Liposomes for Intra-Articular Analgesic Drug Delivery in Orthopedics: State-of-Art and Future Perspectives. Insights from a Systematic Mini-Review of the Literature


 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
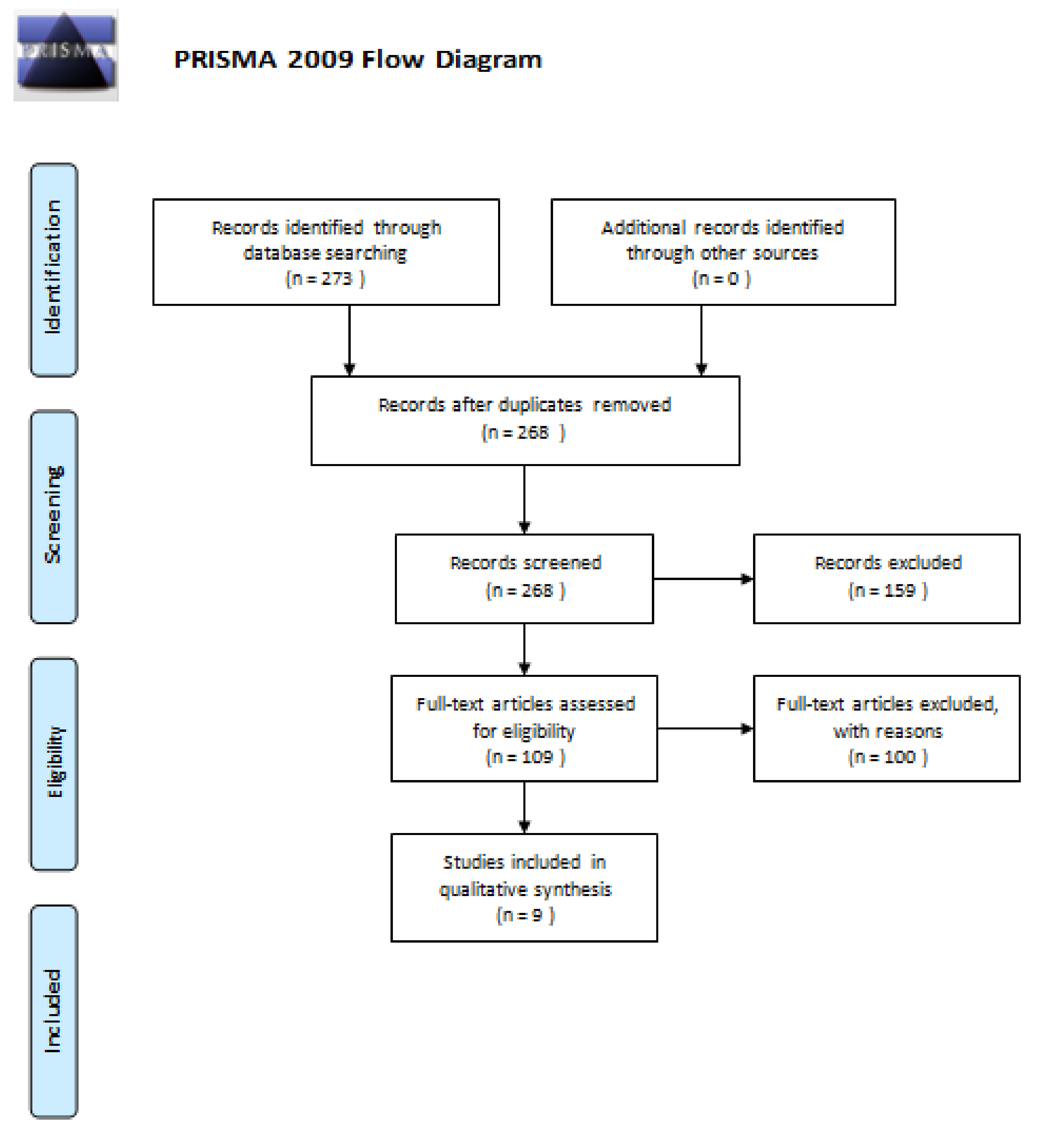
2. Materials and Methods
3. Results
3.1. Analysis of Results
3.2. Technologies for Liposome Design and Fabrication
3.3. Liposomes for Intra-Articular (IA) Injections
3.4. Liposomes in Postsurgical Analgesia
3.5. Liposomes Can Help Prevent Orthopedic Device-Associated Osteomyelitis
3.6. Liposomes in Hirudo Therapy for OA
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Allen, T.M.; Cullis, P.R. Liposomal drug delivery systems: From concept to clinical applications. Adv. Drug Deliv. Rev. 2013, 65, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Bangham, A.; Standish, M.; Watkins, J. Diffusion of univalent ions across the lamellae of swollen phospholipids. J. Mol. Biol. 1965, 13, 238–252. [Google Scholar] [CrossRef]
- Immordino, M.L.; Dosio, F.; Cattel, L. Stealth liposomes: Review of the basic science, rationale, and clinical applications, existing and potential. Int. J. Nanomed. 2006, 1, 297–315. [Google Scholar]
- Goulart, L.R.; Dantas, N.; Silva, A.; Madurro, J.M.; Brito-Madurro, A.G.; Ueira-Vieira, C.; Fujimura, P.; Maia, Y.; Santos, P.S.; Freschi, A.P.; et al. Frontiers of biology in human diseases: Strategies for biomolecule’s discovery, nanobiotechnologies and biophotonics. BMC Proc. 2014, 8 (Suppl. 4). [Google Scholar] [CrossRef] [Green Version]
- Sahoo, S.K.; Parveen, S.; Panda, J. The present and future of nanotechnology in human health care. Nanomed. Nanotechnol. Biol. Med. 2007, 3, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Kalaycioglu, G.D.; Aydogan, N. Preparation and investigation of solid lipid nanoparticles for drug delivery. Colloids Surf. Physicochem. Eng. Asp. 2016, 510, 77–86. [Google Scholar] [CrossRef]
- Trucillo, P.; Campardelli, R.; Reverchon, E. Supercritical CO 2 assisted liposomes formation: Optimization of the lipidic layer for an efficient hydrophilic drug loading. J. CO2 Util. 2017, 18, 181–188. [Google Scholar] [CrossRef]
- Campardelli, R.; Santo, I.E.; Cabral-Albuquerque, E.C.; De Melo, S.A.B.V.; Della Porta, G.; Reverchon, E. Efficient encapsulation of proteins in submicro liposomes using a supercritical fluid assisted continuous process. J. Supercrit. Fluids 2016, 107, 163–169. [Google Scholar] [CrossRef]
- Situ, W.; Song, X.; Luo, S.; Liang, Y. A nano-delivery system for bioactive ingredients using supercritical carbon dioxide and its release behaviors. Food Chem. 2017, 228, 219–225. [Google Scholar] [CrossRef]
- Patil, Y.P.; Jadhav, S. Novel methods for liposome preparation. Chem. Phys. Lipids 2014, 177, 8–18. [Google Scholar] [CrossRef]
- Mozafari, M.R. Liposomes: An overview of manufacturing techniques. Cell. Mol. Biol. Lett. 2005, 10, 711–719. [Google Scholar] [PubMed]
- Trucillo, P.; Campardelli, R.; Reverchon, E. A versatile supercritical assisted process for the one-shot production of liposomes. J. Supercrit. Fluids 2019, 146, 136–143. [Google Scholar] [CrossRef]
- Trucillo, P.; Campardelli, R.; Scognamiglio, M.; Reverchon, E. Control of liposomes diameter at micrometric and nanometric level using a supercritical assisted technique. J. CO2 Util. 2019, 32, 119–127. [Google Scholar] [CrossRef]
- Harrington, K.; Syrigos, K.; Vile, R.G. Liposomally targeted cytotoxic drugs for the treatment of cancer. J. Pharm. Pharmacol. 2002, 54, 1573–1600. [Google Scholar] [CrossRef]
- Lonez, C.; Vandenbranden, M.; Ruysschaert, J.-M. Cationic lipids activate intracellular signaling pathways. Adv. Drug Deliv. Rev. 2012, 64, 1749–1758. [Google Scholar] [CrossRef]
- Huang, W.-C.; Deng, B.; Lin, C.; Carter, K.A.; Geng, J.; Razi, A.; He, X.; Chitgupi, U.; Federizon, J.; Sun, B.; et al. A malaria vaccine adjuvant based on recombinant antigen binding to liposomes. Nat. Nanotechnol. 2018, 13, 1174–1181. [Google Scholar]
- Dearling, J.L.; Packard, A.B. Molecular imaging in nanomedicine – A developmental tool and a clinical necessity. J. Control. Release 2017, 261, 23–30. [Google Scholar] [CrossRef]
- De Lima, M.C.P.; Neves, S.; Filipe, A.; Duzgunes, N.; Simões, S. Cationic liposomes for gene delivery: From biophysics to biological applications. Curr. Med. Chem. 2003, 10, 1221–1231. [Google Scholar] [CrossRef]
- Slingerland, M.; Guchelaar, H.-J.; Gelderblom, H. Liposomal drug formulations in cancer therapy: 15 years along the road. Drug Discov. Today 2012, 17, 160–166. [Google Scholar] [CrossRef]
- Hoven, J.M.V.D.; Van Tomme, S.R.; Metselaar, J.M.; Nuijen, B.; Beijnen, J.H.; Storm, G. Liposomal Drug Formulations in the Treatment of Rheumatoid Arthritis. Mol. Pharm. 2011, 8, 1002–1015. [Google Scholar] [CrossRef]
- Knobloch, K.; Yoon, U.; Vogt, P.M. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Cranio Maxillofac. Surg. 2011, 39, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Paolino, D.; Cosco, D.; Gaspari, M.; Celano, M.; Wolfram, J.; Voce, P.; Puxeddu, E.; Filetti, S.; Celia, C.; Ferrari, M.; et al. Targeting the thyroid gland with thyroid-stimulating hormone (TSH)-nanoliposomes. Biomaterials 2014, 35, 7101–7109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celia, C.; Ferrati, S.; Bansal, S.; Van De Ven, A.L.; Ruozi, B.; Zabre, E.; Hosali, S.; Paolino, D.; Sarpietro, M.G.; Fine, D.; et al. Sustained zero-order release of intact ultra-stable drug-loaded liposomes from an implantable nanochannel delivery system. Adv. Health Mater. 2013, 3, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Pasut, G.; Paolino, D.; Celia, C.; Mero, A.; Joseph, A.S.; Wolfram, J.; Cosco, D.; Schiavon, O.; Shen, H.; Fresta, M. Polyethylene glycol (PEG)-dendron phospholipids as innovative constructs for the preparation of super stealth liposomes for anticancer therapy. J. Control. Release 2015, 199, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Uhl, K.; Katinger, H. Liposomes produced in a pilot scale: Production, purification and efficiency aspects. Eur. J. Pharm. Biopharm. 2002, 54, 213–219. [Google Scholar] [CrossRef]
- Bangham, A.D.; Hill, M.W.; Miller, N.G.A. Preparation and Use of Liposomes as Models of Biological Membranes. In Methods in Membrane Biology; Korn, E.D., Ed.; Springer: Boston, MA, USA, 1974; Volume 1, pp. 1–68. [Google Scholar] [CrossRef]
- Mui, B.; Chow, L.; Hope, M.J. Extrusion Technique to Generate Liposomes of Defined Size. Methods Enzymol. 2003, 367, 3–14. [Google Scholar]
- Andar, A.; Hood, R.R.; Vreeland, W.N.; DeVoe, D.L.; Swaan, P.W. Microfluidic Preparation of Liposomes to Determine Particle Size Influence on Cellular Uptake Mechanisms. Pharm. Res. 2013, 31, 401–413. [Google Scholar] [CrossRef]
- Charcosset, C.; Juban, A.; Valour, J.-P.; Urbaniak, S.; Fessi, H. Preparation of liposomes at large scale using the ethanol injection method: Effect of scale-up and injection devices. Chem. Eng. Res. Des. 2015, 94, 508–515. [Google Scholar] [CrossRef]
- Otake, K.; Shimomura, T.; Goto, T.; Imura, T.; Furuya, T.; Yoda, S.; Takebayashi, Y.; Sakai, H.; Abe, M. Preparation of Liposomes Using an Improved Supercritical Reverse Phase Evaporation Method. Langmuir 2006, 22, 2543–2550. [Google Scholar] [CrossRef]
- Meure, L.A.; Knott, R.; Foster, N.R.; Dehghani, F. The Depressurization of an Expanded Solution into Aqueous Media for the Bulk Production of Liposomes. Langmuir 2009, 25, 326–337. [Google Scholar] [CrossRef]
- Zhao, L.; Temelli, F. Preparation of liposomes using a modified supercritical process via depressurization of liquid phase. J. Supercrit. Fluids 2015, 100, 110–120. [Google Scholar] [CrossRef]
- Lesoin, L.; Crampon, C.; Boutin, O.; Badens, E. Preparation of liposomes using the supercritical anti-solvent (SAS) process and comparison with a conventional method. J. Supercrit. Fluids 2011, 57, 162–174. [Google Scholar] [CrossRef]
- Gabizon, A.; Shmeeda, H.; Barenholz, Y. Pharmacokinetics of Pegylated Liposomal Doxorubicin. Clin. Pharmacokinet. 2003, 42, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Rivankar, S. An overview of doxorubicin formulations in cancer therapy. J. Cancer Res. Ther. 2014, 10, 853. [Google Scholar] [CrossRef] [PubMed]
- Petre, C.E.; Dittmer, D.P. Liposomal daunorubicin as treatment for Kaposi’s sarcoma. Int. J. Nanomed. 2007, 2, 277–288. [Google Scholar]
- Bomgaars, L.R.; Geyer, J.; Franklin, J.; Dahl, G.; Park, J.; Winick, N.; Klenke, R.; Berg, S.L.; Blaney, S.M. Phase I Trial of Intrathecal Liposomal Cytarabine in Children with Neoplastic Meningitis. J. Clin. Oncol. 2004, 22, 3916–3921. [Google Scholar] [CrossRef] [PubMed]
- Della Porta, G.; Ciardulli, M.C.; Maffulli, N. Microcapsule Technology for Controlled Growth Factor Release in Musculoskeletal Tissue Engineering. Sports Med. Arthrosc. Rev. 2018, 26, e2–e9. [Google Scholar] [CrossRef]
- Santo, I.E.; Campardelli, R.; Cabral-Albuquerque, E.C.; De Melo, S.A.B.V.; Della Porta, G.; Reverchon, E. Liposomes preparation using a supercritical fluid assisted continuous process. Chem. Eng. J. 2014, 249, 153–159. [Google Scholar] [CrossRef]
- Ciaglia, E.; Montella, F.; Trucillo, P.; Ciardulli, M.; Di Pietro, P.; Amodio, G.; Remondelli, P.; Vecchione, C.; Reverchon, E.; Maffulli, N.; et al. A bioavailability study on microbeads and nanoliposomes fabricated by dense carbon dioxide technologies using human-primary monocytes and flow cytometry assay. Int. J. Pharm. 2019, 570, 118686. [Google Scholar] [CrossRef]
- Larsen, C.; Østergaard, J.; Larsen, S.W.; Jensen, H.; Jacobsen, S.; Lindegaard, C.; Andersen, P.H. Intra-articular depot formulation principles: Role in the management of postoperative pain and arthritic disorders. J. Pharm. Sci. 2008, 97, 4622–4654. [Google Scholar] [CrossRef]
- Maudens, P.; Jordan, O.; Allémann, E. Recent advances in intra-articular drug delivery systems for osteoarthritis therapy. Drug Discov. Today 2018, 23, 1761–1775. [Google Scholar] [CrossRef] [PubMed]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, preparation, and applications. Nanoscale Res. Lett. 2013, 8, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.; Stuart, J.M.; Magid, R.; Danila, D.C.; Hunsaker, T.; Pinkhassik, E.; Hasty, K.A. Theranostic immunoliposomes for osteoarthritis. Nanomed. Nanotechnol.Biol. Med. 2014, 10, 619–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanniasinghe, A.S.; Bender, V.; Manolios, N. The Potential of Liposomal Drug Delivery for the Treatment of Inflammatory Arthritis. Semin. Arthritis Rheum. 2009, 39, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Jiang, D.; Wang, Z.; Wu, G.; Miao, L.; Huang, L. Intra-articular delivery of liposomal celecoxib–hyaluronate combination for the treatment of osteoarthritis in rabbit model. Int. J. Pharm. 2013, 441, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhong, Z.-H.; Yu, H.-T.; Liu, B. Exogenous expression ofIL-1RaandTGF-β1promotes in vivo repair in experimental rabbit osteoarthritis. Scand. J. Rheumatol. 2015, 44, 404–411. [Google Scholar] [CrossRef]
- Bonanomi, M.H.; Velvart, M.; Stimpel, M.; Roos, K.M.; Fehr, K.; Weder, H.G. Studies of pharmacokinetics and therapeutic effects of glucocorticoids entrapped in liposomes after intraarticular application in healthy rabbits and in rabbits with antigen-induced arthritis. Rheumatol. Int. 1987, 7, 203–212. [Google Scholar] [CrossRef]
- Accreditata, X.C.N.S.S.I.C.O.D.P.; Cipollaro, L.; Aicale, R.; Maccauro, G.; Maffulli, N. Single- versus double-integrated screws in intramedullary nailing systems for surgical management of extracapsular hip fractures in the elderly: A systematic review. J. Biol. Regul. Homeost. Agents 2019, 33, 175–182. [Google Scholar]
- Hutchinson, H.L. Local infiltration of liposome bupivacaine in orthopedic trauma patients: Case-based reviews. Am. J. Orthop. 2014, 43, S13–S16. [Google Scholar]
- Nota, S.P.; Spit, S.A.; Voskuyl, T.; Bot, A.G.; Hageman, M.G.; Ring, D. Opioid Use, Satisfaction, and Pain Intensity After Orthopedic Surgery. Psychosomatics 2015, 56, 479–485. [Google Scholar] [CrossRef]
- Wu, C.L.; Naqibuddin, M.; Rowlingson, A.J.; Lietman, S.A.; Jermyn, R.M.; Fleisher, L.A. The Effect of Pain on Health-Related Quality of Life in the Immediate Postoperative Period. Anesth. Analg. 2003, 97, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Capdevila, X.; Dadure, C.; Bringuier, S.; Bernard, N.; Biboulet, P.; Gaertner, E.; Macaire, P. Effect of Patient-controlled Perineural Analgesia on Rehabilitation and Pain after Ambulatory Orthopedic Surgery. Anesthesiology 2006, 105, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Ranawat, A.S.; Ranawat, C.S. Pain Management and Accelerated Rehabilitation for Total Hip and Total Knee Arthroplasty. J. Arthroplast. 2007, 22, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Alter, T.; Liss, F.E.; Ilyas, A.M. A Prospective Randomized Study Comparing Bupivacaine Hydrochloride Versus Bupivacaine Liposome for Pain Management After Distal Radius Fracture Repair Surgery. J. Hand Surg. 2017, 42, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Burbridge, M.; Jaffe, R.A. Exparel: A New Local Anesthetic with Special Safety Concerns. Anesth. Analg. 2015, 121, 1113–1114. [Google Scholar] [CrossRef]
- Lonner, J.H.; Scuderi, G.R.; Lieberman, J.R. Potential utility of liposome bupivacaine in orthopedic surgery. Am. J. Orthop. 2015, 44, 111–117. [Google Scholar]
- Kendall, M.C.; Alves, L.J.C.; De Oliveira, G. Liposome Bupivacaine Compared to Plain Local Anesthetics to Reduce Postsurgical Pain: An Updated Meta-Analysis of Randomized Controlled Trials. Pain Res. Treat. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Barrington, J.W.; Emerson, R.H.; Lovald, S.T.; Lombardi, A.V.; Berend, K.R. No Difference in Early Analgesia Between Liposomal Bupivacaine Injection and Intrathecal Morphine After TKA. Clin. Orthop. Relat. Res. 2016, 475, 94–105. [Google Scholar] [CrossRef] [Green Version]
- Amundson, A.W.; Johnson, R.L.; Abdel, M.P.; Mantilla, C.B.; Panchamia, J.K.; Taunton, M.J.; Kralovec, M.E.; Hebl, J.R.; Schroeder, D.R.; Pagnano, M.W.; et al. A Three-arm Randomized Clinical Trial Comparing Continuous Femoral Plus Single-injection Sciatic Peripheral Nerve Blocks versus Periarticular Injection with Ropivacaine or Liposomal Bupivacaine for Patients Undergoing Total Knee Arthroplasty. Anesthesiology 2017, 126, 1139–1150. [Google Scholar] [CrossRef]
- Bramlett, K.; Onel, E.; Viscusi, E.R.; Jones, K. A randomized, double-blind, dose-ranging study comparing wound infiltration of DepoFoam bupivacaine, an extended-release liposomal bupivacaine, to bupivacaine HCl for postsurgical analgesia in total knee arthroplasty. Knee 2012, 19, 530–536. [Google Scholar] [CrossRef]
- Premkumar, A.; Samady, H.; Slone, H.; Hash, R.; Karas, S.; Xerogeanes, J. Liposomal Bupivacaine for Pain Control After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2016, 44, 1680–1686. [Google Scholar] [CrossRef] [PubMed]
- Schroer, W.C.; Diesfeld, P.G.; Lemarr, A.R.; Morton, D.J.; Reedy, M.E. Does Extended-Release Liposomal Bupivacaine Better Control Pain Than Bupivacaine After Total Knee Arthroplasty (TKA)? A Prospective, Randomized Clinical Trial. J. Arthroplast. 2015, 30, 64–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagsby, D.T.; Ireland, P.H.; Meneghini, R.M. Liposomal Bupivacaine Versus Traditional Periarticular Injection for Pain Control After Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 1687–1690. [Google Scholar] [CrossRef] [PubMed]
- Webb, B.T.; Spears, J.R.; Smith, L.S.; Malkani, A.L. Periarticular injection of liposomal bupivacaine in total knee arthroplasty. Arthroplast. Today 2015, 1, 117–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mont, M.A.; Beaver, W.B.; Dysart, S.H.; Barrington, J.W.; Del Gaizo, D.J. Local Infiltration Analgesia with Liposomal Bupivacaine Improves Pain Scores and Reduces Opioid Use After Total Knee Arthroplasty: Results of a Randomized Controlled Trial. J. Arthroplast. 2018, 33, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrington, J.W. Opioid-Sparing Pain Control in Outpatient Total Joint Arthroplasty. Am. J. Orthop. 2016, 45, S2–S5. [Google Scholar]
- Tateosian, V.; Gan, T.J. Another quest for the holy grail of abolishing post operative nausea and vomiting. J. Clin. Anesthes. 2017, 41, 58–59. [Google Scholar] [CrossRef]
- Barrington, J.W.; Olugbode, O.; Lovald, S.T.; Ong, K.; Watson, H.; Emerson, R. Liposomal Bupivacaine: A Comparative Study of More Than 1000 Total Joint Arthroplasty Cases. Orthop. Clin. N. Am. 2015, 46, 469–477. [Google Scholar] [CrossRef]
- Calhoun, J.H.; Manring, M.; Shirtliff, M. Osteomyelitis of the Long Bones. Semin. Plast. Surg. 2009, 23, 59–72. [Google Scholar] [CrossRef] [Green Version]
- Lamagni, T. Epidemiology and burden of prosthetic joint infections. J. Antimicrob. Chemother. 2014, 69, i5–i10. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.-M.; Zhang, Y.; Chen, F.; Khutsishvili, I.; Fehringer, E.V.; Marky, L.A.; Bayles, K.W.; Wang, D. Prevention of orthopedic device-associated osteomyelitis using oxacillin-containing biomineral-binding liposomes. Pharm. Res. 2012, 29, 3169–3179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildebrandt, J.-P.; Lemke, S. Small bite, large impact–saliva and salivary molecules in the medicinal leech, Hirudo medicinalis. Naturwissenschaften 2011, 98, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Koeppen, D.; Aurich, M.; Rampp, T. Medicinal leech therapy in pain syndromes: A narrative review. Wien. Med. Wochenschr. 2013, 164, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Barkley, T.W. Medicinal leech therapy. Nursing 2015, 45, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Rai, P.K.; Singh, A.K.; Singh, O.P.; Rai, N.P.; Dwivedi, A.K. Efficacy of leech therapy in the management of osteoarthritis (Sandhivata). Selendang Ayu Oil Spill Lessons Learn. 2011, 32, 213–217. [Google Scholar] [CrossRef]
- Shakouri, A.; Adljouy, N.; Balkani, S.; Mohamadi, M.; Hamishehkar, H.; Abdolalizadeh, J.; Shakouri, S.K. Effectiveness of topical gel of medical leech(Hirudo medicinalis)saliva extract on patients with knee osteoarthritis: A randomized clinical trial. Complement. Ther. Clin. Pract. 2018, 31, 352–359. [Google Scholar] [CrossRef]
- Beaussier, M.; Sciard, D.; Sautet, A. New modalities of pain treatment after outpatient orthopaedic surgery. Orthop. Traumatol. Surg. Res. 2016, 102, S121–S124. [Google Scholar] [CrossRef]
- Li, C.; Qu, J.; Pan, S.; Qu, Y. Local infiltration anesthesia versus epidural analgesia for postoperative pain control in total knee arthroplasty: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2018, 13, 112. [Google Scholar] [CrossRef]
- Elvir-Lazo, O.L.; White, P.F. The role of multimodal analgesia in pain management after ambulatory surgery. Curr. Opin. Anaesthesiol. 2010, 23, 697–703. [Google Scholar] [CrossRef]
- Elvir-Lazo, O.L.; White, P.F. Postoperative Pain Management After Ambulatory Surgery: Role of Multimodal Analgesia. Anesthesiol. Clin. 2010, 28, 217–224. [Google Scholar] [CrossRef]
- Dahl, J.B.; Møiniche, S. Pre-emptive analgesia. Br. Med. Bull. 2004, 71, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Cummings, I.K.; Chahar, P. Liposomal bupivacaine: A review of a new bupivacaine formulation. J. Pain Res. 2012, 5, 257–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asche, C.V.; Ren, J.; Kim, M.; Gordon, K.; McWhirter, M.; Kirkness, C.S.; Maurer, B.T. Local infiltration for postsurgical analgesia following total hip arthroplasty: A comparison of liposomal bupivacaine to traditional bupivacaine. Curr. Med. Res. Opin. 2017, 33, 1283–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkness, C.S.; Asche, C.V.; Ren, J.; Kim, M.; Rainville, E.C. Cost–benefit evaluation of liposomal bupivacaine in the management of patients undergoing total knee arthroplasty. Am. J. Heal. Pharm. 2016, 73, e247–e254. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors (Year) | Study Design | Sample Size | Age | Gender | Disorder | Procedures | Treatment | Result | Adverse Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Alter et al. (2017) [55] | Prospective, randomized, single-blinded, single-center clinical trial, sample size a priori computed, systematic recruitment | 41, 20 receiving Exparel, 21 receiving marcaine | 63 ± 15 years receiving Exparel, 57 ± 15 years receiving marcaine | 16 women (80%) receiving Exparel, 17 (81%) receiving marcaine | Distal Radius Fracture | Distal Radius Fracture Repair Surgery | Exparel 20 mL+ 10 mL 0.5% Marcaine | Exparel use resulted in decreased pain (4.0 versus 6.0, p < 0.05) and opioid consumption (1.2 versus 2.0 pills, 7.3 versus 12.5 oral morphine equivalents) only on the day of surgery and not thereafter | 16/20 receiving Exparel and 11/21 receiving marcaine experienced hand numbness, 1/20 receiving Exparel and 4/21 receiving marcaine reported itching, nausea, drowsiness/dizziness, and lack of energy |
| Amundson et al. (2017) [60] | Three-arm, parallel, single blinded (outcome adjudicator-blinded), superiority, randomized-controlled, single-center clinical trial, sample size a priori computed, systematic recruitment | 157 (out of an initial list of 165 patients), 52 receiving Exparel, 55 receiving Ropivacaine, 50 receiving peripheral nerve block | 67 ± 8 years receiving Exparel, 68 ± 8 years receiving Ropivacaine, 67 ± 9 years receiving peripheral nerve block | 27 women (52%) receiving Exparel, 34 (62% receiving Ropivacaine), 25 (50%) receiving peripheral nerve block | Patients needing total knee arthroplasty | Elective, Unilateral, Primary, Total Knee Arthroplasty | Exparel 20 mL (266 mg) + 100 mL Saline +120 mL (300 mg) Ropivacaine | No significant benefit of liposomal bupivacaine over ropivacaine in periarticular injections for total knee arthroplasty (post-operative day 1 median maximal pain score was lower for peripheral nerve blockade, p = 0.016, median difference -1 [95%CI -2 to 0]), patients receiving Exparel exhibited improved physical quality of life (p = 0.048), as well as those receiving Ropivacaine (p = 0.001), but not those receiving peripheral nerve block | 6 patients fell (2 receiving peripheral nerve block, 1 receiving Ropivacaine, 1 receiving Exparel), 6 patients had a wound infection (2 for each group) |
| Bramlett et al. (2012) [61] | Phase 2, randomized, parallel-group, double-blinded, dose-ranging, multi-center clinical trial, sample size a priori computed, systematic recruitment | 138 (out of an initial list of 164 screened patients and of 144 randomized patients), four discontinued the trial, two experienced serious adverse events, one died, one left for other reasons, 27 receiving DepoFoam 133 mg, 25 receiving DepoFoam 266 mg, 26 receiving DepoFoam 399 mg, 24 receiving DepoFoam 532 mg, 32 receiving Bupivacaine | 61.4 ± 7.0 years receiving DepoFoam 133 mg; 61.1 ± 8.7 years receiving DepoFoam 266 mg; 61.8 ± 6.3 years receiving DepoFoam 399 mg, 64.9 ± 7.3 years receiving DepoFoam 532 mg, 62.2 ± 7.2 years receiving Bupivacaine 150 mg | 15 women (53.6%) receiving DepoFoam 133 mg; 12 women (48.0%) receiving DepoFoam 266 mg; 15 women (57.7%) receiving DepoFoam 399 mg; 20 women (80.0%) receiving DepoFoam 532 mg; 23 women (67.6%) receiving Bupivacaine 150 mg | Patients needing total knee arthroplasty | Unilateral, Primary, Total Knee Arthroplasty | Exparel 20 mL (266 mg) + 40 mL Saline + 50% Bupivacaine 30 mL + 30 mL NS | Exparel was associated with statistically significantly greater analgesia compared with bupivacaine HCl in terms of pain at rest and pain with activity | Overall 112 (81.2%) experienced at least one side-effect (79.8% receiving DepoFoam versus 85.3% receiving Bupivacaine) |
| Premkumar et al. (2016) [62] | Prospective, double-blinded, randomized, positive-controlled, single-center clinical trial, systematic recruitment | 32 (out of an initial list of 35 patients), follow-up rate of 90.6%, 16 receiving Exparel, 16 receiving Bupivacaine | 24.1 ± 7.3 years receiving Exparel, 25.5 ± 6.8 years receiving Bupivacaine | 33% women receiving Exparel, 47% women receiving Bupivacaine | Injury of the anterior cruciate ligament | Anterior Cruciate Ligament Reconstruction with a soft tissue quadriceps tendon autograft | Exparel/Bupivacaine 20 mL + 20 mL 0.9% Saline | No significant differences in postoperative pain, recovery time, mobility, pain location or opioid use between patients receiving liposomal bupivacaine or 0.25% bupivacaine HCl | Not reported |
| Schroer et al. (2015) [63] | Prospective, randomized, clinical trial, systematic (consecutive) recruitment | 111, 58 receiving Exparel, 53 receving Bupivacaine | 67 ± 8.8 (48–86) years receiving Exparel, 68.6 ± 9.2 (52-89) receiving Bupivacaine | 34 women (59%) receiving Exparel, 32 women (60%) receiving Bupivacaine | Patients undergoing a total knee arthroplasty | Unilateral, Cemented Total Knee Arthroplasty through a mini-subvastus approach, anteriorly stabilized, with resurfacing of patelle | Exparel 20 mL (266 mg) + 30 mL 0.25% Bupivacaine + 0.25% Bupivacaine 60 mL | Liposomal bupivacaine did not demonstrate improved pain scores, lower narcotic use, or better knee motion during hospitalization | 3 cases (5%) and 2 controls (4%) had post-operatve nausea |
| Bagsby et al. (2014) [64] | Retrospective, cohort study, systematic (consecutive) recruitment | 150; 65 receiving Exparel, 85 receiving Ropivacaine | 63.13 ± 10.32 years receiving Exparel, 65.19 ± 9.21 years receiving Ropivacaine | 47 (72.3%) women receiving Exparel, 61 (70.9%) women receiving Ropivacaine | Patients undergoing total knee arthroplasty | Total Knee Arthroplasty | Exparel 20 cc + 30 cc Saline + 30 cc 0.5% Marcaine | Exparel provided inferior pain control compared to Ropivacaine (p = 0.04), being more expensive | In the Exparel group, 3/65 patients (4.6%) reported a wound drainage at 3–4 weeks post-surgery and an acute postoperative methicillin sensitive staphilococcal infection requiring reoperation |
| Webb et al. (2015) [65] | Retrospective, case-control study, systematic (consecutive) recruitment | 100; 50 receiving Exparel, 50 serving as controls | 64 (46–88) years receiving Exparel, 64 (38–85) years serving as controls | 34 (68%) women receiving Exparel, 32 (64%) serving as controls | Patients undergoing total knee arthroplasty | Total Knee Arthroplasty | Exparel 20 mL (266 mg) + 40 mL Saline | Use of Exparel resulted in decreased narcotic usage (60.97 mg oral morphine equivalent versus 89.74 mg, p = 0.009). Periarticular Total Knee Arthroplasty injection using liposomal bupivacaine in patients with a Body Mass Index less than 40 kg/m2 and few co-morbidities lead to earlier hospital discharge ((2.64 days versus 3.06 days, p = 0.004) and decreased narcotic usage over 24–48 h (110.66 mg versus 182.47 mg, p = 0.013), and over 48–72 h (49.61 mg versus 112.65 mg, p = 0.004) | Not reported |
| Mont et al. (2018) [66] | Phase 4, randomized, double-blinded, active-controlled, parallel-group, multi-center clinical trial, sample size a priori computed, systematic recruitment | 139 (out of an initial list of 140 patients), 70 receiving Exparel, 69 receiving Bupivacaine | 66 ± 8.61 years receiving Exparel, 66 ± 7.21 years receiving Bupivacaine | 43 women (61.4%) receiving Exparel, 39 women (56.5%) receiving Bupivacaine | Patients with degenerative knee osteoarthritis undergoing total knee arthroplasty | Primary, Unilateral, Tricompartimental, Total Knee Arthroplasty | Exparel 20 mL (266 mg) + 40 mL Saline + 50% Bupivacaine 20 mL | Exparel provides significantly reduced postsurgical pain (area under the curve of visual analog scale pain intensity score 12–48 h post-surgery 180.8 versus 209.3, p = 0.0381), reduced opioid consumption (18.7 mg versus 84.9, p = 0.0048), percentage of patients (p < 0.01), and time to first opioid rescue (p = 0.0230) | 64.3% receiving Exparel versus 56.5% receiving Bupivacaine experienced mild-to-modest adverse events |
| Barrington et al. (2015) [69] | Prospective, randomized clinical trial, sample size power calculated a posteriori, systematic (consecutive) recruitment | 2248; 1124 receiving a classical, well-established multimodal analgesia, including peri-articular injection, 1124 receiving Exparel (pre-post design) | 63.1 (19.0–95.0) years receiving the multimodal analgesia, 65.8 (32.0–96.0) years receiving Exparel, for hip procedures, 66.7 (36.0–93.0) years receiving the multimodal analgesia, 66.7 (38.0–97.0) years for receiving Exparel, for knee procedures | 56.5% women receiving the multimodal analgesia, 57.2% receiving Exparel, for hip procedures, 58.7% women receiving the multimodal analgesia, 57.5% receiving Exparel, for knee procedures | Patients undergoing knee/hip arthroplasty | Knee/Hip Arthroplasty (primary knee, 48%, revision knee, 45%, unicompartmental knee, 56%, bilateral knee, 46%, primary hip, 50%, revision hip, 47%, and bilateral hip, 50%) | Exparel versus multimodal analgesia | Improved overall mean VAS pain scores for hip (1.67 versus 2.30, p < 0.0001) and for knee (2.21 versus 2.52, p < 0.0001) procedures, an increased number of pain-free patients, decreased hospital length of stay (p < 0.0001), trends toward decreased falls (p = 0.021), and decreased overall cost | Not reported |
| Techniques | Disadvantages | Author (Year) |
|---|---|---|
| Bangham method |
| Bangham et al. (1974) [26] |
| Extrusion method | Mui et al. (2003) [27] | |
| Microfluidic channel | Andar et al. (2014) [28] | |
| Ethanol Injection | Charcosset et al. (2015) [29] |
| Techniques | Disadvantages | Author (Year) |
|---|---|---|
| Supercritical reverse phase evaporation |
| Otake et al. (2006) [30] |
| Depressurization of an Expanded Solution into Aqueous Media | Meure et al. (2009) [31] | |
| Depressurization of an Expanded Liquid Organic Solution | Zhao, Tamelli (2015) [32] | |
| Supercritical Anti-Solvent | Lesoin et al. (2011) [33] |
| Commercialized Liposomes Formulation | Commercial Name | Author (Year) |
|---|---|---|
| PEGylated liposomal doxorubicin | (Doxil/Caelyx) | Gabizon et al. (2003) [34] |
| Non-PEGylated liposomal doxorubicin | (Myocet) | Rivankar (2014) [35] |
| Liposomal daunorubicin | (DaunoXome) | Petre, Dittmer (2007) [36] |
| Liposomal cytarabine | (DepoCyt) | Bomgaars et al. (2004) [37] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cipollaro, L.; Trucillo, P.; Bragazzi, N.L.; Della Porta, G.; Reverchon, E.; Maffulli, N. Liposomes for Intra-Articular Analgesic Drug Delivery in Orthopedics: State-of-Art and Future Perspectives. Insights from a Systematic Mini-Review of the Literature. Medicina 2020, 56, 423. https://doi.org/10.3390/medicina56090423
Cipollaro L, Trucillo P, Bragazzi NL, Della Porta G, Reverchon E, Maffulli N. Liposomes for Intra-Articular Analgesic Drug Delivery in Orthopedics: State-of-Art and Future Perspectives. Insights from a Systematic Mini-Review of the Literature. Medicina. 2020; 56(9):423. https://doi.org/10.3390/medicina56090423
Chicago/Turabian StyleCipollaro, Lucio, Paolo Trucillo, Nicola Luigi Bragazzi, Giovanna Della Porta, Ernesto Reverchon, and Nicola Maffulli. 2020. "Liposomes for Intra-Articular Analgesic Drug Delivery in Orthopedics: State-of-Art and Future Perspectives. Insights from a Systematic Mini-Review of the Literature" Medicina 56, no. 9: 423. https://doi.org/10.3390/medicina56090423
APA StyleCipollaro, L., Trucillo, P., Bragazzi, N. L., Della Porta, G., Reverchon, E., & Maffulli, N. (2020). Liposomes for Intra-Articular Analgesic Drug Delivery in Orthopedics: State-of-Art and Future Perspectives. Insights from a Systematic Mini-Review of the Literature. Medicina, 56(9), 423. https://doi.org/10.3390/medicina56090423