
Epidemiology of Musculoskeletal Injuries in Adult Athletes: A Scoping Review

 ,
,  , and
, and
Abstract
:1. Introduction
- injuries/1000 h exposures (/1000 h) which represents the number of injuries per 1000 h of exposures;
- injuries/1000 athlete-exposures (/1000 AEs), which is based on the total number of athletes exposed during a competition or training irrespective of their actual time of exposure [7]. An athlete-exposure is defined as “one athlete’s participation in one practice or game in which there is a possibility of sustaining an athletic injury” [6];
- injuries/1000 player-hours, represents the actual time of player-exposure that is the probability of injury for 1 player over 1000 h of total exposure” [7].
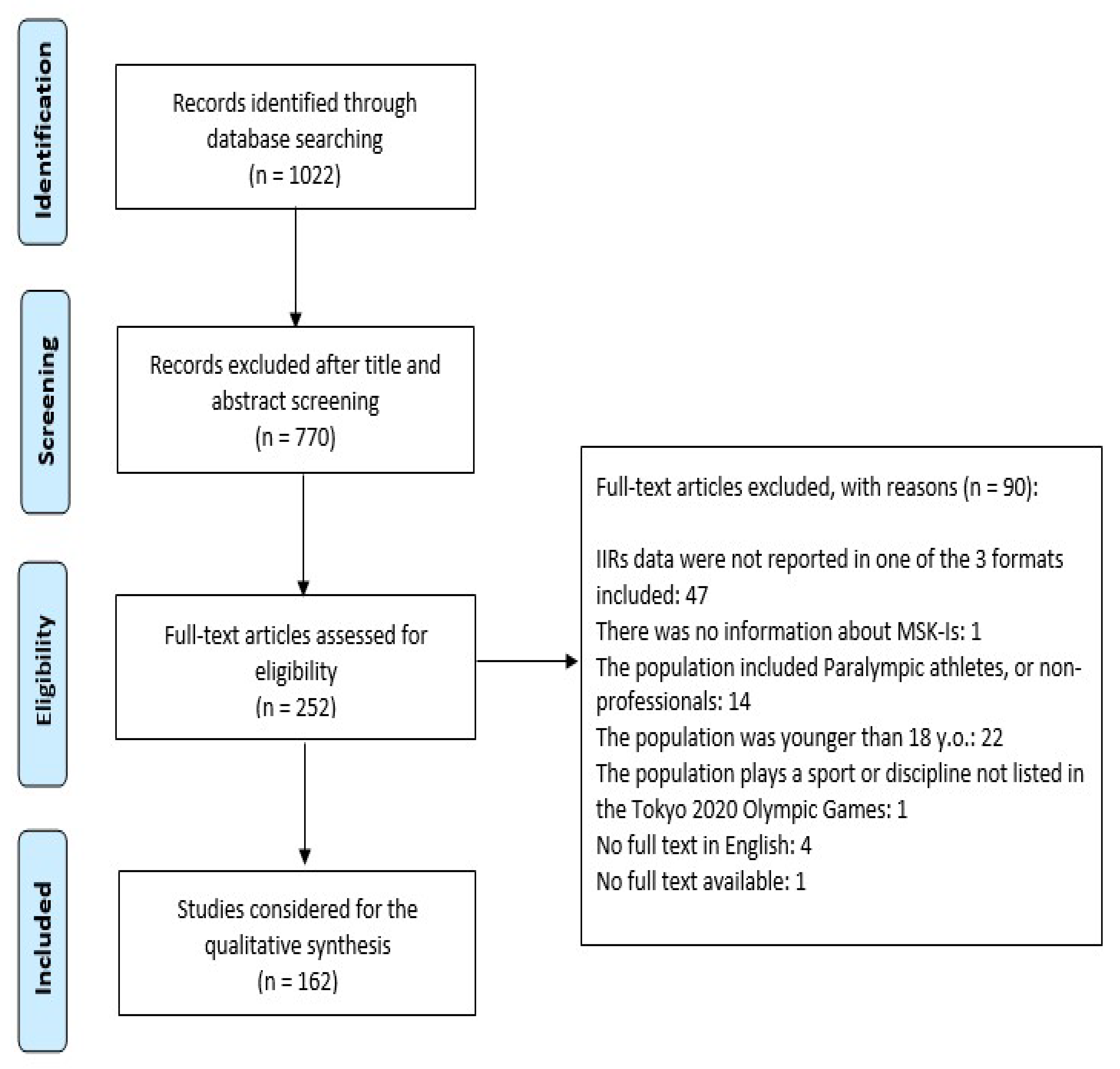
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, D.R.; Baker, R.J. Musculoskeletal injuries in sports. Prim. Care 2006, 33, 545–579. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Mccrory, P.; LaPrade, R.F.; Meeuwisse, W.H.; Engebretsen, L. The IOC Manual of Sports Injuries, 1st ed.; Wiley and Sons: Oxford, UK, 2012. [Google Scholar]
- Araújo, C.G.; Scharhag, J. Athlete: A working definition for medical and health sciences research. Scand. J. Med. Sci. Sports 2016, 26, 4–7. [Google Scholar] [CrossRef]
- International Olympic Committee. Available online: https://stillmed.olympic.org/media/Document%20Library/OlympicOrg/Games/Summer-Games/Games-Tokyo-2020-Olympic-Games/Programme-Tokyo2020-EN.pdf (accessed on 23 May 2021).
- Soligard, T.; Steffen, K.; Palmer, D.; Alonso, J.M.; Bahr, R.; Lopes, A.D.; Dvorak, J.; Grant, M.E.; Meeuwisse, W.; Mountjoy, M.; et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: A prospective study of 11274 athletes from 207 countries. Br. J. Sports Med. 2017, 51, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Armsey, T.D.; Hosey, R.G. Medical aspects of sports: Epidemiology of injuries, preparticipation physical examination, and drugs in sports. Clin. Sports Med. 2004, 23, 255–279. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.H.; Fuller, C.W. The influence of methodological issues on the results and conclusions from epidemiological studies of sports injuries: Illustrative examples. Sports Med. 2006, 36, 459–472. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mountjoy, M.; Miller, J.; Junge, A. Analysis of water polo injuries during 8904 player matches at FINA World Championships and Olympic games to make the sport safer. Br. J. Sports Med. 2019, 53, 25–31. [Google Scholar] [CrossRef]
- Chase, K.I.; Caine, D.J.; Goodwin, B.J.; Whitehead, J.R.; Romanick, M.A. A prospective study of injury affecting competitive collegiate swimmers. Res. Sports Med. 2013, 21, 111–123. [Google Scholar] [CrossRef]
- Niestroj, C.K.; Schöffl, V.; Küpper, T. Acute and overuse injuries in elite archers. J. Sports Med. Phys. Fit. 2018, 58, 1063–1070. [Google Scholar] [CrossRef]
- Krabak, B.J.; Waite, B.; Schiff, M.A. Study of Injury and Illness Rates in Multiday Ultramarathon Runners. Med. Sci. Sports Exerc. 2011, 43, 2314–2320. [Google Scholar] [CrossRef]
- Rebella, G. A prospective study of injury patterns in collegiate pole vaulters. Am. J. Sports Med. 2015, 43, 808–815. [Google Scholar] [CrossRef]
- Posner, M.; Cameron, K.L.; Wolf, J.M.; Belmont, P.J., Jr.; Owens, B.D. Epidemiology of Major League Baseball injuries. Am. J. Sports Med. 2011, 39, 1676–1680. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.W.; Hamstra-Wright, K.L.; Dick, R.; Grove, K.A.; Agel, J. Descriptive epidemiology of collegiate women’s softball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J. Athl. Train 2007, 42, 286–294. [Google Scholar] [PubMed]
- Zuckerman, S.L.; Wegner, A.M.; Roos, K.G.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. Injuries sustained in National Collegiate Athletic Association men’s and women’s basketball, 2009/2010–2014/2015. Br. J. Sports Med. 2018, 52, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Siewe, J.; Rudat, J.; Zarghooni, K.; Sobottke, R.; Eysel, P.; Herren, C.; Knöll, P.; Illgner, U.; Michael, J. Injuries in competitive boxing. A prospective study. Int. J. Sports Med. 2015, 36, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Walrod, B.; Turner, W.; Hartz, C. A Prospective Cohort Study of Collegiate Fencing Injuries. Curr. Sports Med. Rep. 2019, 18, 361–366. [Google Scholar] [CrossRef]
- Theilen, T.M.; Mueller-Eising, W.; Wefers Bettink, P.; Rolle, U. Injury data of major international field hockey tournaments. Br. J. Sports Med. 2016, 50, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Junge, A.; Dvořák, J. Football injuries during the 2014 FIFA World Cup. Br. J. Sports Med. 2015, 49, 599–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joeng, H.S.; Na, Y.M.; Lee, S.Y.; Cho, Y.J. Injuries among Korean Female Professional Golfers: A Prospective Study. J. Sports Sci. Med. 2018, 17, 492–500. [Google Scholar]
- Kay, M.C.; Register-Mihalik, J.K.; Gray, A.D.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. The Epidemiology of Severe Injuries Sustained by National Collegiate Athletic Association Student-Athletes, 2009–2010 Through 2014–2015. J. Athl. Train 2017, 52, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Luig, P.; Krutsch, W.; Nerlich, M.; Henke, T.; Klein, C.; Bloch, H.; Platen, P.; Achenbach, L. Increased injury rates after the restructure of Germany’s national second league of team handball. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1884–1891. [Google Scholar] [CrossRef] [PubMed]
- Bromley, S.J.; Drew, M.K.; Talpey, S.; McIntosh, A.S.; Finch, C.F. A systematic review of prospective epidemiological research into injury and illness in Olympic combat sport. Br. J. Sports Med. 2018, 52, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Lystad, R.P.; Augustovičová, D.; Harris, G.; Beskin, K.; Arriaza, R. Epidemiology of injuries in Olympic-style karate competitions: Systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Toohey, L.A.; Drew, M.K.; Finch, C.F.; Cook, J.L.; Fortington, L.V. A 2-Year Prospective Study of Injury Epidemiology in Elite Australian Rugby Sevens: Exploration of Incidence Rates, Severity, Injury Type, and Subsequent Injury in Men and Women. Am. J. Sports Med. 2019, 47, 1302–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.; Leong, D.; Vaz Pardal, C.; Lin, C.Y.; Kam, J.W. Injury and illness surveillance at the International Sailing Federation Sailing World Championships 2014. Br. J. Sports Med. 2016, 50, 673–981. [Google Scholar] [CrossRef]
- Schöffl, V.R.; Kuepper, T. Injuries at the 2005 World Championships in Rock Climbing. Wilderness Environ. Med. 2006, 17, 187. [Google Scholar] [CrossRef]
- Dakic, J.G.; Smith, B.; Gosling, C.M. Musculoskeletal injury profiles in professional Women’s Tennis Association players. Br. J. Sports Med. 2018, 52, 723–729. [Google Scholar] [CrossRef]
- Gosling, C.M.; Gabbe, B.J.; Forbes, A.B. Triathlon related musculoskeletal injuries: The status of injury prevention knowledge. J. Sci. Med. Sport 2008, 11, 396–406. [Google Scholar] [CrossRef]
- Baugh, C.M.; Weintraub, G.S.; Gregory, A.J.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. Descriptive Epidemiology of Injuries Sustained in National Collegiate Athletic Association Men’s and Women’s Volleyball, 2013–2014 to 2014–2015. Sports Health 2018, 10, 60–69. [Google Scholar] [CrossRef]
- Aasa, U.; Svartholm, I.; Andersson, F.; Berglund, L. Injuries among weightlifters and powerlifters: A systematic review. Br. J. Sports Med. 2017, 51, 211–219. [Google Scholar] [CrossRef]
- Raske, A.; Norlin, R. Injury incidence and prevalence among elite weight and power lifters. Am. J. Sports Med. 2002, 30, 248–256. [Google Scholar] [CrossRef]
- Agel, J.; Ransone, J.; Dick, R.; Oppliger, R.; Marshall, S.W. Descriptive epidemiology of collegiate men’s wrestling injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J. Athl. Train 2007, 42, 303–310. [Google Scholar]
- Cohen, S.B.; Sheridan, S.; Ciccotti, M.G. Return to sports for professional baseball players after surgery of the shoulder or elbow. Sports Health 2011, 3, 105–111. [Google Scholar] [CrossRef]
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J. Athl. Train 2007, 42, 311–319. [Google Scholar]
- Markolf, K.L.; Burchfield, D.M.; Shapiro, M.M.; Shepard, M.F.; Finerman, G.A.; Slauterbeck, J.L. Combined knee loading states that generate high anterior cruciate ligament forces. J. Orthop. Res. 1995, 13, 930–935. [Google Scholar] [CrossRef]
- Murtaugh, K. Field hockey injuries. Curr. Sports Med. Rep. 2009, 8, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Junge, A.; Langevoort, G.; Pipe, A.; Peytavin, A.; Wong, F.; Mountjoy, M.; Beltrami, G.; Terrell, R.; Holzgraefe, M.; Charles, R.; et al. Injuries in team sport tournaments during the 2004 Olympic Games. Am. J. Sports Med. 2006, 34, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, E.A.; van Mechelen, W.; de Vente, W. The effect of preventive measures on the incidence of ankle sprains. Clin. J. Sports Med. 2000, 10, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naicker, M.; McLean, M.; Esterhuizen, T.M. Poor peak dorsiflexor torque associated with incidence of ankle injury in elite female field hockey players. J. Sci. Med. Sport 2007, 10, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Reilly, T.; Seaton, A. Physiological strain unique to field hockey. J. Sports Med. Phys. Fit. 1990, 30, 142–146. [Google Scholar]
- Wanivenhaus, F.; Fox, A.J.; Chaudhury, S.; Rodeo, S.A. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health 2012, 4, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Cairns, M.A.; Hasty, E.K.; Herzog, M.M.; Ostrum, R.F.; Kerr, Z.Y. Incidence, Severity, and Time Loss Associated With Collegiate Football Fractures, 2004–2005 to 2013–2014. Am. J. Sports Med. 2018, 46, 987–994. [Google Scholar] [CrossRef]
- WHO. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]


{kind=link}
| Sport (Disciplines) | Injury Sites 2 | Types of Injury | IIRs 1,2 |
|---|---|---|---|
| Aquatic (Swimming [9], Marathon swimming, Diving, Artistic swimming, Water polo [10]) | Swimming: upper extremity (38.7%), lower extremity (42.0%), body trunk (19.3%) Water polo: upper extremity (38.7%), lower extremity (18.8%), body trunk (16.9%) | Swimming: tendonitis (58%), strain (35.5%), and sprain (6.5%) Water polo: (sub)luxation/sprain (22.7%), strain (9.9%), tendinosis/arthritis/bursitis/impingement or similar (9.1%), fracture (5.1%), muscle spasm (4.0%), tendon/ligament rupture (1.1%) | Swimming: 3.04/1000 h (95% CI 2.04, 4.49) or 5.55/1000 AEs (95% CI 3.73, 8.18) Water polo: 56.2/1000 h (95% CI ± 6.74) competition |
| Archery [11] | Overuse: upper extremity (86.2%), body trunk (11.8%). Acute: upper extremity (83.4%). | Overuse: tendons, ligaments, and articulation injuries (67.9%) Acute: fractures (83.3%) | 0.00536/1000 h (overuse and acute) |
| Athletics [12,13] | Marathon: lower extremity (92.6%) Pole vault: upper extremity (20.8%), lower extremity (59.8%), body trunk (18.1%) | Marathon: tendonitis (10.3%), strain (2.4%), sprain (2.3%), bursitis (1.0%) (major and minor injuries) Pole vault: strain (37.5%), sprain (18.1%), stress reaction (13.9%), tendinitis (11.1%), fracture (11.1%) | Marathon: 65.0/1000 h (95% CI 61.4, 68.7); major MSK-Is 0.8/1000 h (95% CI 0.4, 1.3), minor MSK-Is 11.2/1000 h (95% CI 9.8, 12.9) Pole vault: 7.9/1000 AEs (95% CI, 6.2, 10.0) |
| Badminton | Data not available | Data not available | Data not available |
| Baseball [14]/Softball [15] | Baseball: upper extremity (51.4%), lower extremity (30.6%), body trunk (11.7%) Softball: upper extremity (33.1%), lower extremity (42.1%), body trunk (9.8%) | Baseball: data not available Softball: ligament sprain, muscle-tendon strain (data not available) | Baseball: 3.61/1000 AEs (95% CI = 3.49, 3.74) Softball: 4.30/1000 AEs (95% CI = 4.13, 4.47) competition; 2.67/1000 AEs (95% CI = 2.57, 2.77) training |
| Basketball (3 × 3, basketball [16]) | Men: upper extremity (18.5%), lower extremity (58.7%), body trunk (8.4%) Women: upper extremity (14.5%), lower extremity (63.1%), body trunk (6.4%) | Men: sprain (30.1%), strain (14.3%), tendonitis (3.8%), fracture (3.2%), dislocation (3.0%), spasm (2.6%), inflammation (1.8%) Women: sprain (29.0%), strain (16.7%), tendonitis (5.2%), inflammation (4.6%), dislocation (3.2%), fracture (3.0%), spasm (2.6%) | Men: 7.97/1000 AEs (95% CI 7.65, 8.30) Women: 6.54/1000 AEs (95% CI 6.22, 6.85) |
| Boxing [17] | Upper extremity (24.5%), lower extremity (15.6%), body trunk (14.1%) | Tear (12.0%), pain (7.8%), strain (4.2%), rupture (2.0%), fracture (1.0%) | 12.8/1000 h (training) |
| Canoeing (slalom, sprint) | Data not available | Data not available | Data not available |
| Cycling (BMX freestyle, BMX racing, mountain bike, road, track) | Data not available | Data not available | Data not available |
| Equestrian (eventing, dressage, jumping) | Data not available | Data not available | Data not available |
| Fencing [18] | Upper extremity (42.9%), lower extremity (35.7%), body trunk (21.4) | Sprain (25.0%), Pain (25.0%) | 2.43/1000 AEs |
| Hockey (field hockey [19]) | Men: upper extremity (19.0%), lower extremity (41.0%), body trunk (4.0%) Women: upper extremity (14.0%), lower extremity (28.0%), body trunk (0.0%) | Data not available | 36.2/1000 player-hours (95% CI 31.6, 40.8) Men: 48.3/1000 player-hours (95% CI 30.9, 65.8) Women: 29.1/1000 player-hours (95% CI 18.6,39.7) |
| Football (soccer [20]) | Upper extremity (10%), lower extremity (65%), body trunk (7%) | Strain/muscle fibre rupture (24%), sprain/dislocation (8%), fracture (6%), tendon or ligament rupture/meniscus lesion (4%) | 29.3/1000 h (95% CI 21.9, 36.7); 50.8/1000 player-hours (95% CI 41.0, 60.6) |
| Golf [21] | Upper extremity (40.7%), lower extremity (26.1%), body trunk (29.0%) | Tendinosis/tendinopathy (21.2%), ligament sprain (13.6%), meniscus lesions (11.2%), muscle strain, rupture, or tear (9.1%), and inflammation of unknown cause (7.0%) | 8.5/1000 AEs (competition), and 3.3/1000 AEs (training) |
| Gymnastics [22] (artistic, rhythmic, trampoline) | Severe injuries: upper extremity (16.5%), lower extremity (64.5%), body trunk (8.9%) | Severe injuries: sprain (31.6%), strain (13.9%), fracture (13.9%), dislocation (8.9%), sub-luxation (3.8%), inflammation (2.5%) | Women: 1.40/1000 AEs (95% CI 1.09, 1.71) |
| Handball [23] | Upper extremity (28.7%), lower extremity (52.0%), body trunk (17.2%) | Sprain (26.5%), rupture (12.2%), strain (4.9%), fracture (4.4%), subluxation/dislocation (2.3%) | 4.3/1000 player-hours |
| Judo [24] | Upper extremity (10.2%), lower extremity (9.7%), body trunk (10.9%) | Data not available | 4.2/1000 h (training) |
| Karate [25] (kata, kumite) | Lower extremity (12.0%) | Data not available | 88.3/1000 AEs (95% CI 66.6, 117.2) |
| Modern pentathlon | Data not available | Data not available | Data not available |
| Rowing | Data not available | Data not available | Data not available |
| Rugby (rugby sevens [26]) | Upper extremity (21.4%), lower extremity (58.3%), body trunk (5.5%) | Joint sprains (25.2%), muscle injury (16.7%), tendon injury (12.1%), cartilage injury/impingement (9.3%), joint dislocation/instability (5.5%), bone injury (5.5%) | 43.2/1000 player-hours (95% CI, 43.0–43.3) |
| Sailing [27] | Upper extremity (12%), lower extremity (23%), body trunk (29%) | Muscle cramp/spasm (20%), muscle strain (13%), sprain (13%), tendinopathy (13%) | 0.59/1000 h |
| Shooting | Data not available | Data not available | Data not available |
| Skateboarding | Data not available | Data not available | Data not available |
| Sport climbing [28] | Lower extremity (11.1%), body trunk (5.6%) | Sprain (11.1%), fractures (5.6%) | 3.1/1000 h |
| Surfing | Data not available | Data not available | Data not available |
| Table tennis | Data not available | Data not available | Data not available |
| Taekwondo [24] | Upper extremity (22.8%), lower extremity (9.1%) | Data not available | 19.09/1000 AEs (competition) |
| Tennis [29] | Upper extremity (23.2%), lower extremity (51.4), body trunk (18.5%) | Muscle rupture/tear/spasm/cramp (32.9%), synovitis (20.4%), tendon tear/tendinopathy/bursitis (17.6%), ligament injury (8.3%), dislocation/subluxation/instability (6.0%), lesion of meniscus/articular cartilage (3.2%), fasciitis (2.3%), fracture (0.9%) | 56.6/1000 h (95% CI: 49.5, 64.6) competition; 62.7/1000 h (95% CI: 54.8, 71.6) training |
| Triathlon [30] | Upper extremity/shoulder (up to 19%), lower extremity (36–85%), body trunk (up to 72%) | Muscle/tendon lesions (30–55%), tendinitis (13–25%), and ligament/joint injuries (6–29%) | 17.4/1000 h (competition), 0.7–5.4/1000 h (training) |
| Volleyball (beach volleyball, volleyball [31]) | Men: upper extremity (30.5%), lower extremity (46.3%), body trunk (12.2%) Women: upper extremity (19.2%), lower extremity (58.0%), body trunk (11.7%) | Men: sprains (22.0%), and strain (19.5%), inflammatory conditions (19.5%), fracture (6.1%), dislocation/subluxation (2.4%), entrapment/impingement (2.4%), sacroiliac dysfunction (1.2%), spasm (1.2%) Women: sprains (23.8%), strain (21.4%), inflammatory conditions (14.7%), fracture (2.8%), spasm (2.4%), entrapment/impingement (2.0%), patella femoral pain syndrome (1.8%), sacroiliac dysfunction (1.4%), dislocation/subluxation (1.0%) | Men: 4.69/1000 AEs (95% CI, 3.68–5.70) Women: 7.07/1000 AEs (95% CI, 6.45–7.68) |
| Weightlifting [32,33] | Upper extremity (39%), lower extremity (23%), body trunk (37%) | Data not available | 2.4–3.3/1000 h (training) |
| Wrestling (Greco-Roman, freestyle) [34] | Upper extremity (23.1%), lower extremity (35.8%), body trunk (10.5%) | Knee internal derangements (18.9%), ankle ligament sprains (7.4%), shoulder strains (4.6%) | 5.7/1000 AEs (95% CI 5.5–5.8) training; 26.4/1000 AEs (95% CI 25.4–27.3) competition |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gimigliano, F.; Resmini, G.; Moretti, A.; Aulicino, M.; Gargiulo, F.; Gimigliano, A.; Liguori, S.; Paoletta, M.; Iolascon, G. Epidemiology of Musculoskeletal Injuries in Adult Athletes: A Scoping Review. Medicina 2021, 57, 1118. https://doi.org/10.3390/medicina57101118
Gimigliano F, Resmini G, Moretti A, Aulicino M, Gargiulo F, Gimigliano A, Liguori S, Paoletta M, Iolascon G. Epidemiology of Musculoskeletal Injuries in Adult Athletes: A Scoping Review. Medicina. 2021; 57(10):1118. https://doi.org/10.3390/medicina57101118
Chicago/Turabian StyleGimigliano, Francesca, Giuseppina Resmini, Antimo Moretti, Milena Aulicino, Fiorinda Gargiulo, Alessandra Gimigliano, Sara Liguori, Marco Paoletta, and Giovanni Iolascon. 2021. "Epidemiology of Musculoskeletal Injuries in Adult Athletes: A Scoping Review" Medicina 57, no. 10: 1118. https://doi.org/10.3390/medicina57101118
APA StyleGimigliano, F., Resmini, G., Moretti, A., Aulicino, M., Gargiulo, F., Gimigliano, A., Liguori, S., Paoletta, M., & Iolascon, G. (2021). Epidemiology of Musculoskeletal Injuries in Adult Athletes: A Scoping Review. Medicina, 57(10), 1118. https://doi.org/10.3390/medicina57101118