007 | 2076 cases among 25,750 | All cancers | Any hypnotic > 132 pill/year vs. non-users | 1.35 (1.18–1.55) |
| Kao_B (2012) [27] | Prospective cohort | Taiwan | 1996–2000 | 3520 cases among 119,239 | All cancers | Benzodiazepine ≥ 2 month vs. non-users | 1.19 (1.08–1.32) |
| Kao_Z (2012) [28] | Prospective cohort | Taiwan | 1998–2000 | 1047/2924 | All cancers | Zolpidem vs. never-use | 1.68 (1.55–1.82) |
| Pottegard (2012) [29] | Case-control | Denmark | 2002–2009 | 149360/1194729 | All cancers | All benzodiazepine any related drugs (cumulative amount ≥ 500 defined daily dose) vs. never use | 1.09 (1.04–1.14) |
| Jaussent (2013) [30] | Prospective cohort | France | 1999–2011 | 1454 cases among 6696 | All cancers | Hypnotic vs. never-use | 0.96 (0.74–1.23) |
| Harnod_B (2014) [31] | Prospective cohort | Taiwan | 2000–2009 | 274 cases among 62,050 | Brain cancer | Benzodiazepine ≥ 2 month vs. never-use | 3.15 (2.37–4.20) |
| Harnod_Z (2015) [32] | Prospective cohort | Taiwan | 2000–2009 | 37810/37810 | Brain cancer | Zolpidem ≥ 520 mg/year vs. never-use | 1.85 (1.21–2.82) |
| Iqbal (2014) [33] | Case-control | Taiwan | 1998–2009 | 42500/255000 | All cancers | Benzodiazepine ≥ 2 month vs. never-use | 1.21 (1.18–1.24) |
| Hung (2016) [34] | Case-control | Taiwan | 2006–2011 | 1454/1448 | Hepatocellular carcinoma | Clonazepam vs. never-use | 0.93 (0.76–1.13) |
| Lin (2016) [35] | Prospective cohort | Taiwan | 2002–2004 | 1728 cases among 6924 | All cancers | Zolpidem vs. never-use | 1.75 (1.02–3.0) |
| Lai (2017) [36] | Case-control | Taiwan | 2011–2012 | 77986/77986 | Hepatocellular carcinoma | Benzodiazepine vs. never-use | 1.5 (1.45–2.44) |
| Thygesen (2017) [37] | Case-control | Danish | 2002–2009 | 1854/4950 | All cancers | Benzodiazepine > 500 DDD (1–5 years) vs. never-use | 1.09 (1.00–1.19) |
| Lai (2019) [38] | Case-control | Taiwan | 2000–2013 | 4912/4912 | Colorectal | Zolpidem vs. never-use | 1.05 (0.95–1.15) |
| Factors | Study Number | Summary OR or RR (95% CI) | Heterogeneity I2 (%) | Random/Fixed Effects |
|---|---|---|---|---|
| All | 27 | 1.17 (1.09–1.26) | 79% | Random |
| Region | ||||
| America | 14 | 1.15 (0.95–1.36) | 62% | Random |
| Europe | 6 | 1.09 (1.05–1.14) | 0% | Random |
| Asia | 7 | 1.24 (1.09–1.42) | 91% | Random |
| Type of cancer | ||||
| Brain cancer | 5 | 1.93 (1.29–2.88) | 82% | Random |
| Malignant melanoma | 4 | 1.01 (0.78–1.31) | 0% | Fixed |
| Esophagus cancer | 6 | 1.56 (1.32–1.84) | 0% | Fixed |
| Breast cancer | 10 | 1.08 (0.96–1.22) | 61% | Random |
| Liver cancer | 7 | 1.38 (1.17–1.63) | 89% | Random |
| Lung cancer | 5 | 1.24 (1.04–1.48) | 80% | Random |
| Stomach cancer | 3 | 1.18 (1.05–1.34) | 4% | Fixed |
| Pancreatic cancer | 2 | 1.38 (1.20–1.58) | 0% | Fixed |
| Colon cancer | 7 | 1.11 (1.01–1.23) | 59% | Random |
| Ovarian cancer | 7 | 1.07 (0.86–1.33) | 50% | Random |
| Renal cancer | 4 | 1.51 (1.18–1.94) | 60% | Random |
| Prostate cancer | 4 | 1.29 (1.07–1.55) | 70% | Random |
| Gender | ||||
| Female | 9 | 1.01 (0.89–1.14) | 42% | Fixed |
| Male and Female | 19 | 1.22 (1.13–1.32) | 83% | Random |
| Elderly ≥ 65 | 4 | 1.16 (0.92–1.47) | 84% | Random |
| Anxiolytics/ Sedatives | ||||
| Anxiolytics benzodiazepines | 9 | 1.09 (0.95–1.26) | 30% | Random |
| Sedatives benzodiazepines and Z-drugs | 10 | 1.26 (1.10–1.45) | 93% | Random |
| Duration of hypnotics use | ||||
| <6 months | 12 | 1.03 (1.02–1.04) | 35% | Fixed |
| ≥6 months | 13 | 1.05 (1.02–1.08) | 0% | Fixed |
| ≥5 years | 9 | 1.11 (1.02–1.21) | 0% | Fixed |
| Cumulative yearly dose | ||||
| Lower | 5 | 1.03 (1.01–1.05) | 10% | Fixed |
| Moderate | 6 | 1.30 (0.97–1.75) | 95% | Random |
| Highest | 6 | 2.03 (1.19–3.46) | 97% | Random |
| Type of hypnotics | ||||
| Long-acting (Diazepam) | 8 | 0.97 (0.93–1.01) | 37% | Fixed |
| Intermediate-acting | 4 | 1.21 (0.93–1.57) | 88% | Random |
| Short-acting | 9 | 1.29 (1.12–1.48) | 92% | Random |
| Methodological quality | ||||
| High quality | 19 | 1.14 (1.04–1.25) | 92% | Random |
| Low quality | 10 | 1.59 (1.27–1.98) | 85% | Random |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, T.-R.; Yang, L.-J.; Wu, T.-W.; Chao, Y.-C. Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Medicina 2020, 56, 513. https://doi.org/10.3390/medicina56100513
Peng T-R, Yang L-J, Wu T-W, Chao Y-C. Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Medicina. 2020; 56(10):513. https://doi.org/10.3390/medicina56100513
Chicago/Turabian StylePeng, Tzu-Rong, Li-Jou Yang, Ta-Wei Wu, and You-Chen Chao. 2020. "Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies" Medicina 56, no. 10: 513. https://doi.org/10.3390/medicina56100513
APA StylePeng, T. -R., Yang, L. -J., Wu, T. -W., & Chao, Y. -C. (2020). Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Medicina, 56(10), 513. https://doi.org/10.3390/medicina56100513