Complement Activation on Endothelial Cell-Derived Microparticles—A Key Determinant for Cardiovascular Risk in Patients with Systemic Lupus Erythematosus?


{kind=link}
Abstract
:1. Background
2. Gap in Knowledge
3. Endothelial-Derived Microparticles as Markers of Disease Activity in SLE
4. Hypothesis Driven Outlook
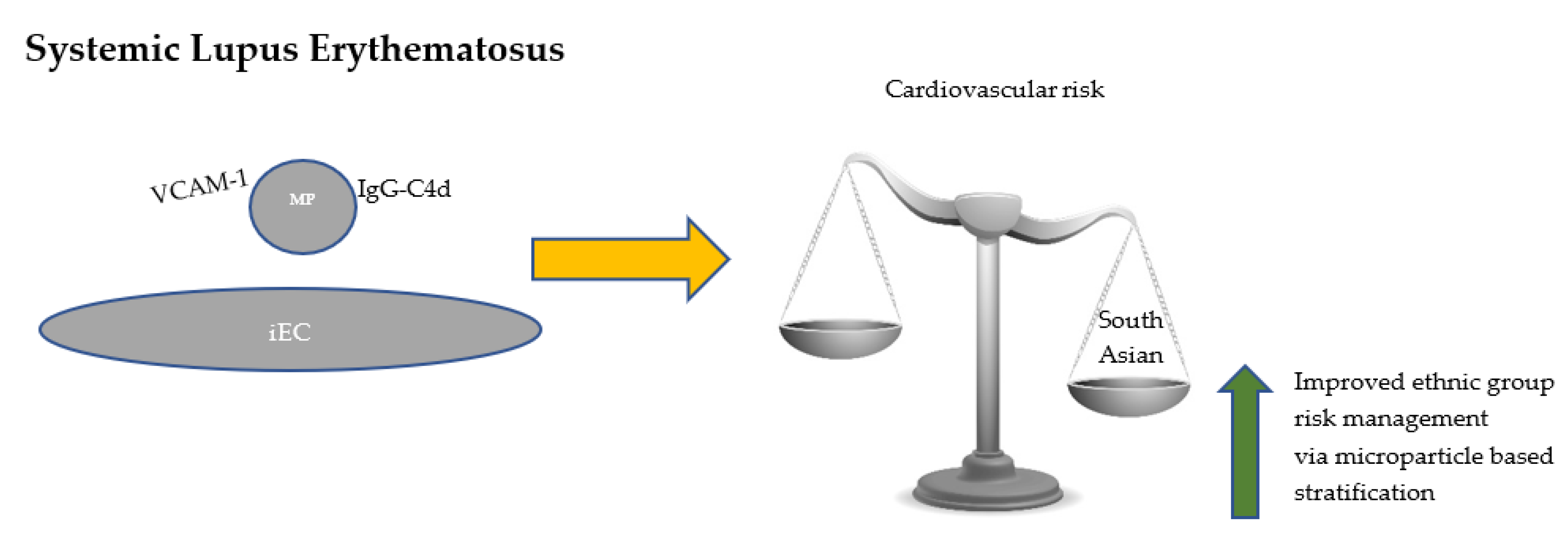
5. A Necessary Focus on Patients with SLE Who Are of South Asian Origin
Author Contributions
Funding
Conflicts of Interest
References
- Pickering, M.C.; Walport, M.J. Links between complement abnormalities and systemic lupus erythematosus. Rheumatology 2000, 39, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batool, S.; Abbasian, N.; Burton, J.O.; Stover, C. Microparticles and their Roles in Inflammation: A Review. Open Immunol. J. 2013, 6, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Burbano, C.; Villar-Vesga, J.; Orejuela, J.; Muñoz, C.; Vanegas, A.; Vásquez, G.; Rojas, M.; Castaño, D. Potential Involvement of Platelet-Derived Microparticles and Microparticles Forming Immune Complexes during Monocyte Activation in Patients with Systemic Lupus Erythematosus. Front. Immunol. 2018, 9, 322. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.C.; Tesse, A.; Zonairi, F.; Andrianstsitohaina, R. Shed membrane microparticles from circulating and vascular cells in regulating vascular function. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Boulanger, C.M.; Dignat-George, F. Microparticles: An introduction. Arter. Thromb. Vasc. Biol. 2011, 31, 2–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cointe, S.; Judicone, C.; Robert, S.; Mooberry, M.J.; Poncelet, P.; Wauben, M.; Nieuwland, R.; Key, N.S.; Dignat-George, F.; Lacroix, R. Standardization of microparticle enumeration across different flow cytometry platforms: Results of a multicentre collaborative workshop. J. Thromb. Haemost. 2017, 15, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Mobarrez, F.; Vikerfors, A.; Gustafsson, J.T.; Gunnarsson, I.; Zickert, A.; Larsson, A.; Pisetsky, D.S.; Wallen, H.; Svenungsson, E. Microparticles in the blood of patients with systemic lupus erythematosus (SLE): Phenotypic characterization and clinical associations. Sci. Rep. 2016, 6, 36025. [Google Scholar] [CrossRef]
- Shao, W.H. The Role of Microparticles in Rheumatic Diseases and their Potentials as Therapeutic Tools. J. Mol. Immunol. 2016, 1, 101. [Google Scholar]
- Diehl, P.; Fricke, A.; Sander, L.; Stamm, J.; Bassler, N.; Htun, N.; Ziemann, M.; Helbing, T.; El-Osta, A.; Jowett, J.B.M.; et al. Microparticles: Major transport vehicles for distinct microRNAs in circulation. Cardiovasc. Res. 2012, 93, 633–644. [Google Scholar] [CrossRef]
- Mackenzie, A.; Wilson, H.L.; Kiss-Tothm, E.; Dower, S.K.; North, R.A.; Supernant, A. Rapis secretion of interleukin-1β by microvesicle shedding. Immunity 2001, 15, 825–835. [Google Scholar] [CrossRef]
- Ardoin, S.P.; Shanahan, J.C.; Pisetsky, D.S. The role of microparticles in inflammation and thrombosis. Scand. J. Immunol. 2007, 66, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Gandino, I.J.; Scolnik, M.; Bertiller, E.; Scaglioni, V.; Catoggio, L.J.; Soriano, E.R. Complement levels and risk of organ involvement in patients with systemic lupus erythematosus. Lupus Sci. Med. 2017, 4, e000209. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Ullal, A.J.; Gauley, J.; Ning, T.C. Microparticles as mediators and biomarkers of rheumatic disease. Rheumatology 2012, 51, 1737–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carreira, P.; Isenberg, D. Recent developments in biologic therapies for the treatment of patients with systemic lupus erythematosus. Rheumatology 2019, 58, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Sciatti, E.; Cavazzana, I.; Vizzardi, E.; Bonadei, I.; Fredi, M.; Taraborelli, M.; Ferizi, R.; Merta, M.; Tincani, A.; Franceschini, F. Systemic lupus erythematous and endothelial dysfunction: A close relationship. Curr. Rheumatol. Rev. 2019, 15, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Durante, A.; Bronzato, S. The increased cardiovascular risk in patients affected by autoimmune diseases: Review of the various manifestations. J. Clin. Med. Res. 2015, 7, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Hernandez, J.; Cortes, R. Extracellular Vesicles as Biomarkers of Systemic Lupus Erythematosus. Dis. Markers 2015, 2015, 613536. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, C.T.; Østergaard, O.; Stener, L.; Iversen, L.V.; Truedsson, L.; Gullstrand, B.; Jacobsen, S.; Heegaard, N.H.H. Increased IgG on cell-derived plasma microparticles in systemic lupus erythematosus is associated with autoantibodies and complement activation. Arthritis Rheum. 2012, 64, 1227–1236. [Google Scholar] [CrossRef]
- Winberg, L.K.; Nielsen, C.H.; Jacobsen, S. Surface complement C3 fragments and cellular binding of microparticles in patients with SLE. Lupus Sci. Med. 2017, 4, e000193. [Google Scholar] [CrossRef]
- Atehortúa, L.; Rojas, M.; Vásquez, G.; Muñoz-Vahos, C.H.; Vanegas-García, A.; Posada-Duque, R.A.; Castaño, D. Endothelial activation and injury by microparticles in patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Res. Ther. 2019, 21, 34. [Google Scholar] [CrossRef] [Green Version]
- Fortin, P.R.; Cloutier, N.; Bissonnette, V.; Aghdassi, E.; Eder, L.; Simonyan, D.; Laflamme, N.; Boilard, E. Distinct Subtypes of Microparticle-containing Immune Complexes Are Associated with Disease Activity, Damage, and Carotid Intima-media Thickness in Systemic Lupus Erythematosus. J. Rheumatol. 2016, 43, 2019–2025. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, E.M.; Moreno-Martinez, D.; Wilkinson, F.L.; McHugh, N.J.; Bruce, I.N.; Pauling, J.; Alexander, Y.; Parker, B. Microparticle subpopulations are potential markers of disease progression and vascular dysfunction across a spectrum of connective tissue disease. BBA Clin. 2016, 7, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, B.; Al-Husain, A.; Pemberton, P.; Yates, A.P.; Ho, P.; Gorodkin, R.; Teh, L.S.; Alexande, M.Y.; Bruce, L.N. Suppression of inflammation reduces endothelial microparticles in active systemic lupus erythematosus. Ann. Rheum. Dis. 2014, 73, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, O.; Nielsen, C.T.; Tanassi, J.T.; Iversen, L.V.; Jacobsen, S.; Heegaard, N.H.H. Distinct proteome pathology of circulating microparticles in systemic lupus erythematosus. Clin. Proteom. 2017, 14, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, J.T.; Simard, J.F.; Gunnarsson, I.; Elvin, K.; Lundberg, I.E.; Hansson, L.-O.; Larsson, A.; Svenungsson, E. Risk factors for cardiovascular mortality in patients with systemic lupus erythematosus, a prospective cohort study. Arthritis Res. Ther. 2012, 14, R46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraaij, T.; Nilsson, S.C.; van Kooten, C.; Okrój, M.; Blom, A.M.; Teng, Y.O. Measuring plasma C4D to monitor immune complexes in lupus nephritis. Lupus Sci. Med. 2019, 6, e000326. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Kaplan, M. Cardiovascular disease in systemic lupus erythematosus. An update. Curr. Opin. Rheumatol. 2018, 30, 441–448. [Google Scholar] [CrossRef]
- Felten, R.; Sagez, F.; Gavand, P.E.; Martin, T.; Korganow, A.S.; Sordet, C.; Javier, R.M.; Soulas-Sprauel, P.; Rivière, M.; Scher, F.; et al. 10 most important contemporary challenges in the management of SLE. Lupus Sci. Med. 2019, 6, e000303. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Chung, E.K.; Wu, Y.L.; Savelli, S.L.; Nagaraja, H.N.; Zhou, B.; Hebert, M.; Jones, K.N.; Shu, Y.; Kitzmiller, K.; et al. Gene copy-number variation and associated polymorphisms of complement component C4 in human systemic lupus erythematosus (SLE): Low copy number is a risk factor for and high copy number is a protective factor against SLE susceptibility in European Americans. Am. J. Hum. Genet. 2007, 80, 1037–1054. [Google Scholar] [CrossRef] [Green Version]
- Biró, E.; van den Goor, J.M.; de Mol, B.A.; Schaap, M.C.; Ko, L.Y.; Sturk, A.; Hack, C.E.; Nieuwland, R. Complement activation on the surface of cell-derived microparticles during cardiac surgery with cardiopulmonary bypass—is retransfusion of pericardial blood harmful? Perfusion 2011, 26, 21–29. [Google Scholar] [CrossRef]
- Chen, J.Y.; Wu, Y.L.; Mok, M.Y.; Wu, Y.-J.J.; Lintner, K.E.; Wang, C.-M.; Chung, E.K.; Yang, Y.; Zhou, B.; Wang, H. Effects of Complement C4 Gene Copy Number Variations, Size Dichotomy, and C4A Deficiency on Genetic Risk and Clinical Presentation of Systemic Lupus Erythematosus in East Asian Populations. Arthritis Rheumatol. 2016, 68, 1442–1453. [Google Scholar] [CrossRef] [PubMed]
- Siezenga, M.A.; Chandie Shaw, P.K.; van der Geest, R.N.; Mollnes, T.E.; Daha, R.D.; Rabelink, T.J.; Berger, S.P. Enhanced complement activation is part of the unfavourable cardiovascular risk profile in South Asians. Clin. Exp. Immunol. 2009, 157, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Somani, R.; Grant, P.J.; Kain, K.; Catto, A.J.; Carter, A.M. Complement C3 and C-reactive protein are elevated in South Asians independent of a family history of stroke. Stroke 2006, 37, 2001–2006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somani, R.; Richardson, V.R.; Standeven, K.F.; Grant, P.J.; Carter, A.M. Elevated properdin and enhanced complement activation in first-degree relatives of South Asian subjects with type 2 diabetes. Diabetes Care 2012, 35, 894–899. [Google Scholar] [CrossRef] [Green Version]
- Brady, E.M.; Webb, D.R.; Morris, D.H.; Khunti, K.; Talbot, D.S.C.; Sattar, N.; Davies, M.J. Investigating endothelial activation and oxidative stress in relation to glycaemic control in a multiethnic population. Exp. Diabetes Res. 2012, 2012, 386041. [Google Scholar] [CrossRef]
- Dotsenko, O.; Chaturvedi, N.; Thom, S.A.M.; Wright, A.R.; Mayet, J.; Shore, A.; Schalkwijk, C.; Hughes, A.D. Platelet and leukocyte activation, atherosclerosis and inflammation in European and South Asian men. J. Thromb. Haem. 2007, 5, 2036–2042. [Google Scholar] [CrossRef] [Green Version]
- Khunti, K.; Morris, D.H.; Weston, C.L.; Gray, L.J.; Webb, D.R.; Davies, M.J. Joint Prevalence of Diabetes, Impaired Glucose Regulation, Cardiovascular Disease Risk and Chronic Kidney Disease in South Asians and White Europeans. PLoS ONE 2013, 8, e55580. [Google Scholar] [CrossRef] [Green Version]
- Agouni, A.; Parray, A.S.; Akhtar, N.; Mir, F.A.; Bourke, P.J.; Joseph, S.; Morgan, D.M.; Santos, M.D.; Wadiwala, M.F.; Kamran, S.; et al. There is selective increase in pro-thrombotic circulating extracellular vesicles in acute ischemic stroke and transient ischemic attack: A study of patients from the Middle East and Southeast Asia. Front. Neurol. 2019, 10, 251. [Google Scholar] [CrossRef]
- Ghosh, P.; Kumar, A.; Kumar, S.; Aggarwal, A.; Sinha, N.; Misra, R. Subclinical atherosclerosis and endothelial dysfunction in young South-Asian patients with systemic lupus erythematosus. Clin. Rheumatol. 2009, 28, 1259–1265. [Google Scholar] [CrossRef]
- Bedi, U.S.; Singh, S.; Syed, A.; Aryafar, H.; Arora, R. Coronary Artery Disease in South Asians: An Emerging Risk Group. Cardiol. Rev. 2006, 14, 74–80. [Google Scholar] [CrossRef]
- Lewis, M.J.; Jawad, A.S. The effect of ethnicity and genetic ancestry on the epidemiology, clinical features and outcome of systemic lupus erythematosus. Rheumatology 2017, 56 (Suppl. 1), i67–i77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, D.Y.; Chan, T.M. Lupus Nephritis in Asia: Clinical Features and Management. Kidney Dis. (Basel) 2015, 1, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Al-Homood, I.A. Thrombosis in systemic lupus erythematosus: A review article. ISRN Rheumatol. 2012, 2012, 428269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.P.; Gordon, C. Systemic lupus erythematosus: Clinical presentations. Autoimmun. Rev. 2010, 10, 43–45. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, N.; Tu, X.; Egan, A.J.; Stover, C. Complement Activation on Endothelial Cell-Derived Microparticles—A Key Determinant for Cardiovascular Risk in Patients with Systemic Lupus Erythematosus? Medicina 2020, 56, 533. https://doi.org/10.3390/medicina56100533
Martin N, Tu X, Egan AJ, Stover C. Complement Activation on Endothelial Cell-Derived Microparticles—A Key Determinant for Cardiovascular Risk in Patients with Systemic Lupus Erythematosus? Medicina. 2020; 56(10):533. https://doi.org/10.3390/medicina56100533
Chicago/Turabian StyleMartin, Naomi, Xiaodie Tu, Alicia J. Egan, and Cordula Stover. 2020. "Complement Activation on Endothelial Cell-Derived Microparticles—A Key Determinant for Cardiovascular Risk in Patients with Systemic Lupus Erythematosus?" Medicina 56, no. 10: 533. https://doi.org/10.3390/medicina56100533
APA StyleMartin, N., Tu, X., Egan, A. J., & Stover, C. (2020). Complement Activation on Endothelial Cell-Derived Microparticles—A Key Determinant for Cardiovascular Risk in Patients with Systemic Lupus Erythematosus? Medicina, 56(10), 533. https://doi.org/10.3390/medicina56100533