Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application

 ,
,  ,
,
Abstract
:
1. Introduction
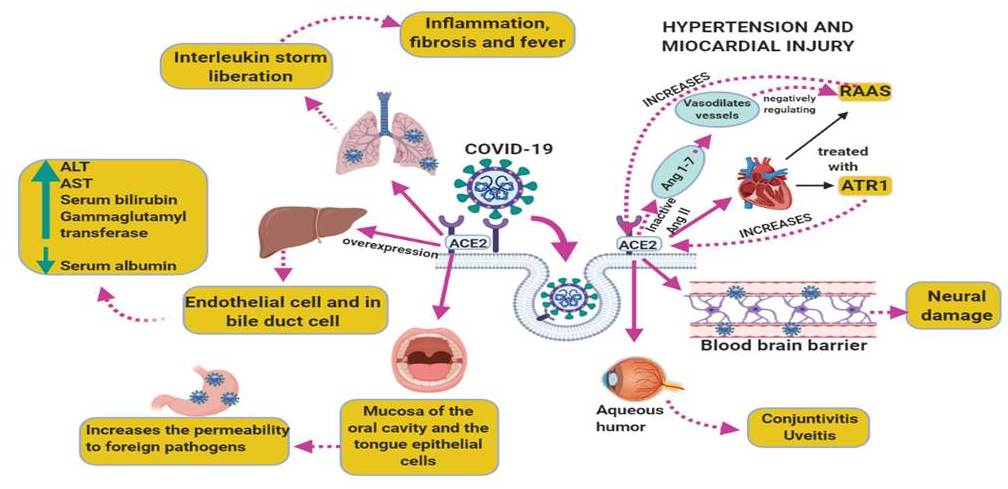
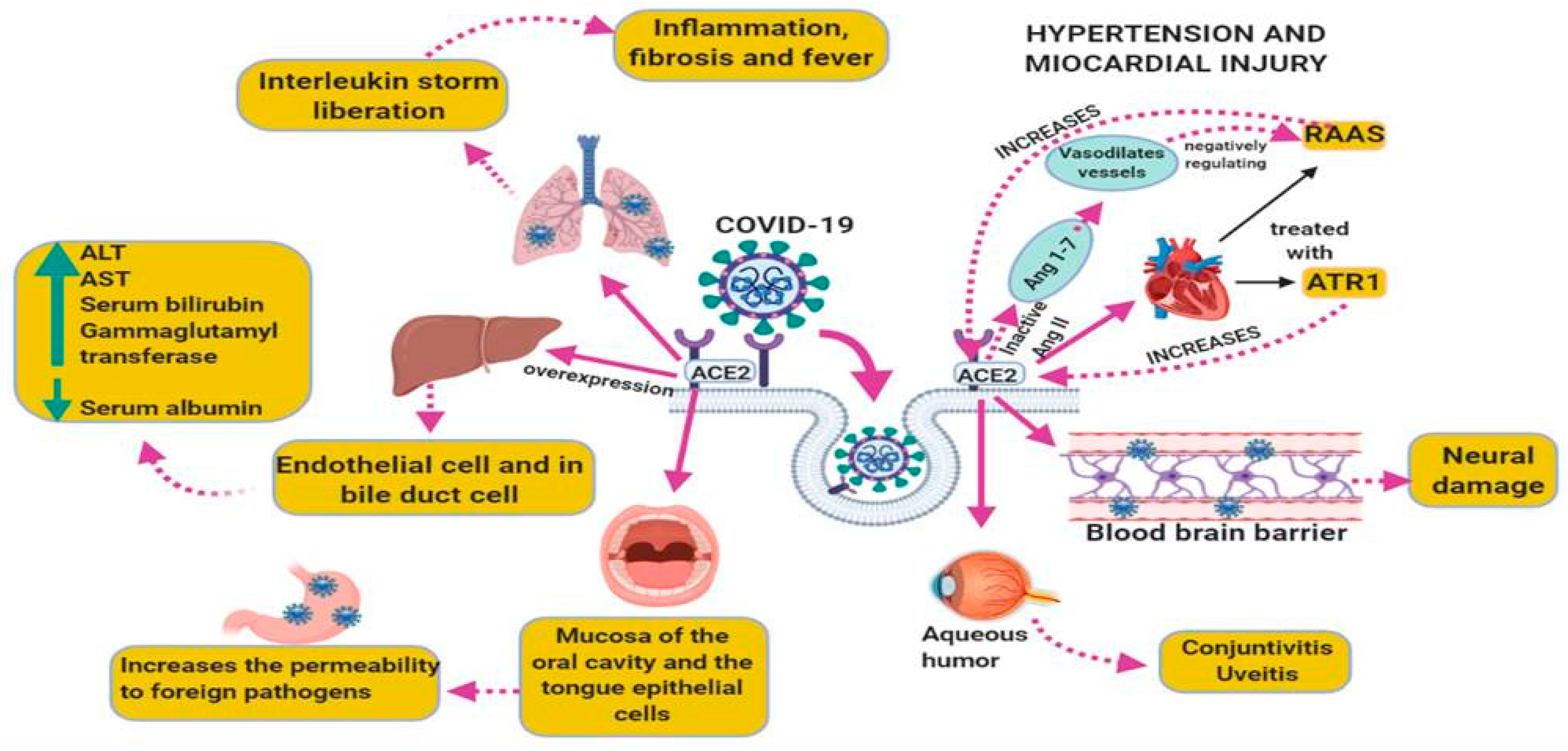
2. Inter-Relations between the Virus and the Host Cell Interaction of the Mechanism with the Comorbidities Found in the Severe Forms of COVID-19
2.1. COVID-19 and CVD (Hypertension and Myocardial Injury)
2.2. COVID-19 and Liver Diseases
2.3. COVID-19 and the Respiratory System and Its Association with the Inflammatory Process
2.4. SARS-Cov-2 Associated with Oxidative Stress and Inflammatory Process
3. Treatment of COVID-19
Chloroquine and Hydroxychloroquine
4. Drawbacks of Chloroquine and Hydroxychloroquine
5. Anti-Inflammatory Drugs
6. Corticosteroids
7. Arbidol
8. Danoprevir
9. Importance of Choosing Therapies According to Comorbidities
10. Proposal of Adjuvant Antioxidant Therapy by Our Group
11. N-acetylcysteine
12. Vitamin C and E
13. Melatonin
14. Quercetin
15. Pentoxifylline
Proposal of Therapeutic Management with Antioxidants
16. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vankadari, N.; Wilce, J.A. Emerging WuHan (COVID-19) Coronavirus: Glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26. Emerg. Microbes Infect. 2020, 9, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, I.M.; Abdelmalek, D.H.; Elshahat, M.E.; Elfiky, A.A. COVID-19 Spike-host cell receptor GRP78 binding site prediction. J. Infect. 2020, 80, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Neuman, B.W.; Buchmeier, M.J. Supramolecular architecture of the coronavirus particle. Adv. Virus Res. 2016, 96, 1–27. [Google Scholar] [PubMed]
- Qu, C.; Zhang, S.; Li, Y.; Wang, Y.; Peppelenbosch, M.P.; Pan, Q. Mitochondria in the biology, pathogenesis and treatment of hepatitis virus infections. Rev. Med. Virol. 2019, 29, 2075. [Google Scholar] [CrossRef]
- Mondal, S.P.; Cardona, C. Microbiología Veterinaria; Stanchi, N.O., Ed.; Inter-Médica: Buenos Aires, Argentina, 2007; ISBN 97-950-555-321-12007. [Google Scholar]
- Seah, I.; Agrawal, R. Can the coronavirus disease 2019 (COVID-19) affect the eyes. A review of coronaviruses and ocular implications in humans and animals. Ocul. Immunol. Inflamm. 2020, 28, 391–395. [Google Scholar] [CrossRef]
- Li, C.; Yang, Y.; Ren, L. Genetic Evolution Analysis of 2019 Novel Coronavirus and Coronavirus from Other Species. Infect. Genet. Evol. 2020, 82, 104285. [Google Scholar] [CrossRef]
- Feng, H.; Yu, D.; Weina, L. Coronavirus Disease 2019 (COVID-19): What We Know. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Singhal, T. Review of Coronavirus Disease-2019 (COVID-19). Indian. J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Conner, E.M.; Grisham, M.B. Inflammation, free radicals and antioxidants. Nutrition 1996, 12, 274–277. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Nai-Huei, W.; Nitsche, A.; et al. SARS-CoV-2 cell Entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Abdul-Hafez, A.; Mohamed, T.; Omar, H.; Shemis, M.; Uhal, B.D. The renin angiotensin system in liver and lung: Impact and therapeutic potential in organ fibrosis. J. Lung Pulm. Respir. Res. 2018, 5, 00160. [Google Scholar] [PubMed] [Green Version]
- Rubio-Ruiz, M.E.; Hafidi-El, M.; Perez-Torres, I.; Banos, G.; Guarner, V. Medicinal agents and metabolic síndrome. Curr. Med. Chem. 2013, 20, 2626–2640. [Google Scholar] [CrossRef] [PubMed]
- Driggin, E.; Madhavan, M.V.; Bikdeli, B.; Chuich, T.; Laracy, J.; Biondi-Zoccai, G. Cardiovascular considerations for patients, health care workers and health systems during the COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2352–2371. [Google Scholar] [CrossRef]
- Guan, G.W.; Gao, L.; Wang, J.W.; Wen, X.J.; Mao, T.H.; Peng, S.W.; Zhang, T.; Chen, X.M.; Lu, F.M. Exploring the mechanism of liver enzyme abnormalities in patients with novel coronavirus-infected pneumonia. Zhonghua. Gan Zang Bing Za Zhi 2020, 28, 002. [Google Scholar]
- Lake, M.A. What We Know So Far: COVID-19 Current Clinical Knowledge and Research. Clin. Med. (Lond.) 2020, 20, 124–127. [Google Scholar] [CrossRef] [Green Version]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection. Lancet Respir. Med. 2020, 8, 21. [Google Scholar] [CrossRef]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [Green Version]
- Smyth, L.J.; Cañadas-Garre, M.; Cappa, R.C.; Maxwell, A.P.; McKnight, A.J. Genetic associations between genes in the renin-angiotensin-aldosterone system and renal disease: A systematic review and meta-analysis. BMJ Open 2019, 9, 026777. [Google Scholar] [CrossRef] [Green Version]
- Ishiyama, Y.; Gallagher, P.E.; Averill, D.B.; Tallant, E.A.; Brosnihan, K.B.; Ferrario, C.M. Upregulation of angiotensin-converting enzyme 2 after myocardial infarction by blockade of angiotensin II receptors. Hypertension 2004, 43, 970–976. [Google Scholar] [CrossRef] [Green Version]
- Furuhashi, M.; Mita, T.; Moniwa, N.; Hoshina, K.; Ishimura, S.; Fuseya, T.; Yuki Watanabe, H.Y.; Yoshida, H.; Shimamoto, K.; Miura, T. Angiotensin II receptor blockers decrease serum concentration of fatty acid-binding protein 4 in patients with hypertension. Hypertens. Res. 2015, 38, 252–259. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Wei, D.; et al. Crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Boettler, T.; Newsome, P.N.; Mondelli, M.U.; Maticic, M.; Cordero, E.; Cornberg, M.; Berg, T. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper. JHEP Rep. 2020, 2, 100113. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Shi, L.; Fu-Sheng, W. Liver injury in COVID-19: Management and challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and Liver. J. Hepatol. 2020. [Google Scholar] [CrossRef]
- Hu, L.L.; Wang, W.J.; Zhu, Q.J.; Yang, L. Novel coronavirus pneumonia related liver injury: Etiological analysis and treatment strategy. Zhonghua Gan Zang Bing Za Zhi 2020, 28, 1. [Google Scholar]
- Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar]
- Banales, J.M.; Huebert, R.C.; Karlsen, T.; Strazzabosco, M.; LaRusso, N.F.; Gores, G.J. Cholangiocyte pathobiology. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 269–281. [Google Scholar] [CrossRef]
- Ling, X.; Jia, L.; Mengji, L.; Dongliang, Y.; Xin, Z. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar]
- Bangash, M.N.; Patel, J.; Parekh, D. COVID-19 and the liver: Little cause for concern. Lancet Gastroenterol. Hepatol. 2020, 5, 529–530. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.; Ronconi, G.; Caraffa, A. Induction of pro-Inflammatory cytokines (IL-1 and IL-6) and lung inflammation by coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 1. [Google Scholar] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, 248. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Procalcitonin in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chim. Acta 2020, 505, 190–191. [Google Scholar] [CrossRef] [PubMed]
- Ricciardolo, F.L.; Caramori, G.; Ito, K.; Capelli, A.; Brun, P.; Abatangelo, G.; Papi, A.; Chung, K.F.; Adcock, I.; Barnes, P.J.; et al. Nitrosative stress in the bronchial mucosa of severe chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2005, 116, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Ito, K.; Adcock, I.M. Corticosteroid resistance in chronic obstructive pulmonary disease: Inactivation of histone deacetylase. Lancet 2004, 363, 731–733. [Google Scholar] [CrossRef]
- Singh, V.P.; Aggarwal, R.; Singh, S.; Banik, A.; Ahmad, T.; Patnaik, B.R.; Nappanveettil, G.; Singh, K.P.; Aggarwal, M.L.; Ghosh, B.; et al. Metabolic syndrome is associated with increased oxo-nitrative stress and asthma-like changes in lungs. PLoS ONE 2015, 10, e0129850. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Roche, L.; Mesta, F. Oxidative stress as key player in severe acute respiratory syndrome coronavirus (SARS-CoV) infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef]
- Russell, J.A. Management of sepsis. N. Engl. J. Med. 2006, 355, 1699–1713. [Google Scholar] [CrossRef] [Green Version]
- Rivers, E.P.; McIntyre, L.; Morro, D.C.; Rivers, K.K. Early and innovative interventions for severe sepsis and septic shock: Taking advantage of a window of opportunity. CMAJ 2005, 173, 1054–1065. [Google Scholar] [CrossRef] [Green Version]
- Clapp, B.R.; Hingorani, A.D.; Kharbanda, R.K.; Mohamed-Ali, V.; Stephens, J.W.; Vallance, P.; MacAllister, R.J. Inflammation-induced endothelial dysfunction involves reduced nitric oxide bioavailability and increased oxidant stress. Cardiovasc. Res. 2004, 64, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Manzano-Pech, L.; Rubio-Ruíz, M.E.; Soto, M.E.; Guarner-Lans, V. Nitrosative stress and its association with cardiometabolic disorders. Molecules 2020, 25, 2555. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Ying, Y. The Inhibitory effect of curcumin on virus-induced cytokine storm and its potential use in the associated severe pneumonia. Front. Cell Dev. Biol. 2020, 8, 479. [Google Scholar] [CrossRef]
- Protti, A.; Singer, M. Bench-to-bedside review: Potential strategies to protect or reverse mitochondrial dysfunction in sepsis-induced organ failure. Crit. Care 2006, 10, 228–232. [Google Scholar] [CrossRef] [Green Version]
- Dan, L.; Xiaodan, L.; Yonggang, Z.; Joey, K.; Ling, L.; Yiyi, Z.; Xu, C.; Li, Q.; Sun, X.; Tian, H.; et al. Chloroquine and hydroxychloroquine are associated with reduced cardiovascular risk: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2018, 12, 1685–1695. [Google Scholar]
- Colson, P.; Rolain, J.M.; Raoult, D. Chloroquine for the 2019 novel coronavirus SARS-CoV-2. Int. J. Antimicrob. Agents 2020, 55, 105923. [Google Scholar] [CrossRef]
- Touret, F.; de Lamballerie, X. Of chloroquine and COVID-19. Antivir. Res. 2020, 177, 104762. [Google Scholar] [CrossRef] [PubMed]
- Al-Bari, M.A.A. Targeting endosomal acidification by chloroquine analogs as a promising strategy for the treatment of emerging viral diseases. Pharmacol. Res. Perspec. 2017, 5, 00293. [Google Scholar] [CrossRef]
- Routy, J.P.; Angel, J.B.; Patel, M.; Kanagaratham, C.; Radzioch, D.; Kema, I.; Gilmore, N.; Ancuta, P.; Singer, J.; Jenabian, M.A. Assessment of chloroquine as a modulator of immune activation to improve CD4 recovery in immune nonresponding HIV-infected patients receiving antiretroviral therapy. HIV Med. 2015, 16, 48–56. [Google Scholar] [CrossRef]
- Van den Borne, B.E.; Dijkmans, B.A.; de Rooij, H.H.; le Cessie, S.; Verweij, C.L. Chloroquine and hydroxychloroquine equally affect tumor necrosis factor-alpha, interleukin 6 and interferon-gamma production by peripheral blood mononuclear cells. J. Rheumatol. 1997, 24, 55–60. [Google Scholar]
- Devaux, C.A.; Rolain, J.; Colson, P.; Raoult, D. New insights on the antiviral effects of chloroquine against coronavirus: What to expect for COVID-19. Int. J. Antimicrob. Agents 2020, 105938. [Google Scholar] [CrossRef] [PubMed]
- Cortegiani, A.; Ingoglia, G.; Ippolito, M.; Giarratano, A.; Einav, S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J. Crit. Care 2020, 57, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Rolain, J.M.; Lagier, J.C.; Brouqui, P.; Raoult, D. Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105932. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.K.; Shilton, B.H. Chloroquine binding reveals flavin redox switch function of quinone reductase 2. J. Biol. Chem. 2013, 288, 11242–11251. [Google Scholar] [CrossRef] [Green Version]
- Blaum, B.S.; Stehle, T. Sialic acids in nonenveloped virus infections. Adv. Carbohydr. Chem. Biochem. 2019, 76, 65–111. [Google Scholar]
- Sahraei, Z.; Shabani, M.; Shokouhi, S.; Saffaei, A. Aminoquinolines against coronavirus disease 2019 (COVID-19): Chloroquine or hydroxychloroquine. Int. J. Antimicrob. Agents 2020, 55, 105945. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 20, 105949. [Google Scholar] [CrossRef]
- Haeusler, I.L.; Chan, X.H.S.; Guérin, P.J.; White, N.J. The arrhythmogenic cardiotoxicity of the quinoline and structurally related antimalarial drugs: A systematic review. BMC Med. 2018, 16, 200. [Google Scholar] [CrossRef]
- McGhie, T.K.; Harvey, P.; Su, J.; Anderson, N.; Tomlinson, G.; Touma, Z. Electrocardiogram abnormalities related to anti-malarials in systemic lupus erythematosus. Clin. Exp. Rheumatol. 2018, 36, 545–551. [Google Scholar]
- Zuo, X.; Meng, F.; Wu, F.; Zhao, X.; Li, C.; Cheng, G.; Qin, F.X. Combinatorial screening of a panel of FDA-approved drugs identifies several candidates with anti-Ebola activities. Biochem. Biophys. Res. Commun. 2020, 522, 862–868. [Google Scholar]
- Dyer, O. Two Ebola treatments halve deaths in trial in DRC outbreak. BMJ 2019, 366, l5140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchesnokov, E.P.; Feng, J.Y.; Porter, D.P.; Götte, M. Mechanism of inhibition of Ebola virus RNA-dependent RNA polymerase by remdesivir. Viruses 2019, 11, 326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, C.J.; Tchesnokov, E.P.; Feng, J.Y.; Porter, D.P.; Gotte, M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from middle east respiratory syndrome coronavirus. J. Biol. Chem. 2020, 295, 4773–4779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Tawfiq, J.A.; Al-Homoud, A.H.; Memish, Z.A. Remdesivir as a possible therapeutic option for the COVID-19. Travel Med. Infect. Dis. 2020, 34, 101615. [Google Scholar] [CrossRef]
- Stebbing, J.; Phelan, A.; Griffin, I. COVID-19: Combining antiviral and anti-inflammatory treatments. Mikrobiol. Epidemiol. Immunobiol. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Cunningham, A.C.; Goh, H.P.; Koh, D. Treatment of COVID-19: Old tricks for new challenges. Crit. Care 2020, 24, 91. [Google Scholar] [CrossRef] [Green Version]
- Russell, C.D.; Millar, J.E.; Baillie, J.K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef] [Green Version]
- Blaising, J.; Polyak, S.J.; Pécheur, E.I. Arbidol as a broad-spectrum antiviral: An update. Antivir. Res. 2014, 107, 84–94. [Google Scholar] [CrossRef]
- Boriskin, Y.S.; Leneva, I.A.; Pécheur, E.I.; Polyak, S.J. Arbidol: A broad-spectrum antiviral compound that blocks viral fusion. Curr. Med. Chem. 2008, 15, 997–1005. [Google Scholar] [CrossRef]
- Gagarinova, V.M.; Ignat’eva, G.S.; Sinitskaia, L.V.; Ivanova, A.M.; Rodina, M.A.; Tur’eva, A.V. The New Chemical Preparation Arbidol: Its Prophylactic Efficacy During Influenza Epidemics. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 1993, 5, 40–43. [Google Scholar]
- Shuster, A.M.; Shumilov, V.I.; Shevtsov, V.A.; Mar’in, G.G.; Kozlov, V.N. Arbidol used in the prophylaxis of acute respiratory viral infections and their complications in servicemen. Voen. Med. Zhurnal 2004, 325, 44–45. [Google Scholar]
- Treatment and Prevention of Traditional Chinese Medicines (TCMs) on2019-nCoV Infection. Xiyanping (ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2020 Mar 12–Identifier NCT04275388). Available online: https://clinicaltrials.gov/ct2/show/NCT04251871 (accessed on 5 February 2020).
- Xiyanping Injection for the Treatment of New Coronavirus Infected Pneumonia. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2020 Mar 12–Identifier NCT04295551. Available online: https://clinicaltrials.gov/ct2/show/NCT04275388 (accessed on 19 February 2020).
- Markham, A.; Keam, S.J. Danoprevir: First Global Approval. Drugs 2018, 78, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Multicenter Clinical Study on the Efficacy and Safety of Xiyanping Injection in the Treatment of the New Coronavirus Infection Pneumonia (General and Severe), Danoprevir-Ritonavir (ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2020 Mar 12–Identifier NCT04291729. Available online: https://clinicaltrials.gov/ct2/show/NCT04295551 (accessed on 4 March 2020).
- Okubo, K.; Isono, M.; Asano, T.; Sato, A. Lopinavir-ritonavir combination induces endoplasmic reticulum stress and kills urological cancer cells. Anticancer Res. 2019, 39, 5891–5901. [Google Scholar] [CrossRef]
- Gao, C.; Wang, Y.; Gu, X.; Shen, X.; Zhou, D.; Zhou, S.; Huang, J.A.; Cao, B.; Guo, Q. Association between cardiac injury and mortality in hospitalized patients infected with avian influenza A (H7N9). Virus. Crit. Care Med. 2020, 48, 451–458. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Li, C.; Huang, A.; Xia, S.; Lu, S.; Shi, Z.; Lu, L.; Jiang, S.; Yang, Z.; Wu, Y.; et al. Potent binding of 2019 novel coronavirus spike protein by a SARS coronavirus-specific human monoclonal antibody. Emerg. Microbes Infect. 2020, 9, 382–385. [Google Scholar] [CrossRef] [Green Version]
- Funk, D.J.; Parrillo, J.E.; Kumar, A. Sepsis and septic shock: A history. Crit. Care Clin. 2009, 25, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Sotoudeh, R.; Hadjzadeh, M.A.; Gholamnezhad, Z.; Aghaei, A. The anti-diabetic and antioxidant effects of a combination of Commiphora mukul, Commiphora myrrha and Terminalia chebula in diabetic rats. Avicenna. J. Phytomed. 2019, 9, 454–464. [Google Scholar]
- Tarazi, R.C. Sympathomimetic agents in the treatment of shock. Ann. Intern. Med. 1974, 81, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Chalupsky, K.; Lobysheva, I.; Nepveu, F.; Gadea, I.; Beranova, P.; Entlicher, G.; Stoclet, J.C.; Muller, B. Relaxant effect of oxime derivatives in isolated rat aorta: Role of nitric oxide (NO) formation in smooth muscle. Biochem. Pharmacol. 2004, 67, 1203–1214. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Djillali, B.M.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Jean-Louis, V.; Guyatt, G.; Angus, C.D.; Abraham, E.; Bernard, G.; Bombardier, C.; Calandra, T.; Jørgensen, H.S.; Sylvester, R.; et al. Outcome measures for clinical research in sepsis: A report of the 2nd Cambridge colloquium of the International sepsis forum. Crit. Care Med. 2005, 33, 1708–1716. [Google Scholar] [CrossRef]
- Lovat, R.; Preiser, J.C. Antioxidant therapy in intensive care. Curr. Opin. Crit. Care 2003, 9, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Galvão, A.M.; de Andrade, A.D.; de Souza Maia, M.B.; Ramos da Silva, K.E.; Bezerra, A.; Melo, J.F.; Morais, N.G.; Costa, T.B.; Castro, C.M. Antioxidant supplementation for the treatment of acute lung injury: A meta-analysis. Rev. Bras. Ter. Intensiva 2011, 23, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.J.; Biswas, R.S.; Mehta, H.J.; Joo, M.; Sadikot, R.T. Alternative and natural therapies for acute lung injury and acute respiratory distress syndrome. BioMed Res. Int. 2018, 2018, 2476824. [Google Scholar] [CrossRef] [Green Version]
- Kawabata, K.; Hagio, T.; Matsuoka, S. The role of neutrophil elastase in acute lung injury. Eur. J. Pharmacol. 2002, 451, 1–10. [Google Scholar] [CrossRef]
- Rahman, I.; MacNee, W. Regulation of redox glutathione levels and gene transcription in lung inflammation: Therapeutic approaches. Free Radic. Biol. Med. 2000, 28, 1405–1420. [Google Scholar] [CrossRef]
- Koksel, O.; Cinel, I.; Tamer, L.; Cinel, L.; Ozdulger, A.; Kanik, A.; Ercan, B.; Oral, U. N-acetylcysteine inhibits peroxynitrite-mediated damage in oleic acid-induced lung injury. Pulm. Pharmacol. Ther. 2004, 17, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Sciuto, A.M.; Strickland, P.T.; Kennedy, T.P.; Gurtner, G.H. Protective effects of N acetylcysteine treatment after phosgene exposure in rabbits. Am. J. Respir. Crit. Care Med. 1995, 151, 768–772. [Google Scholar] [CrossRef]
- Fan, J.; Shek, P.N.; Suntres, Z.E.; Li, Y.H.; Oreopoulos, G.D.; Rotstein, O.D. Liposomal antioxidants provide prolonged protection against acute respiratory distress syndrome. Surgery 2000, 128, 332–338. [Google Scholar] [CrossRef]
- Christofidou-Solomidou, M.; Muzykantov, V.R. Antioxidant strategies in respiratory medicine. Treat. Res. Med. 2006, 5, 47–78. [Google Scholar] [CrossRef] [PubMed]
- Moradi, M.; Mojtahedzadeh, M.; Mandegari, A.; Soltan-Sharifi, M.S.; Najafi, A.; Khajavi, M.R.; Hajibabayee, M.; Ghahremani, M.H. The role of glutathione-S-transferase polymorphisms on clinical outcome of ALI/ARDS patient treated with N-acetylcysteine. Respir. Med. 2009, 103, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peake, S.L.; Moran, J.L.; Leppard, P.I. N-acetyl-L-cysteine depresses cardiac performance in patients with septic shock. Crit. Care Med. 1996, 24, 1302–1310. [Google Scholar] [CrossRef]
- Spapen, H.; Zhang, H.; Demanet, C.; Vleminckx, W.; Vincent, J.L.; Huyghens, L. Does N-acetyl-L-cysteine influence cytokine response during early human septic shock. Chest 1998, 113, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molnár, Z.; Shearer, E.; Lowe, D. N-Acetylcysteine treatment to prevent the progression of multisystem organ failure: A prospective, randomized, placebo-controlled study. Crit. Care Med. 1999, 27, 1100–1104. [Google Scholar] [CrossRef]
- Rank, N.; Michel, C.; Haertel, C.; Lenhart, A.; Welte, M.; Meier-Hellmann, A.; Spies, C. N-acetylcysteine increases liver blood flow and improves liver function in septic shock patients: Results of a prospective, randomized, double-blind study. Crit. Care Med. 2000, 2, 3799–3807. [Google Scholar] [CrossRef]
- Paterson, R.L.; Galley, H.F.; Webster, N.R. The effect of N-acetylcysteine on nuclear factor-kappa B activation, interleukin-6, interleukin-8 and intercellular adhesion molecule-1 expression in patients with sepsis. Crit. Care Med. 2003, 31, 2574–2578. [Google Scholar] [CrossRef]
- Bernard, G.R.; Wheeler, A.P.; Arons, M.M.; Morris, P.E.; Paz, H.L.; Russell, J.A.; Wright, P.E. A trial of antioxidants N-acetylcysteine and procysteine in ARDS. The Antioxidant in ARDS Study Group. Chest 1997, 112, 164–172. [Google Scholar] [CrossRef]
- Berger, M.M.; Vitamin, C. requirements in parenteral nutrition. Gastroenterology 2009, 137, 70–78. [Google Scholar] [CrossRef]
- May, J.M.; Harrison, F.E. Role of vitamin C in the function of the vascular endothelium. Antioxid. Redox Signal. 2013, 19, 2068–2083. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.M.; Oudemans-van Straaten, H.M. Vitamin C supplementation in the critically ill patient. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin C revisited. Crit. Care 2014, 18, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schorah, C.J.; Downing, C.; Piripitsi, A.; Gallivan, L.; Al-Hazaa, A.H.; Sanderson, M.J.; Bodenham, A. Total vitamin C, ascorbic acid and dehydroascorbic acid concentrations in plasma of critically ill patients. Am. J. Clin. Nutr. 1996, 63, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Spoelstra-de Man, A.M.E.; de Grooth, H.J.; Elbers, P.W.G.; Oudemans-van Straaten, H.M. Response to Adjuvant vitamin C in cardiac arrest patients undergoing renal replacement therapy: An appeal for a higher high-dose. Crit. Care 2018, 22, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, A.A.; Truwit, J.D.; Hite, R.D.; Morris, P.E.; DeWilde, C.; Priday, A.; Fisher, B.; Thacker, L.R.; Natarajan, R.; Brophy, D.F.; et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: The CITRIS-ALI randomized clinical trial. JAMA 2019, 322, 1261–1270. [Google Scholar]
- Pontes-Arruda, A.; Aragão, A.M.; Albuquerque, J.D. Effects of enteral feeding with eicosapentaenoic acid, gammalinolenic acid and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Crit. Care Med. 2006, 34, 2325–2333. [Google Scholar] [CrossRef] [Green Version]
- Nathens, A.B.; Neff, M.J.; Jurkovich, G.J.; Klotz, P.; Farver, K.; Ruzinski, J.T.; Radella, F.; Garcia, I.; Maier, R.V. Randomized, prospective trial of antioxidant supplementation in critically ill surgical patients. Ann. Surg. 2002, 236, 814–822. [Google Scholar] [CrossRef]
- Traber, M.G.; Atkinson, J. Vitamin E, antioxidant and nothing more. Free Radic. Biol. Med. 2007, 43, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Crimi, E.; Liguori, A.; Condorelli, M.; Cioffi, M.; Astuto, M.; Bontempo, P.; Pignalosa, O.; Vietri, M.T.; Molinari, A.M.; Sica, V.; et al. The beneficial effects of antioxidant supplementation in enteral feeding in critically ill patients: A prospective, randomized, double-blind, placebo-controlled trial. Anesth. Analg. 2004, 99, 857–863. [Google Scholar] [CrossRef]
- Howe, K.P.; Clochesy, J.M.; Goldstein, L.S.; Owen, H. Mechanical ventilation antioxidant trial. Am. J. Crit. Care 2015, 24, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Azzi, A. Molecular mechanism of alpha-tocopherol action. Free Radic. Biol. Med. 2007, 43, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Pappolla, M.A. Melatonin relieves the neural oxidative burden that contributes to dementias. Ann. N. Y. Acad. Sci. 2004, 1035, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J. Pineal melatonin: Cell biology of its synthesis and of its physiological interactions. Endocr. Rev. 1991, 12, 151–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydogan, S.; Yerer, M.B.; Goktas, A. Melatonin and nitric oxide. J. Endocrinol. Investig. 2006, 29, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Escames, G.; Guerrero, J.M.; Reiter, R.J.; Garcia, J.J.; Munoz-Hoyos, A.; Ortiz, G.G.; Oh, C.S. Melatonin and vitamin E prevent nitric oxide-induced lipid peroxidation in rat brain homogenates. Neurosci. Lett. 1997, 230, 147–150. [Google Scholar] [CrossRef]
- García, J.J.; Reiter, R.J.; Guerrero, J.M.; Escames, G.; Yu, B.P.; Oh, C.S. Muñoz-Hoyos, A. Melatonin prevents changes in microsomal membrane fluidity during induced lipid peroxidation. FEBS Lett. 1997, 408, 297–300. [Google Scholar] [CrossRef] [Green Version]
- Martín, M.; Macías, M.; Escames, G.; Reiter, R.J.; Agapito, M.T.; Ortiz, G.G.; Acuña-Castroviejo, D. Melatonin-induced increased activity of the respiratory chain complexes I and IV can prevent mitochondrial damage induced by ruthenium red in vivo. J. Pineal. Res. 2000, 28, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Urata, Y.; Honma, S.; Goto, S.; Todoroki, S.; Iida, T.; Cho, S.; Honma, K.; Kondo, T. Melatonin induces gamma-glutamylcysteine synthetase mediated by activator protein-1 in human vascular endothelial cells. Free Radic. Biol. Med. 1999, 27, 838–847. [Google Scholar] [CrossRef]
- Sewerynek, E.; Melchiorri, D.; Chen, L.D.; Reiter, R.J. Melatonin reduces both basal and bacterial lipopolysaccharide induced lipid peroxidation in vitro. Free Radic. Biol. Med. 1995, 19, 903–909. [Google Scholar] [CrossRef]
- Yang, J.; Hooper, W.C.; Phillips, D.J.; Talkington, D.F. Regulation of proinflammatory cytokines in human lung epithelial cells infected with Mycoplasma pneumoniae. Infect. Immun. 2002, 70, 3649–3655. [Google Scholar] [CrossRef] [Green Version]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.A.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Primers 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C. Quercetin: Potentials in the prevention and therapy of disease. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Kim, J.H.; Lee, C.H.; Ahn, Y.; Song, J.J.H.; Baek, S.H.; Kwon, D.H. Antiviral activity of quercetin 7-rhamnoside against porcine epidemic diarrhea virus. Antivir. Res. 2009, 81, 77–81. [Google Scholar] [CrossRef]
- Choi, H.J.; Song, J.H.; Park, K.S.; Kwon, D.H. Inhibitory effects of quercetin 3-rhamnoside on influenza A virus replication. Eur. J. Pharm. Sci. 2009, 37, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Andres, S.; Pevny, S.; Ziegenhagen, R.; Bakhiya, N.; Schäfer, B.; Hirsch-Ernst, K.I.; Lampen, A. Safety aspects of the use of quercetin as a dietary supplement. Mol. Nutr. Food Res. 2018, 62, 1700447. [Google Scholar] [CrossRef] [PubMed]
- Vlietinck, A.J.; Vanden, B.D.A.; Haemers, A. Present status and prospects of flavonoids as anti-viral agents. Prog. Clin. Biol. Res. 1988, 280, 283–299. [Google Scholar]
- Chiow, K.H.; Phoon, M.C.; Putti, T.; Tan, B.K.; Chow, V.T. Evaluation of antiviral activities of Houttuynia cordata Thunb. extract, quercetin, quercetrin and cinanserin on murine coronavirus and dengue virus infection. Asian Pac. J. Trop. Med. 2016, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Speer, E.M.; Dowling, D.J.; Ozog, L.S.; Xu, J.; Yang, J.; Kennady, G.; Levy, O. Pentoxifylline inhibits the production of inflammatory cytokines mediated by TLR and inflammasome in human blood with greater efficacy and potency in neonates. Pediatr. Res. 2017, 81, 806–816. [Google Scholar] [CrossRef] [Green Version]
- Harris, E.S.; Schulzke, M.; Patole, S.K. Pentoxifylline in preterm neonates: A systematic review. Paediatr. Drugs 2010, 12, 301–311. [Google Scholar] [CrossRef]
- Shabaan, A.E.; Nasef, N.; Shouman, B.; Nour, I.; Mesbah, A.; Abdel-Hady, H. Pentoxifylline therapy for late-onset sepsis in preterm infants: A randomized controlled trial. Pediatr. Infect. Dis. J. 2015, 34, 143–148. [Google Scholar] [CrossRef]
- Akdag, A.; Dilmen, U.; Haque, K.; Dilli, D.; Erdeve, O.; Goekmen, T. Role of IgM-enriched intravenous pentoxifylline and/or immunoglobulin in the treatment of neonatal sepsis. Am. J. Perinatol. 2014, 31, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Pammi, M.; Haque, K.N. Pentoxifylline for the treatment of sepsis and necrotizing enterocolitis in neonates. Cochrane Database Syst. Rev. 2015, 3, 004205. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Mechanism of Action | Adverse Effect | |
|---|---|---|---|
| Chloroquine and Hydroxychloroquine | ↓ | IL-1β mRNA expression in THP-1 cells. | Cardiovascular effects, particularly prolongation of the QT interval in the electrocardiogram and hypotension have been found with the use of several quinolines and other structurally related antimalarial drugs. |
| IL-6 and IL-1 in monocytes and macrophages and decreases the activity of the enzyme quinone reductase 2 [50]. | |||
| Ѳ | The replication of some DNA and RNA viruses [52,53]. | ||
| Suppresses the entrance of viruses into host cells and inhibits glycosylation of viral proteins [48]. | |||
| Alkalinizing the endosomal pH in the phagolysosome and by blocking the glycosylation of cellular receptor of SARS-CoV. | |||
| Suppresses phosphorylation of caspase-1 and of the p38 mitogen-activated protein kinase in THP-1 cells. | |||
| Suppresses IL-6, IL-12, TNF-α and IFN-α, β and γ [50,51]. | |||
| Suppresses the binding of the SARS-CoV-2 to target cells [51]. | |||
| Remdesivir | Ѳ | Suppresses coronaviral replication including that of MERS-CoV and SARS-CoV [64]. | Increase in plasma glucose levels. |
| Remdesivir acts on viral RNA polymerase evading proofreading by viral exo-nuclease, diminishing viral RNA production [64,65]. | |||
| Anti-Inflammatory Drugs | ↓ | Combinations of baricitinib with direct-acting antivirals could diminish viral replication, viral infectivity and the anormal host inflammatory response [66]. | These drugs are metabolized in the liver and most of the metabolites produced are eliminated in urine. Therefore, their metabolism may be impaired by damage to the liver and kidneys. |
| (Ruxolitinib, Fedratinib and Baricitinib) | Ѳ | Suppresses the JAK-STAT signaling [66]. | |
| Corticosteroids | ↑ | Decreases the immune responses while increasing the clearance of the pathogen [67,68,69]. | Systemic inflammation is associated to adverse outcomes in severe cases. |
| Ѳ | The lung inflammation [67,68,69]. | The treatment using corticosteroid should not be employed for lung injury induced by SARS-CoV-2. | |
| Arbidol/Umifenovir | Ѳ | Arbidol unites to lipid and protein residues suppressing the entrance of the virus entry and its fusion, budding, replication, assembly and viral resistance [70,71,72]. | Arbidol has only been used with a pharmacological approach and therefore, there are insufficient data on its toxicity. |
| Danoprevir | Ѳ | Is an HCV NS3 protease inhibitor [73]. |
| Treatment | Antioxidant Effect | Clinical Effect | |
|---|---|---|---|
| NAC | ↑ | The synthesis of glutathione and glutathione-S-transferase activity [100]. | Lipid peroxidation, chloramine concentration, damage to ACE, lung edema and the concentrations of thromboxane and leukotriene B2 and B4 were diminished in the lungs. |
| ↓ | The levels of IL-8, IL-6, ICAM and decreases activation of NFκB [101,102]. | ||
| Vitamin C and E | ↑ | The adhesiveness of leukocytes in the microcirculation [108,109]. | The combined effect of therapy with vitamin E and vitamin C in severe post-operative patients resulted in a decrease in the incidence of ARDS or pneumonia, a decrease in organ failure and a tendency to decrease mortality at 28 days. |
| Ѳ | The production of OONO− and O2− by inhibiting the NAPH oxidase, the activation of protein phosphatase 2A and TNF-α [109,110,111,112]. | ||
| MT | ↑ | The intracellular glutathione synthesis [122]. | Melatonin enhances the immune response by improving proliferation and maturation of natural killing cells, T and B lymphocytes, granulocytes and monocytes in both bone marrow and other tissues and also presents anti-inflammatory action and induces the up-regulation of Nrf2 with therapeutic effects on hepato protection and cardio protection. |
| ↓ | The levels of hydroperoxide in mitochondria by restoring glutathione homeostasis and mitochondrial function in organelles under oxidative stress [120,123]. | ||
| QRC | Ѳ | The H+ −ATPase of the lysosomal membrane and the ATPase of proteins related to resistance to many drugs elevating the bioavailability drugs [126,127,128]. | It has antiviral, cardioprotective, antioxidant, anti-inflammatory and anti-carcinogenic effects. |
| Pentoxifylline | ↑ | The glutathione levels, it maintains mitochondrial viability [133]. | Decreases duration of respiratory support and antibiotic treatment, diminished the need for vasopressors, resulted in a shorter hospitalization time and decreased incidence of metabolic acidosis, thrombocytopenia and disseminated intravascular coagulopathy. |
| ↓ | The levels of CRP and TNF-α [134]. | ||
| Ѳ | TNF-α production [132]. | ||
| Identification of the Case and Integral Study | Management by the Intensive Care Specialist | Proposed Treatment Assays | Additional Proposed Antioxidant Therapy to the Medical Management in COVID-19 Patients with Pneumonia | Drug Interactions |
|---|---|---|---|---|
| 1. Identification of infected cases having a medical history (healthy or with simple or combined comorbidities), age, body mass index. 2. Integral laboratory tests, including total cholesterol, HDL, LDL, triglycerides, D dimer, troponins, natriuretic peptide, creatine phosphokinase, Cl, Na, K, magnesium, phosphorus. Evaluation of hepatic and renal function. 3. Chest X-ray and/or computerized tomography. 4. Cardiovascular: electrocardiogram, echocardiogram. 5. When a cardiovascular disease is present, a multidisciplinary management involving a cardiologist is suggested (this applies to all cases). | 1. Antibiotics, according to requirements. A culture if an associated bacterial infection is present. 2. Mechanical ventilation. 3. Hemodynamic Management. 4. Extracorporeal membrane oxygenation if necessary (this applies to all cases). | The patient may be treated with any of the therapies suggested by the clinical assays in standard doses. Only one or a combination of two antioxidants may be applied. When the pulmonary function is compromised, a combination of NAC and vitamin C is suggested. (This applies to all cases). | NAC dose: 600 mg/24 h orally or through a nasal enteral tube for 5 days. It should not be used when there is a gastric ulcer or antecedents of asthma or a cysteine allergy. | Anti-cholinergic drugs, anti-histaminic drugs. |
| MT dose: 5 mg tablet (10 capsules)/24 h orally or through a nasal enteral tube for five days. It is safe and has a low toxicity. It is contraindicated during pregnancy, diabetes mellitus and when a patient has high systemic hypertension of the blood, and care must be taken when it is used together with some antihypertensive drugs. | Sedatives, Luvox contraceptives and cocaine increase the effect of MT. Verapamil, nifedipine, caffeine, alcohol and immunosuppressors decrease the MT effect. | |||
| Vit C dose: 1 g every 6 h orally or through a nasal enteral tube for 5 days. It should not be used in patients with gastric ulcers, falciform anemia or during pregnancy. At high doses > 3 g, it may interact with medications used in patients with diabetes mellitus, hypertension, or Parkinson’s disease. | Aluminum, estrogens, protease inhibitors, antivirals: nelfinavir amprenavir, ritonavir, saquinavir, statins, glimepiride, glipizide, metformin, pioglitazone, rosiglitazone, antihypertensive drugs. | |||
| Vit E, dose capsules of 400 UI that are the equivalent of 400 mg every 12 h for 5 days. It should not be used when retinitis pigmentosa is present. | Simvastatin and niacin, chemotherapy, anticoagulants and antiplatelet agents and non-steroidal anti-inflammatory drugs. | |||
| QRC, at a dose of 500 mg every 12 h. It is safe for most people, but is not contraindicated during pregnancy. The dose should be adjusted in patients with renal failure. | Quinolones, uroseptal, cyclosporine, celecoxib, diclofenac, ibuprofen, Fluvastatin, irbesartan, losartan. | |||
Initial evaluation. | Measures that are jointly evaluated according to the initial evaluation. | Measures that are jointly evaluated according to the initial evaluation. | Pentoxifylline (vasodilator, inhibitor of IL-6), at a dose of 400 mg daily orally or IV. Patients that are intolerant to methylxanthines might not tolerate it. (The doses of the elected antioxidants and/or pentoxifylline are similar in all cases. The selection must be taken according to contraindications and drug interactions). Measures that are jointly evaluated according to the initial evaluation.  | Coumarin, heparin, indandione derivatives, cefotetan, cefamandole, valproic acid and plicamycin may increase the risk of bleeding. Final evaluation.  |
| Evaluate and Apply According to the Patient’s Comorbidities | ||||
| Diabetes Mellitus with or without Hypertension NAC or MT or QRC or vit E + pentoxifylline. | Hypertension NAC or MT (if antihypertensive drugs that may interfere are not being used) or QRC or vit E (if anticoagulants are not being used) or pentoxifylline. | Obesity Without Another Comorbidity NAC or MT or QRC or vit E or vit C + pentoxifylline. Obesity + SAH + DM NAC or QRC + pentoxifylline. | Renal Insufficiency without Substitute Management (Dose Adjustment) NAC or MT or QRC or vit E + pentoxifylline. In Patients in Dialysis of Hemodialysis Standard dose. | Heart Failure NAC or MT or QRC or vit E + pentoxifylline. Monitor if the patient uses antiplatelet or anticoagulant digoxin or has an arrhythmia. |
| Ischemic Heart Disease NAC or MT or QRC or Vit E + Pentoxifylline Adjust if there is use of antihypertensive drugs that interact with any of them | Myocarditis NAC or MT or QRC or Vit E + Pentoxifylline On Dialysis or Hemodialysis Standard dose. Immunoglobulin should be the treatment of choice except contraindication | Arrhythmias NAC or MT or QRC or + Pentoxifylline | Chronic Obstructive Pulmonary Disease NAC or MT or QRC or + Pentoxifylline Smoking NAC or MT or QRC or Vit C + Pentoxifylline | Immune Suppression NAC or Vit E (if anticoagulants are not being used) or Pentoxifylline Cancer NAC or QRC |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soto, M.E.; Guarner-Lans, V.; Soria-Castro, E.; Manzano Pech, L.; Pérez-Torres, I. Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application. Medicina 2020, 56, 386. https://doi.org/10.3390/medicina56080386
Soto ME, Guarner-Lans V, Soria-Castro E, Manzano Pech L, Pérez-Torres I. Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application. Medicina. 2020; 56(8):386. https://doi.org/10.3390/medicina56080386
Chicago/Turabian StyleSoto, María Elena, Verónica Guarner-Lans, Elizabeth Soria-Castro, Linaloe Manzano Pech, and Israel Pérez-Torres. 2020. "Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application" Medicina 56, no. 8: 386. https://doi.org/10.3390/medicina56080386
APA StyleSoto, M. E., Guarner-Lans, V., Soria-Castro, E., Manzano Pech, L., & Pérez-Torres, I. (2020). Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application. Medicina, 56(8), 386. https://doi.org/10.3390/medicina56080386