Intravenous r-tPA Dose Influence on Outcome after Middle Cerebral Artery Ischemic Stroke Treatment by Mechanical Thrombectomy

 , ,
, , 
Abstract
:1. Introduction
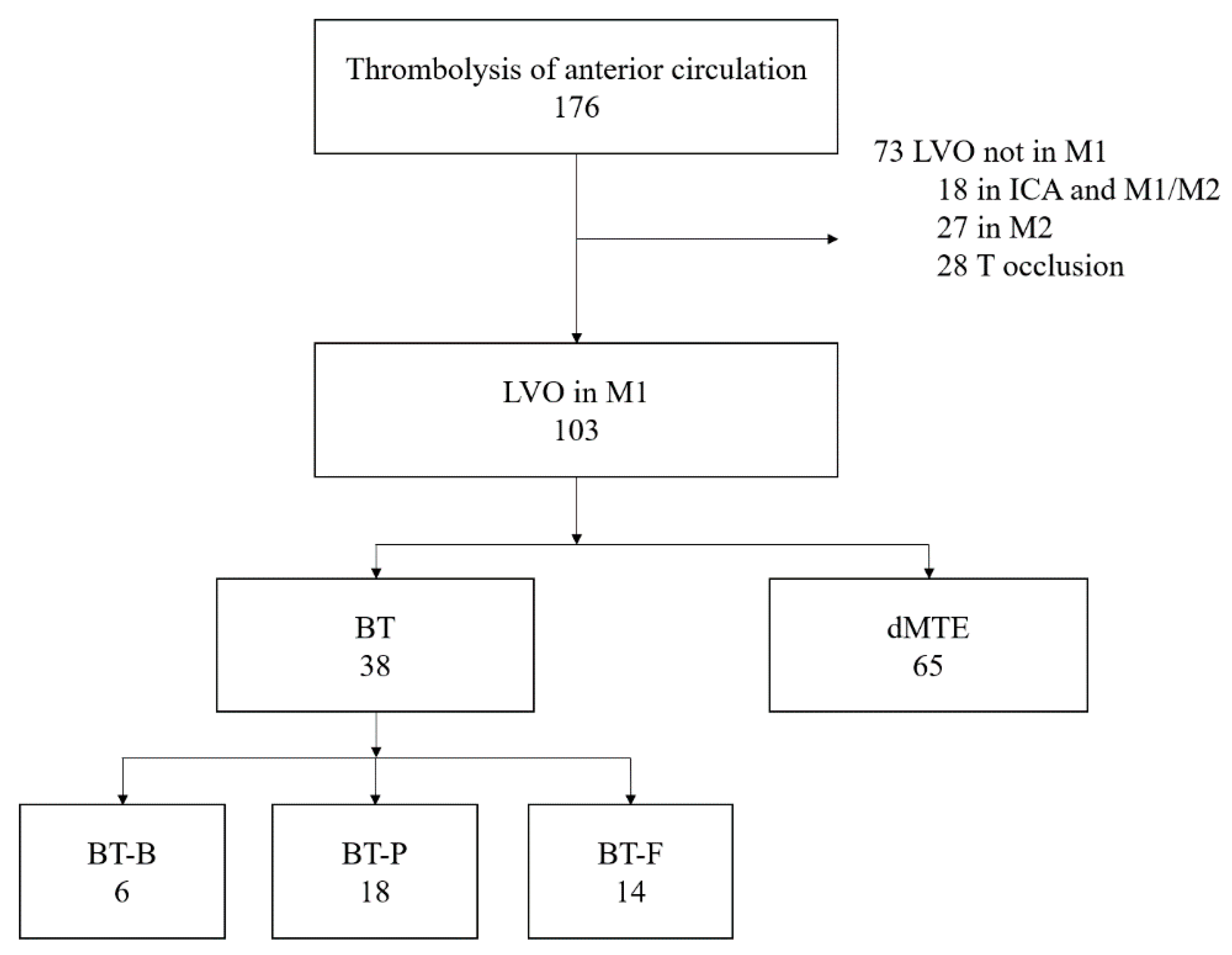
2. Materials and Methods
2.1. Outcome Measures
2.2. Statistical Analysis
3. Results
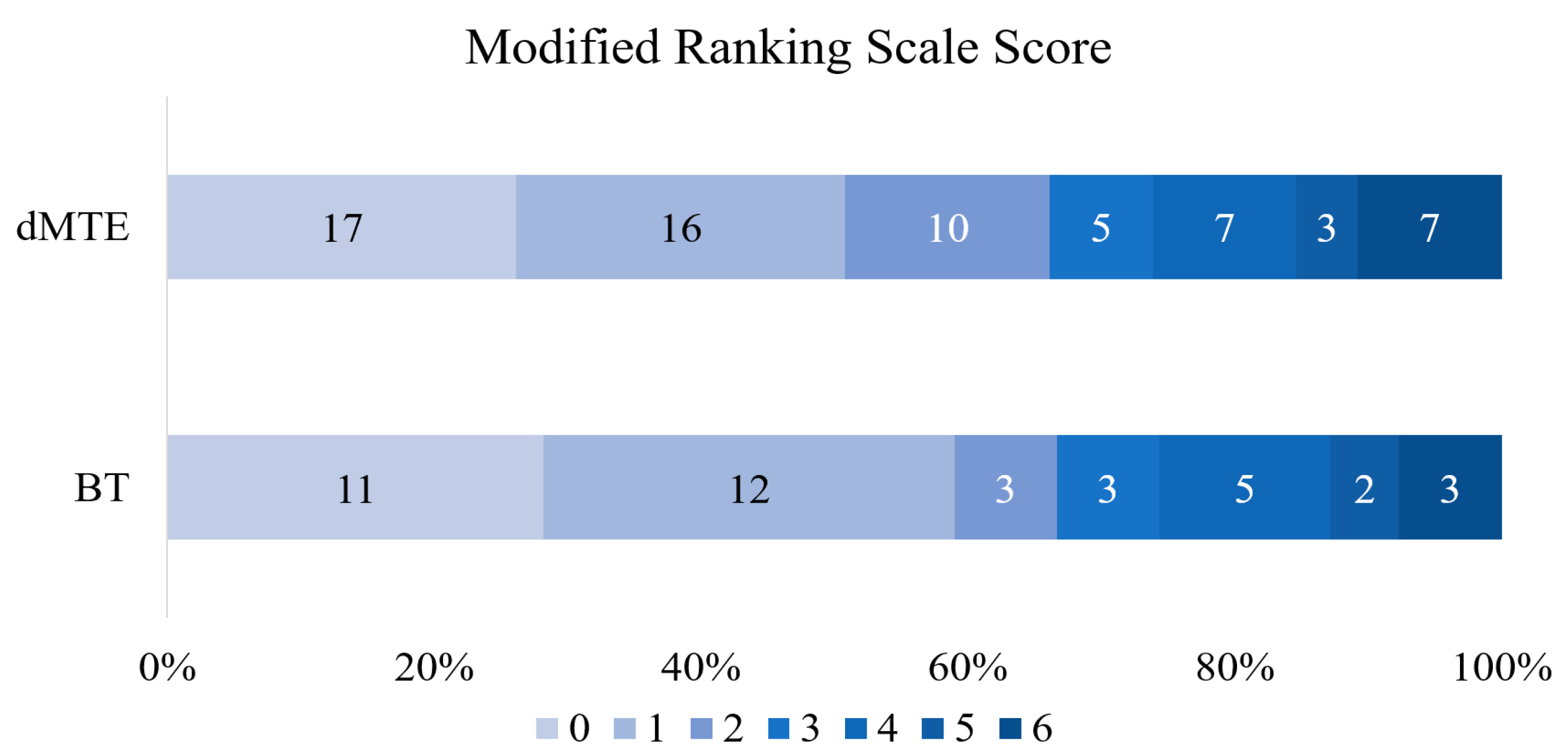
3.1. BT vs. dMTE
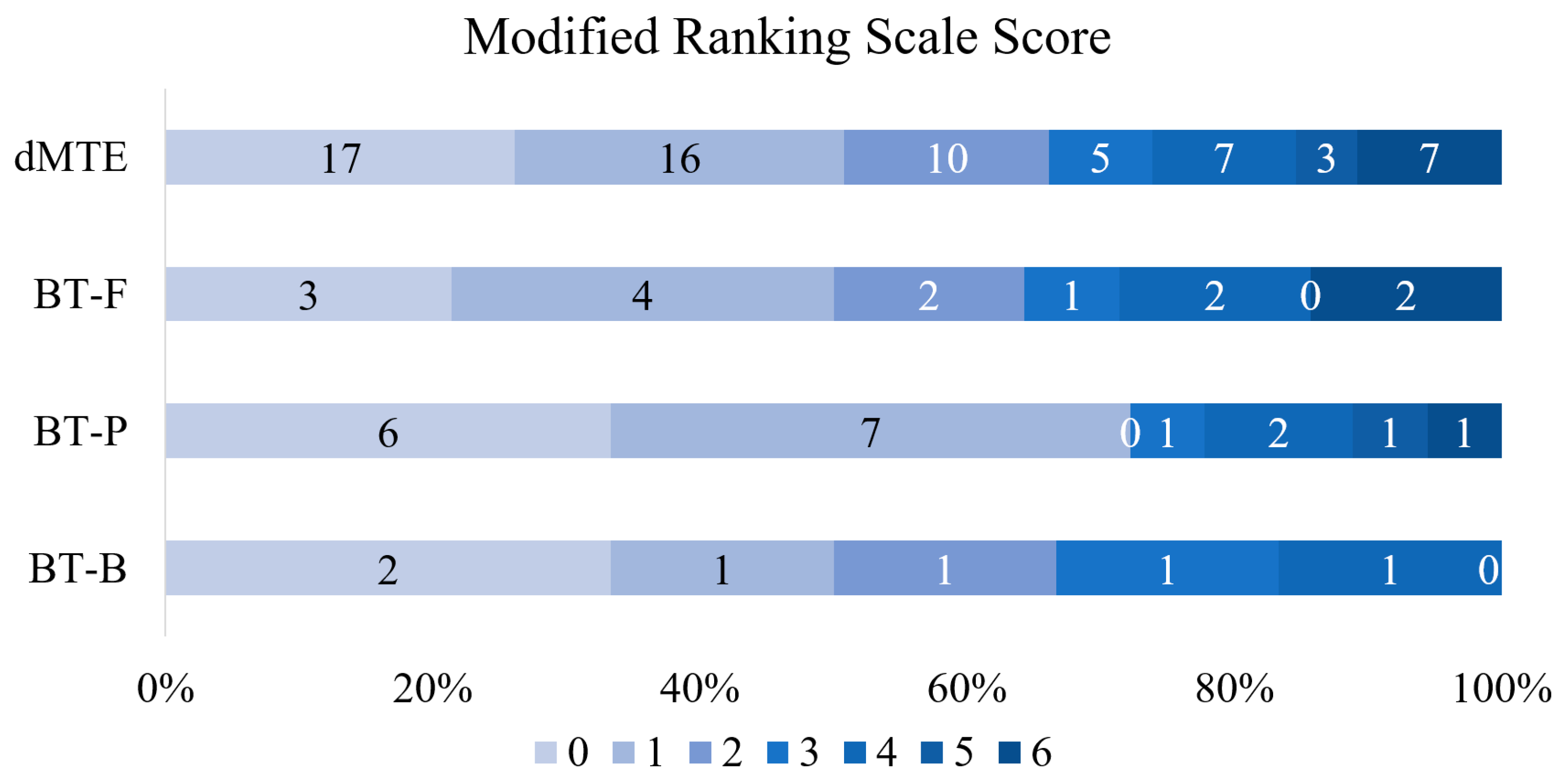
3.2. Various Dosages of r-tPA vs. dMTE
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Powers, W.J.; Derdeyn, C.; Biller, J.; Coffey, C.S.; Hoh, B.L.; Jauch, E.; Johnston, K.C.; Johnston, S.C.; Khalessi, A.A.; Kidwell, C.S.; et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients with Acute Ischemic Stroke Regarding Endovascular Treatment. Stroke 2015, 46, 3020–3035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellwald, S.; Weber, R.; Dobrocky, T.; Nordmeyer, S.; Jung, S.; Hadisurya, J.; Mordasini, P.; Mono, M.-L.; Stracke, C.P.; Sarikaya, H.; et al. Direct Mechanical Intervention Versus Bridging Therapy in Stroke Patients Eligible for Intravenous Thrombolysis. Stroke 2017, 48, 3282–3288. [Google Scholar] [CrossRef] [PubMed]
- Fischer, U.; Kaesmacher, J.; Molina, C.A.; Selim, M.H.; Alexandrov, A.V.; Tsivgoulis, G. Primary Thrombectomy in tPA (Tissue-Type Plasminogen Activator) Eligible Stroke Patients with Proximal Intracranial Occlusions. Stroke 2017, 49, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.; Parsons, M.W.; Oxley, T.; et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; De Miquel, M.A.; Molina, C.A.; Rovira, À.; Román, L.S.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Demchuk, A.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; Van Zwam, W.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.; Van Der Lugt, A.; De Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Yang, P.; Zhang, Y.; Zhang, L.; Zhang, Y.; Treurniet, K.M.; Chen, W.; Peng, Y.; Han, H.; Wang, J.; Wang, S.; et al. Endovascular Thrombectomy with or without Intravenous Alteplase in Acute Stroke. N. Engl. J. Med. 2020, 382, 1981–1993. [Google Scholar] [CrossRef]
- Phan, K.; Dmytriw, A.A.; Maingard, J.; Asadi, H.; Griessenauer, C.J.; Ng, W.; Kewagamang, K.; Mobbs, R.J.; Moore, J.M.; Ogilvy, C.S.; et al. Endovascular Thrombectomy Alone versus Combined with Intravenous Thrombolysis. World Neurosurg. 2017, 108, 850–858.e2. [Google Scholar] [CrossRef]
- Mistry, E.A.; Mistry, A.M.; Nakawah, M.O.; Chitale, R.V.; James, R.F.; Volpi, J.J.; Fusco, M.R. Mechanical Thrombectomy Outcomes with and without Intravenous Thrombolysis in Stroke Patients. Stroke 2017, 48, 2450–2456. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Damaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2018, 49, e138. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.; Higashida, R.; Wechsler, L.; Gent, M.; Rowley, H.; Kase, C.S.; Pessin, M.; Ahuja, A.; Callahan, F.; Clark, W.M.; et al. Intra-arterial Prourokinase for Acute Ischemic Stroke. JAMA 1999, 282, 2003–2011. [Google Scholar] [CrossRef]
- Kaesmacher, J.; Mordasini, P.; Arnold, M.; López-Cancio, E.; Cerdà, N.; Boeckh-Behrens, T.; Kleine, J.F.; Goyal, M.; Hill, M.D.; Pereira, V.M.; et al. Direct mechanical thrombectomy in tPA-ineligible and -eligible patients versus the bridging approach: A meta-analysis. J. NeuroInterv. Surg. 2018, 11, 20–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gariel, F.; Lapergue, B.; Bourcier, R.; Berge, J.; Barreau, X.; Mazighi, M.; Kyheng, M.; Labreuche, J.; Fahed, R.; Blanc, R.; et al. Mechanical Thrombectomy Outcomes with or without Intravenous Thrombolysis. Stroke 2018, 49, 2383–2390. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zi, W.; Hao, Y.; Yang, D.; Shi, Z.; Lin, M.; Wang, S.; Liu, W.; Wang, Z.; Guo, F.; et al. Direct endovascular treatment: An alternative for bridging therapy in anterior circulation large-vessel occlusion stroke. Eur. J. Neurol. 2017, 24, 935–943. [Google Scholar] [CrossRef]
- Broeg-Morvay, A.; Mordasini, P.; Bernasconi, C.; Bühlmann, M.; Pult, F.; Arnold, M.; Schroth, G.; Jung, S.; Mattle, H.P.; Gralla, J.; et al. Direct Mechanical Intervention Versus Combined Intravenous and Mechanical Intervention in Large Artery Anterior Circulation Stroke. Stroke 2016, 47, 1037–1044. [Google Scholar] [CrossRef]
- Weber, R.; Nordmeyer, H.; Hadisurya, J.; Heddier, M.; Stauder, M.; Stracke, P.; Berger, K.; Chapot, R. Comparison of outcome and interventional complication rate in patients with acute stroke treated with mechanical thrombectomy with and without bridging thrombolysis. J. NeuroInterv. Surg. 2016, 9, 229–233. [Google Scholar] [CrossRef]
- Kass-Hout, T.; Kass-Hout, O.; Mokin, M.; Thesier, D.M.; Yashar, P.; Orion, D.; Jahshan, S.; Hopkins, L.N.; Siddiqui, A.H.; Snyder, K.V.; et al. Is Bridging with Intravenous Thrombolysis of Any Benefit in Endovascular Therapy for Acute Ischemic Stroke? World Neurosurg. 2014, 82, e453–e458. [Google Scholar] [CrossRef]
- Ferrigno, M.; Bricout, N.; Leys, D.; Estrade, L.; Cordonnier, C.; Personnic, T.; Kyheng, M.; Hénon, H. Intravenous Recombinant Tissue-Type Plasminogen Activator: Influence on Outcome in Anterior Circulation Ischemic Stroke Treated by Mechanical Thrombectomy. Stroke 2018, 49, 1377–1385. [Google Scholar] [CrossRef]
- Kellert, L.; Wollenweber, F.A.; Thomalla, G.; Nolte, C.H.; Fiehler, J.; Ringleb, P.A.; Dorn, F. Thrombolysis management in thrombectomy patients: Real-life data from German stroke centres. Eur. Stroke J. 2017, 2, 356–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abilleira, S.; Ribera, A.; Cardona, P.; Rubiera, M.; López-Cancio, E.; Amaro, S.; Rodríguez-Campello, A.; Camps-Renom, P.; Cánovas, D.; De Miquel, M.A.; et al. Outcomes After Direct Thrombectomy or Combined Intravenous and Endovascular Treatment Are Not Different. Stroke 2017, 48, 375–378. [Google Scholar] [CrossRef]
- Guedin, P.; Larcher, A.; Decroix, J.-P.; Labreuche, J.; Dreyfus, J.-F.; Evrard, S.; Wang, A.; Graveleau, P.; Tassan, P.; Picó, F.; et al. Prior IV Thrombolysis Facilitates Mechanical Thrombectomy in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Rha, J.-H.; Saver, J.L. The Impact of Recanalization on Ischemic Stroke Outcome. Stroke 2007, 38, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Behrens, L.; Möhlenbruch, M.; Stampfl, S.; Ringleb, P.A.; Hametner, C.; Kellert, L.; Pham, M.; Herweh, C.; Bendszus, M.; Rohde, S. Effect of thrombus size on recanalization by bridging intravenous thrombolysis. Eur. J. Neurol. 2014, 21, 1406–1410. [Google Scholar] [CrossRef] [PubMed]
- Bhogal, P.; Bücke, P.; Ganslandt, O.; Bäzner, H.; Henkes, H.; Pérez, M.A. Mechanical thrombectomy in patients with M1 occlusion and NIHSS score ≤5: A single-centre experience. Stroke Vasc. Neurol. 2016, 1, 165–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| BT (n = 38) | dMTE (n = 65) | p Value | |
|---|---|---|---|
| Baseline characteristics | |||
| Sex female, n (%) | 22 (57.9) | 39 (60) | 0.835 |
| Age, y mean (SD) | 67.1 (9.6) | 68.4 (11.8) | 0.347 |
| NIHSS on admission, median (range) | 14 (4–20) | 13 (2–24) | 0.635 |
| ASPECTS on admission CT, median (range) | 9 (6–10) | 9 (6–10) | 0.689 |
| Clot length mm, mean (SD) | 14.8 (8.2) | 15.7 (7.1) | 0.452 |
| Vascular and other risk factors, n (%) | |||
| Hypertension | 34 (89.5) | 53 (81.5) | 0.286 |
| Diabetes mellitus | 4 (10.5) | 14 (21.5) | 0.158 |
| Atrial fibrillation | 21 (58.3) | 33 (50.8) | 0.468 |
| Coronary heart disease | 17 (44.7) | 32 (49.2) | 0.661 |
| Heart failure | 15 (39.5) | 23 (35.4) | 0.680 |
| Use of anticoagulants, n (%) | 3 * (7.89) | 17 (28.33) | 0.022 |
| Vital signs | |||
| Systolic blood pressure, mean (SD) | 150.7 (25.4) | 153.9 (28.2) | 0.983 |
| Diastolic blood pressure, mean (SD) | 85.0 (12.3) | 85.7 (12.3) | 0.321 |
| Mean blood pressure, mean (SD) | 109.8 (14.4) | 108.5 (17.8) | 0.485 |
| Pulse, mean (SD) | 80.2 (14.9) | 82.3 (23.8) | 0.524 |
| Treatment | |||
| Median time from neurologist’s consultation to MTE, h (IQR) | 01:23:00 (00:30:45) | 01:12:00 (00:27:30) | 0.113 |
| Median time from image to MTE, h (IQR) | 00:46:30 (00:37:45) | 00:42:30 (00:26:15) | 0.625 |
| Median time from symptom onset to recanalization, h (IQR) | 04:00:00 (01:12:30) | 03:50:30 (02:07:30) | 0.865 |
| Median time from symptom onset to MTE, h (IQR) | 03:10:00 (01:14:00 | 03:00:00 (02:19:00) | 0.994 |
| Median duration of MTE, h (IQR) | 00:42:30 (00:30:00) | 00:30:00 (00:25:00) | 0.025 |
| Duration of hospitalization, days, mean (SD) | 24.5 (4.4) | 21.4 (2.6) | 0.036 |
| Outcome | |||
| Successful reperfusion (TICI 2b-3), n (%) | 33 (86.8) | 58 (89.2) | 0.717 |
| Complete reperfusion (TICI 3), n (%) | 22 9 (57.9) | 35 (53.9) | 0.691 |
| NIHSS change during first 24 h, median (range) | 5 (−5, 17) | 6 (−6, 19) | 0.665 |
| Complications, n (%) | |||
| sICH | 4 (10.5) | 1 (1.5) | 0.121 |
| aICH | 4 (10.5) | 7 (10.8) | 0.831 |
| Distal embolization | 5 (13.2) | 8 (12.3) | 0.787 |
| Clinical outcome after 3 months | |||
| Functional independence (mRS 0–2), n (%) | 26 (68.4) | 43 (66.2) | 0.814 |
| Excellent clinical outcome (mRS 0–1), n (%) | 23 (60.5) | 33 (50.8) | 0.340 |
| Mortality at 90 days, n (%) | 2 (5.3) | 5 (7.7) | 0.638 |
| BT-B (n = 6) | BT-P (n = 18) | BT-F (n = 14) | dMTE (n = 65) | p Value | |
|---|---|---|---|---|---|
| Baseline characteristics | |||||
| Sex female, n (%) | 3 (50.0) | 12 (66.7) | 7 (50.0) | 39 (60.0) | 0.722 |
| Age, y mean (SD) | 65.3 (7.5) | 67.6 (10.3) | 67.4 (9.3) | 68.4 (11.8) | 0.649 |
| NIHSS on admission, median (range) | 9.5 (5–18) | 14 (4–20) | 13.5 (5–20) | 13 (2–24) | 0.581 |
| ASPECTS on admission CT, median (range) | 9 (7–10) | 9.5 (7–10) | 8.5 (6–10) | 9 (6–10) | 0.329 |
| Clot length mm, mean (SD) | 16.2 (8.3) | 13.6 (5) | 18.3 (8.4) | 14.8 (8.2) | 0.360 |
| Vascular and other risk factors, n (%) | |||||
| Hypertension | 5 (83.3) | 16 (88.9) | 13 (92.9) | 53 (81.5) | 0.697 |
| Diabetes mellitus | 1 (16.7) | 1 (5.6) | 2 (14.3) | 14 (21.5) | 0.459 |
| Atrial fibrillation | 2 (33.3) | 11 (61.1) | 8 (57.1) | 33 (50.8) | 0.729 |
| Coronary heart disease | 1 (16.7) | 9 (50.0) | 7 (50.0) | 32 (49.2 | 0.490 |
| Heart failure | 2 (33.3) | 7 (38.9) | 6 (42.9) | 23 (35.4) | 0.953 |
| Use of anticoagulants, n (%) | 0 (0.0) | 2 * (11.1) | 1 * (7.1) | 17 (28.3) | 0.134 |
| Vital signs | |||||
| Systolic blood pressure, mean (SD) | 146.0 (25.1) | 158.1 (28.7) | 153.7 (21.7) | 153.9 (28.2) | 0.711 |
| Diastolic blood pressure, mean (SD) | 82.6 (4.3) | 86.0 (13.4) | 90.6 (12.4) | 85.7 (12.3) | 0.449 |
| Mean blood pressure, mean (SD) | 103.7 (11.2) | 110.0 (16.3) | 111.6 (13.1) | 108.5 (17.8) | 0.608 |
| Pulse, mean (SD) | 71.6 (6.3) | 83.9 (19.0) | 78.3 (8.2) | 82.3 (23.8) | 0.402 |
| Treatment | |||||
| Median time from neurologist’s consultation to MTE, h (IQR) | 00:59:00 (00:31:00) | 01:21:00 (00:27:00) | 01:34:00 (00:45:00) | 01:12:00 (00:27:30) | 0.017 |
| Median time from image to MTE, h (IQR) | 00:28:00 (00:24:00) | 00:38:00 (00:20:00) | 01:13:00 (00:39:00) | 00:42:30 (00:26:15) | 0.005 |
| Median time from symptom onset to MTE, h (IQR) | 02:24:30 (01:50:00) | 03:05:00 (01:03:00) | 03:30:00 (01:17:00) | 03:00:00 (02:15:00) | 0.792 |
| Median time from symptom onset to r-tPA, h (IQR) | 01:57:00 (02:10:15) | 02:22:30 (01:26:15) | 01:49:00 (00:53:30) | 0.280 | |
| Median time from symptom onset to recanalization, h (IQR) | 03:22:00 (01:47:00) | 03:55:00 (01:04:00) | 04:12:00 (01:33:00) | 03:50:30 (02:07:30) | 0.531 |
| Median duration of MTE, h (IQR) | 00:50:00 (00:32:00) | 00:40:00 (00:35:00) | 00:45:00 (00:30:00) | 00:30:00 (00:25:00) | 0.125 |
| Duration of hospitalization (days), mean (SD) | 28.3 (14.6) | 21.3 (5.5) | 27.0 (7.9) | 21.4 (2.6) | 0.928 |
| Outcome | |||||
| Successful reperfusion (TICI 2b-3), n (%) | 5 (83.3) | 15 (83.3) | 13 (92.9) | 58 (89.2) | 0.825 |
| Complete reperfusion (TICI 3), n (%) | 3 (50.0) | 11 (61.1) | 8 (57.1) | 35 (53.8) | 0.943 |
| NIHSS change during first 24 h, median (range) | 6 (1–13) | 6.8 (−5, 17) | 6 (−5, 16) | 6 (−6, 19) | 0.990 |
| Complications, n (%) | |||||
| sICH | 0 (0) | 0 (0) | 4 (28.6) | 1 (1.5) | <0.001 |
| aICH | 0 (0) | 1 (5.6) | 3 (21.4) | 7 (10.8) | 0.410 |
| Distal embolization | 1 (16.7) | 3 (16.7) | 1 (7.1) | 8 (12.3) | 0.865 |
| Clinical outcome after 3 months | |||||
| Functional independence (mRS 0–2), n (%) | 4 (66.7) | 13 (72.2) | 9 (64.3) | 43 (66.2) | 0.427 |
| Excellent clinical outcome (mRS 0–1), n (%) | 3 (50) | 13 (72.2) | 7 (50) | 33 (50.8) | 0.926 |
| Mortality at 90 days, n (%) | 0 (0) | 1 (5.6) | 1 (7.1) | 5 (7.7) | 0.905 |
| Groups Pairs | dMTE and BT-B | dMTE and BT-P | dMTE and BT-F | BT-B and BT-P | BT-B and BT-F | BT-P and BT-F | |
|---|---|---|---|---|---|---|---|
| Dependent Variable | |||||||
| sICH | 1.000 | 1.000 | <0.001 | 1.000 | 0.040 | 0.001 | |
| Median time from neurologist’s consultation to MTE | 1.000 | 1.000 | 0.036 | 0.719 | 0.041 | 0.597 | |
| Median time from image to MTE | 0.932 | 1.000 | 0.029 | 1.000 | 0.019 | 0.015 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurminas, M.; Berūkštis, A.; Misonis, N.; Blank, K.; Tamošiūnas, A.E.; Jatužis, D. Intravenous r-tPA Dose Influence on Outcome after Middle Cerebral Artery Ischemic Stroke Treatment by Mechanical Thrombectomy. Medicina 2020, 56, 357. https://doi.org/10.3390/medicina56070357
Kurminas M, Berūkštis A, Misonis N, Blank K, Tamošiūnas AE, Jatužis D. Intravenous r-tPA Dose Influence on Outcome after Middle Cerebral Artery Ischemic Stroke Treatment by Mechanical Thrombectomy. Medicina. 2020; 56(7):357. https://doi.org/10.3390/medicina56070357
Chicago/Turabian StyleKurminas, Marius, Andrius Berūkštis, Nerijus Misonis, Karmela Blank, Algirdas Edvardas Tamošiūnas, and Dalius Jatužis. 2020. "Intravenous r-tPA Dose Influence on Outcome after Middle Cerebral Artery Ischemic Stroke Treatment by Mechanical Thrombectomy" Medicina 56, no. 7: 357. https://doi.org/10.3390/medicina56070357
APA StyleKurminas, M., Berūkštis, A., Misonis, N., Blank, K., Tamošiūnas, A. E., & Jatužis, D. (2020). Intravenous r-tPA Dose Influence on Outcome after Middle Cerebral Artery Ischemic Stroke Treatment by Mechanical Thrombectomy. Medicina, 56(7), 357. https://doi.org/10.3390/medicina56070357