A Patient with Cryoglobulinemic Membranoproliferative GN (MPGN) Who Survived COVID-19 Disease: Case Presentation and Current Data of COVID-19 Infection in Dialysis and Transplanted Patients in Greece



 ,
, 
Abstract
:1. Introduction
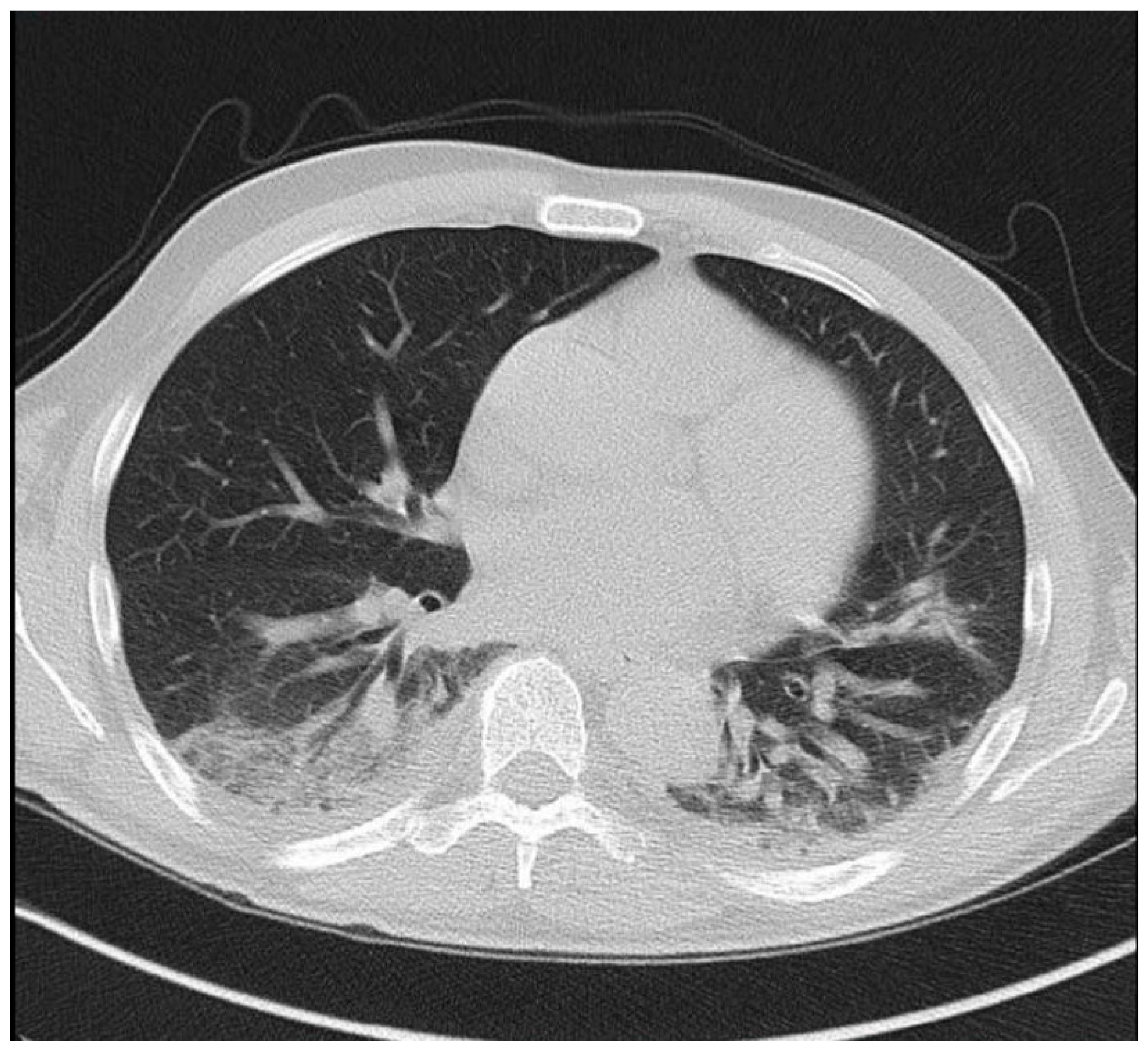
2. Case Report
3. Discussion
3.1. Symptoms at Presentation
3.2. Risk Factors
3.3. Disease Course and Treatment of Immunocompromised Individuals
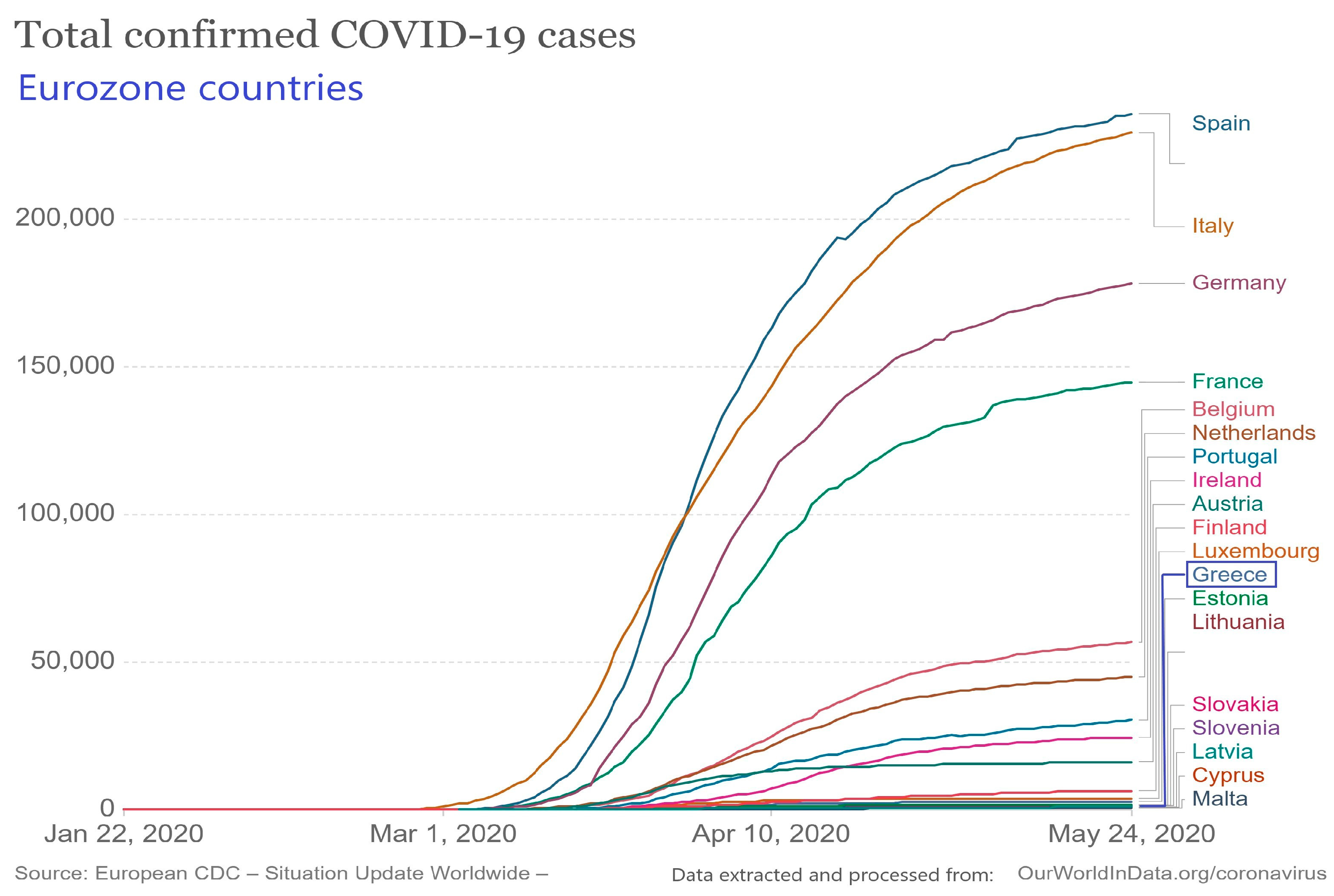
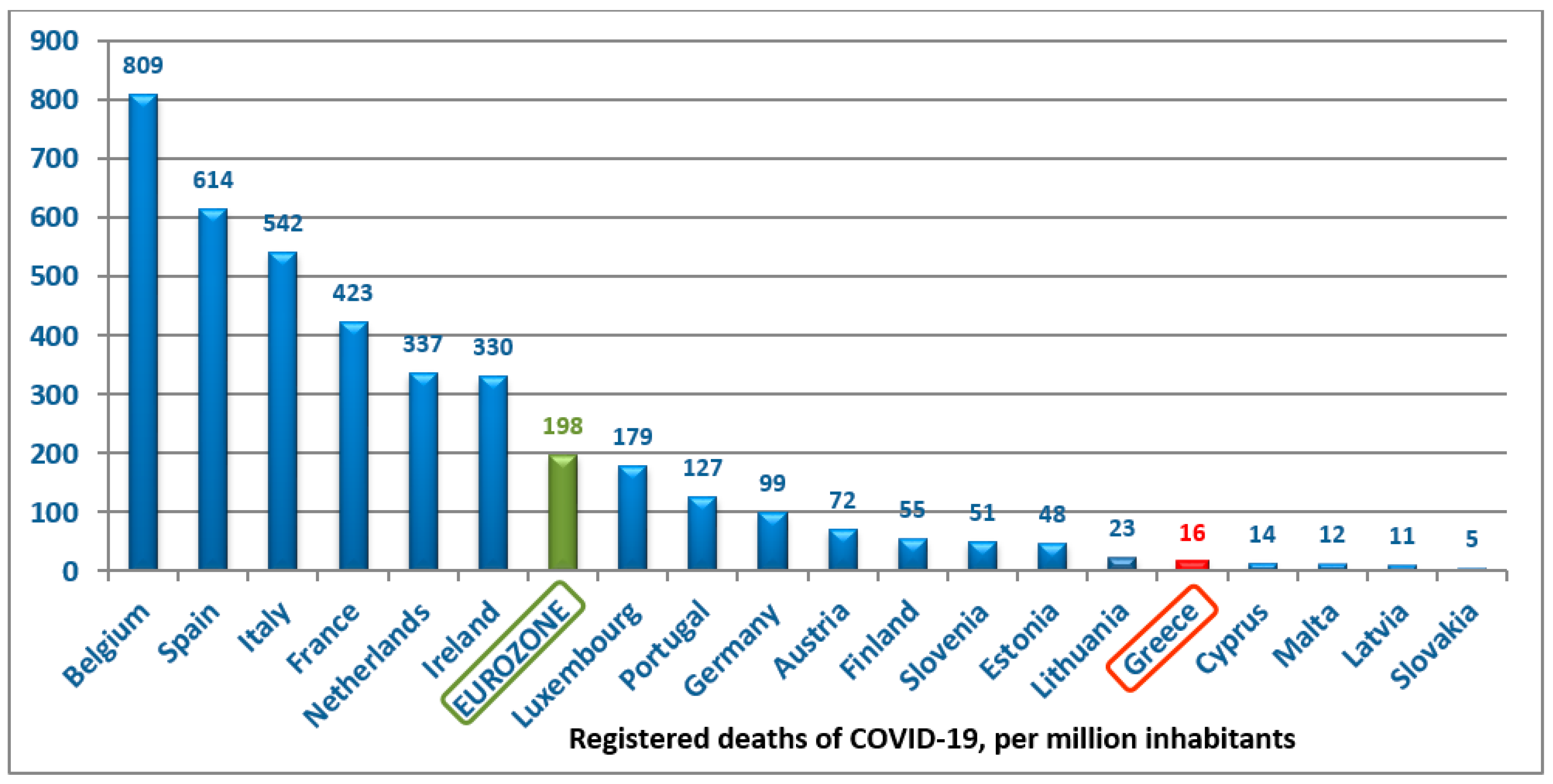
3.4. Epidemiology and Impact of Preventive Measures
- personnel training and application of infection control measures (hand hygiene, facial mask and gloves);
- apredefined pathway in the Emergency Department for suspected cases, namelyscreening with NAT and isolation in a separate ward until the first COVID-19 PCR, after whichpatients with positive tests are transferred to one of the four referral hospitals of Athens, andpatients with negative tests are transferred to the normal ward under isolation until the second negative test; and
- limitation of elective surgical procedures, including cessation of living donor transplantations.Guidelines were provided by the Hellenic Transplant Organisation on 15 March and the Hellenic Society of Nephrology on 17 March to all transplant centers and to all hospitals and dialysis units, respectively.
- Patients undergoing maintenance dialysis were briefly evaluated for symptoms consistent with COVID-19 and had their body temperature measured before entering the Dialysis Unit. Handwashing and facemask use were mandatory upon entrance to the facility. Patients were separated by a distance of at least 1.5 m from each other and were required to keep their facemasks on during the entire dialysis session. No food or fluid intake was allowed while in the treatment area.
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xu, J.; Zhao, S.; Teng, T.; Abdalla, A.E.; Zhu, W.; Xie, L.; Wang, Y.; Guo, X. Systematic Comparison of Two Animal-to-Human Transmitted Human Coronaviruses: SARS-CoV-2 and SARS-CoV. Viruses 2020, 12, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, P.; Lu, X.; Xu, C.; Sun, W.; Pan, B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Bomback, A.S.; Canetta, P.A.; Ahn, W.; Ahmad, S.B.; Radhakrishnan, J.; Appel, G.B. How COVID-19 Has Changed the Management of Glomerular Diseases. Clin. J. Am. Soc. Nephrol. 2020, 15, 876–879. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Piva, S.; Latronico, N.; et al. Management of Patients on Dialysis and With Kidney Transplantation During the SARS-CoV-2 (COVID-19) Pandemic in Brescia, Italy. Kidney Int. Rep. 2020, 5, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Popoola, J.; Shah, S.; Ster, I.C.; Quan, V.; Phanish, M. COVID-19 infection in kidney transplant recipients. Kidney Int. 2020, 97, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- ERACODA—The ERA-EDTA COVID-19 Database for Patients on Kidney Replacement Therapy. Available online: https://www.era-edta.org/en/covid-19-news-and-information/ (accessed on 6 May 2020).
- European Centre for Disease Prevention and Control. “COVID-19 Situation Update for the EU/EEA”. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 24 May 2020).
- Guillen, E.; Pineiro, G.J.; Revuelta, I.; Rodriguez, D.; Bodro, M.; Moreno, A.; Campistol, J.M.; Diekmann, F.; Ventura-Aguiar, P. Case report of COVID-19 in a kidney transplant recipient: Does immunosuppression alter the clinical presentation? Arab. Archaeol. Epigr. 2020, 20, 1875–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Hear. Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.; Gong, N.; Liu, B.; Lu, X.; Chen, D.; Chen, S.; Shu, H.; Ma, K.; Xu, X.; Guo, Z.; et al. Coronavirus Disease 2019 Pneumonia in Immunosuppressed Renal Transplant Recipients: A Summary of 10 Confirmed Cases in Wuhan, China. Eur. Urol. 2020, 77, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Nacif, L.S.; Zanini, L.Y.; Waisberg, D.R.; Pinheiro, R.S.; Galvão, F.; Andraus, W.; D’Albuquerque, L.C. COVID-19 in solid organ transplantation patients: A systematic review. Clinics 2020, 75, e1983. [Google Scholar] [CrossRef]
- Jüni, P.; Rothenbühler, M.; Bobos, P.; Thorpe, K.E.; Da Costa, B.R.; Fisman, D.N.; Slutsky, A.S.; Gesink, D. Impact of climate and public health interventions on the COVID-19 pandemic: A prospective cohort study. Can. Med Assoc. J. 2020, 192, E566–E573. [Google Scholar] [CrossRef]
- Johnson, K.M.; Belfer, J.J.; Peterson, G.R.; Boelkins, M.R.; Dumkow, L.E. Managing COVID-19 in Renal Transplant Recipients: A Review of Recent Literature and Case Supporting Corticosteroid-sparing Immunosuppression. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 517–524. [Google Scholar] [CrossRef]
- Thiel, J.; Rizzi, M.; Engesser, M.; Dufner, A.-K.; Troilo, A.; Lorenzetti, R.; Voll, R.E.; Venhoff, N. B cell repopulation kinetics after rituximab treatment in ANCA-associated vasculitides compared to rheumatoid arthritis, and connective tissue diseases: a longitudinal observational study on 120 patients. Arthritis Res. 2017, 19, 101. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 News and Information for the ERA-EDTA Community and Kidney Patients. Available online: https://www.era-edta.org/en/covid-19-news-and-information/#toggle-id-8 (accessed on 5 May 2020).
- National Public Health Organization (NPHO). “Current State of Covid-19 Outbreak in Greece and Timeline of Key Containment Events”. Available online: https://eody.gov.gr/en/current-state-of-covid-19-outbreak-in-greece-and-timeline-of-key-containment-events/ (accessed on 4 March 2020).
- National Public Health Organization (NPHO). Available online: https://eody.gov.gr/0410_briefing_covid19/ (accessed on 24 May 2020).
- Reported Cases and Deaths by Country, Territory, or Conveyance. Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 24 May 2020).
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 24 May 2020).
- University of Oxford. Available online: https://ourworldindata.org/coronavirus#confirmed-cases-vs-deaths (accessed on 24 May 2020).
- Greek Ministry of Health. The National Registry of Patients with End Stage Renal Disease, Coordination and Control Service of the Programme of End Stage Renal Disease; Athens, Greece, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total Population | Confirmed Cases | Prevalence | Confirmed Deaths | Mortality | Case Fatality Rate | |
|---|---|---|---|---|---|---|
| Hemodialysispatients | 11,590 | 28 | 0.24% | 6 | 0.23% | 21% |
| Transplantrecipients | 2567 | 1 | 0.038% | 0 | 0% | 0% |
| General population | 10,724,000 | 2878 ¹ | 0.026% ¹ | 171 | 0.0015% | 5.9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marinaki, S.; Tsiakas, S.; Skalioti, C.; Lourida, P.; Argyraki, A.; Grigorakos, K.; Boletis, I. A Patient with Cryoglobulinemic Membranoproliferative GN (MPGN) Who Survived COVID-19 Disease: Case Presentation and Current Data of COVID-19 Infection in Dialysis and Transplanted Patients in Greece. Medicina 2020, 56, 355. https://doi.org/10.3390/medicina56070355
Marinaki S, Tsiakas S, Skalioti C, Lourida P, Argyraki A, Grigorakos K, Boletis I. A Patient with Cryoglobulinemic Membranoproliferative GN (MPGN) Who Survived COVID-19 Disease: Case Presentation and Current Data of COVID-19 Infection in Dialysis and Transplanted Patients in Greece. Medicina. 2020; 56(7):355. https://doi.org/10.3390/medicina56070355
Chicago/Turabian StyleMarinaki, Smaragdi, Stathis Tsiakas, Chrysanthi Skalioti, Panayiota Lourida, Aikaterini Argyraki, Konstantinos Grigorakos, and Ioannis Boletis. 2020. "A Patient with Cryoglobulinemic Membranoproliferative GN (MPGN) Who Survived COVID-19 Disease: Case Presentation and Current Data of COVID-19 Infection in Dialysis and Transplanted Patients in Greece" Medicina 56, no. 7: 355. https://doi.org/10.3390/medicina56070355
APA StyleMarinaki, S., Tsiakas, S., Skalioti, C., Lourida, P., Argyraki, A., Grigorakos, K., & Boletis, I. (2020). A Patient with Cryoglobulinemic Membranoproliferative GN (MPGN) Who Survived COVID-19 Disease: Case Presentation and Current Data of COVID-19 Infection in Dialysis and Transplanted Patients in Greece. Medicina, 56(7), 355. https://doi.org/10.3390/medicina56070355