Clinical Predictors of Preeclampsia in Pregnant Women with Chronic Kidney Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definitions
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Comparison between Women With and Without Preeclampsia
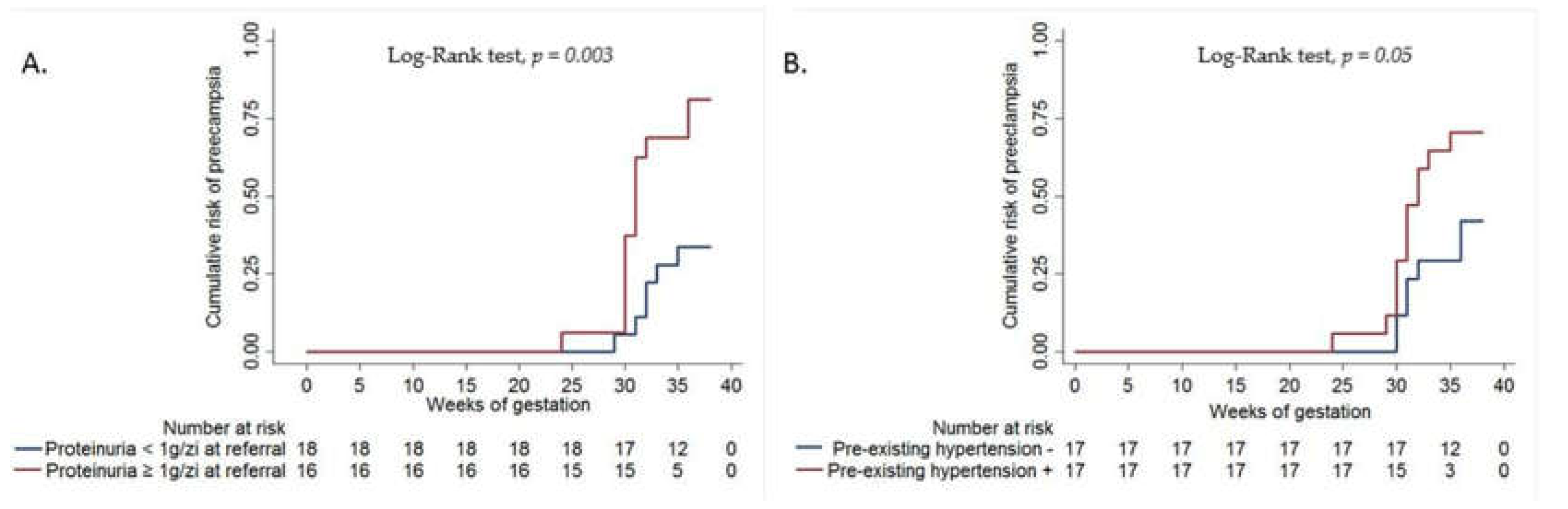
3.3. Predictors of Superimposed Preeclampsia
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nevis, I.F.; Reitsma, A.; Dominic, A.; McDonald, S.; Thabane, L.; Akl, E.A.; Hladunewich, M.; Akbari, A.; Joseph, G.; Sia, W.; et al. Pregnancy outcomes in women with chronic kidney disease: A systematic review. Clin. J. Am. Soc. Nephrol. 2011, 6, 2587–2598. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Attini, R.; Vasario, E.; Conijn, A.; Biolcati, M.; D’Amico, F.; Consiglio, V.; Bontempo, S.; Todros, T. Pregnancy and chronic kidney disease: A challenge in all CKD stages. Clin. J. Am. Soc. Nephrol. 2010, 5, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Davison, J. Chronic kidney disease in pregnancy. BMJ 2008, 336, 211–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steegers, E.A.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-eclampsia. Lancet 2010, 376, 631–644. [Google Scholar] [CrossRef]
- Bramham, K.; Parnell, B.; Nelson-Piercy, C.; Seed, P.T.; Poston, L.; Chappell, L.C. Chronic hypertension and pregnancy outcomes: Systematic review and meta-analysis. BMJ 2014, 348, g2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirose, N.; Ohkuchi, A.; Usui, R.; Matsubara, S.; Suzuki, M. Risk of preeclampsia in women with CKD, dialysis or kidney transplantation. Med. J. Obstet. Gynecol. 2014, 2, 1028. [Google Scholar]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Vigotti, F.; Fassio, F.; Rolfo, A.; Giuffrida, D.; Pani, A.; Gaglioti, P.; Todros, T. Pregnancy in chronic kidney disease: Questions and answers in a changing panorama. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 625–642. [Google Scholar] [CrossRef]
- Rolfo, A.; Attini, R.; Nuzzo, A.M.; Piazzese, A.; Parisi, S.; Ferraresi, M.; Todros, T.; Piccoli, G.B. Chronic kidney disease may be differentially diagnosed from preeclampsia by serum biomarkers. Kidney Int. 2013, 83, 177–181. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar]
- Tranquilli, A.L.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.M.; Steyn, W.; Zeeman, G.G.; Brown, M.A. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014, 4, 97–104. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- van der Graaf, A.M.; Toering, T.J.; Faas, M.M.; Lely, A.T. From preeclampsia to renal disease: A role of angiogenic factors and the renin-angiotensin aldosterone system? Nephrol. Dial. Transplant. 2012, 27, iii51–iii57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, K.; Bramham, K.; Seed, P.T.; Kurlak, L.O.; Mistry, H.D.; Nelson-Piercy, C.; Lightstone, L.; Chappell, L.C. Diagnostic Indicators of Superimposed Preeclampsia in Women With CKD. Kidney Int. Rep. 2019, 4, 842–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regal, J.F.; Burwick, R.M.; Fleming, S.D. The Complement System and Preeclampsia. Curr. Hypertens. Rep. 2017, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Maxia, S.; Lepori, N.; Tuveri, M.; Massidda, M.; Marchi, C.; Mura, S.; et al. Risk of adverse pregnancy outcomes in women with CKD. J. Am. Soc. Nephrol. 2015, 26, 2011–2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, X.; Lv, J.; Liu, Y.; Wang, J.; Ma, X.; Shi, S.; Liu, L.; Zhang, H. Pregnancy and kidney outcomes in patients with IgA nephropathy: A cohort study. Am. J. Kidney Dis. 2017, 70, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Ma, X.X.; Hao, L.; Liu, L.J.; Lv, J.C.; Zhang, H. A systematic review and meta-analysis of outcomes of pregnancy in CKD and CKD outcomes in pregnancy. Clin. J. Am. Soc. Nephrol. 2015, 10, 1964–1978. [Google Scholar] [CrossRef]
- Webster, P.; Webster, L.M.; Cook, H.T.; Horsfield, C.; Seed, P.T.; Vaz, R.; Santos, C.; Lydon, I.; Homsy, M.; Lightstone, L.; et al. A Multicenter Cohort Study of Histologic Findings and Long-Term Outcomes of Kidney Disease in Women Who Have Been Pregnant. Clin. J. Am. Soc. Nephrol. 2017, 12, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Langer, B.; Grima, M.; Coquard, C.; Bader, A.M.; Schlaeder, G.; Imbs, J.L. Plasma active renin, angiotensin I, and angiotensin II during pregnancy and in preeclampsia. Obstet. Gynecol. 1998, 91, 196–202. [Google Scholar] [CrossRef]
- Stanhewicz, A.E.; Jandu, S.; Santhanam, L.; Alexander, L.M. Increased Angiotensin II Sensitivity Contributes to Microvascular Dysfunction in Women Who Have Had Preeclampsia. Hypertension 2017, 70, 382–389. [Google Scholar] [CrossRef]
- Kobori, H.; Nangaku, M.; Navar, L.G.; Nishiyama, A. The intrarenal renin angiotensin system: From physiology to the pathobiology of hypertension and kidney disease. Pharmacol. Rev. 2007, 59, 251–287. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.C.; Ahmad, S.; Mi, T.; Xia, L.; Abbasi, S.; Hewett, P.W.; Sun, C.; Ahmed, A.; Kellems, R.E.; Xia, Y. Angiotensin II induces soluble fms like tyrosine kinase-1 release via calcineurin signaling pathway in pregnancy. Circ. Res. 2007, 100, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, Z.; Yildirim, T.; Yilmaz, R.; Aybal-Kutlugun, A.; Altun, B.; Kucukozkan, T.; Erdem, Y. Association between urinary angiotensinogen, hypertension and proteinuria in pregnant women with preeclampsia. J. Renin Angiotensin Aldosterone Syst. 2015, 16, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuyama, H.; Nobumoto, E.; Okimoto, N.; Inoue, S.; Segawa, T.; Hiramatsu, Y. Superimposed preeclampsia in women with chronic kidney disease. Gynecol. Obstet. Investig. 2012, 74, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, A.; Attini, R.; Tavassoli, E.; Neve, F.V.; Nigra, M.; Cicilano, M.; Nuzzo, A.M.; Giuffrida, D.; Biolcati, M.; Nichelatti, M.; et al. Is it possible to differentiate chronic kidney disease and preeclampsia by means of new and old biomarkers? A prospective study. Dis. Markers. 2015, 127083, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bramham, K.; Seed, P.T.; Lightstone, L.; Nelson-Piercy, C.; Gill, C.; Webster, P.; Poston, L.; Chappell, L.C. Diagnostic and predictive biomarkers for pre-eclampsia in patients with established hypertension and chronic kidney disease. Kidney Int. 2016, 89, 874–885. [Google Scholar] [CrossRef] [Green Version]
- Diaconu, C.C.; Nastasa, A.; Zaki, A.; Istratie, B.; Nazari, R.; Iancu, M.A.; Balaceanu, A. A comparative analysis of the hypertension treatment depending on comorbidities: Insights from clinical practice. J. Hypertens. 2016, 34, E320–E321. [Google Scholar] [CrossRef]


{kind=link}
| Patients Characteristics | Overall (N = 34) | Preeclampsia (N = 19) | No Preeclampsia (N = 15) | p-value |
|---|---|---|---|---|
| Maternal age (mean, years) | 24.26± 3.96 | 23.15±2.31 | 25.66±5.13 | 0.06 |
| ≥30 years (%) | 3 (8.8%) | 0 (%) | 3 (20%) | 0.02a |
| Nulliparity (%) | 29 (85.3%) | 18 (94.7%) | 11 (73.3%) | 0.07 |
| BMI (mean, kg/m2) | 21.91±3.36 | 22.28±3.26 | 21.45±3.54 | 0.48 |
| ≥25 kg/m2 (%) | 8 (23.5%) | 4 (21.1%) | 4 (26.7%) | 0.70 |
| Primary kidney disease (%) | 26 (76.5%) | 16 (84.2%) | 10 (66.7%) | |
| Glomerulonephritis Tubulointerstitial disease (%) | 5 (14.7%) | 2 (10.5%) | 3 (20%) | 0.20 |
| Diabetic kidney disease (%) | 3 (8.8%) | 1 (5.3%) | 2 (13.3%) | |
| Pre-existing hypertension (%) | 17 (50%) | 12 (63.2%) | 5 (33.3%) | 0.08 |
| Dyslipidemia (%) | 9 (26.5%) | 6 (31.6%) | 3 (20%) | 0.44 |
| Hepatitis B virus infection (%) | 3 (8.8%) | 2(10.5%) | 1(6.7%) | 0.69 |
| Hepatitis C virus infection (%) | 3 (8.8%) | 1 (5.3%) | 2 (13.3%) | 0.41 |
| Urinary tract infections (%) | 17 (50%) | 11 (57.9%) | 6 (40%) | 0.30 |
| Creatinine at referral (mean, mg/dL) | 1.6 ±0.6 | 1.79±0.75 | 1.36±0.40 | 0.05 |
| Creatinine at birth (mean, mg/dL) | 1.6±0.8 | 1.93±0.98 | 1.20±0.33 | 0.01 a |
| eGFR at referral (mean, ml/min) | 51.2± 22.8 | 46.16± 22.65 | 57.65±22 | 0.14 |
| eGFR at birth (mean, ml/min) | 51.5±21.8 | 42.62± 18 | 62.79± 21.4 | 0.005 a |
| CKD stage (%) | 0.23 | |||
| G1-G2 | 8 (23.5%) | 3 (15.8%) | 5 (33.3%) | |
| G3-G4 | 26(76.5%) | 16 (84.2%) | 10 (66.7%) | |
| Proteinuria at referral (median, g/24 h) | 0.87 (0.42−1.50) | 1.30 (0.67−1.50) | 0.63 (0.30−0.85) | 0.02 a |
| Proteinuria ≥ 1 g/day at referral (%) | 16 (47.1%) | 13 (68.7%) | 3 (20%) | 0.005 a |
| Fetal death (%) | 1 (3.1%) | 1 (5.3%) | 0 (0%) | 0.27 |
| Low birth weight (%) | 17 (50%) | 16 (84.2%) | 1 (6.7%) | <0.001 a |
| Cox Univariate Regression | Cox Multivariate Regression | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-value | HR | 95% CI | p-value |
| Maternal age | 0.88 | 0.75−1.03 | 0.12 | - | - | - |
| Nulliparity | 4 | 0.53−30.07 | 0.17 | - | - | - |
| Creatinine at referral | 1.57 | 0.87−2.73 | 0.13 | - | - | - |
| Proteinuria ≥ 1 g/day at referral | 3.91 | 3.74−9.98 | 0.008 | 4.10 | 1.52−11.02 | 0.005 |
| Pre-existing hypertension | 2.31 | 0.90−5.92 | 0.07 | 2.62 | 1.01−6.77 | 0.04 |
| Proteinuria ≥ 1 g/day at Referral | Pre-Existing Hypertension | |||
|---|---|---|---|---|
| Value | 95% CI | Value | 95% CI | |
| Sensitivity (%) | 68.42% | 43.45%−87.42% | 63.16% | 38.36%−83.71% |
| Specificity (%) | 80% | 51.91%−95.67% | 66.67% | 38.38%−88.18% |
| +LHR | 3.42 | 1.19%−9.85 | 1.89 | 0.86%−4.19 |
| -LHR | 0.39 | 0.19%−0.80 | 0.55 | 0.28%−1.10 |
| PPV (%) | 81.2% | 60.09%−92.58% | 70.59% | 12.04%−84.15% |
| NPV (%) | 66.67% | 49.61%−80.25% | 58.82% | 41.77%−73.99% |
| Accuracy (%) | 73.53% | 55.64%−87.12% | 64.71% | 46.49%−80.25% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorohan, B.M.; Andronesi, A.; Ismail, G.; Jurubita, R.; Obrisca, B.; Baston, C.; Harza, M. Clinical Predictors of Preeclampsia in Pregnant Women with Chronic Kidney Disease. Medicina 2020, 56, 213. https://doi.org/10.3390/medicina56050213
Sorohan BM, Andronesi A, Ismail G, Jurubita R, Obrisca B, Baston C, Harza M. Clinical Predictors of Preeclampsia in Pregnant Women with Chronic Kidney Disease. Medicina. 2020; 56(5):213. https://doi.org/10.3390/medicina56050213
Chicago/Turabian StyleSorohan, Bogdan Marian, Andreea Andronesi, Gener Ismail, Roxana Jurubita, Bogdan Obrisca, Cătălin Baston, and Mihai Harza. 2020. "Clinical Predictors of Preeclampsia in Pregnant Women with Chronic Kidney Disease" Medicina 56, no. 5: 213. https://doi.org/10.3390/medicina56050213
APA StyleSorohan, B. M., Andronesi, A., Ismail, G., Jurubita, R., Obrisca, B., Baston, C., & Harza, M. (2020). Clinical Predictors of Preeclampsia in Pregnant Women with Chronic Kidney Disease. Medicina, 56(5), 213. https://doi.org/10.3390/medicina56050213