Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Subjects and Setting
2.2. Study Design
2.3. Oral Examination
2.4. Oral Hygiene Procedures Implemented by Nurse
2.5. Statistical Analysis
- Fixed effect: age, sex, days, intervention, number of remaining teeth, tube feeding/oral ingestion, days after hospitalization, medication
- Random effect: days after hospitalization
- Covariance Type: AR1
- Link functions: normal
2.6. Ethics
3. Results
3.1. Characteristics of the Subjects Participating in this Study
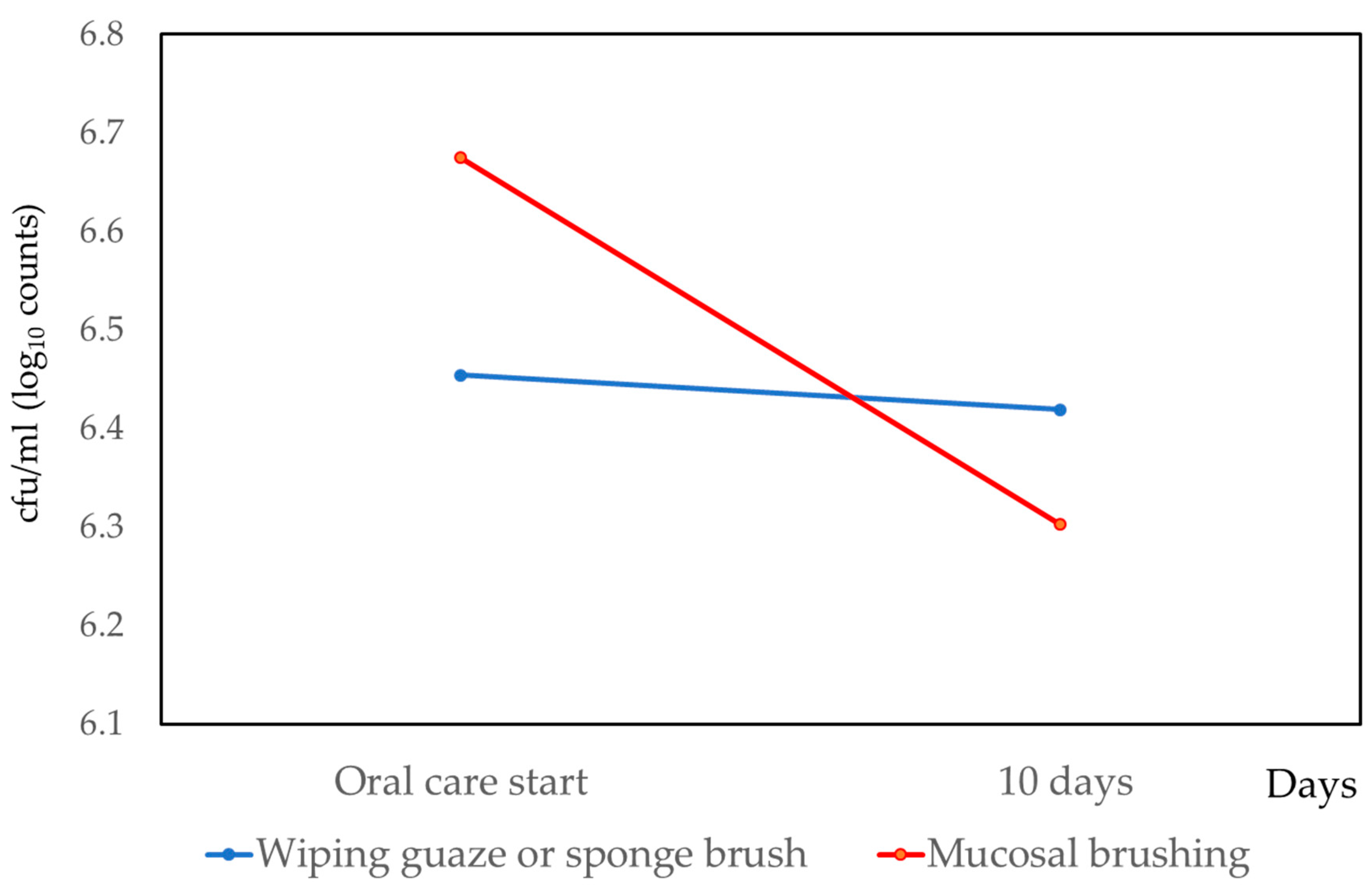
3.2. Changes of Bacteria on Tongue Surface
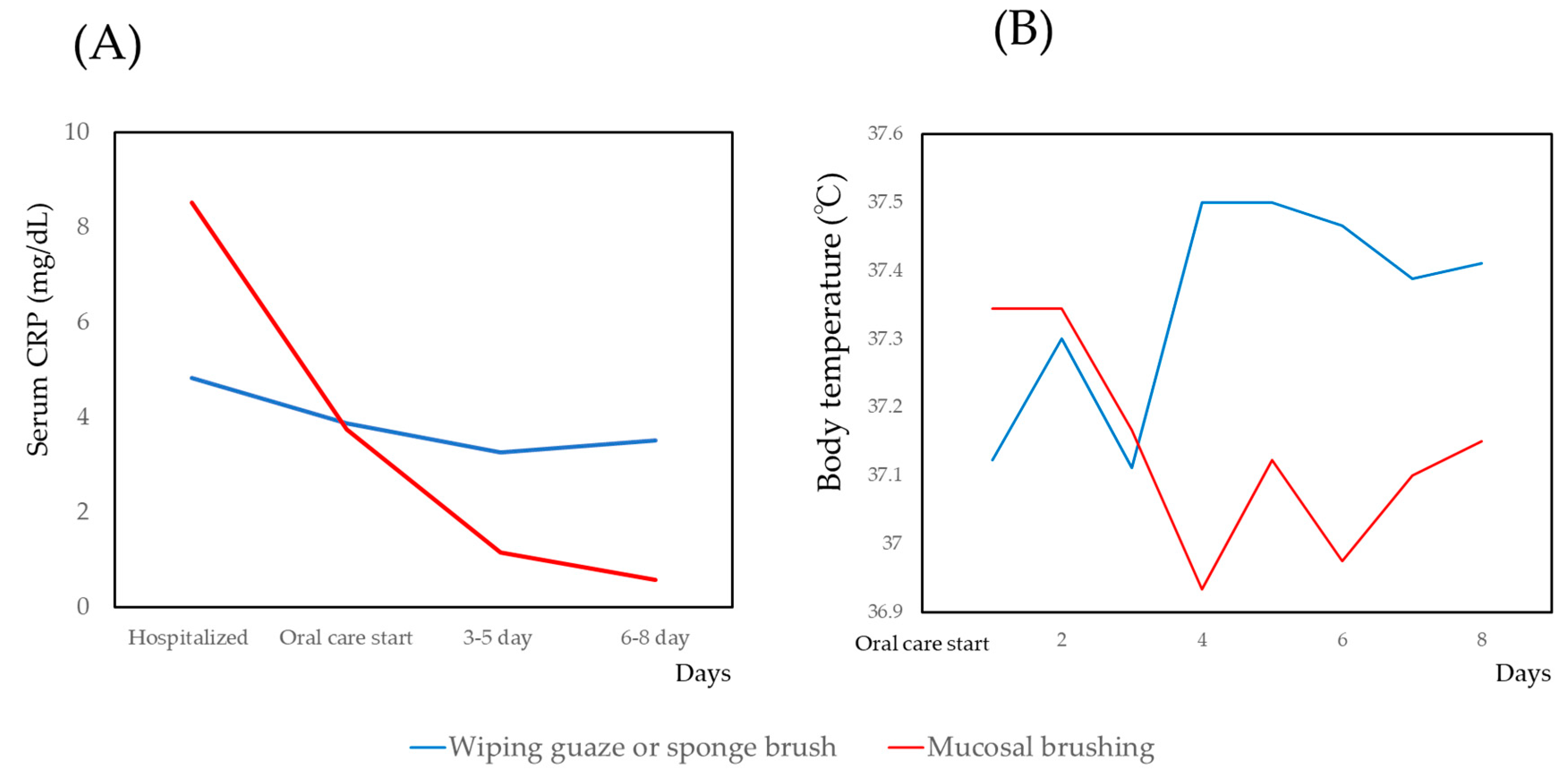
3.3. Changes of CRP and Body Temperature
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sjögren, P.; Wårdh, I.; Zimmerman, M.; Almståhl, A.; Wikström, M. Oral care and mortality in older adults with pneumonia in hospitals or nursing homes: Systematic review and meta-analysis. J. Am. Geriatr. Soc. 2016, 64, 2109–2115. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, P.; Nilsson, E.; Forsell, M.; Johansson, O.; Hoogstraate, J. A systematic review of the preventive effect of oral hygiene on pneumonia and respiratory tract infection in elderly people in hospitals and nursing homes: Effect estimates and methodological quality of randomized controlled trials. J. Am. Geriatr. Soc. 2008, 56, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, A.; Leake, J.L. Systematic review of the association between respiratory diseases and oral health. J. Periodontol. 2006, 77, 1465–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marin, S.; Serra-Prat, M.; Ortega, O.; Clavé, P. Healthcare-related cost of oropharyngeal dysphagia and its complications pneumonia and malnutrition after stroke: A systematic review. BMJ Open 2020, 10, e031629. [Google Scholar] [CrossRef] [PubMed]
- Labeit, B.; Pawlitzki, M.; Ruck, T.; Muhle, P.; Claus, I.; Suntrup-Krueger, S.; Warnecke, T.; Meuth, S.G.; Wiendl, H.; Dziewas, R. The Impact of Dysphagia in Myositis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2150. [Google Scholar] [CrossRef]
- López-Liria, R.; Parra-Egeda, J.; Vega-Ramírez, F.A.; Aguilar-Parra, J.M.; Trigueros-Ramos, R.; Morales-Gázquez, M.J.; Rocamora-Pérez, P. Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4104. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.; McAuley, D.F.; Walshe, M.; McGaughey, J.; Anand, R.; Fallis, R.; Blackwood, B. Interventions for oropharyngeal dysphagia in acute and critical care: A systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1326–1338. [Google Scholar] [CrossRef]
- Pillai, R.S.; Iyer, K.; Neto, R.S.; Kothari, S.F.; Nielsen, J.F.; Kothari, M. Oral Health and Brain Injury: Causal or Casual Relation? Cerebrovasc. Dis. Extra 2018, 8, 1–15. [Google Scholar] [CrossRef]
- Dai, R.; Lam, O.L.; Lo, E.C.; Li, L.S.; Wen, Y.; McGrath, C. A systematic review and meta-analysis of clinical, microbiological, and behavioural aspects of oral health among patients with stroke. J. Dent. 2015, 43, 171–180. [Google Scholar] [CrossRef]
- Kothari, M.; Pillai, R.S.; Kothari, S.F.; Neto, R.S.; Kumar, A.; Nielsen, J.F. Oral health status in patients with acquired brain injury: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 205–219. [Google Scholar] [CrossRef]
- Pirrone, M.; Pinciroli, R.; Berra, L. Microbiome, biofilms, and pneumonia in the ICU. Curr. Opin. Infect. Dis. 2016, 29, 160–166. [Google Scholar] [CrossRef]
- Dickson, R.P.; Erb-Downward, J.R.; Huffnagle, G.B. The role of the bacterial microbiome in lung disease. Expert Rev. Respir. Med. 2013, 7, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boisvert, A.A.; Cheng, M.P.; Sheppard, D.C.; Nguyen, D. Microbial biofilms in pulmonary and critical care diseases. Ann. Am. Thorac. Soc. 2016, 13, 1615–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mammen, M.J.; Scannapieco, F.A.; Sethi, S. Oral-lung microbiome interactions in lung diseases. Periodontology 2020, 83, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, V.; Torwane, N.A.; Tyagi, S.; Maran, S. Effectiveness of various tongue cleaning aids in the reduction of tongue coating and bacterial load: A Comparative Clinical Study. J. Contemp. Dent. Pract. 2019, 20, 444–448. [Google Scholar]
- Quirynen, M.; Avontroodt, P.; Soers, C.; Zhao, H.; Pauwels, M.; van Steenberghe, D. Impact of tongue cleansers on microbial load and taste. J. Clin. Periodontol. 2004, 31, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Ibayashi, H.; Nishiyama, T.; Tanaka, M.; Pham, T.M.; Yano, J.; Sakai, K.; Kobayashi, A.; Yakura, N.; Matsuda, S. Effects of oral health care on salivary flow rate in patients with type 2 diabetes: Preliminary study. Asia. Pac. J. Public Health 2009, 21, 279–286. [Google Scholar] [CrossRef]
- Kikutani, T.; Tamura, F.; Takahashi, Y.; Konishi, K.; Hamada, R. A novel rapid oral bacteria detection apparatus for effective oral care to prevent pneumonia. Gerodontology 2012, 29, e560–e565. [Google Scholar] [CrossRef]
- Nishimura, K.; Kagaya, H.; Shibata, S.; Onogi, K.; Inamoto, Y.; Ota, K.; Miki, T.; Tamura, S.; Saitoh, E. Accuracy of Dysphagia Severity Scale rating without using videoendoscopic evaluation of swallowing. Jpn. J. Compr. Rehabil. Sci. 2015, 6, 124–128. [Google Scholar] [CrossRef]
- Kumar, N.N.; Panchaksharappa, M.G.; Annigeri, R.G. Modified schirmer test—A screening tool for xerostomia among subjects on antidepressants. Arch. Oral Biol. 2014, 59, 829–834. [Google Scholar] [CrossRef]
- Nomura, Y.; Morozumi, T.; Nakagawa, T.; Sugaya, T.; Kawanami, M.; Suzuki, F.; Takahashi, K.; Abe, Y.; Sato, S.; Makino-Oi, A.; et al. Site-level progression of periodontal disease during a follow-up period. PLoS ONE 2017, 12, e0188670. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Takei, N.; Ishii, T.; Takada, K.; Amitani, Y.; Koganezawa, H.; Fukuhara, S.; Asai, K.; Uozumi, R.; Bessho, K. Factors that affect oral care outcomes for institutionalized elderly. Int. J. Dent. 2018, 2018, 2478408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, Y.; Fujita, Y.; Ishihara, Y.; Kakuta, E.; Okada, A.; Maki, K.; Hanada, N. Effects of cariogenic bacteria and sealant evaluated by International Caries Detection Assessment System. Open Dent. J. 2019, 13, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Tachibana, M.; Yoshida, A.; Ansai, T.; Takata, Y.; Akifusa, S.; Fukuhara, M.; Hamasaki, T.; Okuda, K.; Takehara, T. Prevalence of periodontopathic bacteria on the tongue dorsum of elderly people. Gerodontology 2006, 23, 123–126. [Google Scholar] [CrossRef]
- Teramoto, S.; Yoshida, K.; Hizawa, N. Update on the pathogenesis and management of pneumonia in the elderly-roles of aspiration pneumonia. Respir. Investig. 2015, 53, 178–184. [Google Scholar] [CrossRef]
- Kageyama, S.; Takeshita, T.; Furuta, M.; Tomioka, M.; Asakawa, M.; Suma, S.; Takeuchi, K.; Shibata, Y.; Iwasa, Y.; Yamashita, Y. Relationships of variations in the tongue microbiota and pneumonia mortality in nursing home residents. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, T.; Tomioka, M.; Shimazaki, Y.; Matsuyama, M.; Koyano, K.; Matsuda, K.; Yamashita, Y. Microfloral characterization of the tongue coating and associated risk for pneumonia-related health problems in institutionalized older adults. J. Am. Geriatr. Soc. 2010, 8, 1050–1057. [Google Scholar] [CrossRef]
- Hong, C.; Aung, M.M.; Kanagasabai, K.; Lim, C.A.; Liang, S.; Tan, K.S. The association between oral health status and respiratory pathogen colonization with pneumonia risk in institutionalized adults. Int. J. Dent. Hyg. 2018, 16, e96–e102. [Google Scholar] [CrossRef]
- Asakawa, M.; Takeshita, T.; Furuta, M.; Kageyama, S.; Takeuchi, K.; Hata, J.; Ninomiya, T.; Yamashita, T. Tongue microbiota and oral health status in community-dwelling elderly adults. mSphere 2018, 3, e00332-18. [Google Scholar] [CrossRef] [Green Version]
- Abe, S.; Ishihara, K.; Adachi, M.; Okuda, K. Tongue-coating as risk indicator for aspiration pneumonia in edentate elderly. Arch. Gerontol. Geriatr. 2008, 47, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Kikutani, T.; Tamura, F.; Tashiro, H.; Yoshida, M.; Konishi, K.; Hamada, R. Relationship between oral bacteria count and pneumonia onset in elderly nursing home residents. Geriatr. Gerontol. Int. 2015, 15, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Bordas, A.; McNab, R.; Staples, A.M.; Bowman, J.; Kanapka, J.; Bosma, M.P. Impact of different tongue cleaning methods on the bacterial load of the tongue dorsum. Arch. Oral Biol. 2008, 53, S13–S18. [Google Scholar] [CrossRef]
- Shigeishi, H.; Ohta, K.; Fujimoto, S.; Nakagawa, T.; Mizuta, K.; Ono, S.; Shimasue, H.; Ninomiya, Y.; Higashikawa, K.; Tada, M.; et al. Preoperative oral health care reduces postoperative inflammation and complications in oral cancer patients. Exp. Ther. Med. 2016, 12, 1922–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funahara, M.; Yanamoto, S.; Soutome, S.; Hayashida, S.; Umeda, M. Clinical observation of tongue coating of perioperative patients: Factors related to the number of bacteria on the tongue before and after surgery. BMC Oral Health 2018, 18, 223. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Matsuo, K.; Okamoto, M.; Nakata, H.; Sakamoto, H.; Fujita, M. Perioperative changes in oral bacteria number in patients undergoing cardiac valve surgery. J. Oral Sci. 2019, 61, 526–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odgaard, L.; Kothari, M. Prevalence and association of oral candidiasis with dysphagia in individuals with acquired brain injury. Brain Inj. 2018, 32, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Bath, P.M.; Lee, H.S.; Everton, L.F. Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst. Rev. 2018, 10, CD000323. [Google Scholar] [CrossRef]
- Yeates, E.M.; Molfenter, S.M.; Steele, C.M. Improvements in tongue strength and pressure-generation precision following a tongue-pressure training protocol in older individuals with dysphagia: Three case reports. Clin. Interv. Aging 2008, 3, 735–747. [Google Scholar] [CrossRef] [Green Version]
- Dai, R.; Lam, O.L.T.; Lo, E.C.M.; Li, L.S.W.; McGrath, C. A randomized clinical trial of oral hygiene care programmes during stroke rehabilitation. J. Dent. 2017, 61, 48–54. [Google Scholar] [CrossRef]
- Dai, R.; Lam, O.L.T.; Lo, E.C.M.; Li, L.S.W.; McGrath, C. Effect of oral hygiene programmes on oral opportunistic pathogens during stroke rehabilitation. Oral Dis. 2019, 25, 617–633. [Google Scholar] [CrossRef]
- Kamieńska, T.M.; Śniatała, R.; Gabryel, H.B.; Lewicka, M.B.; Cofta, S. Periodontal status and subgingival biofilms in cystic fibrosis adults. Pol. J. Microbiol. 2019, 68, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamieńska, T.P.; Lewicka, M.B.; Gabryel, H.B. Salivary biomarkers and oral microbial load in relation to the dental status of adults with cystic fibrosis. Microorganisms 2019, 13, 692. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Gauze or Sponge Brush (n = 8) | Mucosal Brushing (n = 9) | Total (n = 17) | p-Value | |
|---|---|---|---|---|
| Age | 87.22 +/− 8.41 | 92.00 +/− 3.54 | 89.61 +/− 6.72 | 0.249 |
| Men/Women | 1/7 | 1/8 | 2/16 | 0.765 |
| Tube feeding/oral ingestion | 2/6 | 5/4 | 7/10 | 0.201 |
| Denture use | 5 | 5 | 10 | 0.722 |
| Number of remaining teeth | 2.22 +/− 3.35 | 0.79 +/− 1.39 | 1.50 +/− 2.60 | 0.451 |
| Serum levels of CRP (mg/dL) (day of hospitalization) | 3.12 +/− 4.29 | 4.89 +/− 5.41 | 3.95 +/− 4.78 | 0.700 |
| Body temperature (°C) | ||||
| Day of hospitalization | 34.04 +/− 10.3 | 37.23 +/− 0.45 | 35.54 +/− 7.47 | 0.961 |
| Day of oral care start | 37.12 +/− 0.25 | 37.24 +/− 0.44 | 37.18 +/− 0.36 | 0.504 |
| Oral bacteria (log10 cfu) | 4.26 +/− 2.7 | 5.81 +/− 2.46 | 5.04 +/− 2.63 | 0.233 |
| Dysphagia Slight injury/Slander/Severe | 1/6/1 | 1/4/4 | 2/10/5 | 0.620 |
| Wettability of saliva | 0.89 +/− 1.62 | 1.11 +/− 1.83 | 1.00 +/− 1.68 | 0.920 |
| Gauze or Sponge Brush (n = 8) | Mucosal Brushing (n = 9) | |
|---|---|---|
| Aspiration pneumonia | 4 | 4 |
| Acute pyelonephritis | 1 | 2 |
| Urinary tract infection (UTI) | 1 | 1 |
| Cholangitis | 1 | 0 |
| Epilepsy, convulsive seizure | 1 | 0 |
| Aphagia | 0 | 1 |
| Hypernatremia, dehydration | 0 | 1 |
| CRP | Body Temperature | |||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| Intercept | −32.746 (−37.765–−27.727) | <0.001 | 36.900 (35.966–37.834) | <0.001 |
| Age | 0.357 (0.300–0.414) | <0.001 | 0.004 (−0.007–0.015) | 0.455 |
| Sex (Man/Woman) | 2.911 (−0.0560–5.879) | 0.054 | −0.478 (−0.739–−0.216) | <0.001 |
| Intervention (Mucosal brushing/Wiping gauze or sponge brush) | −2.296 (−4.486–−0.107) | 0.040 | −0.067 (−0.068–−0.065) | <0.001 |
| Number of remaining teeth | 0.887 (0.270–1.504) | 0.006 | 0.006 (−0.030–0.041) | 0.751 |
| Tube feeding/Oral ingestion | −0.213 (−2.276–1.849) | 0.835 | −0.024 (−0.200–0.152) | 0.787 |
| Days after hospitalization | 0.095 (0.095–0.095) | <0.001 | 0.001 (−0.015–0.017) | 0.874 |
| Medication (Antipyretic analgesic) | −1.901 (−4.206–0.404) | 0.103 | 0.255 (−0.450–−0.060) | 0.011 |
| Medication (Antibiotic) | 4.101 (3.873–4.329) | <0.001 | 0.120 (−0.143–0.382) | 0.370 |
| BIC | 320.096 | 594.087 | ||
| AICC | 363.105 | 423.837 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakahodo, N.; Nomura, Y.; Oshiro, T.; Otsuka, R.; Kakuta, E.; Okada, A.; Inai, Y.; Takei, N.; Hanada, N. Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms. Medicina 2020, 56, 549. https://doi.org/10.3390/medicina56100549
Nakahodo N, Nomura Y, Oshiro T, Otsuka R, Kakuta E, Okada A, Inai Y, Takei N, Hanada N. Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms. Medicina. 2020; 56(10):549. https://doi.org/10.3390/medicina56100549
Chicago/Turabian StyleNakahodo, Naoko, Yoshiaki Nomura, Takumi Oshiro, Ryoko Otsuka, Erika Kakuta, Ayako Okada, Yuko Inai, Noriko Takei, and Nobuhiro Hanada. 2020. "Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms" Medicina 56, no. 10: 549. https://doi.org/10.3390/medicina56100549
APA StyleNakahodo, N., Nomura, Y., Oshiro, T., Otsuka, R., Kakuta, E., Okada, A., Inai, Y., Takei, N., & Hanada, N. (2020). Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms. Medicina, 56(10), 549. https://doi.org/10.3390/medicina56100549