Evaluation of Contrast Flow Patterns with Cervical Interlaminar Epidural Injection: Comparison of Midline and Paramedian Approaches


Abstract
:1. Introduction
2. Materials and Methods
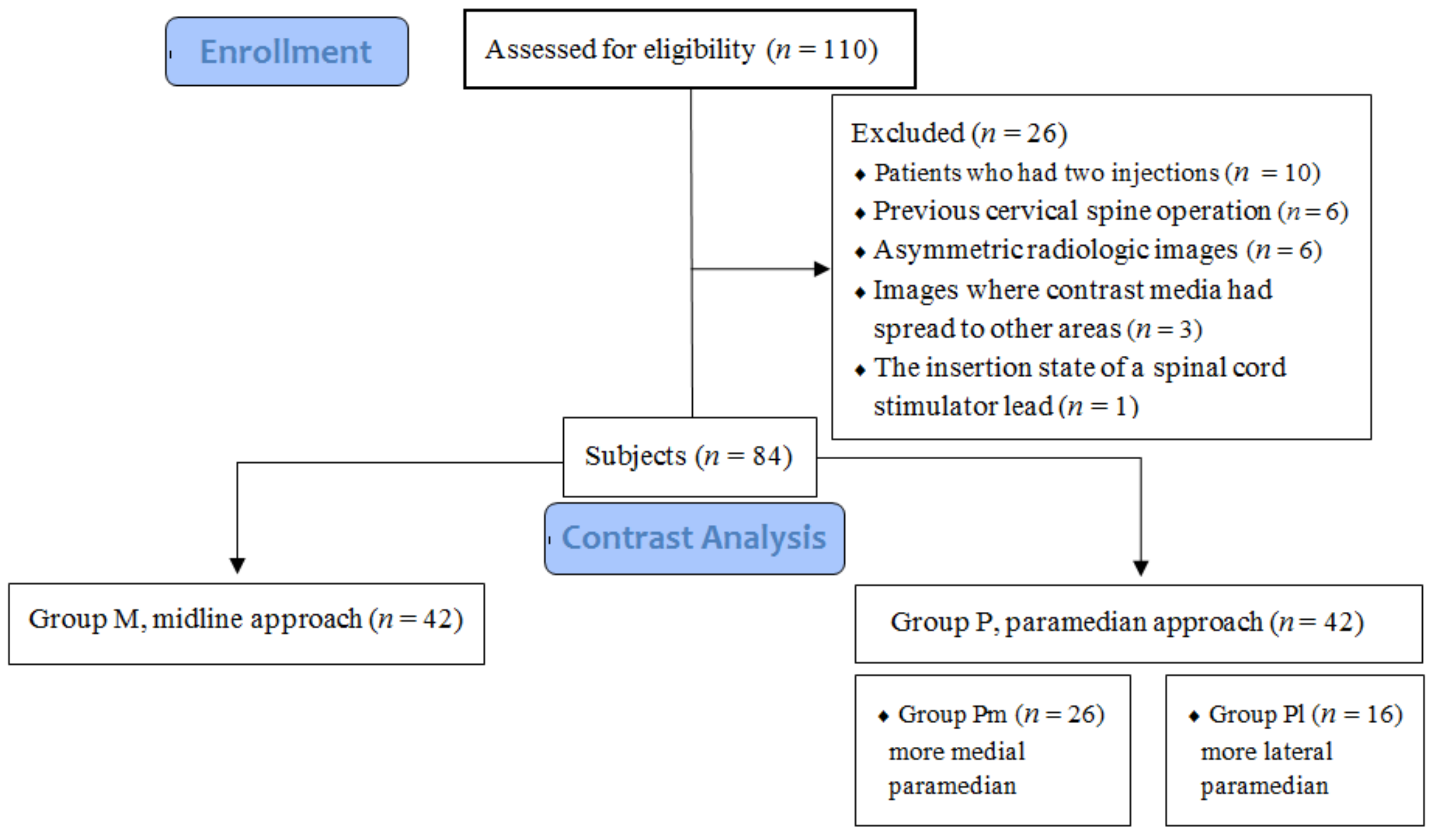
2.1. Study Population and Data
2.2. Injection Technique
2.3. Image and Data Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- House, L.M.; Barrette, K.; Mattie, R.; McCormick, Z.L. Cervical Epidural Steroid Injection: Techniques and Evidence. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Singh, S.; Kaur, S.; Singh, K.; Aujla, K. Correlation between Epidurographic Contrast Flow Patterns and Clinical Effectiveness in Chronic Lumbar Discogenic Radicular Pain Treated with Epidural Steroid Injections Via Different Approaches. Korean J. Pain 2014, 27, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Huntoon, M.A. Anatomy of the cervical intervertebral foramina: Vulnerable arteries and ischemic neurologic injuries after transforaminal epidural injections. Pain 2005, 117, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Scanlon, G.C.; Moeller-Bertram, T.; Romanowsky, S.M.; Wallace, M.S. Cervical transforaminal epidural steroid injections: More dangerous than we think? Spine 2007, 32, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Hwang, S.Y.; Lee, G.Y.; Lee, E.; Kang, H.S. Fluoroscopic cervical paramidline interlaminar epidural steroid injections for cervical radiculopathy: Effectiveness and outcome predictors. Skelet. Radiol. 2014, 43, 933–938. [Google Scholar] [CrossRef]
- Gill, J.; Nagda, J.; Aner, M.; Simopoulos, T. Cervical Epidural Contrast Spread Patterns in Fluoroscopic Antero-Posterior, Lateral, and Contralateral Oblique View: A Three-Dimensional Analysis. Pain Med. 2017, 18, 1027–1039. [Google Scholar] [CrossRef] [Green Version]
- Goel, A.; Pollan, J.J. Contrast flow characteristics in the cervical epidural space: An analysis of cervical epidurograms. Spine 2006, 31, 1576–1579. [Google Scholar] [CrossRef]
- Hashemi, M.; Dadkhah, P.; Taheri, M.; Dehghan, K.; Valizadeh, R. Cervical Epidural Steroid Injection: Parasagittal versus Midline Approach in Patients with Unilateral Cervical Radicular Pain; A Randomized Clinical Trial. Bull. Emerg. Trauma 2019, 7, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Shin, S.S.; Kim, T.S.; Jeong, C.Y.; Yoon, M.H.; Choi, J.I. Fluoroscopically guided cervical interlaminar epidural injections using the midline approach: An analysis of epidurography contrast patterns. Anesth. Analg. 2009, 108, 1658–1661. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, M.P.; Vu, T.N.; Caneris, O.; Slezak, J.; Cohen, S.P.; Sang, C.N. The role of fluoroscopy in cervical epidural steroid injections: An analysis of contrast dispersal patterns. Spine 2002, 27, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.Y.; Kwon, J.W.; Yoon, Y.C.; Lee, J. Cervical interlaminar epidural steroid injection for unilateral cervical radiculopathy: Comparison of midline and paramedian approaches for efficacy. Korean J. Radiol. 2015, 16, 604–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, J.S.; Aner, M.; Nagda, J.V.; Keel, J.C.; Simopoulos, T.T. Contralateral oblique view is superior to lateral view for interlaminar cervical and cervicothoracic epidural access. Pain Med. 2015, 16, 68–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitlock, E.L.; Bridwell, K.H.; Gilula, L.A. Influence of needle tip position on injectate spread in 406 interlaminar lumbar epidural steroid injections. Radiology 2007, 243, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, R. The dorsomedian connective tissue band in the lumbar epidural space of humans: An anatomical study using epiduroscopy in autopsy cases. Anesth. Analg. 1986, 65, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yoon, D.M.; Kwon, T.D.; Yoon, K.B. An evaluation of contrast medium spread on caudal epidurography with the needle positioned toward the affected side in patients with unilateral lumbosacral radiculopathy. Skelet. Radiol. 2012, 41, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Sasakawa, T.; Izumi, Y.; Onodera, Y.; Kunisawa, T. Ultrasound-guided lumbar plexus block using three different techniques: A comparison of ultrasound image quality. J. Anesth. 2018, 32, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Karmakar, M.K.; Lee, A.; Kwok, W.H.; Critchley, L.A.; Gin, T. Quantitative evaluation of the echo intensity of the median nerve and flexor muscles of the forearm in the young and the elderly. Br. J. Radiol. 2012, 85, e140–e145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogan, Q.H. Epidural anatomy examined by cryomicrotome section. Influence of age, vertebral level, and disease. Reg. Anesth. 1996, 21, 395–406. [Google Scholar] [PubMed]
- Ghai, B.; Vadaje, K.S.; Wig, J.; Dhillon, M.S. Lateral parasagittal versus midline interlaminar lumbar epidural steroid injection for management of low back pain with lumbosacral radicular pain: A double-blind, randomized study. Anesth. Analg. 2013, 117, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Nahm, F.S.; Lee, P.B. Comparison of contrast flow and clinical effectiveness between a modified paramedian interlaminar approach and transforaminal approach in cervical epidural steroid injection. Br. J. Anaesth. 2015, 115, 768–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| . | Group | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Total (n = 84) | Group M (n = 42) | Group P (Pm + Pl) | p * | |||
| Overall (n = 42) | Group PI (n = 16) | Group Pm (n = 26) | p† | ||||
| Sex | |||||||
| male | 48 (57.1) | 20 (47.6) | 28 (66.7) | 11 (68.8) | 17 (65.4) | 0.822 1 | 0.078 1 |
| female | 36 (42.9) | 22 (52.4) | 14 (33.3) | 5 (31.3) | 9 (34.6) | ||
| Age (years) | 57.02 ± 12.47 | 57.93 ± 12.97 | 56.12 ± 12.04 | 57.19 ± 11.46 | 55.46 ± 12.56 | 0.658 3 | |
| Impression | |||||||
| HIVD | 48 (57.1) | 24 (57.1) | 24 (57.1) | 7 (43.8) | 17 (65.4) | 0.169 1 | 10.000 1 |
| NF stenosis | 29 (34.5) | 15 (35.7) | 14 (33.3) | 7 (43.8) | 7 (26.9) | 0.261 1 | 0.818 1 |
| Cervical sprain | 4 (4.8) | 1 (2.4) | 3 (7.1) | 1 (6.3) | 2 (7.7) | 1.000 2 | 0.616 2 |
| PHN | 3 (3.6) | 2 (4.8) | 1 (2.4) | 1 (6.3) | 0 (0.0) | 0.381 2 | 1.000 2 |
| Level | |||||||
| C5-C6 | 7 (8.3) | 1 (2.4) | 6 (14.3) | 2 (12.5) | 4 (15.4) | 0.909 2 | <0.001 2 |
| C6-C7 | 23 (27.4) | 5 (11.9) | 18 (42.9) | 8 (50.0) | 10 (38.5) | ||
| C7-T1 | 54 (64.3) | 36 (85.7) | 18 (42.9) | 6 (37.5) | 12 (46.2) | ||
| Group | ||||
|---|---|---|---|---|
| Variable | Overall (n = 84) | Group M (n = 42) | Group P (Pm + Pl) (n = 42) | p Value |
| Brightness ratio | 1.47 (1.17–1.94) | 1.17 (1.10–1.41) | 1.91 (1.50–2.35) | <0.001 1 |
| Ventral spread | ||||
| (+) | 61 (72.6) | 24 (57.1) | 37 (88.1) | 0.001 2 |
| (−) | 23 (27.4) | 18 (42.9) | 5 (11.9) | |
| Group | ||||
|---|---|---|---|---|
| Variable | Overall (n = 42) | Group Pl (n = 16) | Group Pm (n = 26) | p Value |
| Brightness ratio | 1.94 ± 0.53 | 1.92 ± 0.50 | 1.94 ± 0.55 | 0.912 1 |
| Ventral spread | ||||
| (+) | 37 (88.1) | 15 (93.8) | 22 (84.6) | 0.633 2 |
| (−) | 5 (11.9) | 1 (6.3) | 4 (15.4) | |
| Ventral Spread | ||||
|---|---|---|---|---|
| Variable | Overall (n = 84) | (+) (n = 61) | (−) (n = 23) | p Value |
| Brightness ratio | 1.47 (1.17–1.94) | 1.66 (1.41–2.10) | 1.16 (1.09–1.26) | <0.001 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.; Lee, S.E.; Kim, Y.H.; Park, J.H.; Lee, K.H.; Kang, E.; Kim, S.; Kim, J.; Oh, D. Evaluation of Contrast Flow Patterns with Cervical Interlaminar Epidural Injection: Comparison of Midline and Paramedian Approaches. Medicina 2021, 57, 8. https://doi.org/10.3390/medicina57010008
Lee B, Lee SE, Kim YH, Park JH, Lee KH, Kang E, Kim S, Kim J, Oh D. Evaluation of Contrast Flow Patterns with Cervical Interlaminar Epidural Injection: Comparison of Midline and Paramedian Approaches. Medicina. 2021; 57(1):8. https://doi.org/10.3390/medicina57010008
Chicago/Turabian StyleLee, Byeongcheol, Sang Eun Lee, Yong Han Kim, Jae Hong Park, Ki Hwa Lee, Eunsu Kang, Sehun Kim, Jaehwan Kim, and Daeseok Oh. 2021. "Evaluation of Contrast Flow Patterns with Cervical Interlaminar Epidural Injection: Comparison of Midline and Paramedian Approaches" Medicina 57, no. 1: 8. https://doi.org/10.3390/medicina57010008
APA StyleLee, B., Lee, S. E., Kim, Y. H., Park, J. H., Lee, K. H., Kang, E., Kim, S., Kim, J., & Oh, D. (2021). Evaluation of Contrast Flow Patterns with Cervical Interlaminar Epidural Injection: Comparison of Midline and Paramedian Approaches. Medicina, 57(1), 8. https://doi.org/10.3390/medicina57010008