Effects of Chewing Exerciser on the Recovery of Masticatory Function Recovery after Orthognathic Surgery: A Single-Center Randomized Clinical Trial, a Preliminary Study

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
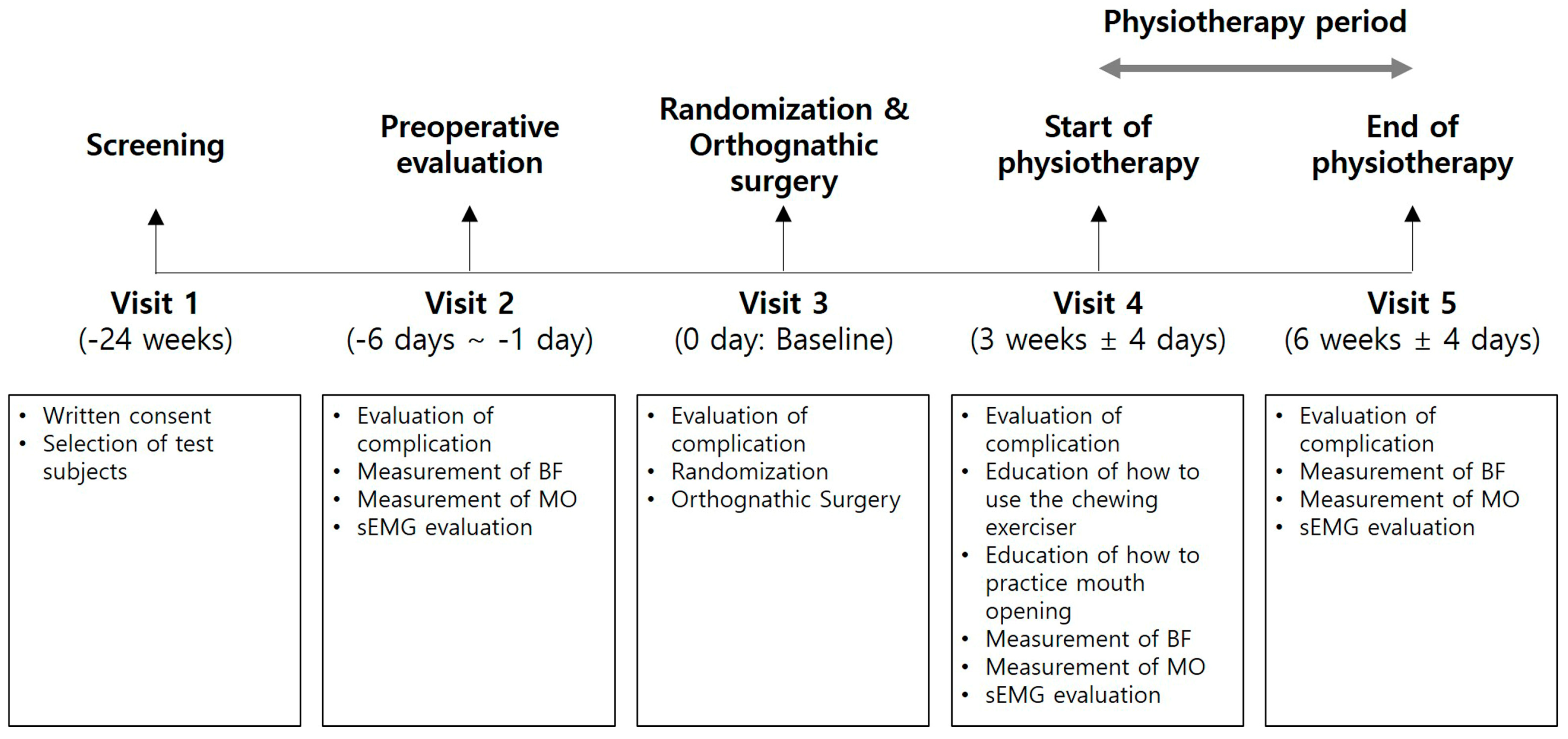
2.1. Study Design/Sample
2.2. Surgical Phase
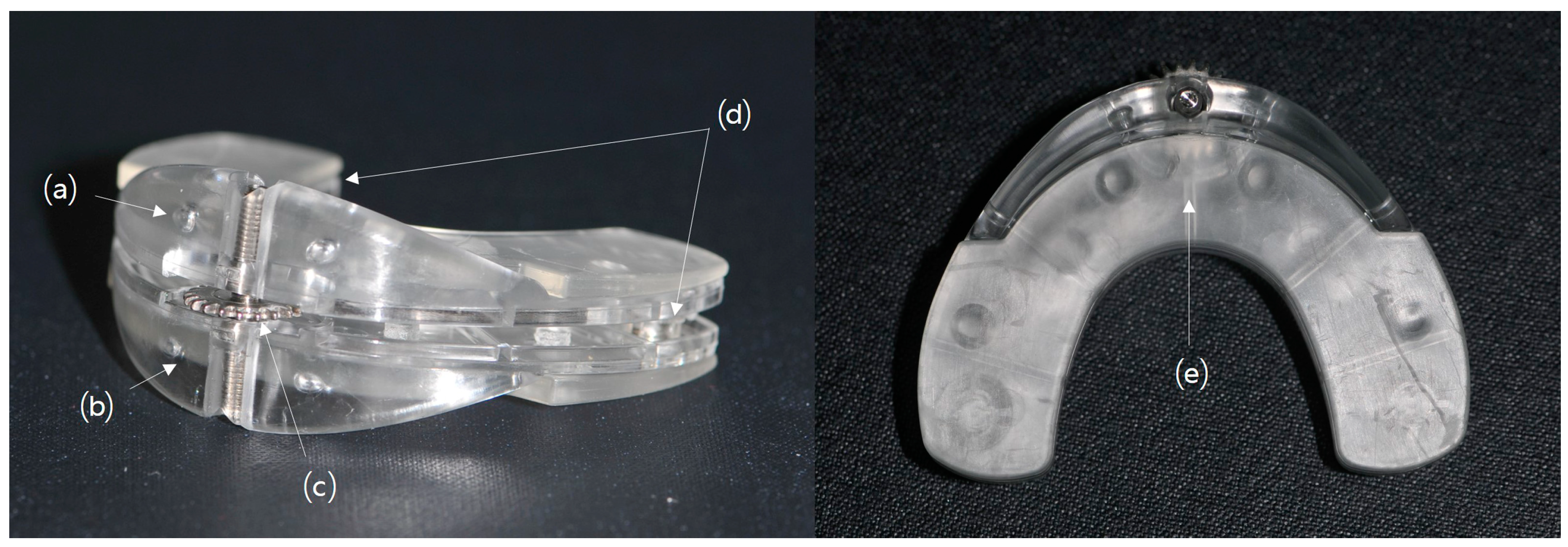
2.3. Use of Chewing Exerciser and Physiotherapy after Surgery
2.4. Evaluation of Masticatory Function
2.5. Statistical Analysis
3. Results
3.1. Subjects
3.2. Bite Force
3.3. Amount of Mouth Opening
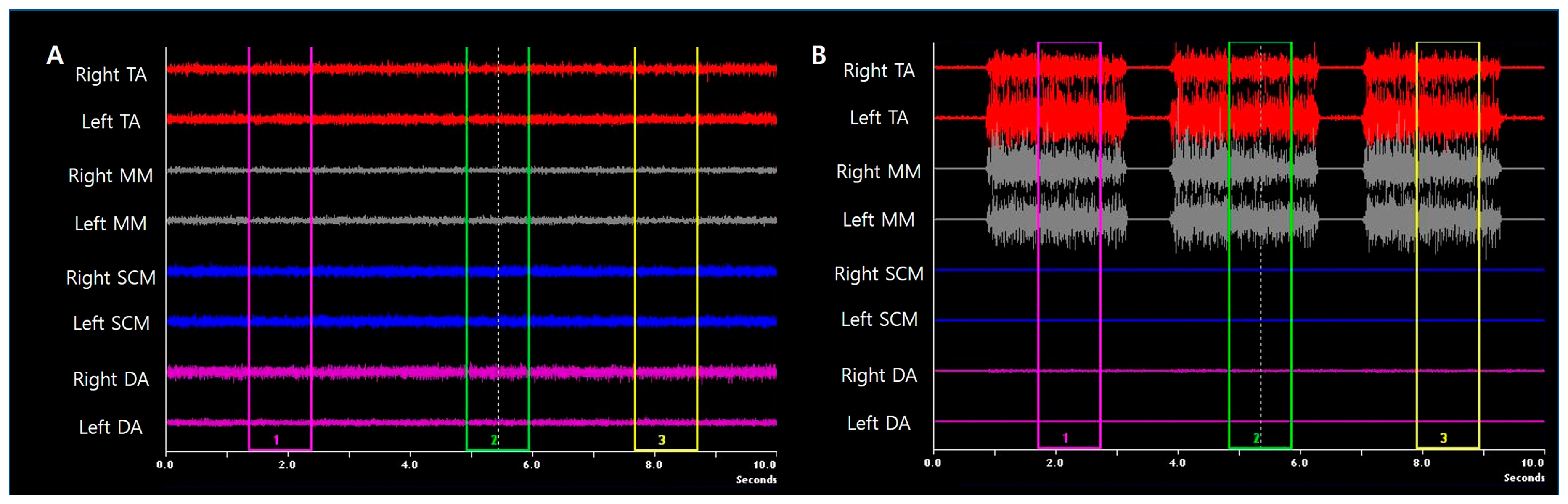
3.4. Surface Electromyography of Masticatory Muscles
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pahkala, R.; Kellokoski, J.K. Surgical-orthodontic treatment and patients’ functional and psychosocial well-being. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.H.; Hägg, U.; Rabie, A.B. Concerns and motivations of skeletal Class III patients receiving orthodontic-surgical correction. Int. J. Adult Orthod. Orthognath. Surg. 2001, 16, 7–17. [Google Scholar]
- Islam, I.; Lim, A.; Wong, R.C.W. Changes in bite force after orthognathic surgical correction of mandibular prognathism: A systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Reyneke, J.P.; Ferretti, C. The Bilateral Sagittal Split Mandibular Ramus Osteotomy. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2016, 24, 27–36. [Google Scholar] [CrossRef]
- Aragon, S.B.; Van Sickels, J.E. Mandibular range of motion with rigid/nonrigid fixation. Oral Surg. Oral Med. Oral Pathol. 1987, 63, 408–411. [Google Scholar] [CrossRef]
- Storum, K.A.; Bell, W.H. Hypomobility after maxillary and mandibular osteotomies. Oral Surg. Oral Med. Oral Pathol. 1984, 57, 7–12. [Google Scholar] [CrossRef]
- Boyd, S.B.; Karas, N.D.; Sinn, D.P. Recovery of mandibular mobility following orthognathic surgery. J. Oral Maxillofac. Surg. 1991, 49, 924–931. [Google Scholar] [CrossRef]
- Kawazoe, Y.; Kobayashi, M.; Tasaka, T.; Tamamoto, M. Effects of therapeutic exercise on masticatory function in patients with progressive muscular dystrophy. J. Neurol. Neurosurg. Psychiatry 1982, 45, 343–347. [Google Scholar] [CrossRef] [Green Version]
- Thompson, D.; Throckmorton, G.S.; Buschang, P.H. The effects of isometric exercise on maximum voluntary bite forces and jaw muscle strength and endurance. J. Oral Rehabil. 2001, 28, 909–917. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Teng, T.T.-Y.; Huang, C.-S.; Chen, Y.-R. The effect of early physiotherapy on the recovery of mandibular function after orthognathic surgery for class III correction. Part II: Electromyographic activity of masticatory muscles. J. Cranio-Maxillofac. Surg. 2015, 43, 138–143. [Google Scholar] [CrossRef]
- Kato, K.; Kobayashi, T.; Kato, Y.; Takata, Y.; Yoshizawa, M.; Saito, C. Changes in masticatory functions after surgical orthognathic treatment in patients with jaw deformities: Efficacy of masticatory exercise using chewing gum. J. Oral Maxillofac. Surg. Med. Pathol. 2012, 24, 147–151. [Google Scholar] [CrossRef]
- Hunsuck, E.E. A modified intraoral sagittal splitting technic for correction of mandibular prognathism. J. Oral Surg. 1968, 26, 250–253. [Google Scholar] [PubMed]
- Park, M.-K.; Cho, S.-M.; Yun, K.-I.; Park, J.U. Change in Bite Force and Electromyographic Activity of Masticatory Muscle in Accordance With Change of Occlusal Plane. J. Oral Maxillofac. Surg. 2012, 70, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Grünheid, T.; Langenbach, G.E.J.; Korfage, J.A.M.; Zentner, A.; Van Eijden, T.M.G.J. The adaptive response of jaw muscles to varying functional demands. Eur. J. Orthod. 2009, 31, 596–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, E.W.-C.; Huang, C.-S.; Lo, L.-J.; Chen, Y.-R. Alteration of Masticatory Electromyographic Activity and Stability of Orthognathic Surgery in Patients with Skeletal Class III Malocclusion. J. Oral Maxillofac. Surg. 2013, 71, 1249–1260. [Google Scholar] [CrossRef]
- Celakil, D.; Ozdemir, F.; Eraydin, F.; Celakil, T. Effect of orthognathic surgery on masticatory performance and muscle activity in skeletal Class III patients. CRANIO® 2018, 36, 174–180. [Google Scholar] [CrossRef]
- Ugolini, A.; Mapelli, A.; Segù, M.; Galante, D.; Sidequersky, F.V.; Sforza, C. Kinematic analysis of mandibular motion before and after orthognathic surgery for skeletal Class III malocclusion: A pilot study. CRANIO® 2017, 35, 94–100. [Google Scholar] [CrossRef]
- Dworkin, S.F.; LeResche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. 1992, 6, 301–355. [Google Scholar]
- Sebastiani, A.M.; Baratto-Filho, F.; Bonotto, D.; Klüppel, L.E.; Rebellato, N.L.B.; Da Costa, D.J.; Scariot, R.; Information, P.E.K.F.C. Influence of orthognathic surgery for symptoms of temporomandibular dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 119–125. [Google Scholar] [CrossRef]
- Disselhorst-Klug, C.; Schmitz-Rode, T.; Rau, G. Surface electromyography and muscle force: Limits in sEMG–force relationship and new approaches for applications. Clin. Biomech. 2009, 24, 225–235. [Google Scholar] [CrossRef]
- Prado, D.G.D.A.; Felix, G.B.; Migliorucci, R.R.; Bueno, M.D.R.S.; Rosa, R.R.; Polizel, M.; Teixeira, I.F.; Gavião, M.B.D. Effects of orofacial myofunctional therapy on masticatory function in individuals submitted to orthognathic surgery: A randomized trial. J. Appl. Oral Sci. 2018, 26, 20170164. [Google Scholar] [CrossRef] [Green Version]
- Deguchi, T.; Garetto, L.P.; Sato, Y.; Potter, R.H.; Roberts, W.E. Statistical analysis of differential lissajous EMG from normal occlusion and Class III malocclusion. Angle Orthod. 1995, 65, 151–160. [Google Scholar] [PubMed]
- Eshghpour, M.; Sani, S.A.D. Electromyographic Analysis of Masseter Muscle after Surgical Correction of Mandibular Prognathism. Int. J. Head Neck Surg. 2012, 3, 121–124. [Google Scholar] [CrossRef]
- Raustia, A.M.; Oikarinen, K.S. Changes in electric activity of masseter and temporal muscles after mandibular sagittal split osteotomy. Int. J. Oral Maxillofac. Surg. 1994, 23, 180–184. [Google Scholar] [CrossRef]
- Trawitzki, L.V.; Dantas, R.; Mello-Filho, F.; Marques, W. Effect of treatment of dentofacial deformities on the electromyographic activity of masticatory muscles. Int. J. Oral Maxillofac. Surg. 2006, 35, 170–173. [Google Scholar] [CrossRef]
- Trawitzki, L.V.; Dantas, R.; Mello-Filho, F.; Marques, W. Masticatory muscle function three years after surgical correction of class III dentofacial deformity. Int. J. Oral Maxillofac. Surg. 2010, 39, 853–856. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| V2 | V4 | V5 | ∆BF | p Value | |||
|---|---|---|---|---|---|---|---|
| V2 vs. V4 | V2 vs. V5 | V4 vs. V5 | |||||
| CE | 188.4 ± 134.0 | 75.6 ± 33.4 | 133.8 ± 55.1 | 58.3 ± 35.4 | 0.002 * | 0.272 | 0.003 * |
| Con | 153.8 ± 54.9 | 85.2 ± 28.3 | 129.6 ± 49.6 | 44.5 ± 35.1 | 0.005 * | 0.114 | 0.007 * |
| p value | 0.947 | 0.262 | 0.869 | 0.391 | |||
| V2 | V4 | V5 | ∆MO | p Value | |||
|---|---|---|---|---|---|---|---|
| V2 vs. V4 | V2 vs. V5 | V4 vs. V5 | |||||
| CE | 52.8 ± 8.4 | 23.0 ± 6.7 | 38.1 ± 6.7 | 15.1 ± 6.2 | 0.002 * | 0.005 * | 0.002 * |
| Con | 53.1 ± 7.4 | 27.5 ± 4.2 | 42.0 ± 3.9 | 14.5 ± 6.6 | 0.005 * | 0.008 * | 0.005 * |
| p value | 0.766 | 0.097 | 0.146 | 0.895 | |||
| V2 | V4 | V5 | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| V2 vs. V4 | V2 vs. V5 | V4 vs. V5 | ||||||
| TA | Resting | CE | 2.28 ± 0.84 | 2.43 ± 0.51 | 3.19 ± 0.94 | 0.686 | 0.249 | 0.046 |
| Con | 1.68 ± 0.83 | 2.37 ± 0.80 | 2.14 ± 1.22 | 0.173 | 0.345 | 0.249 | ||
| p value | 0.200 | 0.810 | 0.078 | |||||
| Clenching | CE | 46.69 ± 28.24 | 38.56 ± 19.96 | 36.95 ± 15.39 | 0.345 | 0.345 | 0.917 | |
| Con | 55.48 ± 18.14 | 41.96 ± 12.98 | 43.80 ± 17.15 | 0.249 | 0.345 | 0.917 | ||
| p value | 0.749 | 0.873 | 0.423 | |||||
| MM | Resting | CE | 1.78 ± 0.81 | 1.52 ± 0.42 | 1.47 ± 0.62 | 0.225 | 0.138 | 0.465 |
| Con | 1.25 ± 0.22 | 1.69 ± 0.59 | 1.65 ± 0.67 | 0.116 | 0.249 | 0.893 | ||
| p value | 0.092 | 0.873 | 0.631 | |||||
| Clenching | CE | 48.49 ± 39.84 | 24.40 ± 19.56 | 23.98 ± 16.68 | 0.116 | 0.075 | 0.917 | |
| Con | 60.43 ± 15.51 | 28.89 ± 18.38 | 35.57 ± 24.93 | 0.028 | 0.116 | 0.753 | ||
| p value | 0.200 | 0.522 | 0.423 | |||||
| SCM | Resting | CE | 2.13 ± 0.69 | 1.98 ± 0.46 | 1.81 ± 0.37 | 0.344 | 0.293 | 0.600 |
| Con | 1.76 ± 0.44 | 2.31 ± 0.72 | 1.87 ± 0.25 | 0.078 | 0.463 | 0.345 | ||
| p value | 0.228 | 0.377 | 0.872 | |||||
| Clenching | CE | 3.13 ± 1.52 | 3.58 ± 1.77 | 4.08 ± 2.85 | 0.463 | 0.753 | 1.000 | |
| Con | 3.42 ± 1.69 | 4.71 ± 1.88 | 2.25 ± 0.47 | 0.173 | 0.141 | 0.028 | ||
| p value | 0.688 | 0.197 | 0.127 | |||||
| DA | Resting | CE | 1.59 ± 0.70 | 1.28 ± 0.24 | 1.43 ± 0.39 | 0.223 | 0.674 | 0.461 |
| Con | 1.48 ± 0.64 | 1.58 ± 0.33 | 1.55 ± 0.27 | 0.753 | 0.462 | 0.674 | ||
| p value | 0.744 | 0.199 | 0.259 | |||||
| Clenching | CE | 1.91 ± 0.88 | 2.23 ± 1.07 | 2.89 ± 2.08 | 0.686 | 0.345 | 0.463 | |
| Con | 2.53 ± 1.74 | 2.21 ± 0.79 | 2.24 ± 0.60 | 0.752 | 0.600 | 0.753 | ||
| p value | 0.936 | 1.000 | 0.936 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.J.; Kwon, I.J.; Almansoori, A.A.; Son, Y.; Kim, B.; Kim, S.-M.; Lee, J.-H. Effects of Chewing Exerciser on the Recovery of Masticatory Function Recovery after Orthognathic Surgery: A Single-Center Randomized Clinical Trial, a Preliminary Study. Medicina 2020, 56, 483. https://doi.org/10.3390/medicina56090483
Yang HJ, Kwon IJ, Almansoori AA, Son Y, Kim B, Kim S-M, Lee J-H. Effects of Chewing Exerciser on the Recovery of Masticatory Function Recovery after Orthognathic Surgery: A Single-Center Randomized Clinical Trial, a Preliminary Study. Medicina. 2020; 56(9):483. https://doi.org/10.3390/medicina56090483
Chicago/Turabian StyleYang, Hoon Joo, Ik Jae Kwon, Akram Abdo Almansoori, Yoojung Son, Bongju Kim, Soung-Min Kim, and Jong-Ho Lee. 2020. "Effects of Chewing Exerciser on the Recovery of Masticatory Function Recovery after Orthognathic Surgery: A Single-Center Randomized Clinical Trial, a Preliminary Study" Medicina 56, no. 9: 483. https://doi.org/10.3390/medicina56090483
APA StyleYang, H. J., Kwon, I. J., Almansoori, A. A., Son, Y., Kim, B., Kim, S.-M., & Lee, J.-H. (2020). Effects of Chewing Exerciser on the Recovery of Masticatory Function Recovery after Orthognathic Surgery: A Single-Center Randomized Clinical Trial, a Preliminary Study. Medicina, 56(9), 483. https://doi.org/10.3390/medicina56090483